Enli2014
6
Correspondence: Yas ¸ar Enli, MD, Department of Medical Biochemistry, Faculty of Medicine, Pamukkale University, Kinikli Kampusu, Morfoloji Binasi, 20070, Denizli, Turkey. Tel: 90 532 7914727. Fax: 90 258 2961765. E-mail: [email protected] (Received 12 August 2013; accepted 12 January 2014) ORIGINAL ARTICLE Adipocytokine concentrations in children with different types of beta-thalassemia YAS ¸ AR ENL 1 , YASEM N I. BALCI 2 , CAFER GÖNEN 1 , EBRU UZUN 2 & AZ Z POLAT 2 Departments of 1 Medical Biochemistry and 2 Pediatric Haematology , Pamukkale University , Faculty of Medicine, Denizli, Turkey Abstract Background. Beta-thalassemia is an inherited blood disorder. It results from the impaired production of β-globin chains, leading to a relative excess of alpha-globin chains. Clinical severity separates this disease into three main subtypes: β- thalassemia major, β-thalassemia intermedia and β-thalassemia minor, the former two being clinically more significant. Inflammatory processes may play an important role in some of the complications of thalassemia. Adipose tissue is one of the most important endocrine and secretory organs that release adipocytokines like adiponectin, resistin and visfatin. Aim. The aim of our study was to analyze adipocytokine concentrations (adiponectin, resistin and visfatin) in different types of β-thalassemia patients and determine any possible correlations with disease severity. Methods. We recruited 29 patients who were transfusion-dependent β-thalassemia-major patients, 17 patients with β-thalassemia intermedia, 30 β-thalassemia minor patients. The control group consisted of 30 healthy children. Anthropometric measurements, complete blood count, biochemical parameters, serum concentrations of adiponectin, resistin, visfatin were performed for all subjects. Results. Resistin and visfatin concentrations were significantly higher in β-thalassemia minor patients than in controls. Adiponectin, resistin and visfatin concentrations were significantly higher in both β-thalassemia intermedia and major patients than in controls. The concentrations of adiponectin, resistin and visfatin were significantly higher in both β-thalassemia inter- media and major patients than in β-thalassemia minor patients. There was no significant difference between β-thalassemia intermedia and β-thalassemia major patients for adipocytokines concentrations. Conclusion. We speculate that these adipocytokines may play a role in the development of complications in β-thalassaemia. Key Words: Beta-thalassemia, adipocytokine, adiponectin, resistin, visfatin Introduction Beta-thalassemias are a group of of hereditary blood disorders characterized by impaired production of the beta-globin chains of hemoglobin resulting in variable phenotypes ranging from severe anemia to clinically asymptomatic individuals [1]. Three main forms have been described: Thalassemia Major, variably referred to as ‘Cooley’s Anemia’ and ‘Mediterranean Anemia’, Thalassemia Intermedia and Thalassemia Minor also called ‘ β-thalassemia carrier’, ‘ β-thalassemia trait’ or ‘heterozygous β- thalassemia’ [2]. Although β-thalassemia is a hereditary haemoglo- binopathy caused by defective haemoglobin β-globin synthesis, leading to excess alpha-globin chains that cause haemolysis and impair erythropoiesis, inflamma- tion is known to play an important role in the development of complications of the disease. A chronic inflammatory state is present in β-thalassemia patients, with increased levels of inflammatory cytokines [3]. Some of these adipocytokines are adiponectin, resistin, visfatin, leptin, plasminogen activator inhib- itor type 1 (PAI-1), tumor necrosis factor α (TNF- α), IL-6 and IL-8 [4,5]. Adipocytokines are considered important players in the etiopathogenesis of numerous metabolic, vascular and inflammatory disorders [6]. Among these cytokines, much attention has been paid to adiponectin, which has significant effects on the inflammatory process [7]. Adiponectin attenu- ates inflammation, oxidative stress, and cytokine production. Resistin is a member of the resistin-like molecule family of cysteine-rich secretory 12-kDa proteins [8]. Scandinavian Journal of Clinical & Laboratory Investigation, 2014; 74: 306–311 ISSN 0036-5513 print/ISSN 1502-7686 online © 2014 Informa Healthcare DOI: 10.3109/00365513.2014.883639 Scand J Clin Lab Invest Downloaded from informahealthcare.com by University Of South Australia on 08/11/14 For personal use only.
