![9.麻酔・鎮静経時的 な観察 が必要 と考えられ る(エキスパートオピニオン ). [推奨 を臨床 に用いる 際の注意点] 鎮静 や全身麻酔](https://static.fdocument.pub/doc/165x107/5ea2ca6ddc27e166df495096/9ieefee-coec-e-oee-efoe-iffffff.jpg)
9.麻酔・鎮静経時的 な観察 が必要 と考えられ る(エキスパートオピニオン ). [推奨 を臨床 に用いる 際の注意点] 鎮静 や全身麻酔

2014年3月18日 慈恵ICU勉強会
金子 貴久
本日のテーマ
• 現代ICUの鎮静スタイル
• 鎮静薬の選択
• 譫妄

現代ICUの鎮静スタイル
現代ICUにおける鎮静の3要素
• Pain • Agita2on (⇔over-‐seda2on) • Delirium
鎮静
• ICU滞在中の患者は挿管、人工呼吸、環境 などから強いストレスを受けている
• 適切な鎮静、興奮および譫妄の予防、治療は集中治療の重要な要素
• 近年、鎮静、興奮および譫妄への介入に 新たな指針が示されている
集中治療 医学文献レビュー 2014~2015 学研メディカル秀潤社, 2014: 164-‐180.

N Engl J Med 2014;370:444-‐54.

Pain
• ICU患者の大多数が痛みを感じている
• 痛みがコントロールされないと エネルギー消費、免疫機能に影響が及ぶ
• コントロールされない痛みは PTSDのリスクとなる
Am J Crit Care 2000;9:20-‐7.
Chest 1988;93:4-‐10.
Crit Care 2010;14(1): R14.
Pain 2001;90:191-‐9.
• ICU患者の痛みの評価は困難である • 痛みは基本的には主観的なものであるが ICU患者の多くは訴える事ができない
• 頻脈や高血圧を痛みの指標とすることは
難しく、鎮痛スケールを用いて客観的に 反復して評価する必要がある
Pain
Intensive Crit Care Nurs 2011;27:46-‐52.
Crit Care Med 2001;29:2258-‐63. Am J Crit Care 2006;15:420-‐7.
過去の鎮静
• 周術期麻酔管理から発展
• 人工呼吸器が未発達 → 患者との同調が困難であり深い鎮静が必要
• 長時間作用型の薬剤、もしくは短時間作用型 薬剤の持続注入での管理が中心
N Engl J Med 2014;370:444-‐54.
過去の鎮静
• 周術期麻酔管理から発展
• 人工呼吸器が未発達 → 患者との同調が困難であり深い鎮静が必要
• 長時間作用型の薬剤、もしくは短時間作用型 薬剤の持続注入での管理が中心
とにかく寝かせて動かさないように!
N Engl J Med 2014;370:444-‐54.

深い鎮静の問題点
• 状態の変化や神経学的徴候、疼痛の 客観的評価が困難
• 鎮痛の不足や譫妄の存在が鎮静によって マスクされる
• 人工呼吸器装着期間やICU滞在期間 入院期間が遷延
Crit Care Med 1996; 24:1953-‐61 Lancet 2010; 375: 475–80
Lancet 2008; 371: 126–34

