I. Newborn Assessment 22/6/2010 - جامعة آل البيت · PDF file–Postnatal...
83
11/07/1432 Miss: kamlah Olaimat I. Newborn Assessment 22/6/2010
Transcript of I. Newborn Assessment 22/6/2010 - جامعة آل البيت · PDF file–Postnatal...

11/07/1432 Miss: kamlah Olaimat
I. Newborn Assessment
22/6/2010
11/07/1432 Miss: kamlah Olaimat 2
Terminology
Newborn refers to a recently born infant in the
first few hours of life
Neonate refers to infants in the first 28 days of
life
Examination precaution
Hand washing
Thermal environment
Light and noise
5-10 minutes examination time
11/07/1432 Miss: kamlah Olaimat
Timing and Types of Newborn
Assessments• Immediately after birth
- Need resuscitation?
- Can be placed with mother?
• Within 1 to 4 hours after birth.
- Adaptation to extra uterine life and progress?
- Determine GA?
-Important history point in caring of newborn?
• Assessment procedures within first 24 hours or before discharge
- Complete physical examination
- Nutritional status and ability to formula-feed or breastfeed

11/07/1432 Miss: kamlah Olaimat
Important History points in caring
of newborn
• Maternal diabetes: Metabolic and congenital defect
• Polyhydramnios: Swallowing defect, GI obstruction
• Oligohydramnios: Renal disease, pulmonary hypoplasia
• Maternal age: Old age and chromosoma
• Rupture of membrane: sepsis
• Delivery type: c/s and TTN
• Maternal blood group: ABO, Rh disease
• Infection risk: Maternal Hepatitis carrier
11/07/1432 Miss: kamlah Olaimat
Initial Assessment
• Modified position which aids drainage of mucus from
nasopharynx and trachea by gravity
• The newborn assessment is performed immediately
after birth.
• Respiratory effort, heart rate and skin color for
perfusion are evaluated using the APGAR scoring
system at 1 and 5 minutes after birth.
• Listen for breath sounds in the mid-axillary area.
• Palpate the pulse at the umbilical stump or apically on
the chest.
11/07/1432 Miss: kamlah Olaimat
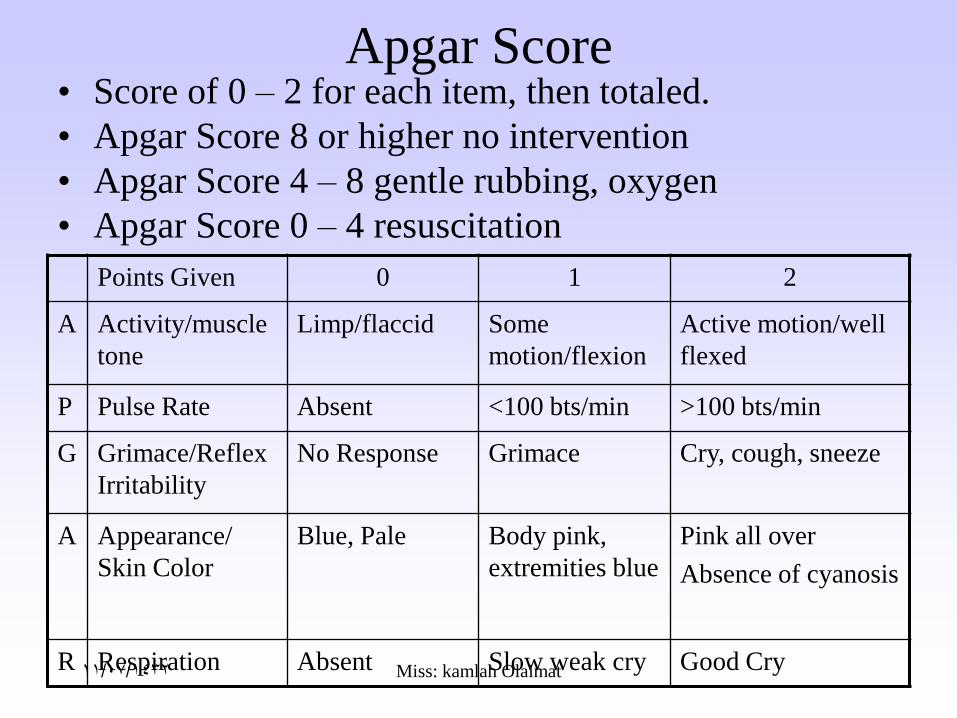
Apgar Score• Score of 0 – 2 for each item, then totaled.
• Apgar Score 8 or higher no intervention
• Apgar Score 4 – 8 gentle rubbing, oxygen
• Apgar Score 0 – 4 resuscitation
Points Given 0 1 2
A Activity/muscle
tone
Limp/flaccid Some
motion/flexion
Active motion/well
flexed
P Pulse Rate Absent <100 bts/min >100 bts/min
G Grimace/Reflex
Irritability
No Response Grimace Cry, cough, sneeze
A Appearance/
Skin Color
Blue, Pale Body pink,
extremities blue
Pink all over
Absence of cyanosis
R Respiration Absent Slow weak cry Good Cry
11/07/1432 Miss: kamlah Olaimat
Assessment of Gestational Age
• An accurate assessment incorporates size
and maturity.
• Assessment methods include:
– Mother’s menstrual history
– Prenatal ultrasonography
– Evaluation of obstetric parameters
– Postnatal maturational examinations
• Dubowitz Assessment of Gestational Age
• New Ballard Score
11/07/1432 Miss: kamlah Olaimat
Postnatal assessment of gestational age
• EDD is not always correct (only accurate 75-85% of the time)
• Performing a gestational exam helps the nurse evaluate for
potential age-related problems. Should be done in the first 4 hours
of life.
• Accuracy within 1-2 weeks
• New Ballard Score (NBS)
– physical maturity
– neuromuscular maturity
Ballard Score tool: each physical and neuromuscular finding is
given a value, and the total score is matched to a gestational age
The maximum score on the Ballard tool is 50, which corresponds to a
gestational age of 44 weeks
11/07/1432 Miss: kamlah Olaimat
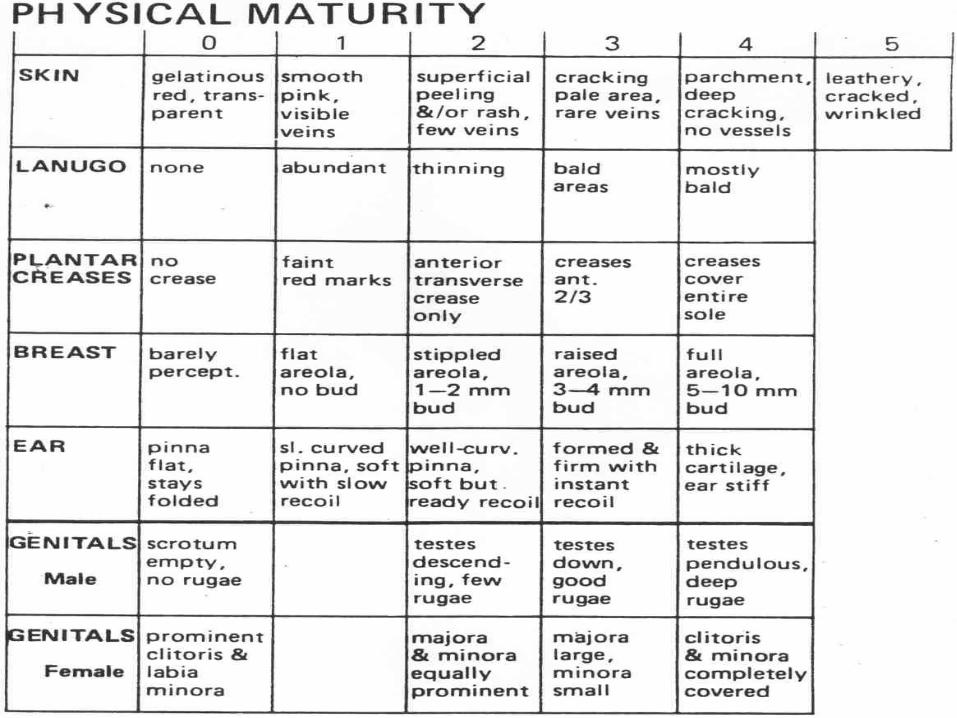
Assessment of Physical Maturity
Characteristics
• Resting posture
Flexion of the thigh & extension of the upper
extremities ( score1or 2)-GA 31wk
Stronger flexion of the arm, hips and thigh (
score 3-GA 35 wk
Hypertonic flexion of all extremities ( score 4
11/07/1432 Miss: kamlah Olaimat
Assessment of Physical Maturity
Characteristics-Cont.
• Plantar Surface-Sole creases
Few sole creases on the anterior portion of the
foot (score 2-GA 35 wk)
Deeper sole creases on the anterior 2/3 of the
sole ( score 3-GA 37 wk)
Deep sole creases down to include the heel (
score 4).

