Women’s Advancement and Leadership in the Biomedical ......and preliminary data was presented in...
28
Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia The gender vicious cycle RESPONSIBLE RESEARCH SERIES MONOGRAPH SARIS no. 6
Transcript of Women’s Advancement and Leadership in the Biomedical ......and preliminary data was presented in...

Women’s Advancement and Leadership in the Biomedical Research Centres of CataloniaThe gender vicious cycle
RESPONSIBLE RESEARCH SERIES
MONOGRAPH SARIS no. 6

AUTHORSMaite Solans1, Paula Adam1,
César Velasco1, Pavel Ovseiko2, Eduard Güell3, Rosie Campbell4 i
Isabelle Vernos5,6 1 Àrea de Recerca, Agència de Qualitat i
Avaluació Sanitàries de Catalunya (AQuAS), Unidad Asociada al CSIC
2 INGENIO (CSIC-UPV)
3 Radcliffe Department of Medicine, University of Oxford
4 Global Institute for Women’s Leadership, King’s College of London
5 ICREA
6 Centre for Genomic Regulation (CRG) and Chair of the CRG Gender Balance
Committee
The SARIS monographs are written for decision-makers, professionals, and non-specialists and aim to analyse topical issues in biomedical research in order to stimulate and foster reflection. The present document is part of the “Responsible Research” series, which addresses the interaction between research and society.
ACKNOWLEDGEMENTSThis study was supported by la the Banking Foundation “la Caixa”, and preliminary data was presented in the Summit for Women’s Advancement and Leadership in Health Research celebrated on the 22nd of October 2019 in Girona. Special thanks to Angel Font and Ignasi López Verdaguer for their support. The authors gratefully acknowledge Joan Marsh, Deputy Editor of The Lancet Psychiatry, who provided valuable expertise about the ‘vicious cycle’, as well as Mara Dierssen, Robert Fabregat, Maria Granell, Federica Righi, Marta Segarra, Carmen Vela and Raquel Yotti for providing their knowledge and expertise in the summit. The authors are grateful to the participants of the summit for their valuable comments, and very specially to Azucena Bardají, Nuria Gavaldà, Reyes Grases, Constanza Jacques Aviñó, Emma Torelló and Anna Ribas for their special participation. Thanks go also to all the professionals from research centres who provided and validated data for this monograph. Finally, especial thanks go to Anna Llovet from the SIRECS/UNEIX and Raúl Méndez and Eduard Suñen from Research Marks Analytics.

3Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia
FOREWORD
In 2018, gender equality became a high priority in the policy agenda of
both the Department of Health of the Government of Catalonia and the
Government of Spain. AQuAS embraced this as an opportunity to take action
in alignment with the Global Call for Action to include gender in research
assessment. In collaboration with the Banking Foundation “la Caixa”, AQuAS
embarked in 2019 on a project with transformative aspirations for gender
equality in science, in line with additional global calls coming from scientific
journals and funding agencies in terms of critically rethinking the how, the
who, the what, and the why, and who in assessment practices that can play
a crucial role in making aspirational changes real.
The present monograph is the first in a series of two in which AQuAS sheds
light to the Catalan health research ecosystem from a gender perspective. The
vision is to give evidence that supports the necessary changes to make our
science a more equalitarian endeavour.
Paula AdamDirector of ResearchAgency for Health Quality and Assessment of Catalonia (AQuAS)

4 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
FOREWORD 3
EXECUTIVE SUMMARY 6
THE GENDER VICIOUS CYCLE 7
The side effect of the vicious cycle 8
‘SHE FIGURES’ IN THE CATALAN BIOMEDICAL RESEARCH CENTRES 11
Women’s advancement in career development 12
Women’s access to research funding 17
Female leadership in decision-making positions 18
Female leadership in scientific publications 22
FINAL CONSIDERATIONS 23
GLOSSARY 24
REFERENCES 25
TABLE OF CONTENTS

Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia
The gender vicious cycle
RESPONSIBLE RESEARCH SERIES
MONOGRAPH SARIS no. 6

7Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia6 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
EXECUTIVE SUMMARY
Gender is increasingly recognised as a grand challenge
of the scientific enterprise, and many important calls
for action have been issued. One poignant example is
the “Vicious cycle” that disadvantages women in
science presented by the editors of The Lancet Jocalyn
Clark and Richard Horton in February 2019. The
vicious cycle implies that women are less likely to
have leading authorship positions in publications, are
less likely to receive funding in their research, have
less access to the relevant positions and are less
frequently appointed to leadership positions and as a
consequence, all these aspects prevent women’s full
participation and contributions in biomedical research
and inevitably means that women’s opinions are less
likely to be voiced.
The data presented in this monograph pivots around
the gendered data from 19 Catalan biomedical
research centres and attempts to illustrate that the
gender challenge concerns the different issues of the
“vicious cycle”.
Data implies that women are having difficulties in
getting ahead in research careers. Biomedical research
centres have a female-dominated workforce, but a
male-dominated leadership. As careers advance, the
share declines. Finishing doctoral studies appears to
be a turning point for drawing the gender scissors in
women’s career development. However, the Catalan
setting is diverse, so four different patterns can be
observed: equalitarian pattern, equalitarian pattern
except female-dominated bottom, V-shaped male-
dominance pattern and classic scissor pattern. In sum,
women’s advancement in career development needs
major changes in a large number of centres.
Also, regarding access to funding, there is a reduced
access for women to prestigious senior fellowship
schemes and significant differences in awarded
funding by gender. In the Catalan biomedical
centres, women are underrepresented in research
decision-making bodies. Male-leadership in decision-
making bodies is highly dependent on scientific
competitiveness, while female-leadership is rather
related to managerial tasks. Finally, female-led
publications are less prominent in number of
publications. Finally, 25% of the lead publications
include diversity or female leadership in the leading
positions while 75% have only men in the leadership
positions in the first, corresponding or last author.
Further research and discussion are needed to
explore all these phenomena, and mainly to
understand the dynamics and reasons behind it.
There is a need to reflect on how organisational
contexts, cultures and regulatory settings can create
equal opportunities for women’s advancement and
to discuss which actions should be taken to remove
career barriers in competitive contexts like the
Catalan setting.
This document sheds individual data
on the gender scissors and the gender
vicious cycle for the 19 biomedical
research centres of Catalonia

7Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia6 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
THE GENDER VICIOUS CYCLE
Gender equality is increasingly recognised as a grand
challenge for scientific enterprise by some of the
most authoritative voices in the academic world.
Many academic publications, such as BMC in 2016,
1 reached approximately a quarter of a trillion US
dollars in 2010. However, not all of this investment
is distributed evenly by gender. It follows, arguably,
that scarce research resources may not be optimally
invested (by either not supporting the best science
or by failing to investigate topics that benefit
women and men equitably The Lancet in 20182
and Cell in 20193 put gender equality high on the
agenda. A very recent but highly significant example
has been the clear message of concern about the
male dominance in panels and conferences made
by Dr Francis Collins4, currently the Director of the
National Institutes of Health (NIH) of the United
States. Dr Collins announced that he would not
accept invitations to speak at conferences and
panels where diversity was not considered. The
Lancet’s theme issue on women in science, medicine,
and global health has created a momentum for
change in academic publishing. Other journals
like Cell3 have also showed determination to give
voice to gender equality. Expert male-only panels
are being challenged, and the contents of research
are increasingly being scrutinised according to
whether gender and sex dimensions are addressed
responsibly.
The editors of The Lancet, Jocalyn
Clark and Richard Horton, exposed
in February 2019 the “Vicious
cycle” that disadvantages women
in science
So, what are the issues? How is it possible that
until recently there has been no global awareness
of evident gender inequalities in science? In fact,
this is not new, and the elephant was in the room
already for a long time. According to the Women
in Research Survey 20195 by the society of Spanish
scientists in the United Kingdom (SRUK / CERU):
70% of women believe they do not have the same
opportunities for career progression as men. This
perception most probably was even greater in the
past decades and go beyond the academic and
scientific world. According to the same survey, 40%
of scientific women in Spain perceive that research
is an extremely competitive environment and this is a
too big obstacle for them. The fact is that Spain offers
one of the most adverse environments for scientific
women. The 2019 Global Talent Competitiveness
Index,6 a global benchmark of countries for issues
related to talent, competitiveness and the future
of work, includes gender equality as an analysis
category. The figures for Spain are alarming: on
leadership opportunities for women, Spain ranks
112 out of 125, being the worst mark among the
hundred analysed indicators. In addition, Spain ranks
very low in equal salaries for both genders (129 out
of 149). Furthermore, motherhood generates a glass
ceiling that hinders career advancement of women
even in countries extremely generous with family-
friendly policies and support.7
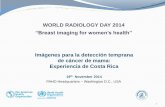
One convincing explanation on the barriers for
women’s advancement in biomedical research is the
so-called “vicious cycle“ by The Lancet8. Women
are less likely to receive funding in their research,
making it more difficult for them to access the most

9Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia8 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6 9Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia8 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
relevant positions, they receive fewer invitations to
conferences or peer review panels, they establish
less ties with other actors and as a consequence
publish in less relevant authorship positions in the
publications. Therefore, this implies poorer ratings
in curriculum evaluations, returning to the starting
point: less funding, and the circle starts again.
Overall, leadership opportunities
for women in Spain rank 112 out
of 125 countries
THE SIDE EFFECT OF THE VICIOUS CYCLE
The “vicious cycle” has an impact on the scientific
results. The consequences go beyond women’s career
advancement. A recent large study examined 1.5
million medical research papers between 2008-2015,
and found a robust link between women’s authorship
and the likelihood of a study including gender and
sex analysis: if a woman is among the authors,
it is 30% more likely that the research includes
differences per sex and gender.9
In 2010, an editorial in Nature10 highlighted the need
for including the gender perspective in the research
agenda. Specifically, the editorial pointed: “medicine
as it is currently applied to women is less evidence-
based than that being applied to men.” Moreover, it
continued: “biomedical research continues to use
many more male subjects than female in both
animal studies and human clinical trials. The
unintended effect is to short-change women’s
health care.” Gender bias in biomedicine, from basic
to translational has been identified in a number of
studies.9,11–13
The purpose of gender-oriented research is to
promote rigorous science that considers sex and
gender, and therefore has the potential to expand
our understanding of health determinants for
all people. Sex and gender are multidimensional
concepts, which means that any given individual
is affected by multiple factors, including genetics,
physiological characteristics, physical characteristics,
gender identity, gender relations, and institutional
gender.14 Given the complexity of understanding the
effects of gender and health, the intersection with
social sciences and other knowledge fields becomes
necessary.
There are several initiatives to encourage relevant
research for women, ranging from guidelines for
gendered research15 to specific research programmes
to cover gendered knowledge gaps. More recently,
governments and research agencies are adopting
legal frameworks and plans in order to implement
those initiatives.

9Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia8 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6 9Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia8 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
The ‘“vicious cycle” of women’s advancement (from Clark J et al. The Lancet 2019, 393(10171):508-10)8
If we go by parts, women’s advancement and career
development is probably the aspect of the vicious
cycle where evidence is crystal-clear. Indicators, such
as the Glass Ceiling Index (GCI), can measure vertical
segregation impact. The GCI is a relative index used
in the reports produced by the European Commission
“She Figures” on research ecosystem.16 A GCI of one
indicates there is no difference between women and
men in terms of their chances of being promoted,
and a GCI score of more than one indicates the
presence of a glass ceiling effect. At the EU level,
the GCI stood at 1.64 in 2016, 0.04 points lower
than in 2013. In all countries for which data were
available for 2016, the GCI was higher than 1.00,
indicating that women face greater difficulties than
men do in advancing to the highest research and
academic posts. Although Spain is not included in
this benchmark, there is similar evidence for medical
positions in Catalonia based on data from Hospital
Clínic of Barcelona.17 This phenomenon is known
as the “leaking pipeline”.Women tend to develop
careers later in life, and are more affected than men
by maternity and paternity leave policies. Gendered
behaviours implies that women feel discouraged in
advancing their careers or remaining in the field of
research.18
In science, women are less likely
to receive funding for their
research, they receive fewer
invitations to conferences or peer
review panels
In terms of access to research funding, gender
bias remains a disputed issue. A number of studies
show unequal access between male and female
peers, even in contexts where women completing
undergraduate and graduate training are more
numerous than men.19 The unequal access to funds
is called Mathilda effect, and can be interpreted as a
gendered version of the Mathew effect, “those who
have more will be given more”, usually interpreted

11Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia10 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
in regards to the type of science that tends to be
more successful in competitions for funding seems
to have a gender. The Mathilda effect20 is named
after the 19th century author and activist Matilda
Joslyn Gage, and highlights the historical tendency
for women’s work to be systematically omitted
and a lack of recognition. A study suggested that
female early career researchers receive significantly
less start-up support from their institutions, and as a
consequence, it would be more difficult for them to
access future research funding.21 Of course, success
rates in grant applications by gender vary significantly
according to the characteristics of the programme,
the socioeconomic context. In the case of Catalonia,
the research programme of the Department of
Health of the Government of Catalonia, called
PERIS, has been funding research and talent for
three years (2017-2019). This programme has a
broad variety of sub programmes ranging from
pre-doctoral to post-doctoral grants, projects and
large programmes. A preliminary analysis shows
inconclusive results since simple success rates
vary broadly from one programme edition to the
next. The solid fact though is only 32% of funded
principal investigators were women.22 Witteman
and colleagues’19 recommended the funders to use
project-based instead of people-based grant review
to guide research investments in order to eliminate
the influence of individual or systemic bias.
Visibility in conferences and expert panels is also
important for career development. This is why the
NIH is officially committed to end “manels” – all-
male speaking panels - in the light of The Lancet
and other calls. Similarly, the European Commission,
the NIH and many other funding agencies (i.e.
National Institutes of Health Research from the UK,
EMBO from Germany) are currently committed to
guarantee gender equality in peer review panels
where funding decisions and scientific opportunities
are addressed. However, in one study developed
in universities, they showed differences with the
perception of excellence and their application in
hiring and promotion processes, so constructions of
excellence that not involve gender ‘misrecognition’
should be developed.23
One crucial element for career development in the
scientific system is authorships in publications.
This is the keystone of advancement in scientific
careers. Being corresponding, first or last author in
original articles is the key of any scientific evaluation
system. Indistinctively of whether it uses the impact-
factor, deciles or quartiles of the journals or not,
although evaluation systems that give more weight
to the mission and context of the publications (as
suggested by the Leiden Manifesto for journals and
the Declaration of San Francisco, DORA, for funding
agencies) are certainly less gender-punitive. In the
area of oncology, the differences are significant.24
In the Cancer Journal for Clinicians, 54.1% first
authors are female whereas the percentage goes
down to 25% as last authors. In Nature Reviews
Cancer, 61.2% first authors are female but only
28.1% are last authors25.
Clark and Horton illustrate the patterns described
above with a “cycle”. Nevertheless, in some cases
one might argue that there is a vicious “circle”, rather
than a “cycle”, that traps women below the glass
ceiling. The consequence is the small improvement
over time. A larger number of women in the first
academic stages of scientific individual journeys do
not correspond to the higher presence of women in
leadership positions. All the aspects mentioned above
prevent women’s full participation and contribution
Women are less likely
to occupy relevant authorship
positions in publications

11Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia10 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
in biomedical research, representing an unacceptable
masking of women’s contribution to research. The
scarcity of women in leadership positions inevitably
means that women’s opinions are less likely to be
voiced, and as a consequence may lead to biased
decision-making. Implicit gender bias in performance
assessment or gender stereotypes, for example,
can influence women’s career advancement and
development.16 Path dependency and implicit biases
are argued to be the bottom line of a system that has
been historically male-driven.26 The notion of path
dependency, which originates in political science,
suggest that current actions depend on existing and
past experiences and decisions. 27 Path dependency in
gender bias applies to institutions, policy applications,
practices, beliefs and written or unwritten rules of
behaviour that structure modern science and society
and may explain the persistence of a glass-ceiling
effect in science. These are often influenced by both
conscious and unconscious gender bias.
‘SHE FIGURES’ IN THE CATALAN BIOMEDICAL RESEARCH CENTRES
The accountability tool of the Department of
Health for the 19 biomedical research centres is
the Outcomes Scoreboard or “Central de Resultats
de Recerca”, which publishes individual data on
resources, transfer and outcomes every two years.
The biomedical research centres included in the
outcomes scoreboard are:
Healthcare-based biomedical research centres Other biomedical research centres
IDIAP Jordi Gol: Institute for Research in Primary Care
CMRB: Center of Regenerative Medicine of Barcelona
IDIBAPS: August Pi i Sunyer Biomedical Research Institute CRG: Centre for Genomic Regulation
IDIBELL: IBellvitge Biomedical Research Institute IBEC: Institute for Bioengineering of Catalonia
IDIBGI: Girona Biomedical Research Institute
ICC: Catalan Institute of Cardiovascular Sciences
IGTP: “Germans Trias i Pujol” Health Sciences Research Institute
IJC: Josep Carreras Leukaemia Research Institute
IRSantPau: Sant Pau Biomedical Research Institute IRB: Institute for Research in Biomedicine
IISPV: Pere Virgili Health Research Institute IRSICAIXA: IrsiCaixa AIDS Research Institute
IMIM: Hospital del Mar Medical Research Institute ISGLOBAL: Barcelona Institute for Global Health
IRBLleida: Biomedical Research Institute of Lleida
VHIO: Vall d’Hebron Institute of Oncology
VHIR: Vall d’Hebron Research Institute
The following chapter pivots around the gendered data from 2017-2018 and attempts to illustrate the “vicious
cycle” described by Jocalyn Clark and Richard Horton.

13Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia12 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
Indicators of the “vicious cycle” of women’s advancement in the Catalan biomedical research centres
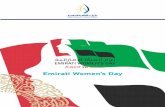
WOMEN’S ADVANCEMENT IN CAREER DEVELOPMENT
investigators and group leaders. Aggregated figures
for the 19 institutes with 8,380 people (head counts,
55% were women) by gender shows a crystal-clear
scissor from 2014 to 2017. Scientific workforce is
74% female-dominated in the early ranks of the
professional categories (technical assistants) not
changing through the four analysed years. The
percentage is slightly lower for trainees (doctoral
candidates), reaching round equality (50%) among
doctoral researchers. It is right after the training
track that the shares switch into an increasingly
male-dominated workforce, although the total
numbers are of course smaller. Finishing doctoral
The share of women
is higher in the early stages
of scientific careers. The turning
point is the end of the doctoral
studies. Leadership positions are
dominated by men
The outcomes scoreboard tool for the Catalan
research system groups the scientific workforce
into five categories: technical assistant, trainees
(doctoral candidates), doctoral researcher, principal

13Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia12 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
studies seems to be the turning point, although in
total the numbers of women who have completed
a doctorate program and started a research career
has increased significantly in recent years. The
improvement of female under-representation for the
post-doctoral positions is nevertheless insufficient
The Gender Scissors of Catalan biomedical research centres, 2014-2017
the denominators are too low. Individual figures
from 2017 show an overall share of women around
50% of the workforce in every institute (except ICCC
and VHIO). Again, the scissors diagrams illustrate
the dimension of the inequalities in many centres,
although there are few exceptions. Individual figures
show four different patterns for women’s career
advancement in the centres:
1. Equalitarian (4% of the total workforce):
centres where gender differences are within the
equality stripe of 40-60 for all categories and the
share of women is higher. This is the case with
Are there any significant differences between
centres? Can we identify patterns in the development
of the workforce through the professional categories
by gender? The disadvantage of disaggregated data
by centre is that, at least for the leadership positions,
considering the overall figures of feminisation of the
biomedical science workforce in Catalonia. That is to
say, the latest data collected for 2017 shows a slight
opening of the scissors but the magnitude of the
imbalance is still far from a gender-equality scenario
marked by the equality stripe of 40% to 60%.
More than 60% of the workforce
is placed in centers with a classical
gender scissor shape -usually
larger centers

15Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia14 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
IDIAPJGol, a centre for primary care research and
female-dominant in all categories and the IJC, a
research centre devoted exclusively to leukaemia
and other malignant blood diseases.
2. Equalitarian except female-dominated
bottom (19% of the workforce): centres where
gender inequalities are present at the bottom of
the professional scale but reach the equality stripe
among trainee researchers (doctoral candidates)
or PhD/doctoral researchers: IISPV, IRBLleida,
VHIO, CMRB, and ISGLOBAL.
3. Classic scissors (63% of the workforce): In
these centres, the lower categories are unequal
beyond 80 to 20 % differences, the scissor cutting
point is at the transition from doctoral researcher
to principal investigator and the upper leading
categories reach inequalities beyond 20% to
80%. This is the case of a great number of the
hospital-based centres: IDIBAPS, IDIBELL, IGTP,
IMIM, IDIBGI, IRSantPau, VHIR and IRSICaixa.
4. V-shaped male-dominance (14% of the
workforce): these centres are within the equality
stripe for the bottom positions but the differences
reach inequality levels for the doctoral researchers
category (CRG) or the principal investigators (IRB,
and IBEC).
There is one exception to this four rules related
to the ICCC (currently associated to IRSantPau)
where women are in greater proportions in all the
categories. In this centre, women represent 76% of
the employees.
Gender scissors in hospital-based biomedical research centres (percent of total), 2017
T/A: Technician/Assistant; TR: Trainee researcher (doctoral candidates); pHD / Doctoral researcher; PI: Principal investigator; GL: Group leader

15Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia14 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
T/A: Technician/Assistant; TR: Trainee researcher (doctoral candidates); pHD / Doctoral researcher; PI: Principal investigator; GL: Group leader
Gender scissors in hospital-based biomedical research centres, 2017 (continuation)
VHIO: n=398; 70% women

17Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia16 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
T/A: Technician /Assistant; TR: Trainee researcher (doctoral candidates); pHD / Doctoral researcher; PI: Principal investigator; GL: Group leader
Gender scissors in other biomedical research centres, 2017

17Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia16 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
In conclusion, biomedical research centres have
a female-dominated workforce directly related to
research (55%) but a male dominated leadership.
One might argue that the 23% of the workforce
that work in equalitarian environments are in
comparatively less competitive environment (outside
Barcelona, or small centres). This is consistent with
the results of the Women in Research Survey (4),
that revealed that 40% of scientific women in Spain
remark that research is an extremely competitive
environment perceived as too big of an obstacle.
The gender scissors presented in this monograph are
based on professional categories and do not reflect
pay differences related to real work.
WOMEN’S ACCESS TO RESEARCH FUNDING
One of the most prestigious human capital
fellowships in Catalonia are the ICREA grants (Catalan
Institution for Research and Advanced Studies).
ICREA fellowships are extremely competitive, aimed
at scientists with an outstanding international
research record and leadership track record, and a
strong focus on publications track. Results flagged
up strong gender differences among the recipents of
this fellowship. In 2017, there were 59 new fellows
within the 19 research centres, including only 11
females (19%). The following chart presents the
share of ICREA grants by gender in 14 biomedical
research centres. Only two centres have a significant
number of female ICREA fellows (CRG and IRB). Yet,
five centres do not have any.
Number of ICREA grantees of 14 biomedical research centres*, 2017
*Those centres that are not in the figure do not have any ICREA fellowship
An example of female difficulties
for carrier advancement is the
ICREA felowships
Another level of evaluation of the outcome of
research is the average level of funding per principal
investigator, defined as the proportion between the
amount of funding obtained and the number of
principal investigators. This average can be calculated
separately for proposals whose principal investigator
is male or female. The indicator shows a diverse
situation in the different centres. On average, the
amount of money obtained per principal investigator
was higher or equalitarian for women led-projects
in a few centres: ICC, ISGLOBAL, IISPV and VHIR.
The opposite was observed for a larger number of
centres. Gender disparities in research funding were
also found in the average amount granted, which was
lower for women-led projects (€72,423.77 versus

19Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia18 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
€125,065.39; F statistic <0.005). Nevertheless, we
should be cautious about considering that men get
more funding than women without considering the
funding success rates, or the number of principal
investigators by gender that submit an application
to competitive calls. Our results could fail to capture
the overall research success of female principal
investigators.
FEMALE LEADERSHIP IN DECISION-MAKING POSITIONS
Lack of female-leadership in
decision-making bodies is
highly dependent on scientific
competitiveness
Decision-making and leadership in biomedical
research centres has been divided in three hierarchical
levels, following the classification used in previous
studies based on an international benchmark of
large hospital-based structures.28 The classification
includes three levels and the data were gathered for
2018: the ‘top level’ includes the directors/CEO and
the external scientific committee, the ‘middle level’
refers to the internal scientific committee and the
coordinators of the scientific areas. Finally, the ‘lower
level’ is related to group leaders, platform coordinators
and managing services managers. The positions that
require (at least in the Catalan and Spanish research
system) a very highly competitive scientific skills are
the members of the direction committee, external
scientific committee, coordinators of scientific
areas and group leaders. The positions that require
managerial leadership skills and therefore are less
dependent on scientific curricula are: management
committee, internal scientific committee, platform
coordinators and service managers. Male leadership
in directive and management responsibilities
is therefore highly dependent on scientific
competitiveness. Female-leadership is rather
related to managerial tasks.
Average amount of competitive funding per principal investigators by gender, 2017*
*The amounts do not include institutional competitve funding obtained

19Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia18 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
Gender differences in scientific and managing positions and dependence from publication-record merits, 2018
While the overall share of women in the different
directing and leadership positions seems to be
related to the dependence on scientific records
of these positions, differences between centres
are significant. While there are centres with a
clear gender dominance (IJC for men and CMRB
for women) or equalitarian (ISGLOBAL) across all
positions, the vast majority have a male dominance
in the lower, middle and higher level, especially in
the positions more dependent on the scientific
records of the researcher.

21Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia20 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
Gen
der
dif
fere
nce
s in
sci
enti
fic
lead
ersh
ip a
nd
man
agem
ent
po
siti
on
s b
y ce
ntr
e, 2
018

21Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia20 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
Gen
der
dif
fere
nce
s in
sci
enti
fic
lead
ersh
ip a
nd
man
agem
ent
po
siti
on
s b
y ce
ntr
e, 2
018
(co
nti
nu
atio
n)
Fem
ale-
lead
ersh
ip is
rel
ated
to
man
ager
ial t
asks

23Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia22 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
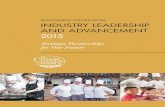
FEMALE LEADERSHIP IN SCIENTIFIC PUBLICATIONS
Becoming principal investigator (PI) is an important
milestone in scientific carriers. In that sense, the
Catalan biomedical and health research centers
present, in average, an equalitarian scenario with
44% of PI being women. The analysis of gender
in scientific publications’ leading positions shows
however a less equalitarian landscape. In a list
of authorship names, let us consider ‘leading
positions’ the first author, the corresponding author
and/or the last author. The following chart shows
an analysis of the publications that are led by
researchers of the centers. Leadership of scientific
publications includes the following positions in
the list of authors: fist author, last author and / or
corresponding author. The number of “female-led
publications” includes publications where at least
one of the three positions is occupied by a woman.
This is compared with “male-only” publications,
which is the number of publications where the three
positions are occupied by men. In fact, the opposite
to female-led publications are publications that are
led only by men. The chart shows that female-led
publications represent between 20% to 30% of the
total number of publications lead by authors of the
centers (25% is the average). That is to say, 75% of
the publications that are lead by researchers of the
centers include only men in the leadership positions.
Gender differences in leadership of publications
Only in 25% of the lead
publications include diversity
or female leadership in
the leading positions

23Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia22 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
FINAL CONSIDERATIONS
This document shows data for the Catalan health
research ecosystem that confirms the vicious cycle
described by The Lancet. In particular, inequalities
are shown in relation to:
– Career advancement and development after PhD
– Relevant positions of publications authorship
– Access to competitive funding (especially
prestigious fellowships)
– Decision-making positions that are highly
dependent on publication records (male-
dominated)
– Managerial decision-making positions (female
dominated)
While there is a wide range of differences across
the 19 analysed centres, these differences suggest
once again that research cannot reach its full
potential unless it can benefit from the talents of all.
Data suggests that comparatively less competitive
environments (outside Barcelona, or small centres)
tend to be more equalitarian. The differences
between genders will not simply diminish over time,
as the underlying factors of the vicious cycle reinforce
each other. There is evidence suggesting the need
to take actions to break the glass ceiling that limits
women’s opportunities and gender equality policies
remain important to discontinue the vicious cycle.
Further research and discussion are needed to explore
all these phenomena, and mainly to understand the
dynamics and reasons behind it, including research
on organisational contexts, cultures and regulatory
settings as means to favour equal opportunities for
women’s career advancement.
Nominal data from the 19 biomedical
research centres shows a clear-cut pattern
of a vicious cycle that difficults cientific
women’s advancement and leadership, as
described in the literature as the ‘gender
vicious cycle’

25Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia24 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
GLOSSARY
Research centre: these are institutions where
research activities are carried out. Healthcare-
based biomedical research centres differ from
other biomedical research centres because they are
associated with a hospital or primary care centre.
This potentiates the dual role of healthcare centres
as research centres.
Technician / Assistant: personnel, with different
degrees of qualification, who participate and can
undertake scientific and technical tasks, laboratory
tasks, office tasks or secretarial tasks, who participate
in research projects or is directly associated .
Trainee researcher (doctoral candidates):
researchers that do research under supervision in
the research centre and are in the process of getting
their doctorate degree.
Equality stripe: range of values that represent an
equal state or standard (40%-60%).
Group leader: researcher leading his/her research
area or field.
Leading author of the publication: authors that
are located in the first, last or corresponding author
position in a publication.
Female-led publications mean that at least one
woman is in one of these positions
Only-male leadership in publications represent
those publications where leadership positions are
occupied only by men.
PhD / Doctoral researcher: researchers that
hold a PhD or equivalent level of experience and
competence. They can have developed, or not, some
level of independence.
Principal investigator: researches that are leading
at least one research grant the same year of the
evaluation.

25Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia24 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
REFERENCES
11. Beery, A. K. & Zucker, I. Sex bias in neuroscience
and biomedical research. Neurosci. Biobehav.
Rev. 35, 565–72 (2011).
12. Hawkes, S., Haseen, F. & Aounallah-Skhiri, H.
Measurement and meaning: reporting sex in
health research. Lancet (London, England) 393,
497–499 (2019).
13. Sugimoto, C. R., Ahn, Y.-Y., Smith, E., Macaluso,
B. & Larivière, V. Factors affecting sex-related
reporting in medical research: a cross-disciplinary
bibliometric analysis. Lancet (London, England)
393, 550–559 (2019).
14. Holdcroft, A. Integrating the dimensions of sex
and gender into basic life sciences research:
methodologic and ethical issues. Gend. Med. 4
Suppl B, S64-74 (2007).
15. Clayton, J. A. Studying both sexes: a guiding
principle for biomedicine. FASEB J. 30, 519–524
(2016).
16. European Commission. She Figures 2018.
Report (2019). doi:10.2777/936
17. Arrizabalaga, P., Abellana, R., Viñas, O., Merino,
A. & Ascaso, C. Gender inequalities in the
medical profession: are there still barriers to
women physicians in the 21st century? Gac.
Sanit. 28, 363–368 (2014).
18. Structural change in research institutions:
Enhancing excellence, gender equality and
efficiency in research and innovation.
(Directorate-General for Research and
Innovation, 2011). doi:10.2777/73084
19. Raymond, J. L. & Goodman, M. B. Funders
should evaluate projects, not people. Lancet
393, 494–495 (2019).
1. Ovseiko, PV., Adam, P. et al. A global call for
action to include gender in research impact
assessment. Heal. Res. Policy Syst. 14, 50
(2016).
2. González-Alvarez, J. Author gender in The
Lancet journals. Lancet (London, England) 391,
2601 (2018).
3. Narasimhan, S. D. A Commitment to Gender
Diversity in Peer Review. Cell 179, 1–2 (2019).
4. Time to End the Manel Tradition | National
Institutes of Health (NIH). Available at: https://
www.nih.gov/about-nih/who-we-are/nih-
director/statements/time-end-manel-tradition.
(Accessed: 1st October 2019)
5. Kingdom, U. 2019 SRUK Survey on Gender
Equality in Research. (2019).
6. INSEAD. The Global Talent Competitiveness
Index 2019 Entrepreneurial Talent and Global
Competitiveness. (2019).
7. Kleven, H., Landais, C. & SSgaard, J. E. Children
and Gender Inequality: Evidence from Denmark.
SSRN Electron. J. (2018). doi:10.2139/
ssrn.3113273
8. Clark, J. & Horton, R. What is The Lancet doing
about gender and diversity? Lancet (London,
England) 393, 508–510 (2019).
9. Nielsen, M. W., Andersen, J. P., Schiebinger, L. &
Schneider, J. W. One and a half million medical
papers reveal a link between author gender and
attention to gender and sex analysis. Nat. Hum.
Behav. 1, 791–796 (2017).
10. Putting gender on the agenda. Nature 465,
665–665 (2010).

27Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia26 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6
20. Rossiter, M. W. The Matthew Matilda Effect in
Science. Soc. Stud. Sci. 23, 325–341 (1993).
21. Sege, R., Nykiel-Bub, L. & Selk, S. Sex differences
in institutional support for junior biomedical
researchers. JAMA - J. Am. Med. Assoc. 314,
1175–1177 (2015).
22. Sistema d’Avaluació de Recerca i la Innovació
en Salut SARIS. Central de Resultats de Recerca.
Convocatòries PERIS. Any 2019. (2019).
23. O’Connor, P. & O’Hagan, C. Excellence in
university academic staff evaluation: a
problematic reality? Stud. High. Educ. 41,
1943–1957 (2016).
24. Sidhu, R. et al. The gender imbalance in
academic medicine: a study of female authorship
in the United Kingdom. J. R. Soc. Med. 102,
337–342 (2009).
25. ESMO Women for Oncology ( W4O ) authorship
study. 38 (2017).
26. HARDING, S. The Science Question in Feminism.
(Cornell University Press, 1986).
27. Wilsford, D. Path Dependency, or Why History
Makes It Difficult but Not Impossible to Reform
Health Care Systems in a Big Way. Journal of
Public Policy 14, 251–283
28. Kuhlmann, E. et al. Closing the gender
leadership gap: a multi-centre cross-country
comparison of women in management and
leadership in academic health centres in the
European Union. Hum. Resour. Health 15, 2
(2017).

27Women’s Advancement and Leadership in the Biomedical Research Centres of Catalonia26 RESPONSIBLE RESEARCH SERIESMONOGRAPH SARIS no. 6

This study was supported by
la Fundació Bancària “la Caixa”
Publisher: Agència de Qualitat i Avaluació Sanitàries de Catalunya (AQuAS)/Agency for Health Quality and Assessment of Catalonia (AQuAS). Departament de Salut/Catalan Ministry of Health, Generalitat de Catalunya/Government of Catalonia
First issue: Barcelona, febrer 2020
Designer: Joana López-Corduente
Portrait illustration:
Some rights reserved: © 2020, Generalitat de Catalunya. Agència de Qualitat i Avaluació Sanitàries de Catalunya
The contents of this work are under a license Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
This license can be accessed at: https://creativecommons.org/licenses/by-nc-nd/4.0/deed.en
The Agency for Health Quality and Assessment of Catalonia (AQuAS)
is part of the Catalan Ministry of Health. Its job is to carry out
data assessment and analysis, and to generate relevant, reliable
information to be used in decision-making processes. AQuAS is
committed to promoting health and to enhancing the sustainability
of the Catalan health system. AQuAs is a founding member of the
International Network of Agencies of Health Technology Assessment
(INAHTA) and the International School on Research Impact
Assessment (ISRIA), corporate member of the Health Technology
Assessment International (HTAi), of the Reference site group “Four
Stars” of the European Innovation Partnership on Active and Healthy
Ageing of the European Commission.
If you are interested in this report you can contact us:
Agència de Qualitat i Avaluació Sanitàries de CatalunyaRoc Boronat, 81-95 (Second floor).
08005 Barcelona (Spain)
Tel.: 00 34 93 551 38 88 | Fax: 00 34 93 551 75 10 |
http://aquas.gencat.cat