Daliy InterrupAon of SedaAve Infusions in CriAcally Ill PaAents Undergoing Mechanical VenAlaAon
N Engl J Med 2000; 342:1471-‐77
【デザイン】ランダム化比較試験 【セッティング】単施設研究 【対象】ICUで人工呼吸管理を 受けている患者128人 【方法】1日1度の鎮静を中断、覚醒 させる介入(DSI)を行った群と 鎮静を継続した群を比較
参考:2011.4.19 慈恵ICU勉強会
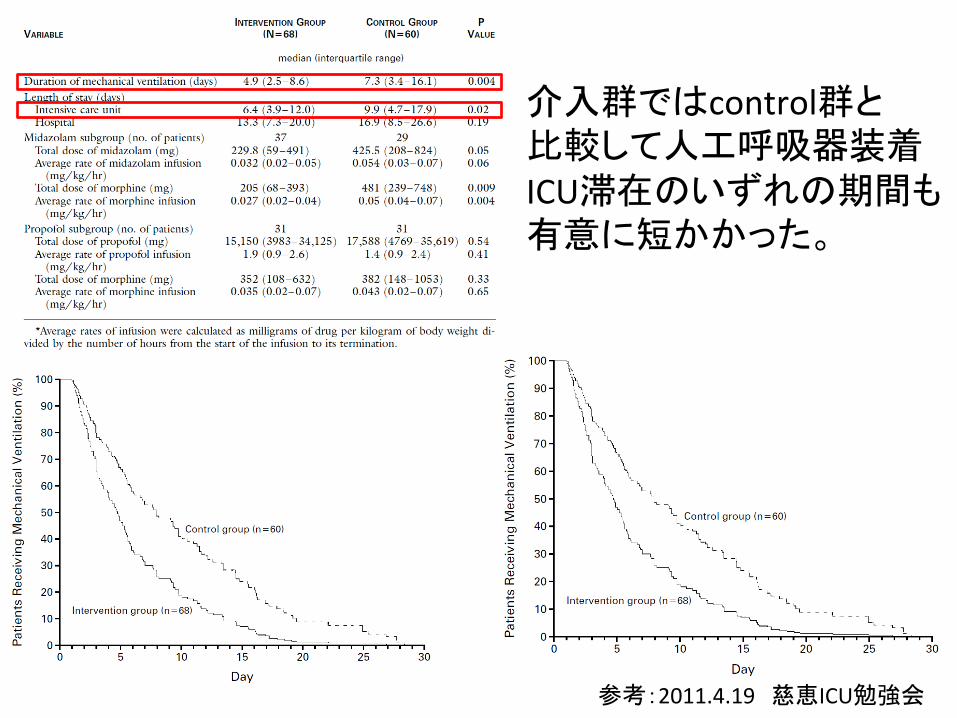
介入群ではcontrol群と 比較して人工呼吸器装着 ICU滞在のいずれの期間も 有意に短かかった。
参考:2011.4.19 慈恵ICU勉強会
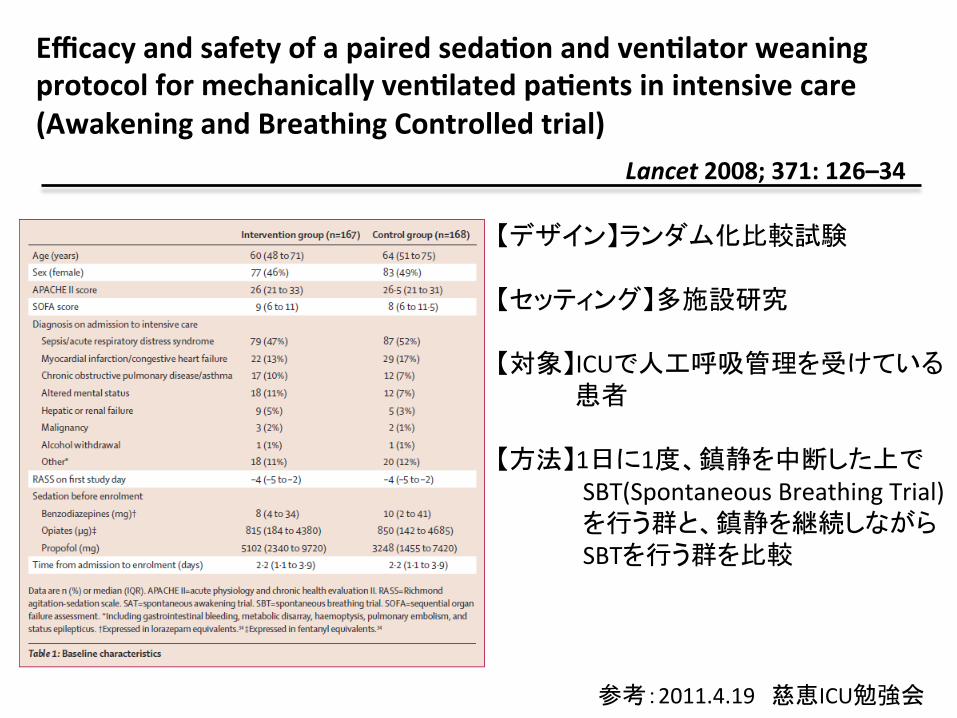
Efficacy and safety of a paired sedaAon and venAlator weaning protocol for mechanically venAlated paAents in intensive care (Awakening and Breathing Controlled trial)
Lancet 2008; 371: 126–34
【デザイン】ランダム化比較試験 【セッティング】多施設研究 【対象】ICUで人工呼吸管理を受けている 患者 【方法】1日に1度、鎮静を中断した上で SBT(Spontaneous Breathing Trial) を行う群と、鎮静を継続しながら SBTを行う群を比較
参考:2011.4.19 慈恵ICU勉強会
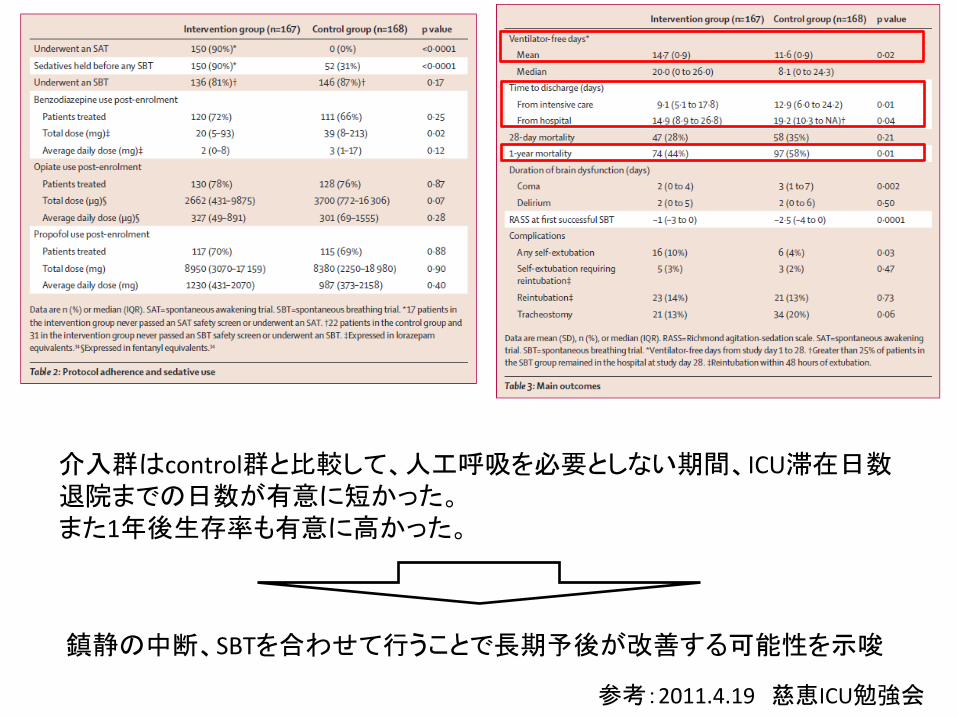
介入群はcontrol群と比較して、人工呼吸を必要としない期間、ICU滞在日数 退院までの日数が有意に短かった。 また1年後生存率も有意に高かった。
鎮静の中断、SBTを合わせて行うことで長期予後が改善する可能性を示唆
参考:2011.4.19 慈恵ICU勉強会
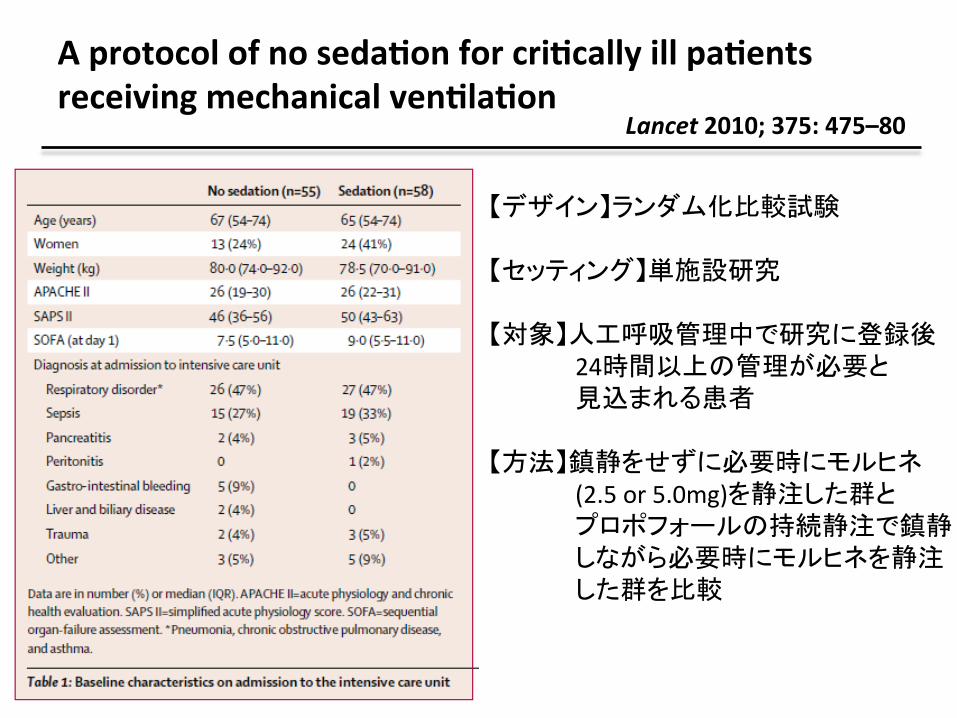
A protocol of no sedaAon for criAcally ill paAents receiving mechanical venAlaAon
Lancet 2010; 375: 475–80
【デザイン】ランダム化比較試験 【セッティング】単施設研究 【対象】人工呼吸管理中で研究に登録後 24時間以上の管理が必要と 見込まれる患者 【方法】鎮静をせずに必要時にモルヒネ (2.5 or 5.0mg)を静注した群と プロポフォールの持続静注で鎮静 しながら必要時にモルヒネを静注 した群を比較
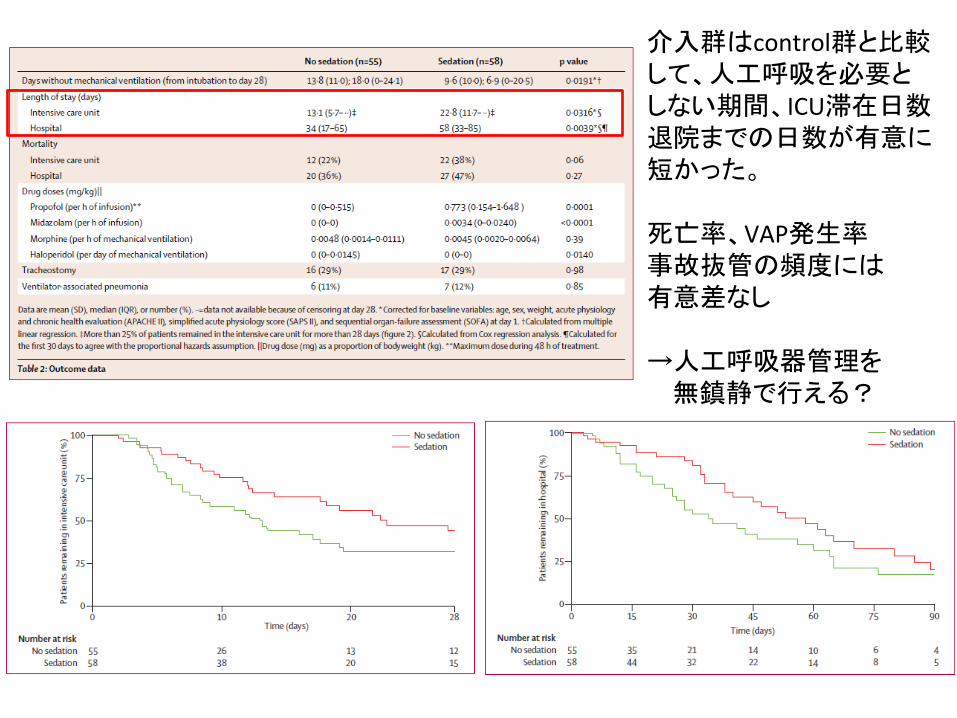
介入群はcontrol群と比較して、人工呼吸を必要と しない期間、ICU滞在日数 退院までの日数が有意に短かった。 死亡率、VAP発生率 事故抜管の頻度には 有意差なし →人工呼吸器管理を 無鎮静で行える?