11/07/1432 Miss: kamlah Olaimat
Assessment of Physical Maturity
Characteristics-Cont.
• Breast tissueGently compress the tissue between the middle and
index fingers and measure the tissue in cm or mm
Visible raised area of ,75 cm diameter ( score 3- GA
38 wk)
10mm breast tissue area ( score 4- GA 40-44 wk
Absence of or decreased breast tissue indicate
premature or SGA.

11/07/1432 Miss: kamlah Olaimat
Assessment of Physical Maturity
Characteristics-Cont.
• Ear form & cartilage
Incurving of the upper 2/3 of the pinna ( score 2- GA 36 wk)
Well-defined incurving of the entire pinna ( score 3)
If the auricle stays in the position in which it is pressed or returns slowly to its original position-≤ 38 wk
11/07/1432 Miss: kamlah Olaimat
Estimation of Gestational Age ()
PHYSICAL CHARACTERISTICS:• Resting posture: assessed undisturbed on a flat surface• Skin: thin, opaque, peeling• Lanugo: decreases as gestational age increases• Sole (plantar) creases: increase with gestational age• Areola and breast bud tissue: increases with age.• Ear form and cartilage distribution: Cartilage gives shape.
Pinna is firm at term.• Male genitals: Size of scrotal sac, the presence of rugae, and
descent of the testicles.• Female genitals: size of labia majora and minora.• Vernix: None in the post term infant. More seen with
prematurity.• Hair: Preterm patchy, term silky.• Skull firmness: increases as the fetus matures.• Nails: long may be a sign of postmaturity.
11/07/1432 Miss: kamlah Olaimat

11/07/1432 Miss: kamlah Olaimat
NEW BALLARD SCORE
SCORE WEEKS
-10 20
-5 22
0 24
5 26
10 28
15 30
20 32
28 34
30 36
38 38
40 40
48 42
50 44
PRETERM
TERM
POSTTERM

11/07/1432 Miss: kamlah Olaimat
NEUROMUSCULAR MATURITY
• Square window-bend wrist so palm is as flat against the arm as possible
– 90 degrees (32 wks or less) –score of 0
– If angle greater than 90 degrees-score is 1
• Arm recoil-arms held with elbows flexed then pulled straight down to sides and released.
– Rapid recoil-score of 4
– Preterm0no recoil-score of 0
• Popliteal angle-thigh flexed to abdomen, hips remain flat on table, lower leg is straightened until resistance met
– If can be fully extended-score is 1
– If angle is less than 90 degrees (measured angle behind knee) score of 5
11/07/1432 Miss: kamlah Olaimat
NEUROMUSCULAR MATURITY
• Scarf sign-arm drawn across body toward other shoulder until resistance is met (measurement of elbow placement to midline)
– If elbow did not reach midline-score of 4
– If elbow goes past midline-score of -1
• Heel to ear-hips on table, foot is moved toward the ear on same side until resistance met
– Foot position relative to knee extension is noted
– Pre-term infant’s leg will remain straight & the foot will be near the ear
– Closer to term more resistance will be felt and more flexion will be noted