-
Upload
hamza-yazid -
Category
Health & Medicine
-
view
108 -
download
0
Transcript of Enli2014

Correspondence: Ya s ar Enli, MD, Department of Medical Biochemistry, Faculty of Medicine, Pamukkale University, Kinikli Kampusu, Morfoloji Binasi, 20070, Denizli, Turkey. Tel: � 90 532 7914727. Fax: � 90 258 2961765. E-mail: [email protected]
(Received 12 August 2013 ; accepted 12 January 2014 )
ORIGINAL ARTICLE
Adipocytokine concentrations in children with different types of beta-thalassemia
YA S AR ENL 1 , YASEM N I. BALCI 2 , CAFER G Ö NEN 1 , EBRU UZUN 2 & AZ Z POLAT 2
Departments of 1 Medical Biochemistry and 2 Pediatric Haematology , Pamukkale University , Faculty of Medicine , Denizli , Turkey
Abstract Background . Beta-thalassemia is an inherited blood disorder. It results from the impaired production of β -globin chains, leading to a relative excess of alpha-globin chains. Clinical severity separates this disease into three main subtypes: β -thalassemia major, β -thalassemia intermedia and β -thalassemia minor, the former two being clinically more signifi cant. Infl ammatory processes may play an important role in some of the complications of thalassemia. Adipose tissue is one of the most important endocrine and secretory organs that release adipocytokines like adiponectin, resistin and visfatin. Aim . The aim of our study was to analyze adipocytokine concentrations (adiponectin, resistin and visfatin) in different types of β -thalassemia patients and determine any possible correlations with disease severity. Methods . We recruited 29 patients who were transfusion-dependent β -thalassemia-major patients, 17 patients with β -thalassemia intermedia, 30 β -thalassemia minor patients. The control group consisted of 30 healthy children. Anthropometric measurements, complete blood count, biochemical parameters, serum concentrations of adiponectin, resistin, visfatin were performed for all subjects. Results . Resistin and visfatin concentrations were signifi cantly higher in β -thalassemia minor patients than in controls. Adiponectin, resistin and visfatin concentrations were signifi cantly higher in both β -thalassemia intermedia and major patients than in controls. The concentrations of adiponectin, resistin and visfatin were signifi cantly higher in both β -thalassemia inter-media and major patients than in β -thalassemia minor patients. There was no signifi cant difference between β -thalassemia intermedia and β -thalassemia major patients for adipocytokines concentrations. Conclusion . We speculate that these adipocytokines may play a role in the development of complications in β -thalassaemia.
Key Words: Beta-thalassemia , adipocytokine , adiponectin , resistin , visfatin
Introduction
Beta-thalassemias are a group of of hereditary blood disorders characterized by impaired production of the beta-globin chains of hemoglobin resulting in variable phenotypes ranging from severe anemia to clinically asymptomatic individuals [1]. Three main forms have been described: Thalassemia Major, variably referred to as ‘ Cooley ’ s Anemia ’ and ‘ Mediterranean Anemia ’ , Thalassemia Intermedia and Thalassemia Minor also called ‘ β -thalassemia carrier ’ , ‘ β -thalassemia trait ’ or ‘ heterozygous β -thalassemia ’ [2].
Although β -thalassemia is a hereditary haemoglo-binopathy caused by defective haemoglobin β -globin synthesis, leading to excess alpha-globin chains that cause haemolysis and impair erythropoiesis, infl amma-tion is known to play an important role in the
development of complications of the disease. A chronic infl ammatory state is present in β -thalassemia patients, with increased levels of infl ammatory cytokines [3].
Some of these adipocytokines are adiponectin, resistin, visfatin, leptin, plasminogen activator inhib-itor type 1 (PAI-1), tumor necrosis factor α (TNF- α ), IL-6 and IL-8 [4,5].
Adipocytokines are considered important players in the etiopathogenesis of numerous metabolic, vascular and infl ammatory disorders [6].
Among these cytokines, much attention has been paid to adiponectin, which has signifi cant effects on the infl ammatory process [7]. Adiponectin attenu-ates infl ammation, oxidative stress, and cytokine production.
Resistin is a member of the resistin-like molecule family of cysteine-rich secretory 12-kDa proteins [8].
Scandinavian Journal of Clinical & Laboratory Investigation, 2014; 74: 306–311
ISSN 0036-5513 print/ISSN 1502-7686 online © 2014 Informa HealthcareDOI: 10.3109/00365513.2014.883639
Scan
d J
Clin
Lab
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Sout
h A
ustr
alia
on
08/1
1/14
For
pers
onal
use
onl
y.

Adipocytokines in b -thalassemia 307
Recent studies have shown the causative association between resistin and systemic infl ammation [9,10], especially in the vascular endothelium [11].
Visfatin (PBEF), a recently discovered 52-kDa adipocytokine, is preferentially produced in and secreted from visceral adipose tissue, which is strongly associated with the metabolic syndrome [12]. Visfatin can be considered a new proinfl ammatory adipocytokine [13]. It can induce proinfl ammatory cytokines such as IL-1, TNF, and IL-6 [14].
The role of adipocytokines in the infl ammation process in β -thalassemia has been investigated in literature. But, there is no study about these adipo-cytokines in different types of β -thalassemia.
The aim of our study was to analyze adipocytok-ines, which are adiponectin, resistin and visfatin, concentrations in different types of Turkish β -thalassemia patients and determine any possible correlations with disease severity.
Materials and methods
A total of 76 patients and 30 healthy subjects were included in our study. We recruited 29 patients who were transfusion-dependent β -thalassemia patients (thalassemia major), 17 patients with β -thalassemia intermedia and 30 β -thalassemia minor patients. The diagnosis of β -thalassemias had been made by CBC (complete blood count), peripheral blood smear, physical examination fi ndings and hemoglobin elec-trophoresis. The control group consisted of 30 healthy children.