Daily SedaAon InterrupAon in Mechanically VenAlated CriAcally Ill PaAents Cared for With a SedaAon Protocol
JAMA. 2012;308:1985-‐92
【デザイン】ランダム化比較試験 【セッティング】多施設研究 【対象】人工呼吸器管理中で研究に登録後 48時間以上の管理が必要と 見込まれる患者 【方法】RASS 0~-‐3を目標に ベンゾジアゼピン、オピオイドの 投与を受ける患者を 1日に1度の鎮静の中断を受ける群 鎮静を継続する群 の2群に分けて比較
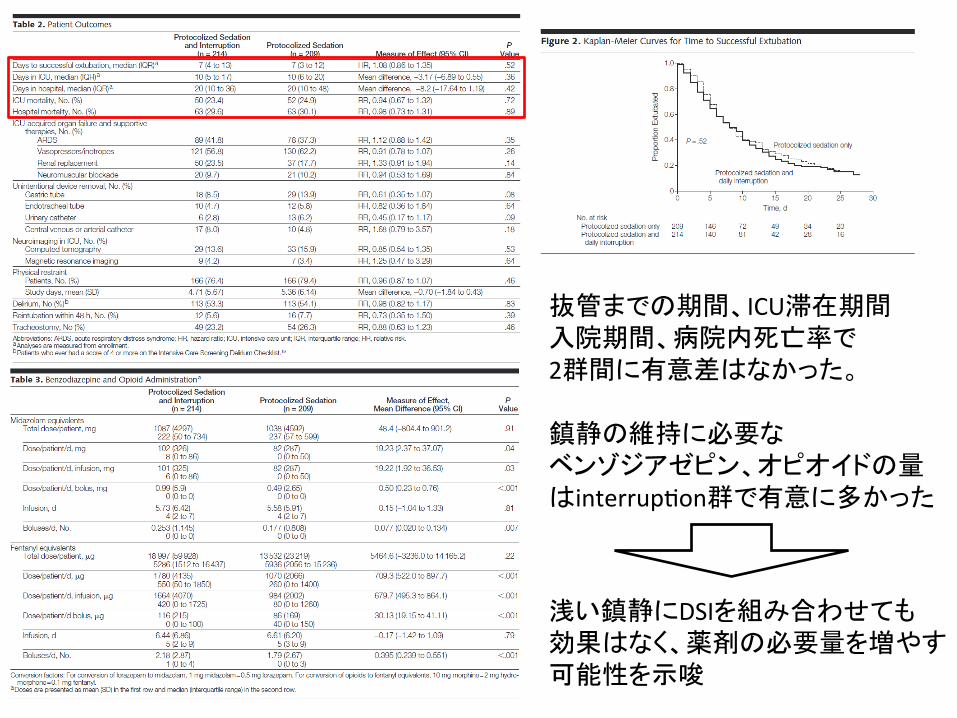
抜管までの期間、ICU滞在期間 入院期間、病院内死亡率で 2群間に有意差はなかった。 鎮静の維持に必要な ベンゾジアゼピン、オピオイドの量はinterrup2on群で有意に多かった
浅い鎮静にDSIを組み合わせても 効果はなく、薬剤の必要量を増やす 可能性を示唆
まとめ
• 鎮痛は重要
• 浅い鎮静が予後を改善させる可能性が 示唆されている
• 鎮静薬が不要であるかについては検討が 必要
• プロトコルに沿った浅い鎮静を行えばDSIは 必須ではない

鎮静薬の選択

ICUで鎮静および鎮痛に使用される薬剤
N Engl J Med 2014;370:444-‐54.
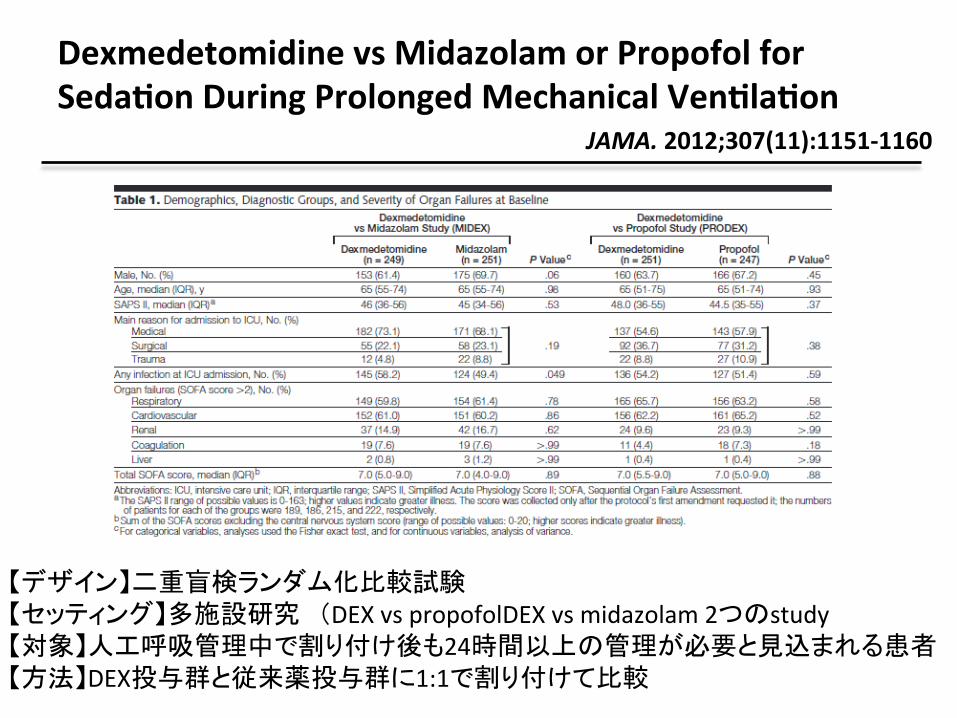
Dexmedetomidine vs Midazolam or Propofol for SedaAon During Prolonged Mechanical VenAlaAon
JAMA. 2012;307(11):1151-‐1160
【デザイン】二重盲検ランダム化比較試験 【セッティング】多施設研究 (DEX vs propofolDEX vs midazolam 2つのstudy 【対象】人工呼吸管理中で割り付け後も24時間以上の管理が必要と見込まれる患者 【方法】DEX投与群と従来薬投与群に1:1で割り付けて比較