11/07/1432 Miss: kamlah Olaimat
Square window Popliteal angle
Scarf sign Heel to ear-hips
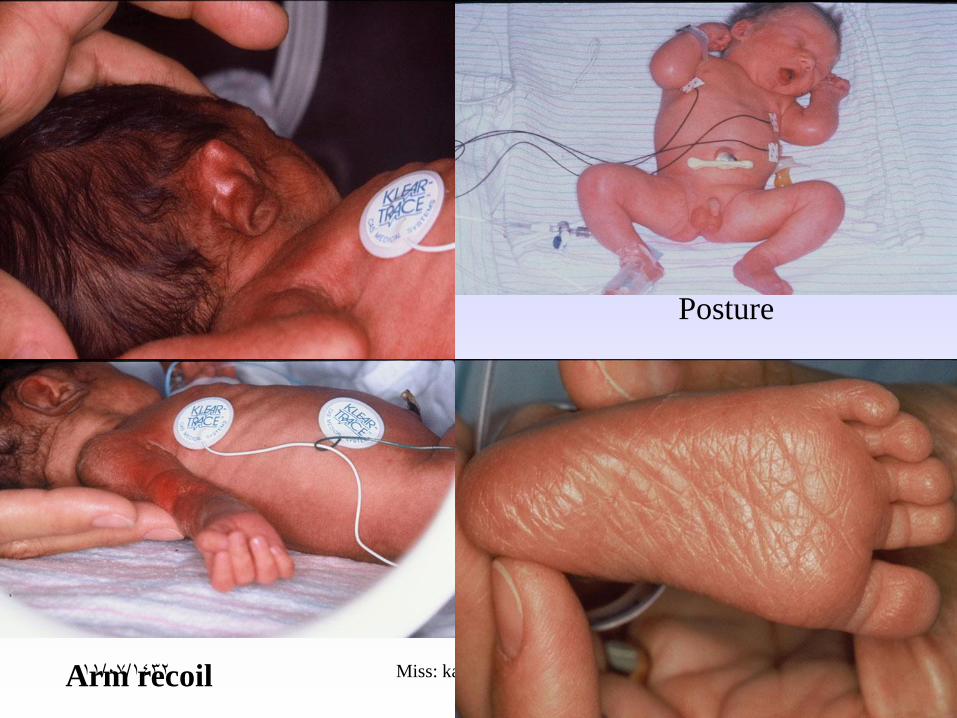
11/07/1432 Miss: kamlah OlaimatArm recoil
Posture

11/07/1432 Miss: kamlah Olaimat

11/07/1432 Miss: kamlah Olaimat
ESTIMATION OF GESTATIONAL
AGENBS - continued SCORING SYSTEM
-10 20 wks 25 34 wks
-5 22 wks 30 36 wks
0 24 wks 35 38 wks
5 26 wks 40 40 wks
10 28 wks 45 42 wks
15 30 wks 50 44 wks
20 32 wks

11/07/1432 Miss: kamlah Olaimat
Case Study
• A nurse has completed the gestational assessment on a
newborn who weighs 3000 g, is 48 cm long, with a head
circumference of 33 cm. His APGAR scores were 8 at one
minute and 9 at five minutes. Other assessment data
include skin dry and cracking, no lanugo, sole creases
covering the whole heel, areola 3 mm, pinna soft with slow
recoil, testes descended with moderate rugae. Reflex data
include square window at 0°; arm recoil 100°; popliteal
angle 100°; scarf sign yield elbow at midline; heel to ear
90°; and posture fully flexed. The parents express concerns
over his small size.
11/07/1432 Miss: kamlah Olaimat
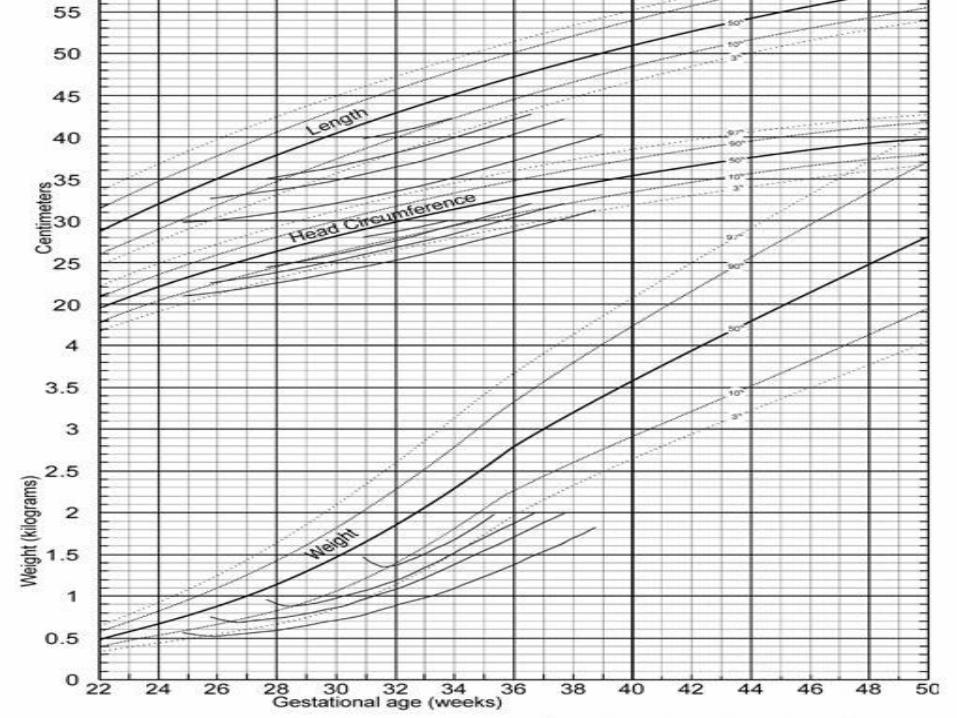
Gestational Age Relationship to Intrauterine Growth
• Growth curves show measures of intrauterine growth in
percentiles for each week of gestation.
• Birth weight is classified as follows:
• Large for gestational age (LGA): weight falls above the
90th percentile for gestational age
• Appropriate for gestational age (AGA): weight falls
between the 90th and 10th percentile for gestational age
• Small for gestational age (SGA): weight falls below the
10th percentile for gestational age
11/07/1432 Miss: kamlah Olaimat
11/07/1432 Miss: kamlah Olaimat 25
Blink reflex:
Used to protect the eye, newborn close his lids when any near object come close to his eye. Elicited by flashing strong light in the newborn’s eye.
Rooting reflex:
Used to help newborn find the food. When brushing the cheek near to the corner of the mouth, the newborn will turn to that direction, it disappear at 6 weeks of life.
11/07/1432 Miss: kamlah Olaimat 26
Swallowing, gag, cough and sneeze reflex: Swallowing occur automatically when food reaches
the posterior portion of the tongue.
Extrusion reflex: Used to protect the newborn from swallowing objects. he extrude any object that is placed in the anterior portion of the tongue. It disappears in the forth month.
Sucking reflex:
Newborn suck when his lips is touch, disappear in 6 months. If never stimulated, it disappears (such as newborn with trachoesophegial shunt, in which food is not allowed to be given by mouth), so newborn is given pacifier to keep this reflex.