Patients with any other infl ammatory, infectious, chronic or hereditary diseases were excluded. Also, patients on medications other than iron chelators and splenectomized patients were excluded in our study. All of the β -thalassemia major patients were using the iron chelator (deferasirox, 10 – 30 mg/kg/day).
The study was approved by the Pamukkale Uni-versity Ethics Committee. Informed consent form was taken from the parents.
Body mass indexes (BMI) were calculated by dividing the weight in kilograms by the square of the height in metres. Full history and thorough clinical examination, anthropometric measurements, com-plete blood count, biochemical parameters, serum concentrations of adiponectin, resistin, visfatin using enzyme linked immuno sorbant assay (ELISA) were performed for all subjects.
Blood samples were collected from β -thalassemia major patients just before a scheduled transfusion and after an overnight fast of 10 – 12 h. From all other patients and healthy children, blood samples were obtained after an overnight fast of 10 – 12 h.
Serum obtained from blood was separated after centrifugation for 15 min at 3,000 rpm at 4 ° C, separated into aliquots and immediately stored at � 70 ° C until assayed.
Red blood cell indices (complete blood count) were measured using a routine automated method (Siemens ADVIA ® 2120i System, Siemens Health-care Diagnostics, Japan). Serum ferritin concentra-tions were measured with Roche Cobas 6000 autoanalyser (Roche-Hitachi Diagnostics, Japan) by using electrochemiluminescence method.
Enzyme immunoassay for adipocytokines were assayed by enzyme-linked immunosorbent assay (ELISA) kits according to the manufacturer ’ s recommended procedure. Serum concentrations of adiponectin (sensitivity: 0.06 μ g/L; linearity: 1.56 – 100 μ g/L) and resistin (sensitivity: 3 ng/L; linearity: 78 – 5000 ng/L) were determined by ELISA kits (Boster Immunoleader, China) and visfatin (sensitiv-ity: 1.85 μ g/L; linearity: 2.3 – 40 μ g/L) by ELISA kits (Phoenix, USA). These adipocytokines were measured in duplicate. Serum concentrations of adiponectin and visfatin were measured in μ g/L, serum resistin concentrations were measured in ng/L.
Statistical analysis
Since many variables had a non-Gaussian distribu-tion with signifi cant skewness, statistical analysis was performed with non-parametric tests: Kruskal-Walis and Mann-Whitney U. Correlations between vari-ables were calculated with Spearman ’ s correlation coeffi cient. The data are expressed as median and 25 – 75 percentiles. Statistical signifi cance was set at p � 0.05. Data were analyzed with the SPSS (Statis-tical Package for the Social Science, version 17.0).
Results
Table I shows the demographic and laboratory char-acteristics of groups. The concentrations of haemo-globin (Hb), hematocrit (Hct), red blood cell count (RBC) were signifi cantly higher in β -thalassemia minor patients than in β -thalassemia intermedia and β -thalassemia major patients ( p � 0.001). The RBC distribution width (RDW) and ferritin concentra-tions were signifi cantly lower in β -thalassemia minor patients than in β -thalassemia intermedia and β -thalassemia major patients ( p � 0.001). The concen-trations of ferritin ( p � 0.001) were signifi cantly lower in β -thalassemia intermedia patients than in β -thalassemia major patients.
Ferritin was positively associated with adiponec-tin ( r � 0.65, p � 0.0001) and resistin ( r � 0.57, p � 0.0001) and visfatin ( r � 0.47, p � 0.0001).
Serum levels of adipocytokines
Adiponectin, resistin, and visfatin serum concentra-tions of all groups are shown in Table II.
Resistin ( p � 0.022) and visfatin ( p � 0.031) con-centrations were signifi cantly higher in β -thalassemia
Scan
d J
Clin
Lab
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Sout
h A
ustr
alia
on
08/1
1/14
For
pers
onal
use
onl
y.

308 Y. Enl i et al.
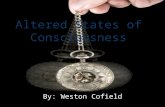
Table I. Demographic and laboratory characteristics of groups.