DEX群はmidazolam群と比較して人工呼吸管理期間が短いが propofolとは有意差なし。 ICU滞在期間はDEX群と従来薬群で有意差なし。

DEX群は従来薬群と比較して覚醒度合、痛みの表現力、看護ケアへの協力度が 高い その他死亡率、入院期間に有意差なし DEX群では低血圧、除脈の発生率が従来薬群と比較して有意に高い
参考:2012年慈恵ICU勉強会

まとめ
• DEXのmidazolam, propofolに対する非劣性が示されたにとどまる
• 鎮静中の神経学的評価の正確性が向上する可能性はあるが、具体的なoutcomeの改善は 示されていない
参考:2012年慈恵ICU勉強会
譫妄
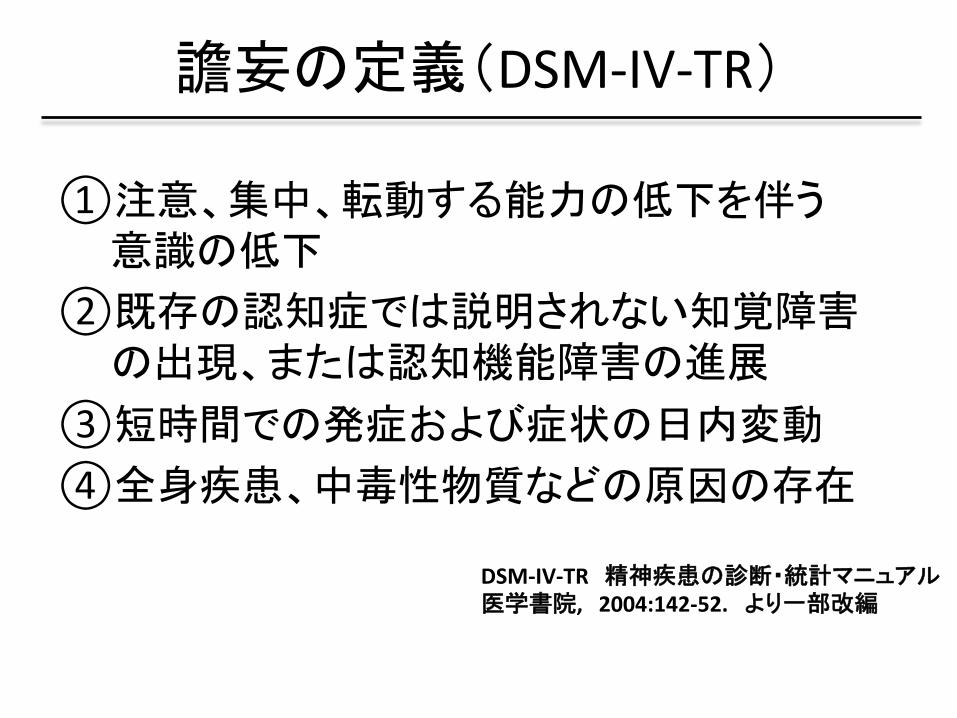
譫妄の定義(DSM-‐IV-‐TR)
① 注意、集中、転動する能力の低下を伴う 意識の低下
② 既存の認知症では説明されない知覚障害の出現、または認知機能障害の進展
③ 短時間での発症および症状の日内変動 ④ 全身疾患、中毒性物質などの原因の存在
DSM-‐IV-‐TR 精神疾患の診断・統計マニュアル 医学書院, 2004:142-‐52. より一部改編

