
September 2012 NIA WOCN - Todo Grass Sintético · September 2012 NIA WOCN 2 ! Pressure on muscle...
25
September 2012 NIA WOCN 1 Joyce Black, PhD, RN, DNP (Hon),CWCN, FAAN Associate Professor, University of Nebraska Medical Center Causes of pressure ulcers ◦ Deep tissue injury etiology ◦ Friction out ◦ Microclimate in Intertriginous Dermatitis Deep Tissue Injury ◦ Pathophysiology Biofilms ◦ Silver Resistance? Pressure ◦ Perpendicular force in excess of capillary flow to tissues, hypoxia develops and tissue dies Shear ◦ Pull and stretch blood vessels as tangential force is applied to tissue, tissue becomes hypoxic Friction is no longer seen as an etiology No pressure component Heat builds up and leads to blistering
Transcript of September 2012 NIA WOCN - Todo Grass Sintético · September 2012 NIA WOCN 2 ! Pressure on muscle...
September 2012 NIA WOCN
1
Joyce Black, PhD, RN, DNP (Hon),CWCN, FAAN Associate Professor,
University of Nebraska Medical Center
} Causes of pressure ulcers ◦ Deep tissue injury etiology ◦ Friction out ◦ Microclimate in
} Intertriginous Dermatitis } Deep Tissue Injury ◦ Pathophysiology
} Biofilms ◦ Silver Resistance?
} Pressure ◦ Perpendicular force in excess