Control β -t * (minor) β -t (inter) β -t (major)
Age (years) 8.5 (6.0 – 11.3) 9.0 (7.0 – 14.0) 9.0 (4.5 – 15.0) 11.0 (7.0 – 15.0)Male/Female 18/12 17/13 10/7 17/12BMI (kg/m 2 ) 16.6 (15.0 – 17.4) ccc 16.8 (14.7 – 18.8) 15.6 (14.8 – 17.0) ff 18.3 (16.5 – 19.9)Hb (g/dl) 13.3 (12.7 – 13.8) aaa, bbb, ccc 11.0 (10.5 – 11.5) ddd, eee 7.5 (6.8 – 8.9) ff 8.8 (8.2 – 9.3)Hct (%) 38.3 (37.0 – 40.0) aaa, bbb, ccc 33.3 (32.0 – 36.4) ddd, eee 26.0 (21.5 – 26.9) 26.0 (24.3 – 27.7)RBC (10 12 /L) 5.25 (5.00 – 5.93) bbb, ccc 5.50 (5.18 – 5.70) ddd, eee 3.70 (3.40 – 3.94) ff 3.20 (3.00 – 3.40) MCV (fL) 78.3 (76.0 – 80.9) aaa, bbb, ccc 63.1 (60.0 – 65.3) eee 64.0 (55.5 – 66.0) 59.0 (54.9 – 61.7) RDW (%) 15.0 (14.6 – 16.0) aaa, bbb, ccc 18.0 (17.0 – 18.8) ddd, eee 24.0 (23.5 – 26.3) f 21.9 (16.7 – 24.6) Ferritin ( μ g/L) 35 (20 – 53) a, bbb, ccc 45 (30 – 65) ddd, eee 739 (573 – 1084) fff 1585 (1029 – 2116)
All the values are shown as median and 25 – 75 percentiles. * β -thalassemia; Hb, haemoglobin; Hct, hematocrit; RBC, red blood cell count; MCV, mean corpuscular volume; RDW, RBC distribution width; a Control vs. β -thalassemia minor ( a p � 0.05, aa p � 0.01, aaa p � 0.001). b Control vs. β -thalassemia intermedia ( b p � 0.05, bb p � 0.01, bbb p � 0.001). c Control vs. β -thalassemia major ( c p � 0.05, cc p � 0.01, ccc p � 0.001). d β -thalassemia minor vs. β -thalassemia intermedia ( d p � 0.05, dd p � 0.01, ddd p � 0.001). e β -thalassemia minor vs. β -thalassemia major ( e p � 0.05, ee p � 0.01, eee p � 0.001). f β -thalassemia intermedia vs. β -thalassemia major ( f p � 0.05, ff p � 0.01, fff p � 0.001).
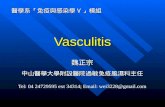
Table II. Serum concentrations of adipocytokines among different groups of β -thalassemia.
Control β -t * (minor) β -t (inter) β -t (major)
Adiponectin ( μ g/L) 1494 (1388 – 1788) bbb, ccc 1524 (1229 – 2136) ddd, eee 2598 (1947 – 3179) 3259 (2200 – 3736) Resistin (ng/L) 2272 (1719 – 2611) a, bbb, ccc 2502 (2198 – 2955) ddd, eee 3324 (2816 – 4250) 3586 (3014 – 4276)Visfatin ( μ g/L) 11.0 (10.6 – 11.3) a, bbb, ccc 11.3 (10.8 – 11.8) ddd, ee 12.2 (11.4 – 13.9) 12.0 (11.1 – 14.7)
All the values are shown as median and 25 – 75 percentiles. * β -thalassemia; a Control vs. β -thalassemia minor ( a p � 0.05, aa p � 0.01, aaa p � 0.001). b Control vs. β -thalassemia intermedia ( b p � 0.05, bb p � 0.01, bbb p � 0.001). c Control vs. β -thalassemia major ( c p � 0.05, cc p � 0.01, ccc p � 0.001). d β -thalassemia minor vs. β -thalassemia intermedia ( d p � 0.05, dd p � 0.01, ddd p � 0.001). e β -thalassemia minor vs. β -thalassemia major ( e p � 0.05, ee p � 0.01, eee p � 0.001). f β -thalassemia intermedia vs. β -thalassemia major ( f p � 0.05, ff p � 0.01, fff p � 0.001).
minor patients than in controls. Adiponectin ( p � 0.0001), resistin ( p � 0.0001) and visfatin ( p � 0.0001) concentrations were signifi cantly higher in β -thalassemia intermedia patients than in controls.
Adiponectin ( p � 0.0001), resistin ( p � 0.0001) and visfatin ( p � 0.0001) concentrations were sig-nifi cantly lower in controls than β -thalassemia major patients.
The concentrations of adiponectin ( p � 0.0001), resistin ( p � 0.003) and visfatin ( p � 0.002) were signifi cantly higher in β -thalassemia intermedia patients than in β -thalassemia minor patients.
Also, adiponectin ( p � 0.0001), resistin ( p � 0.0001) and visfatin ( p � 0.005) concentrations were signifi cantly higher in β -thalassemia major patients than in β -thalassemia minor patients.
There was no signifi cant difference between β -thalassemia intermedia and β -thalassemia major patients for adipocytokines concentrations.
Discussion
In β -thalassemia, the defect in the individual β -globin gene alone cannot fully explain the diversity of various complications such as cardiovascular prob-lems or chronic vascular infl ammation. Chronic hae-molysis, increased adhesiveness of erythrocytes and platelets to endothelial cells, oxidative stress and chronic iron overload participate in the endothelial damage and vascular infl ammation. Endothelial cells
participate in atherogenesis and anti- and pro-infl ammatory responses due to their ability to pro-duce and detect cytokines and their expression of adhesion molecules under certain circumstances [15]. Due to the wide range of functions in which the endothelial cells participate, endothelial dysfunc-tion, injury and activation may participate in numer-ous disease processes including atherosclerosis, diabetes, pulmonary hypertension, infl ammation and the hemoglobinopathies, including β -thalassemias.