• 血液検査や電気生理学検査などでは わからず臨床診断のみである
• 発症率は16%〜89%と幅広い
• hypoac2veとhyperac2veがあり、ICUの 譫妄の中でhyperac2veなものは2%以下と する報告もある
• 高齢、鎮静薬、疾患の重症度などが risk factorとしてあげられる
譫妄の疫学
Intensive Care Med 2001; 27:859-‐64. Crit Care Med 2007;35: 112-‐7.
BMJ 2012; 344:e420.
Am J Respir Crit Care Med 2009; 180:1092-‐7.
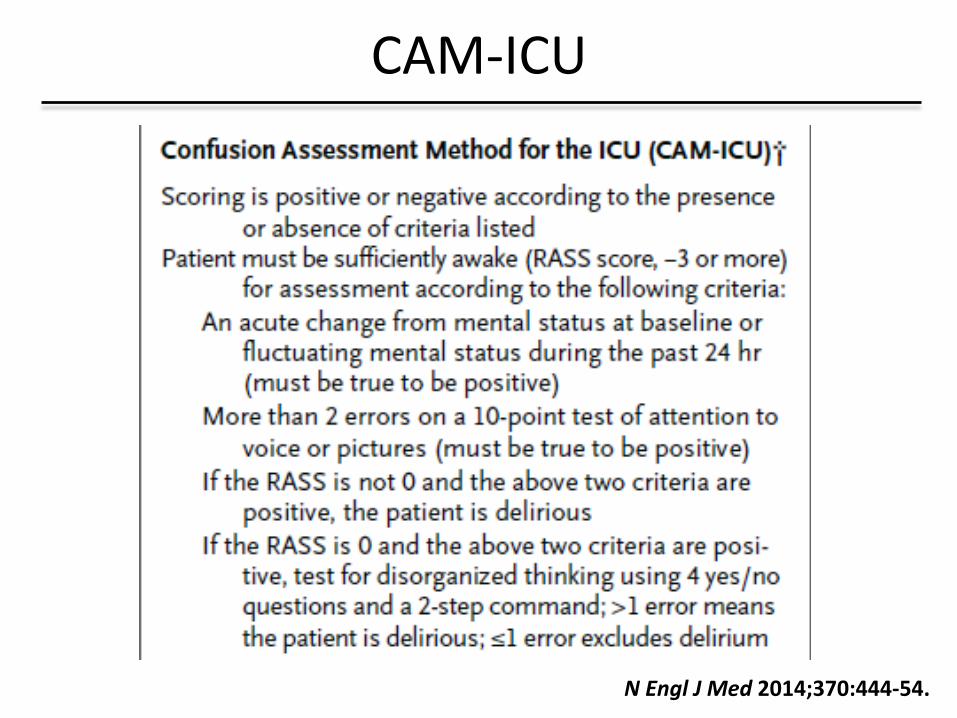
CAM-‐ICU
N Engl J Med 2014;370:444-‐54.
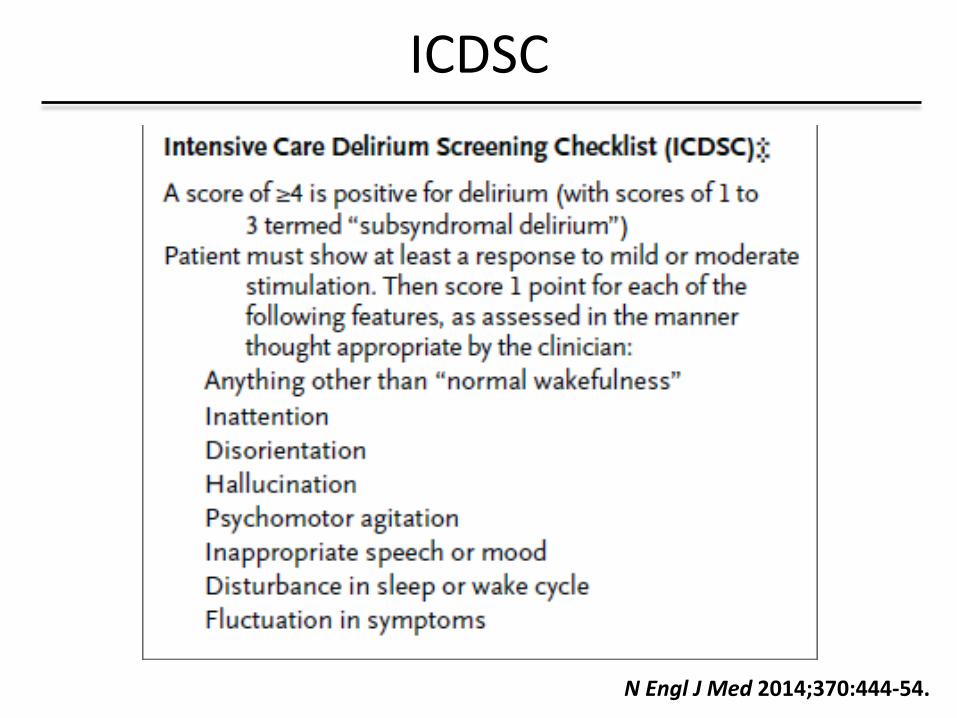
ICDSC
N Engl J Med 2014;370:444-‐54.
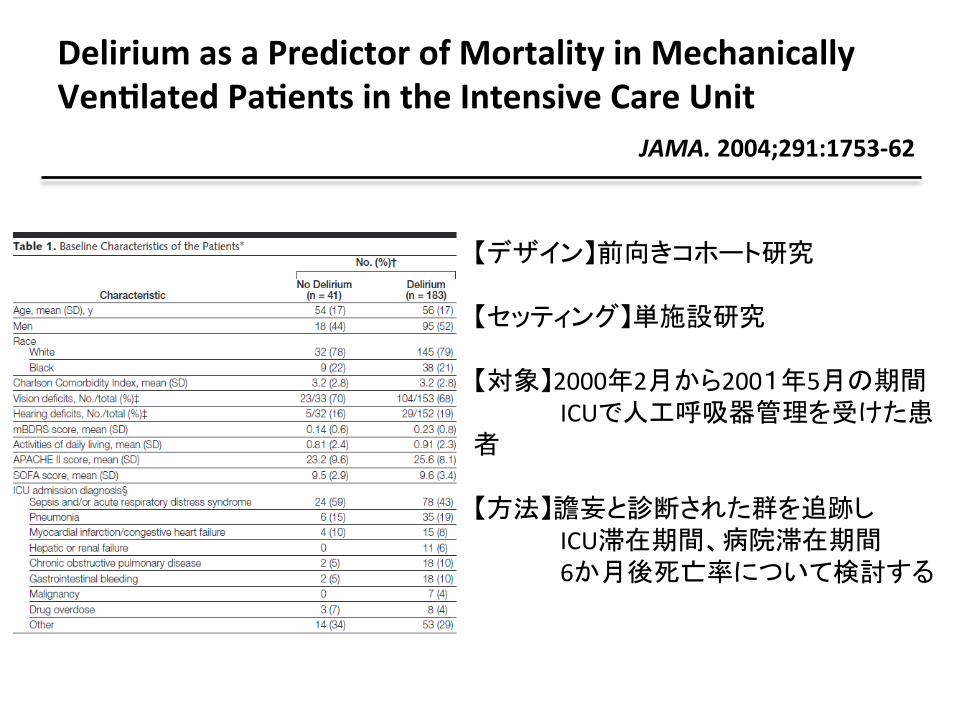
Delirium as a Predictor of Mortality in Mechanically VenAlated PaAents in the Intensive Care Unit
JAMA. 2004;291:1753-‐62
【デザイン】前向きコホート研究 【セッティング】単施設研究 【対象】2000年2月から2001年5月の期間 ICUで人工呼吸器管理を受けた患者 【方法】譫妄と診断された群を追跡し ICU滞在期間、病院滞在期間 6か月後死亡率について検討する
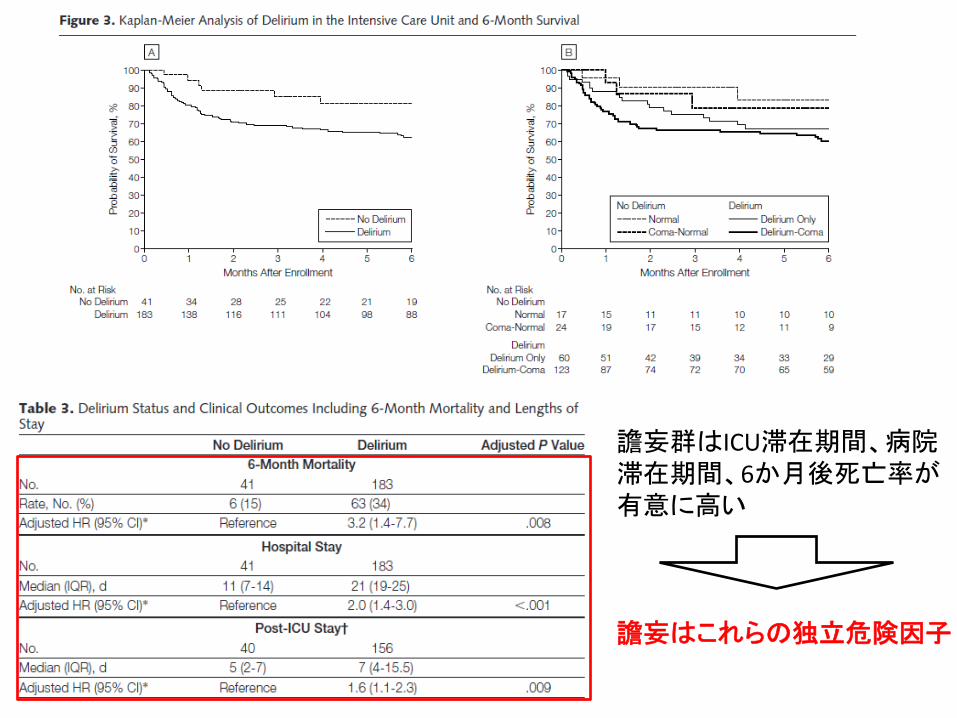
譫妄群はICU滞在期間、病院 滞在期間、6か月後死亡率が 有意に高い 譫妄はこれらの独立危険因子