of capillary flow to tissues, hypoxia develops and tissue dies
} Shear ◦ Pull and stretch blood vessels
as tangential force is applied to tissue, tissue becomes hypoxic � Friction is no longer seen as an
etiology � No pressure component � Heat builds up and leads to
blistering
September 2012 NIA WOCN
2
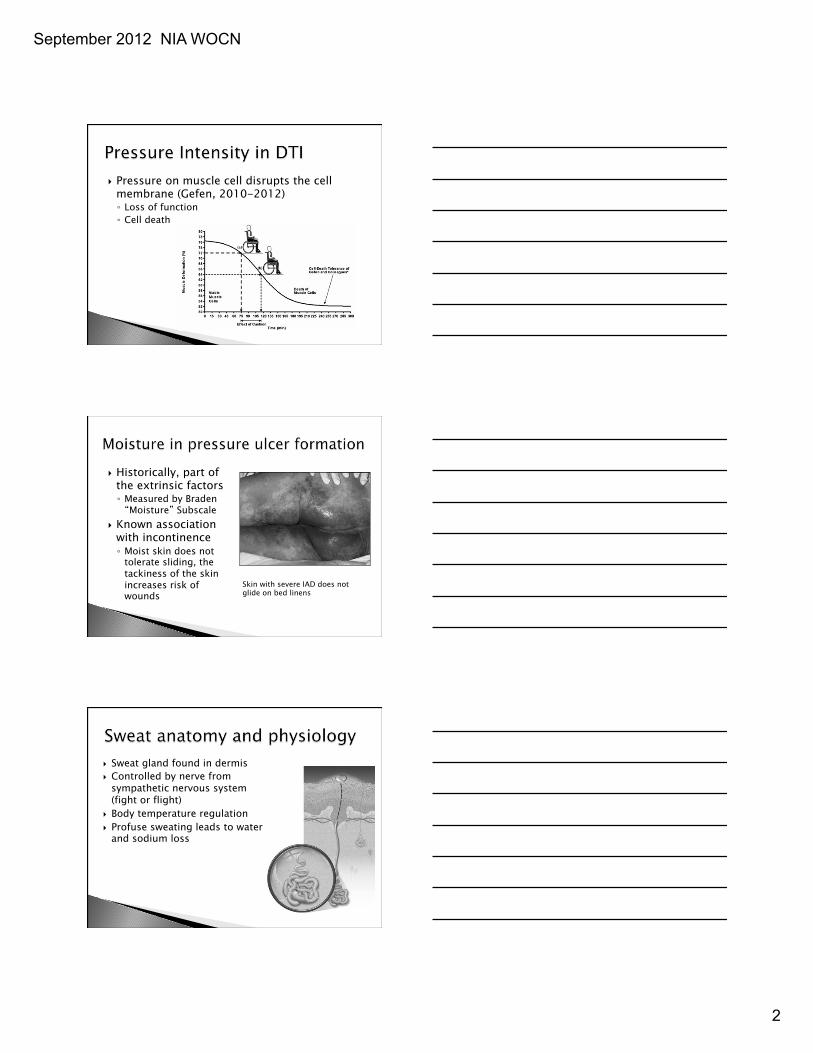
} Pressure on muscle cell disrupts the cell membrane (Gefen, 2010-2012) ◦ Loss of function ◦ Cell death
} Historically, part of the extrinsic factors ◦ Measured by Braden “Moisture” Subscale
} Known association with incontinence ◦ Moist skin does not
tolerate sliding, the tackiness of the skin increases risk of wounds
Skin with severe IAD does not glide on bed linens
} Sweat gland found in dermis } Controlled by nerve from
sympathetic nervous system (fight or flight)
} Body temperature regulation } Profuse sweating leads to water
and sodium loss
September 2012 NIA WOCN
3
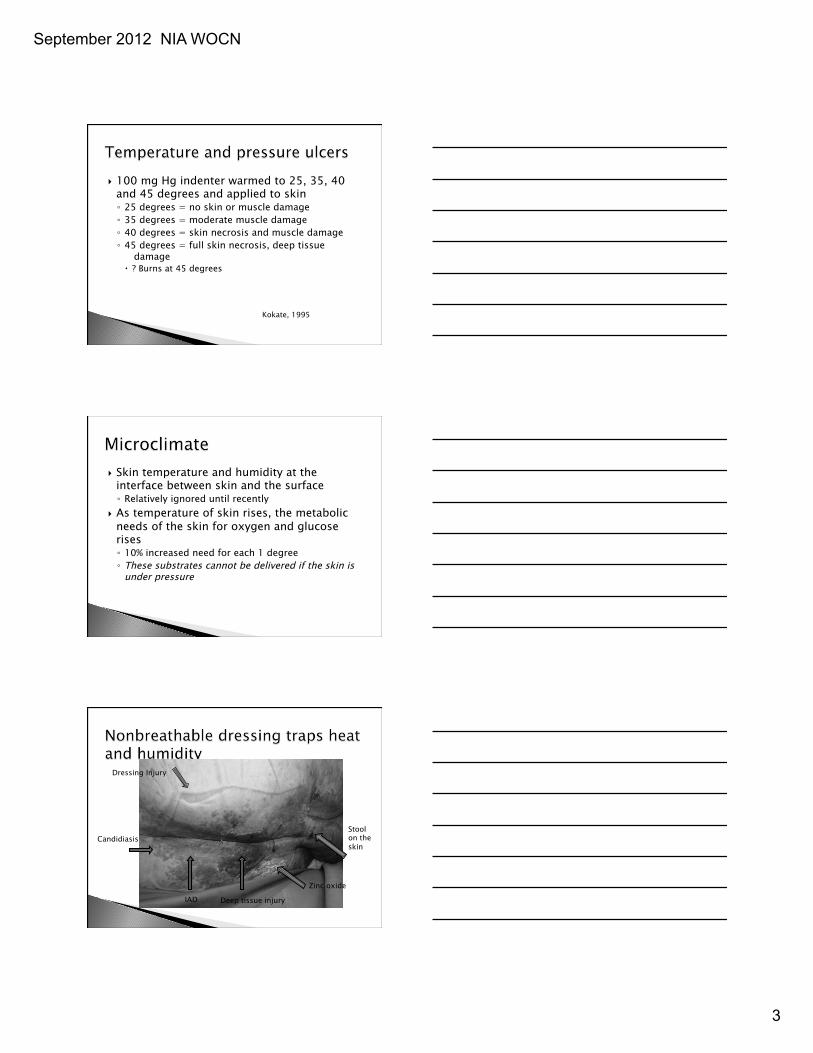
} 100 mg Hg indenter warmed to 25, 35, 40 and 45 degrees and applied to skin ◦ 25 degrees = no skin or muscle damage ◦ 35 degrees = moderate muscle damage ◦ 40 degrees = skin necrosis and muscle damage ◦ 45 degrees = full skin necrosis, deep tissue