In β -thalassemia patients, where vascular com-plications are frequent, there is strong evidence of endothelial cell activation and impaired endothe-lial function [15 – 17]. Endothelial activation in β -thalassemia patients is indicated by increased concentrations of circulating activated endothelial cells in these individuals, as well as elevated TNF- α , IL-1 β and vascular endothelial growth (VEGF) [18,19]. Furthermore, concentrations of vascular endothelial growth factor have been shown to cor-relate with the severity of TI [20]. Concentrations of sVCAM-1, sICAM-1 and sE-selection are reported to be signifi cantly increased in transfu-sion-dependent TM patients and increased levels of IL-6 indicate the presence of infl ammatory processes in individuals [17,19], possibly the result of oxidative stress due, once again, to iron overload. In addition to endothelial cell activation, erythrocytes and leuko-cytes from β -thalassemia individuals have been shown to display enhanced adherence to endothelial cells
Scan
d J
Clin
Lab
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Sout
h A
ustr
alia
on
08/1
1/14
For
pers
onal
use
onl
y.

Adipocytokines in b -thalassemia 309
and sub-endothelial protein, possibly contributing to endothelial activation [21,22].
In thalassemia, the activated and damaged endothelial cells could be the direct source of the increased adiponectin. Adiponectin may take part in the equilibrium between the release of cytokines and adhesion molecules from the endothelium. Elevated adiponectin may be the expression of a counter-regulatory response aimed at mitigating the endothe-lial damage and cardiovascular risk in these patients [7].
In our study, we found the similar results for adiponectin concentrations in different types of β -thalassemia patients. Adiponectin concentrations were increasing while the severity of disease, β -thalassemia major and β -thalassemia intermedia being clinically more signifi cant, was increasing.
Resistin is considered as a pro-infl ammatory cytokine [23]. Similar to adiponectin, resistin seems to have immunomodulatory potential. Recombinant human resistin increases the secretion of proinfl am-matory cytokines such as TNF-alpha, IL-6, and IL-12 in murine and human macrophages [10,24]. In addition, human endothelial cells are activated by recombinant human resistin [10], leading to increased expression of endothelin 1 and several adhesion mol-ecules as well as chemokines in these cells. Resistin may contribute to the development of obesity [25], insulin resistance [26,27] and the metabolic syn-drome [28]. Plasma resistin concentrations increase with increasing infl ammatory mediator levels, pre-dicting the severity of coronary atherosclerosis [29].
Similarly, we found that resistin concentrations were lower in controls than other groups. At the same time, the concentrations of resistin in β -thalassemia major and β -thalassemia intermedia patients were higher than in the other two groups (control and β -thalassemia minor). This fi nding indicates that similar results with adiponectin and resistin concen-tration changes according to the disease severity.
PBEF/Nampt/visfatin has been recently charac-terized as a novel adipocytokine [5]. It was demon-strated potent proinfl ammatory effects of this adipocytokine in human leukocytes [14]. Visfatin might have direct proinfl ammatory responses in cor-onary artery disease pathogenesis [30,31]. Previous studies have shown that visfatin expression is regu-lated by cytokines that promote insulin resistance, such as lipopolysaccharide, interleukin (IL)-1, tumour necrosis factor (TNF) and IL-6 [32 – 34]. A compelling body of evidence suggests a role for vis-fatin as a mediator of the infl ammatory response. The pathophysiological role of visfatin/PBEF in humans is controversial and remains largely unknown [35]. It is upregulated in obesity and in states of insulin resistance, but also exerts insulin mimetic effects in various tissues [36 – 38]. Circulating visfatin has been found to be increased in obesity and in other disor-ders related to insulin resistance and infl ammation
such as type 2 diabetes, polycystic ovary syndrome and infl ammatory bowel disease; progressive β -cell deterioration is also paralleled by increasing visfatin concentrations [39 – 42]. In contrast, other studies have found no relationship between circulating vis-fatin, insulin sensitivity or visceral fat mass and have reported no differences in visfatin gene expression between subcutaneous and visceral adipose tissue [43,44]. Visfatin has been described as a longevity protein that delays replicative senescence and enhances resistance to oxidative stress [36,45]. Visfatin is up-regulated by infection, hypoxia and infl ammatory cytokines and may, in turn, up-regulate the infl ammatory cascade [46 – 48].
Our study demonstrated that the serum concen-trations of visfatin were higher in β -thalassemia major and β -thalassemia intermedia patients compared to β -thalassemia minor patients and controls. Like pre-vious two cytokine levels, visfatin concentrations were increasing as the β -thalassemia diseases severity were increasing.
In conclusion, all results of the our study demon-strate that a novel association between the increasing concentrations of proinfl ammatory adipocytokines (adiponectin, resistin, visfatin) with the severity of beta-thalassemia types.