Early physical and occupaAonal therapy in mechanically venAlated, criAcally ill paAents
Lancet 2009; 373: 1874–82
【デザイン】ランダム化比較試験 【セッティング】多施設研究 【対象】72時間以下の人工呼吸管理が 行われており、さらに24時間以上 の人工呼吸管理が見込まれる 患者 【方法】1日目より理学療法、作業療法を 行った群とプライマリーケア チームよりオーダーがあった際に 治療を行った群を比較
参考:2011.4.19 慈恵ICU勉強会

介入群のICU滞在中の譫妄の発生率および期間はcontrol 群と比較して有意に短い またICU滞在期間を含む入院期間全体でも同様の結果が示された ただしICU滞在期間や入院期間、入院中死亡率には有意差なし
参考:2011.4.19 慈恵ICU勉強会

Haloperidol prophylaxis decreases delirium incidence in elderly paAents a\er noncardiac surgery
Crit Care Med 2012; 40:731–39
【デザイン】ランダム化比較試験 【セッティング】2施設研究 【対象】65歳以上の術後ICU入室患者 【方法】haloperidol 0.5mgを投与後 0.1mg/hrの持続投与を行った 群とプラセボ群を比較
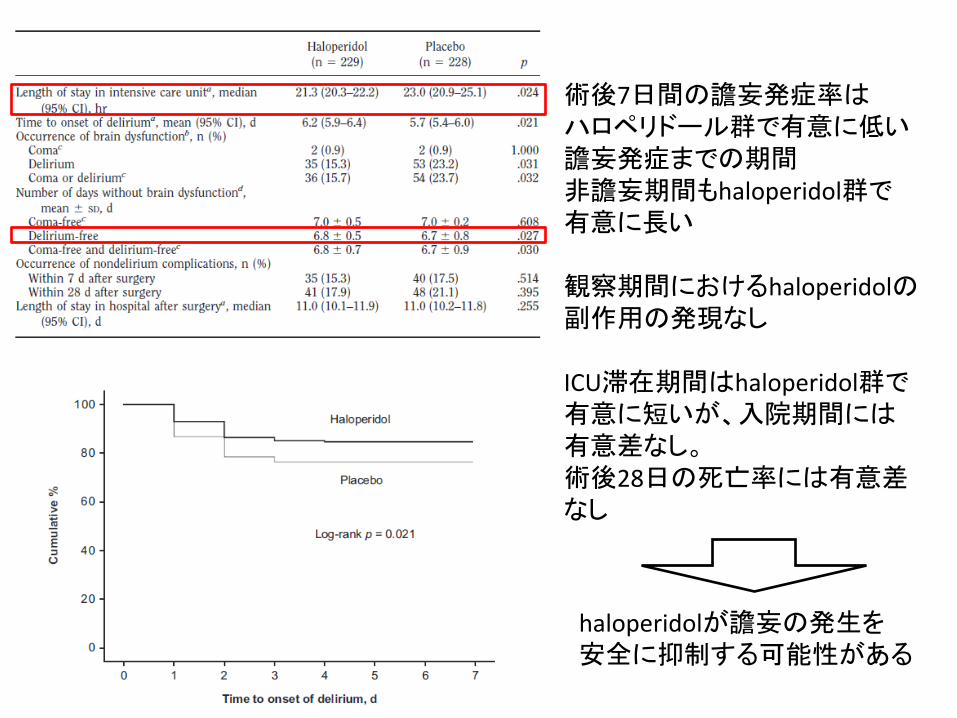
術後7日間の譫妄発症率は ハロペリドール群で有意に低い 譫妄発症までの期間 非譫妄期間もhaloperidol群で 有意に長い 観察期間におけるhaloperidolの副作用の発現なし ICU滞在期間はhaloperidol群で 有意に短いが、入院期間には 有意差なし。 術後28日の死亡率には有意差 なし
haloperidolが譫妄の発生を 安全に抑制する可能性がある
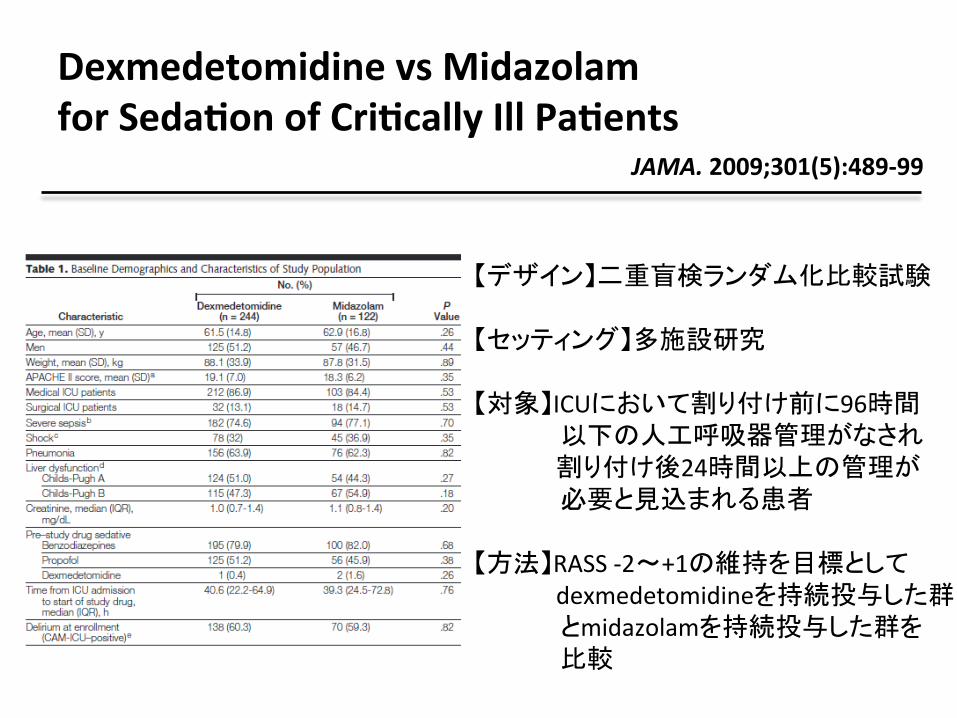
Dexmedetomidine vs Midazolam for SedaAon of CriAcally Ill PaAents
JAMA. 2009;301(5):489-‐99
【デザイン】二重盲検ランダム化比較試験 【セッティング】多施設研究 【対象】ICUにおいて割り付け前に96時間 以下の人工呼吸器管理がなされ 割り付け後24時間以上の管理が 必要と見込まれる患者 【方法】RASS -‐2~+1の維持を目標として dexmedetomidineを持続投与した群 とmidazolamを持続投与した群を 比較

介入期間(抜管もしくは開始より 30日)の譫妄発生率はdexmedetomidine群で有意に 低い。 平均投与期間が短いが 非譫妄期間もdexmedetomidine群で有意に長い。 抜管までの時間は dexmedetomidine群が1.9日短いが ICU滞在期間は変わらず。
Dexmedetomidineでの鎮静が 譫妄発症を予防する可能性がある