11/07/1432 Miss: kamlah Olaimat 27
palmer grasp:
Newborn grasp objects placed in their palm by closing their fingers on it. Disappears by the third month.
Step in place (dancing) or walk in place:
Newborn who are held in vertical position with their feet touching a hard surface, will take a few quick alternating steps. Disappear by the third month.
11/07/1432 Miss: kamlah Olaimat 28
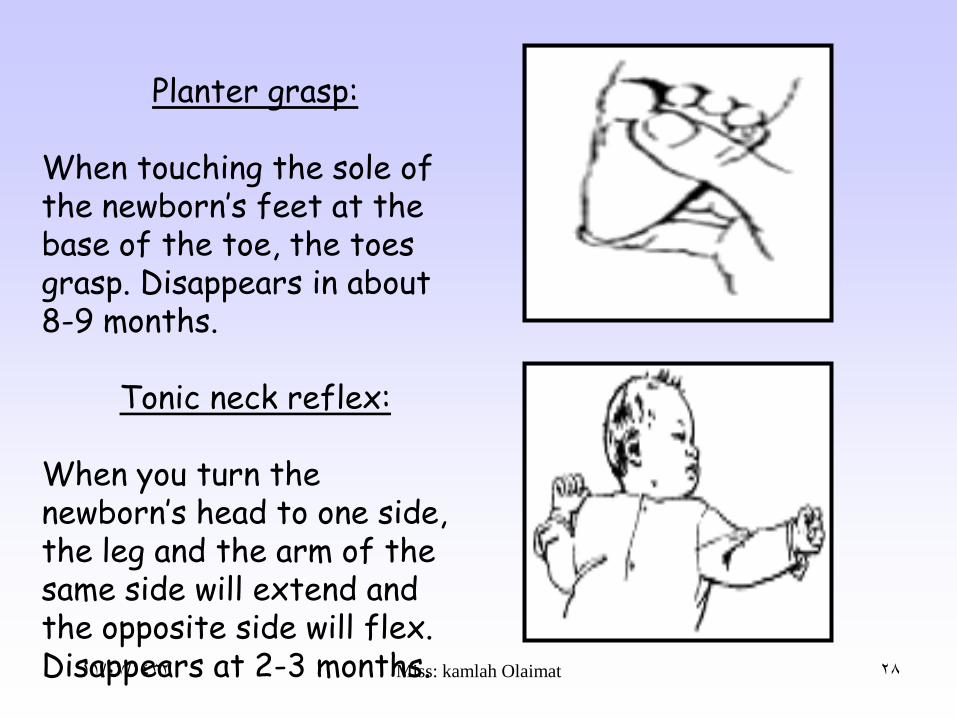
Planter grasp:
When touching the sole of the newborn’s feet at the base of the toe, the toes grasp. Disappears in about 8-9 months.
Tonic neck reflex:
When you turn the newborn’s head to one side, the leg and the arm of the same side will extend and the opposite side will flex. Disappears at 2-3 months.
11/07/1432 Miss: kamlah Olaimat 29
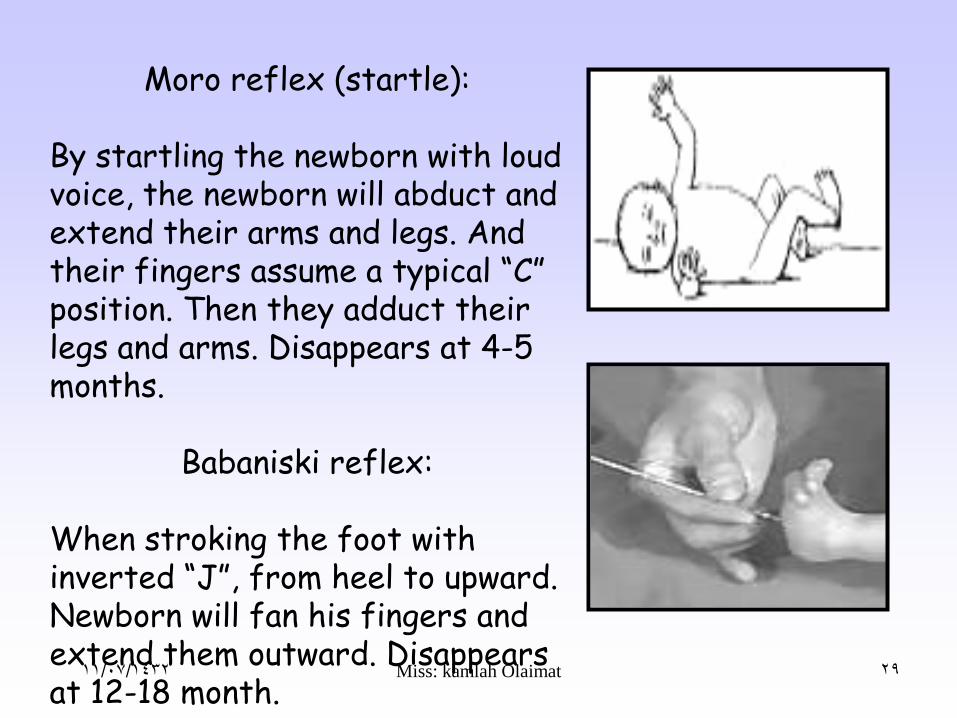
Moro reflex (startle):
By startling the newborn with loud voice, the newborn will abduct and extend their arms and legs. And their fingers assume a typical “C” position. Then they adduct their legs and arms. Disappears at 4-5 months.
Babaniski reflex:
When stroking the foot with inverted “J”, from heel to upward. Newborn will fan his fingers and extend them outward. Disappears at 12-18 month.