According to our fi ndings, we speculate that these proinfl ammatory adipocytokines play an important role in the development of the complications of β -thalassemias via infl ammatory processes. From this point, attenuation of proinfl ammatory adipocy-tokines or augmentation of the function of adiponec-tin, resistin and visfatin might be an effective therapy for the prevention of the complications of β -thalassemias.
Further clinical and experimental research should elucidate the relationship between proinfl ammatory adipocytokines and β -thalassemia types.
Declaration of interest : The authors report no confl icts of interest. The authors alone are respon-sible for the content and writing of the paper.
References
Muncie HL Jr , Campbell J . Alpha and beta thalassemia . Am [1] Fam Physician 2009 ; 80 : 339 – 44 . Weatherall DJ . The thalassaemias . BMJ 1997 ; 314 : 1675 – 8 . [2] Kanavaki I , Makrythanasis P , Lazaropoulou C , Tsironi M , [3] Kattamis A , Rombos I , Papassotiriou I . Soluble endothelial adhesion molecules and infl ammation markers in patients with beta-thalassemia intermedia . Blood Cells Mol Dis 2009 ; 43 : 230 – 4 . Kamada Y , Takehara T , Hayashi N . Adipocytokines and liver [4] disease . J Gastroenterol 2008 ; 43 : 811 – 22 . Fukuhara A , Matsuda M , Nishizawa M , Segawa K , Tanaka [5] M , Kishimoto K , Matsuki Y , Murakami M , Ichisaka T , Murakami H , Watanabe E , Takagi T , Akiyoshi M , Ohtsubo T , Kihara S , Yamashita S , Makishima M , Funahashi T , Yamanaka S , Hiramatsu R , Matsuzawa Y , Shimomura I .
Scan
d J
Clin
Lab
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Sout
h A
ustr
alia
on
08/1
1/14
For
pers
onal
use
onl
y.

310 Y. Enl i et al.
Visfatin: a protein secreted by visceral fat that mimics the effects of ins ü lin . Science 2005 ; 307 : 426 – 30 . Anfossi G , Russo I , Doronzo G , Pomero A , Trovati M . [6] Adipocytokines in atherothrombosis: focus on platelets and vascular smooth muscle cells . Mediators Infl amm 2010 ; 2010 : 174341 . doi: 10.1155/2010/174341 . Chaliasos N , Challa A , Hatzimichael E , Koutsouka F , [7] Bourantas DK , Vlahos AP , Siamopoulou A , Bourantas KL , Makis A . Serum adipocytokine and vascular infl ammation marker levels in Beta-thalassaemia major patients . Acta Hae-matol 2010 ; 124 : 191 – 6 . Chung CP , Long AG , Solus JF , Rho YH , Oeser A , Raggi P , [8] Stein CM . Adipocytokines in systemic lupus erythematosus: relationship to infl ammation, insulin resistance and coro-nary atherosclerosis . Lupus 2009 ; 18 : 799 – 806 . Steppan CM , Bailey ST , Bhat S , Brown EJ , Banerjee [9] RR , Wright CM , Patel HR , Ahima RS , Lazar MA . The hormone resistin links obesity to diabetes . Nature 2001 ; 409 : 307 – 12 . Lehrke M , Reilly MP , Millington SC , Iqbal N , Rader DJ , [10] Lazar MA . An infl ammatory cascade leading to hyperre-sistinemia in humans . PLoS Med 2004 ; 2 : 161 – 8 . Bokarewa M , Nagaev I , Dahlberg L , Smith U , Tarkowski A . [11] Resistin, an adipokine with potent proinfl ammatory proper-ties . J Immunol 2005 ; 174 : 5789 – 95 . Verma S , Li SH , Wang CH , Fedak PW , Li RK , Weisel RD , [12] Mickle DA . Resistin promotes endothelial cell activation: further evidence of adipokineendothelial interaction . Circu-lation 2003 ; 108 : 736 – 40 . Samal B , Sun Y , Stearns G , Xie C , Suggs S , McNiece I . [13] Cloning and characterization of the cDNA encoding a novel human pre-B-cell colony-enhancing factor . Mol Cell Biol 1994 ; 14 : 1431 – 7 . Moschen AR , Kaser A , Enrich B , Mosheimer B , Theurl M , [14] Niederegger H , Tilg H . Visfatin, an adipocytokine with proinfl ammatory and ı mmunomodulating properties . J Immunol 2007 ; 178 : 1748 – 58 . Hartge MM , Unger T , Kintscher U . The endothelium and [15] vascular infl ammation in diabetes . Diab Vasc Dis Res 2007 ; 4 : 84 – 8 . Taher AT , Otrock ZK , Uthman I , Cappellini MD . Thalas-[16] semia and hypercoagulability . Blood Rev 2008 ; 22 : 283 – 92 . Aggeli C , Antoniades C , Cosma C , Chrysohoou C , Tousou-[17] lis D , Ladis V , Karageorga M , Pitsavos C , Stefanadis C . Endothelial dysfunction and infl ammatory process in trans-fusion-dependent patients with beta thalassemia major . Int J Cardiol 2005 ; 105 : 80 – 4 . Butthep P , Bunyaratvej A , Funahara Y , Kitaguchi H , Fucha-[18] roen S , Sato S , Bhamarapravati N . Alterations in vascular endothelial cell-related plasma proteins in thalassaemic patients and their correlation with clinical symptoms . Thromb Haemost 1995 ; 74 : 1045 – 9 . Butthep P , Rummavas S , Wisedpanichkij R , Jindadamron-[19] gwech S , Fucharoen S , Bunyaratvej A . Increased circulating activated endothelial cells, vascular endothelial growth fac-tor, and tumor necrosis factor in thalassemia . Am J Hematol 2002 ; 70 : 100 – 6 . Kyriakou DS , Alexandrakis MG , Kyriakou ES , Liapi D , [20] Kourelis TV , Passam F , Papadakis A . Activated peripheral blood and endothelial cells in thalassemia patients . Ann Hematol 2001 ; 80 : 577 – 83 . Shitrit D , Tamary H , Koren A , Levin C , Bargil-Shitrit A , [21] Sulkes J , Kramer MR . Correlation of vascular endothelial growth factor with the severity of thalassemia intermedia . Blood Coagul Fibrinolysis 2008 ; 19 : 611 – 4 . Hovav T , Goldfarb A , Artmann G , Yedgar S , Barshtein G . [22] Enhanced adherence of beta-thalassaemic erythrocytes to endothelial cells . Br J Haematol 1999 ; 106 : 178 – 81 . Silswal N , Singh AK , Aruna B , Mukhopadhyay S , Ghosh S , [23] Ehtesham NZ . Human resistin stimulates the proinfl amma-tory cytokines TNF-alpha and IL-12 in macrophages by
NF-kappa betaB-dependent pathway . Biochem Biophys Res Commun 2005 ; 334 : 1092 – 101 . Yamamoto K , Kiyohara T , Murayama Y , Kihara S , Okamoto [24] Y , Funahashi T , Ito T , Nezu R , Tsutsui S , Miyagawa JI , Tamura S , Matsuzawa Y , Shimomura I , Shinomura Y . Production of adiponectin, an anti-infl ammatory protein, in mesenteric adi-pose tissue in Crohn ’ s disease . Gut 2005 ; 54 : 789 – 96 . Yu R , Xie S , Chen J , Zhang L , Dai Y . The effects of PACAP [25] and related peptides on leptin, soluble leptin receptor and resistin in normal condition and LPS-induced infl amma-tion . Peptides , 2009 ; 30 : 1456 – 9 . Vozarova de Courten B , Degawa-Yamauchi M , Considine [26] RV , Tataranni PA . High serum resistin is associated with an increase in adiposity but not a worsening of insulin resis-tance in Pima Indians . Diabetes 2004 ; 53 : 1279 – 84 . McTernan PG , Fisher FM , Valsamakis G , Chetty R , [27] Harte A , McTernan CL , Clark PM , Smith SA , Barnett AH , Kumar S . Resistin and type 2 diabetes: regulation of resistin expression by insulin and rosiglitazone and the effects of recombinant resistin on lipid and glucose metabolism in human differentiated adipocytes . J Clin Endocrinol Metab 2003 ; 88 : 6098 – 106 . Silha JV , Krsek M , Skrha JV , Sucharda P , Nyomba BL , [28] Murphy LJ . Plasma resistin, adiponectin and leptin levels in lean and obese subjects: correlations with insulin resistance . Eur J Endocrinol 2003 ; 149 : 331 – 5 . Szapary PO , Bloedon LT , Samaha FF , Duffy D , Wolfe ML , [29] Soffer D , Reilly MP , Chittams J , Rader DJ . Effects of pio-glitazone on lipoproteins, infl ammatory markers, and adi-pokines in nondiabetic patients with metabolic syndrome . Arterioscler Thromb Vasc Biol 2006 ; 26 : 182 – 8 . Mazurek T , Zhang L , Zalewski A , Mannion JD , Diehl JT , [30] Arafat H , Sarov-Blat L , O ’ Brien S , Keiper EA , Johnson AG , Martin J , Goldstein BJ , Shi Y . Human epicardial adipose tissue is a source of infl ammatory mediators . Circulation 2003 ; 108 : 2460 – 6 . Baker AR , Silva NF , Quinn DW , Harte AL , Pagano D , [31] Bonser RS , Kumar S , McTernan PG . Human epicardial adipose tissue expresses a pathogenic profi le of adipocytok-ines in patients with cardiovascular disease . Cardiovasc Dia-betol 2006 ; 5 : 1 – 7 . Ognjanovic S , Bao S , Yamamoto SY , Garibau-Tupas J , [32] Samal B , Bryant-Greenwood GD . Genomic organization of the gene coding for human pre-B-cell colony enhancing fac-tor