Efficacy and safety of queAapine in criAcally ill paAents with delirium Crit Care Med 2010; 38: 419–27
【デザイン】二重盲検ランダム化比較試験 【セッティング】3施設研究 【対象】ICU入室中、譫妄と診断されたうち 経腸栄養が可能で、他の神経学的 合併症を持たない患者 【方法】12時間ごとにque2apine 50mgの 投与を受けた群と プラセボ群を比較 両群で必要に応じてhaloperidol を投与する。
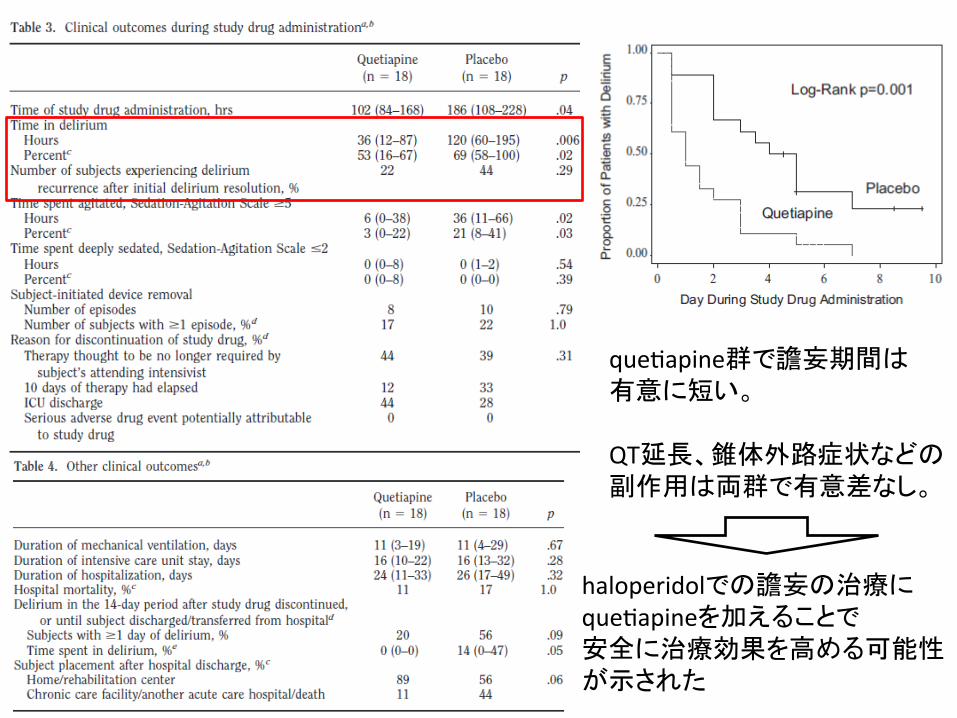
que2apine群で譫妄期間は 有意に短い。 QT延長、錐体外路症状などの 副作用は両群で有意差なし。
haloperidolでの譫妄の治療に que2apineを加えることで 安全に治療効果を高める可能性 が示された
まとめ
• 譫妄は予後を悪化させる独立危険因子であり予防を含めた早期の介入が必要
• 早期のリハビリテーションの開始 haloperidolの投与、dexmedetomidineでの 鎮静が譫妄の予防に有効である可能性が 示されている
• haloperidol, que2apineの併用が譫妄治療に 有効である可能性が示されている

新しいガイドライン
PADガイドライン
• American College of Cri2cal Care Medicineが発表した2013年度版ガイドライン
• Pain, Agita2on, Deliriumの評価、治療に 対する声明および推奨を軸としており PADガイドラインと別称される
• とりわけ譫妄に関する記載が多く 重要視されていることがうかがえる
PADガイドラインの推奨事項

1. Pain and Analgesia a. Incidence of pain i. Adult medical, surgical, and trauma ICU pa2ents rou2nely experience pain, both at rest and with rou2ne ICU care (B). ii. Pain in adult cardiac surgery pa2ents is common and poorly treated; women experience more pain than men acer cardiac surgery (B). iii. Procedural pain is common in adult ICU pa2ents (B). b. Pain assessment i. We recommend that pain be rou2nely monitored in all adult ICU pa2ents (+1B). ii. The Behavioral Pain Scale (BPS) and the Cri2cal-‐Care Pain Observa2on Tool (CPOT) are the most valid and reliable behavioral pain scales for monitoring pain in medical, postopera2ve, or trauma (except for brain injury) adult ICU pa2ents who are unable to self-‐report and in whom motor func2on is intact and behaviors are observable. Using these scales in other ICU pa2ent popula2ons and transla2ng them into foreign languages other than French or English require further valida2on tes2ng (B). iii. We do not suggest that vital signs (or observa2onal pain scales that include vital signs) be used alone for pain assessment in adult ICU pa2ents (–2C). iv. We suggest that vital signs may be used as a cue to begin further assessment of pain in these pa2ents, however (+2C).
Crit Care Med 2013; 41:263–306

c. Treatment of pain i. We recommend that preemp2ve analgesia and/or nonpharmacologic interven2ons (e.g., relaxa2on) be administered to alleviate pain in adult ICU pa2ents prior to chest tube removal (+1C). ii. We suggest that for other types of invasive and poten2ally painful procedures in adult ICU pa2ents, preemp2ve analgesic therapy and/or nonpharmacologic interven2ons may also be administered to alleviate pain (+2C). iii. We recommend that intravenous (IV) opioids be considered as the first-‐line drug class of choice to treat non-‐neuropathic pain in cri2cally ill pa2ents (+1C). iv. All available IV opioids, when 2trated to similar pain intensity endpoints, are equally effec2ve (C). v. We suggest that nonopioid analgesics be considered to decrease the amount of opioids administered (or to eliminate the need for IV opioids altogether) and to decrease opioid-‐ related side effects (+2C). vi. We recommend that either enterally administered gabapen2n or carbamazepine, in addi2on to IV opioids, be considered for treatment of neuropathic pain (+1A). vii. We recommend that thoracic epidural anesthesia/ analgesia be considered for postopera2ve analgesia in pa2ents undergoing abdominal aor2c aneurysm surgery (+1B). viii. We provide no recommenda2on for using a lumbar epidural over parenteral opioids for postopera2ve analgesia in pa2ents undergoing abdominal aor2c aneurysm surgery, due to a lack of benefit of epidural over parenteral opioids in this pa2ent popula2on (0,A).
Crit Care Med 2013; 41:263–306

ix. We provide no recommenda2on for the use of thoracic epidural analgesia in pa2ents undergoing either intrathoracic or nonvascular abdominal surgical procedures, due to insufficient and conflic2ng evidence for this mode of analgesic delivery in these pa2ents (0,B). x. We suggest that thoracic epidural analgesia be considered for pa2ents with trauma2c rib fractures (+2B). xi. We provide no recommenda2on for neuraxial/ regional analgesia over systemic analgesia in medical ICU pa2ents, due to lack of evidence in this pa2ent popula2on (0, No Evidence).
Crit Care Med 2013; 41:263–306