11/07/1432 Miss: kamlah Olaimat 30
Crossed extension:
If one leg is irritated at sole while supine and legs are extended, the newborn will raise the other leg and cross it to the first leg.
Trunk incurvation:
When newborn is on prone position, and touched on one side, he will flex and swing their pelvis toward the touch.
11/07/1432 Miss: kamlah Olaimat 31
1- Hearing:
Fetus hear in uterus before birth, and as they born they hear from near distance. As evidence: they calm in respond to soothing voice and startle at loud voice.
2- Vision:
Newborn see when they born, but they focus on white & black objects at distance of 9-12 inches.
3- Taste:
Newborn prefer sweet taste of milk or glucose water.
4- Smell:
They can smell after clearness of nose from mucus & amniotic fluid.

11/07/1432 Miss: kamlah Olaimat 32
Time Description
First period 15-30 min Reactive period
Looks cyanosis.
Rapid pulse.
Rapid respiration.
alert.
Second period 30-120 min Resting period
Newborn is sleeping.
V/S stabilized.
Color stabilized.
Third period 2-6 hrs Second reactive period
Alert.
Color & V/S signs change with activity.

11/07/1432 Miss: kamlah Olaimat 33
1- baby is no longer under the influence of the maternal hormones.
2- diuresis occur (increase in second to third day of life).
3- newborn pass stool.
4- Limited intake (especially B.F baby). In which milk is low caloric.
Newborn lose 5%-10% of weight during the first 10 days of life, because:
Weight
After loss:
In first day WT is stable. The next 7 days is needed to regain WT for formula feed babies. and 10 days is needed to regain WT for breastfeed babies.

11/07/1432 Miss: kamlah OlaimatWeight 2.5 to 4 kg 34
Length The average length after birth for girls: 53 cm. The average length after birth for boys: 54 cm.
Head Circumference:
From 34-35 cm at birth, not < 33 or > 37.
Chest Circumference
From 32-33 cm at birth. It is less than the head with two cm until age of two years.

11/07/1432 Miss: kamlah Olaimat

11/07/1432 Miss: kamlah Olaimat
Vital Signs• Temperature- first is usually taken axillary,
but may be taken rectally to assure anal patency (36.5-37.5 c° )
– Crying may elevate temperature
– Stabilizes in 8 to 10 hours after delivery
• Axillary vs Rectal about 0.2 to 0.5 difference
• Pulse- 120-160 bpm, unless sleeping (100) or crying (180)
– Apical pulse for one minute
– Color pink with acrocyanosis
– Heart rate may be irregular with crying
• Respirations- 30-60 with periodic breathing
• B/P- only if suspected heart problem or premature infant
– Ranges between 60-80 mm systolic and 40-45 mm diastolic.
11/07/1432 Miss: kamlah Olaimat 37
Newborn lose heat by four mechanisms:
1- convection: heat flow from newborn to cooler air. 2- radiation: transfer heat from body to cold solid object not in contact with the body. 3- evaporation: conversion of liquid to vapor. 4- conduction: transfer heat from body to cold solid object in contact with the body.
Insulation is not efficient because little fat available.** How newborn conserve heat?From the brown fat that available in the
intrascapular, thorax and perineal area. It found in the mature newborn and produce heat by increasing metabolism.
Temperature

11/07/1432 Miss: kamlah Olaimat 38
Conduction
Evaporation
Convection
Radiation
11/07/1432 Miss: kamlah Olaimat
Temperature Assessment
• For neonates and infants, axillary temperatures closely correlate with rectal temperatures and are safer for the infant.
• Axillary temperature, on average, is 0.4 C less than rectal temperature (Kenner, 2003).
• At birth, the neonate’s temperature may decrease at a rate of 0.2 C to 1.0 C per minute, mainly through convective and evaporative heat loss.
• Norms (AAP & ACOG, 2007):
– Rectal or auxiliary temperature of 36.5 C to 37.5 C
– Skin temperature of 36 C to 36.5 C
11/07/1432 Miss: kamlah Olaimat
Heat ProductionThe human body responds to cold in three
ways:
1. Voluntary muscular activity (vasoconstriction and increased movement)
2. Shivering (inefficient in the term newborn)
3. Chemical or nonshivering thermogenesis (brown-fat metabolism for several hours after birth)

11/07/1432 Miss: kamlah Olaimat
Heat Dissipation• Infants respond to overheating by
vasodilation in the skin, which increases heat loss from the blood.
• In the first week of life, immaturity of the skin causes the largest amount of heat loss through evaporation.
• The newborn’s head represents 21 percent of the total body surface area and accounts for a significant proportion of total heat loss (Blackburn, 2007).
11/07/1432 Miss: kamlah Olaimat
Weight and Measurements
• Weight: 2500-4000gms
Wt loss 5%-10% for term newborn, 15% for preterm
Growth 198-200g / wk for the 1st 6 months
• Length: 50cm ( 46-56cm, 2.5 cm/month for 1st 6 months
• Head circumference: 32-37 cm, 2cm larger than chest ((measure right above eyebrows)
• Chest circumference: 32cm (30-35 cm) (measure at nipple line)
11/07/1432 Miss: kamlah Olaimat
Physical Examination
• skin
– Pink is normal
– Acro cyanosis is normal
– Cyanosis
– Jaunduce
• 1st 24 hours
– Pale and grayish color in anemia and acidosis
respectively
– Common skin rash
• Erythema toxicum, mongolian spot,