damage � ? Burns at 45 degrees
Kokate, 1995
} Skin temperature and humidity at the interface between skin and the surface ◦ Relatively ignored until recently
} As temperature of skin rises, the metabolic needs of the skin for oxygen and glucose rises ◦ 10% increased need for each 1 degree ◦ These substrates cannot be delivered if the skin is
under pressure
Dressing Injury
Candidiasis
Deep tissue injury IAD
Zinc oxide
Stool on the skin
September 2012 NIA WOCN
4
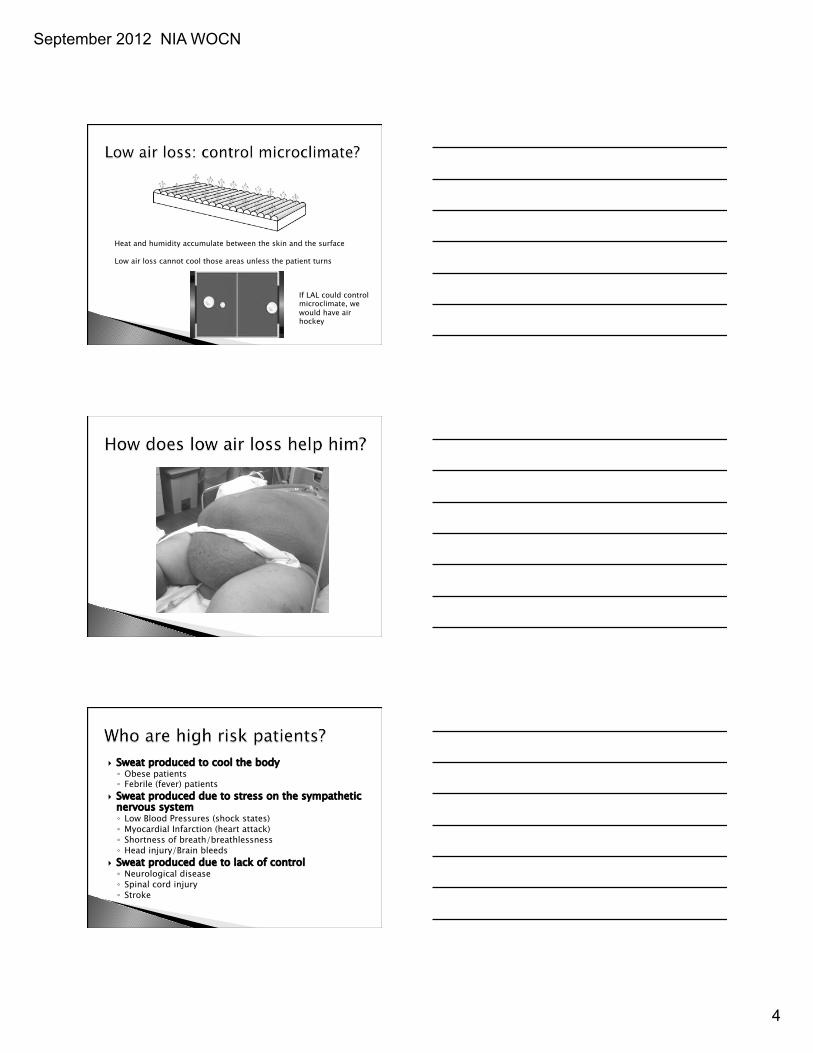
Heat and humidity accumulate between the skin and the surface Low air loss cannot cool those areas unless the patient turns
If LAL could control microclimate, we would have air hockey
} Sweat produced to cool the body ◦ Obese patients ◦ Febrile (fever) patients
} Sweat produced due to stress on the sympathetic nervous system ◦ Low Blood Pressures (shock states) ◦ Myocardial Infarction (heart attack) ◦ Shortness of breath/breathlessness ◦ Head injury/Brain bleeds
} Sweat produced due to lack of control ◦ Neurological disease ◦ Spinal cord injury ◦ Stroke
September 2012 NIA WOCN
5
} Or is the damage from moisture?