2. Agita2on and Seda2on a. Depth of seda2on vs. clinical outcomes i. Maintaining light levels of seda2on in adult ICU pa2ents is associated with improved clinical outcomes (e.g., shorter dura2on of mechanical ven2la2on and a shorter ICU length of stay [LOS]) (B). ii. Maintaining light levels of seda2on increases the physiologic stress response, but is not associated with an increased incidence of myocardial ischemia (B). iii. The associa2on between depth of seda2on and psychological stress in these pa2ents remains unclear (C). iv. We recommend that seda2ve medica2ons be 2trated to maintain a light rather than a deep level of seda2on in adult ICU pa2ents, unless clinically contraindicated (+1B). b. Monitoring depth of seda2on and brain func2on i. The Richmond Agita2on-‐Seda2on Scale (RASS) and Seda2on-‐Agita2on Scale (SAS) are the most valid and reliable seda2on assessment tools for measuring quality and depth of seda2on in adult ICU pa2ents (B). ii. We do not recommend that objec2ve measures of brain func2on (e.g., auditory evoked poten2als [AEPs], Bispectral Index [BIS], Narcotrend Index [NI], Pa2ent State Index [PSI], or state entropy [SE]) be used as the primary method to monitor depth of seda2on in noncomatose, nonparalyzed cri2cally ill adult pa2ents, as these monitors are inadequate subs2tutes for subjec2ve seda2on scoring systems (–1B).
Crit Care Med 2013; 41:263–306
iii. We suggest that objec2ve measures of brain func2on (e.g., AEPs, BIS, NI, PSI, or SE) be used as an adjunct to subjec2ve seda2on assessments in adult ICU pa2ents who are receiving neuromuscular blocking agents, as subjec2ve seda2on assessments may be unobtainable in these pa2ents (+2B). iv. We recommend that EEG monitoring be used to monitor nonconvulsive seizure ac2vity in adult ICU pa2ents with either known or suspected seizures, or to 2trate electrosuppressive medica2on to achieve burst suppression in adult ICU pa2ents with elevated intracranial pressure (+1A). c. Choice of seda2ve i. We suggest that seda2on strategies using nonbenzodiazepine seda2ves (either propofol or dexmedetomidine) may be preferred over seda2on with benzodiazepines (either midazolam or lorazepam) to improve clinical outcomes in mechanically ven2lated adult ICU pa2ents (+2B).
Crit Care Med 2013; 41:263–306

3. Delirium
a. Outcomes associated with delirium i. Delirium is associated with increased mortality in adult ICU pa2ents (A). ii. Delirium is associated with prolonged ICU and hospital LOS in adult ICU pa2ents (A). iii. Delirium is associated with the development of post-‐ICU cogni2ve impairment in adult ICU pa2ents (B). b. Detec2ng and monitoring delirium i. We recommend rou2ne monitoring of delirium in adult ICU pa2ents (+1B). ii. The Confusion Assessment Method for the ICU (CAM-‐ICU) and the Intensive Care Delirium Screening Checklist (ICDSC) are the most valid and reliable delirium monitoring tools in adult ICU pa2ents (A). iii. Rou2ne monitoring of delirium in adult ICU pa2ents is feasible in clinical prac2ce (B). c. Delirium risk factors i. Four baseline risk factors are posi2vely and significantly associated with the development of delirium in the ICU: preexis2ng demen2a, history of hypertension and/or alcoholism, and a high severity of illness at admission (B). ii. Coma is an independent risk factor for the development of delirium in ICU pa2ents (B).
Crit Care Med 2013; 41:263–306

iii. Conflic2ng data surround the rela2onship between opioid use and the development of delirium in adult ICU pa2ents (B). iv. Benzodiazepine use may be a risk factor for the development of delirium in adult ICU pa2ents (B). v. There are insufficient data to determine the rela2onship between propofol use and the development of delirium in adult ICU pa2ents (C). vi. In mechanically ven2lated adult ICU pa2ents at risk of developing delirium, dexmedetomidine infusions administered for seda2on may be associated with a lower prevalence of delirium compared to benzodiazepine infusions (B). d. Delirium preven2on i. We recommend performing early mobiliza2on of adult ICU pa2ents whenever feasible to reduce the incidence and dura2on of delirium (+1B). ii. We provide no recommenda2on for using a pharmacologic delirium preven2on protocol in adult ICU pa2ents, as no compelling data demonstrate that this reduces the incidence or dura2on of delirium in these pa2ents (0,C). iii. We provide no recommenda2on for using a combined nonpharmacologic and pharmacologic delirium preven2on protocol in adult ICU pa2ents, as this has not been shown to reduce the incidence of delirium in these pa2ents (0,C). iv. We do not suggest that either haloperidol or atypical an2psycho2cs be administered to prevent delirium in adult ICU pa2ents (–2C). v. We provide no recommenda2on for the use of dexmedetomidine to prevent delirium in adult ICU pa2ents, as there is no compelling evidence regarding its effec2veness in these pa2ents (0,C).
Crit Care Med 2013; 41:263–306
e. Delirium treatment i. There is no published evidence that treatment with haloperidol reduces the dura2on of delirium in adult ICU pa2ents (No Evidence). ii. Atypical an2psycho2cs may reduce the dura2on of delirium in adult ICU pa2ents (C). iii. We do not recommend administering rivas2gmine to reduce the dura2on of delirium in ICU pa2ents (–1B). iv. We do not suggest using an2psycho2cs in pa2ents at significant risk for torsades de pointes (i.e., pa2ents with baseline prolonga2on of QTc interval, pa2ents receiving concomitant medica2ons known to prolong the QTc interval, or pa2ents with a history of this arrhythmia) (–2C). v. We suggest that in adult ICU pa2ents with delirium unrelated to alcohol or benzodiazepine withdrawal, con2nuous IV infusions of dexmedetomidine rather than benzodiazepine infusions be administered for seda2on to reduce the dura2on of delirium in these pa2ents (+2B).
Crit Care Med 2013; 41:263–306

4. Strategies for Managing Pain, Agita2on, and Delirium to Improve ICU Outcomes a. We recommend either daily seda2on interrup2on or a light target level of seda2on be rou2nely used in mechanically ven2lated adult ICU pa2ents (+1B).
b. We suggest that analgesia-‐first seda2on be used in mechanically ven2lated adult ICU pa2ents (+2B). c. We recommend promo2ng sleep in adult ICU pa2ents by op2mizing pa2ents’ environments, using strategies to control light and noise, clustering pa2ent care ac2vi2es, and decreasing s2muli at night to protect pa2ents’ sleep cycles (+1C). d. We provide no recommenda2on for using specific modes of mechanical ven2la2on to promote sleep in mechanically ven2lated adult ICU pa2ents, as insufficient evidence exists for the efficacy of these interven2ons (0, No Evidence). e. We recommend using an interdisciplinary ICU team approach that includes provider educa2on, preprinted and/or computerized protocols and order forms, and quality ICU rounds checklists to facilitate the use of pain, agita2on, and delirium management guidelines or protocols in adult ICUs (+1B).
Crit Care Med 2013; 41:263–306

N Engl J Med 2014;370:444-‐54.
まとめ
• 多くの文献によって鎮静、譫妄の管理が ICU患者のアウトカムを改善することが 示唆されている。
• 鎮静深度、疼痛、譫妄を評価し、それに 基づく痛みの除去、必要最低限の 鎮静の維持が推奨される。

私見
• 「行動を抑制するため眠らせる」から 「痛み、興奮、譫妄への治療的介入」としての鎮静に移行していると感じた。
• 鎮静薬は各々に明確な優位性が示されて いないため多面的な尺度から吟味して 選択する必要がある。
• 発症した譫妄の治療に関してはさらなる研究が期待される。