11/07/1432 Miss: kamlah Olaimat
Clinical assessment
Skin: some common normal findings• Vernix caseosa: a cream/white cheesy material on the skin at
birth which cleans off easily with oil.
• Lanugo; fine downy hairs seen on the back and shoulders especially in preterm infants.
• Milia: pinpoint whitish papules on nose and cheeks due to blocked sebaceous glands.
• Mongolian blue spots: grey/bluish pigment patches seen in the lumbar area, buttocks and extremities in dark skinned babies.They usually disappear by one year.
• Capillary heamangiomas (“stork bite” naevi): red flat patches which blanch with gentle pressure. Commonly occur on upper eyelids, forehead and nape of the neck.
• Erythema toxicum: small white/yellow papules or pustules on a red base seen on face, trunk and limbs. Develop 1 – 3 days after birth and usually disappear by one week.

11/07/1432 Miss: kamlah Olaimat
Erythema toxicum, acrocyanosis, milia and
mongolian spots

11/07/1432 Miss: kamlah Olaimat
Clinical assessment
HeadAfter these general observations, examine the infant
starting with the head and moving down the body.
• Observe the size and shape of the head (micro- or macrocephaly; cephalhaematoma)
• Check the anterior and posterior fontanelles and that the skull sutures feel normal
• Form and position of ears (low set ears occur in chromosomal abnormalities, e.g. Down syndrome)
• Molding is shaping of fetal head to adapt to the mothers pelvis during labor (suture lines overlap and head elongates)

11/07/1432 Miss: kamlah Olaimat 47
Anterior Fontanel:
At the junction of two parietal & frontal bones.
Diamond in shape, 2-3 cm in width & 3-4 cm in length.
Close at 12-18 months.
Posterior fontanel:
At the junction of two parietal & the occipital bones.
Triangular shape, 1 cm in length.
Close at 2-3 months.

11/07/1432 Miss: kamlah Olaimat
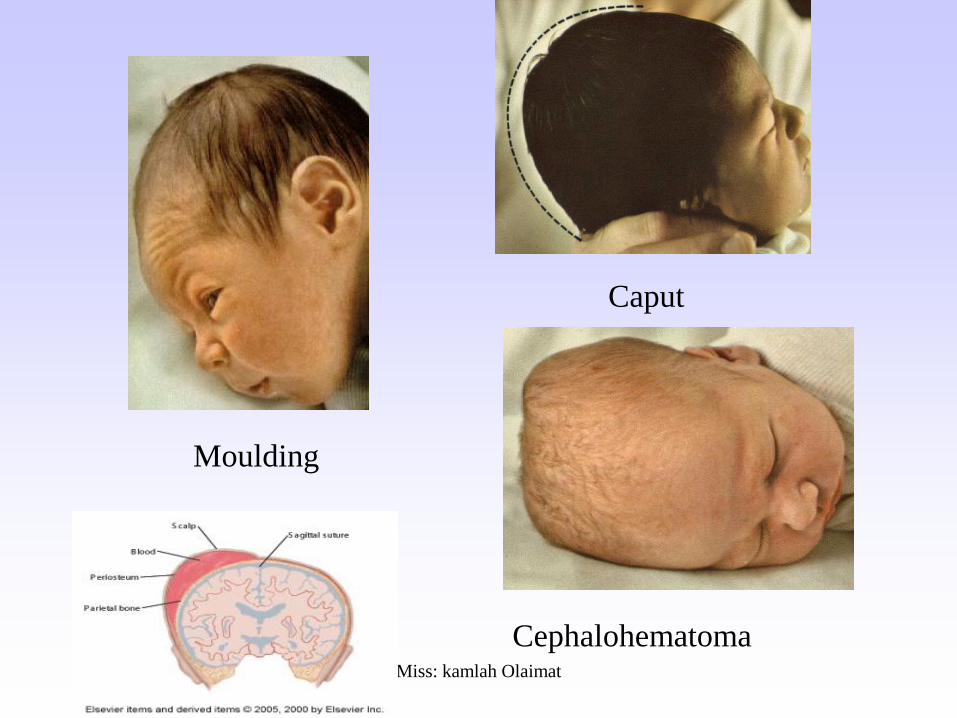
COMPARISON OF
CEPHALHEMATOMA AND CAPUT
SUCCEDANEUM
• CEPHALHEMATOMA –is a collection of blood resulting
from ruptures blood vessels between the surface of a cranial
bone and the periosteal membrane. They may be bilateral or
unilateral and do not cross the suture lines
• CAPUT SUCCEDANEUM
is a localized, easily identifiable, soft area of the scalp,
generally resulting from a long and difficult labor or vacuum
extraction.
11/07/1432 Miss: kamlah Olaimat
Moulding
Caput
Cephalohematoma

11/07/1432 Miss: kamlah Olaimat
• Facial Symmetry
• Eyes- shape, slanted,
hemorrhages,
edema, strabismus
Asymmetry
Slanted eyeshemorrhages
Strabismus

11/07/1432 Miss: kamlah Olaimat
•Nose- patency of
each nares to r/o
“Choanal Atresia”

11/07/1432 Miss: kamlah Olaimat
• Mouth- for cleft lip and palate, for
neonatal teeth, Thrush
Cleft lipCleft palate Thrush
Neonatal teeth

11/07/1432 Miss: kamlah Olaimat
•Ears-
•normal shape
•patent
•even with eyes (low set ears indicate
congenital abnormalities)
•Pits or tags

11/07/1432 Miss: kamlah Olaimat
• Neck and Clavicles- is the neck thick or webbed, do the clavicles feel intact, no crepitus.
11/07/1432 Miss: kamlah Olaimat
Clinical assessment
Cardiovascular and respiratory• Feel femoral and radial pulses for volume, rate and rhythm.
• In aortic coarctation, femoral pulse is reduced, absent or not synchronous with radial pulse.
• If child is sick, measure blood pressure.
• Locate the apex beat and listen to the heart sounds for murmurs.
• Count the respiratory rate
– normal 30 – 40 breaths/min in term infants
– faster in preterms.
– > 60 / minute abnormal
• Observe for respiratory distress: nasal flaring, intercostal and subcostal recession.