and expression in human fetal membranes . J Mol Endo-crinol 2001 ; 26 : 107 – 17 . Kralisch S , Klein J , Lossner U , Bluher M , Paschke R , [33] Stumvoll M , Fasshauer M . Interleukin-6 is a negative regu-lator of visfatin gene expression in 3T3-L1 adipocytes . Am J Physiol Endocrinol Metab 2005 ; 289 : 586 – 90 . Kralisch S , Klein J , Lossner U , Bluher M , Paschke R , [34] Stumvoll M , Fasshauer M . Hormonal regulation of the novel adipocytokine visfatin in 3T3-L1 adipocytes . J Endocrinol 2005 ; 185 : 1 – 8 . Stephens JM , Vidal-Puig AJ . An update on visfatin/pre-B-cell [35] colony enhancing factor, an ubiquitously expressed, illusive cytokine that is regulated in obesity . Curr Opin Lipidol 2006 ; 17 : 128 – 31 . Jia SH , Li Y , Parodo J , Kapus A , Fan L , Rotstein OD , [36] Marshall JC . Pre-B cell colony-enhancing factor inhibits neutrophil apoptosis in experimental infl ammation and clinical sepsis . J Clin Invest 2004 ; 113 : 1318 – 27 . Ye SQ , Simon BA , Maloney JP , Zambelli-Weiner A , [37] Gao L , Grant A , Easley RB , McVerry BJ , Tuder RM , Standiford T , Brower RG , Barnes KC , Garcia JG . Pre-B-cell colony-enhancing factor as a potential novel biomarker in acute lung injury . Am J Respir Crit Care Med 2005 ; 171 : 361 – 70 . Sethi JK , Vidal-Puig A . Visfatin: the missing link between [38] intra-abdominal obesity and diabetes? Trends Mol Med 2005 ; 11 : 44 – 7 .
Scan
d J
Clin
Lab
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Sout
h A
ustr
alia
on
08/1
1/14
For
pers
onal
use
onl
y.

Adipocytokines in b -thalassemia 311
Haider DG , Holzer G , Schaller G , Weghuber D , Widhalm [39] K , Wagner O Kapiotis S, Wolzt M . The adipokine visfatin is markedly elevated in obese children . JPGN 2006 ; 43 : 548 – 9 . Tan BK , Chen J , Digby JE , Keay SD , Kennedy CR , Randeva [40] HS . Increased visfatin messenger ribonucleic acid and pro-tein levels in adipose tissue and adipocytes in women with polycystic ovary syndrome: parallel increase in plasma visfa-tin . J Clin Endocrinol Metab 2006 ; 91 : 5022 – 8 . Chen MP , Chung FM , Chang DM , Tsai JC , Huang HF , [41] Shin SJ , Lee YJ . Elevated plasma level of visfatin/pre-B cell colony-enhancing factor in patients with type 2 diabetes mellitus . J Clin Endocrinol Metab 2006 ; 91 : 295 – 9 . Lopez-Bermejo A , Chico-Julia B , Fernandez-Balsells M , [42] Recasens Esteve E , Casamitjana R , Ricart W , Fern á ndez-Real JM . Serum visfatin increases with progressive beta-cell deterioration . Diabetes 2006 ; 55 : 2871 – 5 . Berndt J , Kloting N , Kralisch S , Kovacs P , Fasshauer M , [43] Schon MR , Stumvoll M , Bl ü her M . Plasma visfatin concen-trations and fat depot-specifi c mRNA expression in humans . Diabetes 2005 ; 54 : 2911 – 6 .
Pagano C , Pilon C , Olivieri M , Mason P , Fabris R , Serra R , [44] Milan G , Rossato M , Federspil G , Vettor R . Reduced plasma visfatin/pre-B cell colony-enhancing factor in obesity is not related to insulin resistance in humans . J Clin Endocrinol Metab 2006 ; 91 : 3165 – 70 . Yang H , Lavu S , Sinclair DA . Nampt/PBEF/Visfatin: a reg-[45] ulator of mammalian health and longevity? Experim Geron-tol 2006 ; 41 : 718 – 26 . Bae SK , Kim SR , Kim JG , Kim JY , Koo TH , Jang HO , [46] Yun I , Yoo MA , Bae MK . Hypoxic induction of human vis-fatin gene is directly mediated by hypoxia-inducible factor-1 . FEBS Lett 2006 ; 580 : 4105 – 13 . Segawa K , Fukuhara A , Hosogai N , Morita K , Okuno Y , [47] Tanaka M , Nakagawa Y , Kihara S , Funahashi T , Komuro R , Matsuda M , Shimomura I . Visfatin in adipocytes is upregu-lated by hypoxia through HIF1alpha-dependent mechanism . Biochem Biophys Res Commun 2006 ; 349 : 875 – 82 . Kendal CE , Bryant-Greenwood GD . Pre-B-cell colonyen-[48] hancing factor (PBEF/Visfatin) gene expression is modu-lated by NF-kappaB and AP-1 in human amniotic epithelial cells . Placenta 2006 ; 28 : 305 – 14 .
Scan
d J
Clin
Lab
Inv
est D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Sout
h A
ustr
alia
on
08/1
1/14
For
pers
onal
use
onl
y.