11/07/1432 Miss: kamlah Olaimat
Chest
- Size- 2” smaller than head
- Shape- cylinder shape is normal. Asymmetry can be caused by Pneumothorax or Diaphragmatic Hernia
- Nipples- location, distance apart, any accessory nipples
11/07/1432 Miss: kamlah Olaimat
Lung Sounds
- clear or moist, equal, sounds in
chest?
- S/S of respiratory distress
- (tachypnea, grunting, retractions,
nasal flaring, cyanosis)
- Rate (listen for 1 full minute)

11/07/1432 Miss: kamlah Olaimat
Factors that initiate Respirations
• 1) Chemical Factors- in O2 and in CO2
causes impulses to stimulate the respiratory
center in the medulla of the brain.
• 2) Thermal Factors- abrupt temperature
change sends impulses to brain
• 3) Mechanical Factors- fetal chest is
compressed during birth, forcing fluid out.
• 4) Factors that maintain respirations-
surfactant, functional residual capacity

11/07/1432 Miss: kamlah Olaimat
Heart Sounds• - Auscultate for rate & rhythm
• - presence of murmurs (murmurs are common in the newborn period- 90% are transient and considered normal)
• Listen for 1 full minute
• Report any abnormal rate, rhythms or sounds to pediatrician
• If suspected heart problem- take B/P on all four extremities

11/07/1432 Miss: kamlah Olaimat
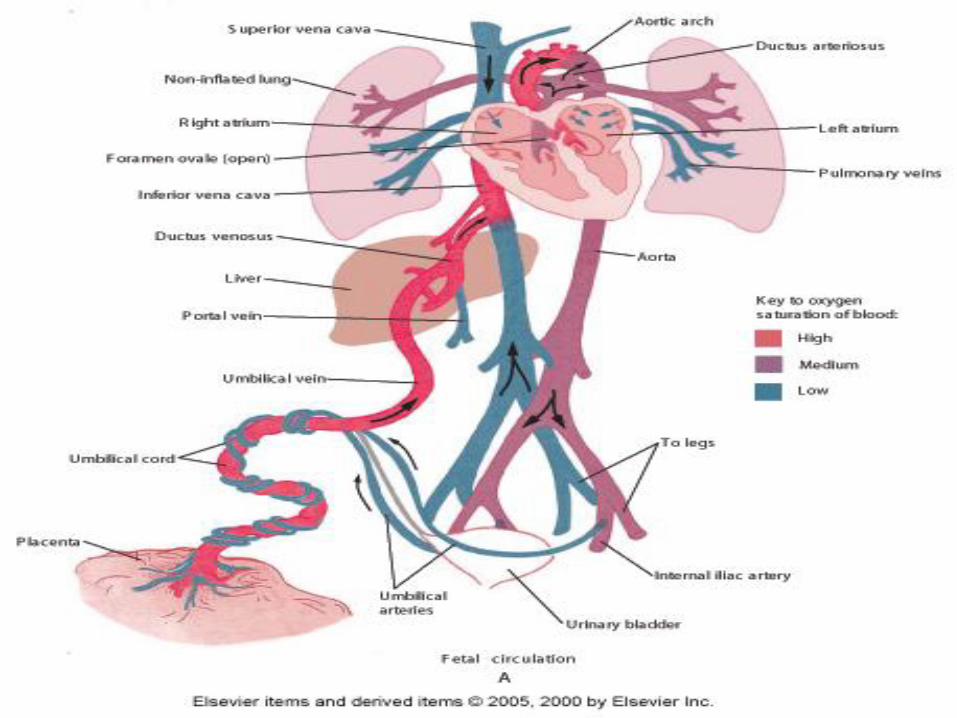
Cardiovascular Adaptation: Transition from
fetal to neonatal circulation
• What is fetal circulation?
• A combination of structures/vessels that are present only during the fetal period, which help shunt the highest oxygenated blood to the head, brain and heart.
• 1) Ductus Arteriosus
• 2) Foramen Ovale
• 3) Ductus Venosus
11/07/1432 Miss: kamlah Olaimat

11/07/1432 Miss: kamlah Olaimat
At birth, after the first few breaths, the
following cardiovascular changes occur:
• 1) Ductus Arteriosus closes in response to O2 and resistance in lungs
• 2) Pulmonary blood vessels dilate in response to demand in lungs
• 3) Foramen Ovale is forced to close because of increased pressure in left side of heart
• 4) Ductus Venosis constricts when umbilical cord is clamped

11/07/1432 Miss: kamlah Olaimat
Abdomen• Inspection
Size- smaller than chest, Shape- rounded, no distention
– Scaphoid
– Distention
– Abdominal wall defect (gastroschisis, Omphalocele)
• Palpation; baby sucking and use warm hands
– Kidneys are normaly palpable
– Liver 2-3 cm
– Spleen palpable
– Bowel sounds- present, hypo, hyper
- Cord- color, # of vessels, clamp on tight (no skin attached), no
bleeding noted
– Hernias ; umbilical and inguinal

11/07/1432 Miss: kamlah Olaimat 64
Intestines is sterile in newborn, it cultured by normal flora in 5-24 hours. ** Stool: First stool: is called meoconium, it is black to green in color, odorless, sticky. 2nd -3rd day: called transitional stool, green in color, loose (like diarrhea).
4th day:
In breastfeed babies: In formula feed babies:
Light yellow with sweat smelling (high in lactic acid). 3-4 times/ day.
Bright yellow, with odor. 2-3 times/day.

11/07/1432 Miss: kamlah Olaimat
Clinical assessment
Spine and genitaliaExamine:
• The spine for dimples, tuft of hair (spina bifida occulta) or cystic swellings (spina bifida cystica)
• Remove the diaper to examine the genitalia. In boys, confirm that both testicles have descended into the scrotum.
• Designate the infant’s sex
• Inspect the perineum and check anus for position and patency (can be done by gently checking rectal temperature)

11/07/1432 Miss: kamlah Olaimat
Genitalia:
- Female- labia may be swollen and red from delivery, hymenal tag, pseudomenses, whitish drainage
- Male- testes should be descended at term, rugae on scrotum, check where urinary meatus comes out
- Hypospadias- urethral opening is on the underside
- Epispadias- urethral opening is on the upperside
-

11/07/1432 Miss: kamlah Olaimat 67
The average first void id within the first 24 hours of life. It is light-colored and odorless. The first void is about 15 ml. The daily urine out put: in first 1-2 days: 30-60ml. By the end of the first week: the total output is about 300ml.
When child perform the following activities, his nervous system consider normal:
Moving extremities. Attempting to control movement. Cry strongly.Demonstrate reflexes

11/07/1432 Miss: kamlah Olaimat
Extremities
• Arms & Hands
• Symmetry
• 10 fingers
• Brachial pulse
• Erb’s palsy: extended arm and internal rotation with limited movement
• Humerous fracture
• Single palmar crease
• Hip dislocation– Female, breach

11/07/1432 Miss: kamlah Olaimat

11/07/1432 Miss: kamlah Olaimat

11/07/1432 Miss: kamlah Olaimat
Polydactly
Syndactyly
Simian Crease

11/07/1432 Miss: kamlah Olaimat
Any problems identified during the initial assessment will need specific management. However, newborn infants are a highly susceptible group and high-quality routine care prevents a multitude of problems. The major elements of routine care include:
• Cord care
• Thermal control
• 24 hour rooming in
• Feeding
• Immunization
• Maternal education on hygiene and every other aspect of routine care
Routine care of the well newborn
Hand washing with soap and water every time a baby is
handled goes a long way in reducing the risk of infection!

11/07/1432 Miss: kamlah Olaimat
• 5) Bathing-
• *remember Thermoregulation
• Good time to observe for any missed abnormalities
• Sponge bath until cord falls off
• 6) Cord care-
• Alcohol, Betadine,
• Teach parents how to care for cord and when to expect it to fall off

11/07/1432 Miss: kamlah Olaimat
• 7) Protection of Infant-Security, ID badges, observation of any suspicious looking people
• 8) Teaching Parents
• NB Care
• Feeding
• When to call the Doctor
• Lab tests
• Hearing Screen

11/07/1432 Miss: kamlah Olaimat
Nursing Care Management of the
Newborn
Nursing Diagnosis
• Risk for ineffective breathing pattern
• Altered nutrition: less than body requirements
• Altered urinary elimination
• Risk for infection
• Knowledge deficit
• Altered family processes

11/07/1432 Miss: kamlah Olaimat
Nursing Plan and Implementation
• Maintenance of cardiopulmonary function
• Maintenance of a neutral thermal environment
• Promotion of adequate hydration and nutrition
• Promotion of skin integrity
• Prevention of complications and preventing safety
• Enhancing parent-newborn attachment
11/07/1432 Miss: kamlah Olaimat
Maintenance of Cardiopulmonary
Function
• Assess vital signs every 6 to 8 hrs or more depending on the newborn’s status.
• “Back to Sleep” , side lying to prevent aspiration and facilitate drainage of mucus.
• Keep bulb syringe readily available.
• Vigorous fingertip stroking of the spine frequently stimulates respiratory activity.
• Cardiac/respiratory monitor may be required.
• At-risk indicators: pallor, cyanosis, ruddy color, and apnea.

11/07/1432 Miss: kamlah Olaimat
Promotion of Adequate Hydration and
Nutrition
• Weigh at the same time each day.
• Weight loss of up to 10% is considered normal during the first week of life.
• Birth weight should be regained by the 2nd week of life.
• The nurse records voiding and stooling patterns.
• The first void should occur within the first 24 hours and passage of stool in the first 48 hours.
• Assess for abdominal distention, bowel sounds, hydration, fluid intake, voiding pattern, and temperature stability.
• Excessive handling may cause an increase in the newborn’s metabolic rate, calorie use and fatigue.
11/07/1432 Miss: kamlah Olaimat
Promotion of Skin Integrity
• Bathing is important for health, appearance, and infection control in the nursery.
• Ongoing skin care includes cleansing of the buttocks and perineal area with water and a mild soap with diaper changes.
• Assess the umbilical cord for signs of bleeding or infection: 1) apply triple dye on admission to nursery and 2) alcohol after each diaper change.
• Cord care with each diaper change.
• Eye and skin care related to phototherapy.
• Skin care following circumcision.

11/07/1432 Miss: kamlah Olaimat
Prevention of Complications and
Promoting Safety
• Pallor may be an early sign of hemorrhage.• Circumcision is assessed for signs of hemorrhage and
infection.• Initial scrub for 2-3 minutes when direct contact with the
newborn is anticipated.• Handwashing between each client contact and contact with
floor, face, or any soiled surface.• Encourage parents to wash hands prior to holding the infant
and wear a gown over street clothes.• Teach parents to limit visitors who may have a communicable
disease.• Check namebands with each encounter with the parents.• Instruct clients in security measures in place to prevent infant
abduction.

11/07/1432 Miss: kamlah Olaimat
Enhancing Parent-Newborn
Attachment
• Involve the entire family in newborn care
• Infant massage may be encouraged
• Increase skin to skin contact
• Read to or play music for the newborn
• Encourage cuddling and talking to the infant

11/07/1432 Miss: kamlah Olaimat
Discharge Planning and Preparation
• Parent teaching
• General instructions for newborn care
• Nasal and oral suctioning
• Wrapping the newborn
• Sleep and activity
• Safety considerations
• Newborn screening and immunization Program
11/07/1432 Miss: kamlah Olaimat
Please take good care of me!
Ref:
1. Ladewig, P., London,M., &
Davidson,M. ( 2010)
Contemporary Maternal-
Newborn Nursing Care, 7th
ed.,Pearson Education Ltd.,
London.
2. Classes.kumc.edu/son/nurs350/a
ssessment_findings_for_bj.htm