Presumption was that skin folds would grown Candida
Literature suggests that skin fold can also contain
Pseudomonas Staphyloccus
September 2012 NIA WOCN
6
} Patients with skin folds seen on admission
} History included conditions that could impair skin and increase infection
} Cultures taken of skin folds before use of InterDry
Pannus: Staphyoloccus coag neg Proteus mirabilis Enterococcus faecalis Candida albicans Escherichia coli
Axilla: Proteus mirablilis Enterococcus faecalis Staphlococcus coag neg Candida albicans VRE
Breast: Proteus mirabilis Staphyoloccus coag neg Diphtheroids
Groin: Staphyoloccus coag neg Candida albicans Diptheroids Proteus mirablis Enterococcus faecalis
Knee: Proteus mirablilis Staphylococcus coag neg
} Incisions placed through skin folds? } Bathing of skin folds and contamination of
surgical sites? ◦ Bath basins heavily contaminated
} Pretreatment of surgical sites? ◦ Really unable to clean patients in preop ◦ Unable to use chlorhexidine on open skin
September 2012 NIA WOCN
7
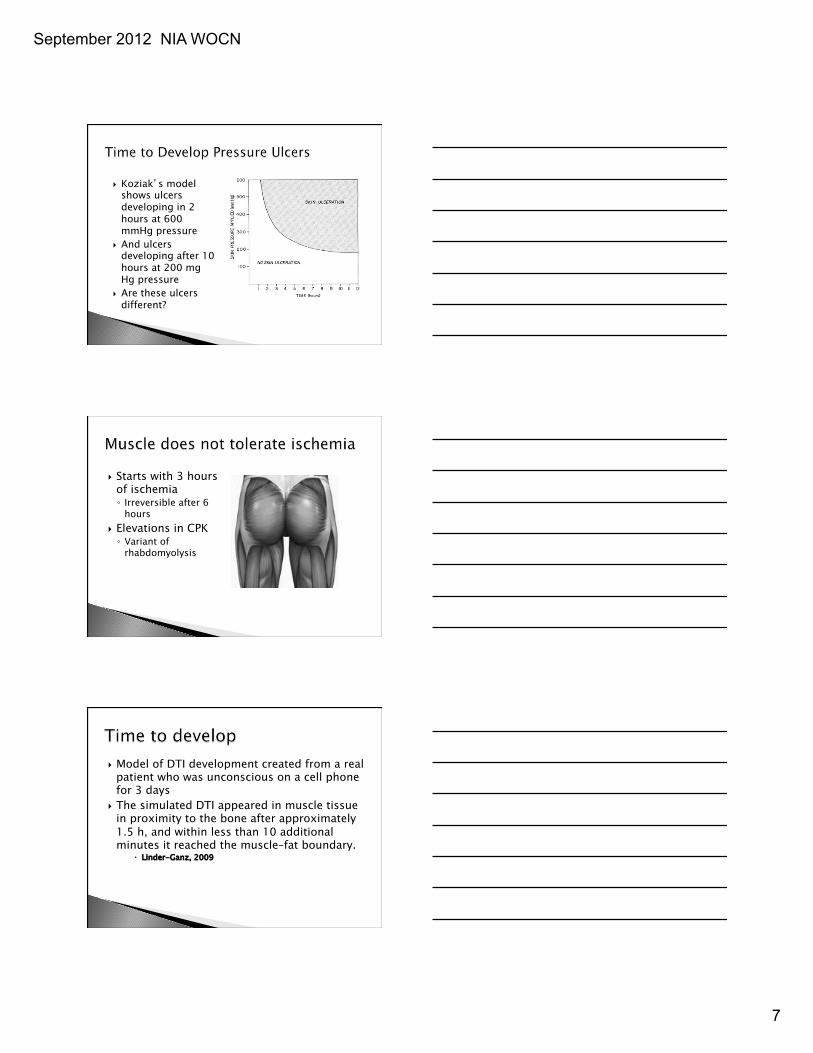
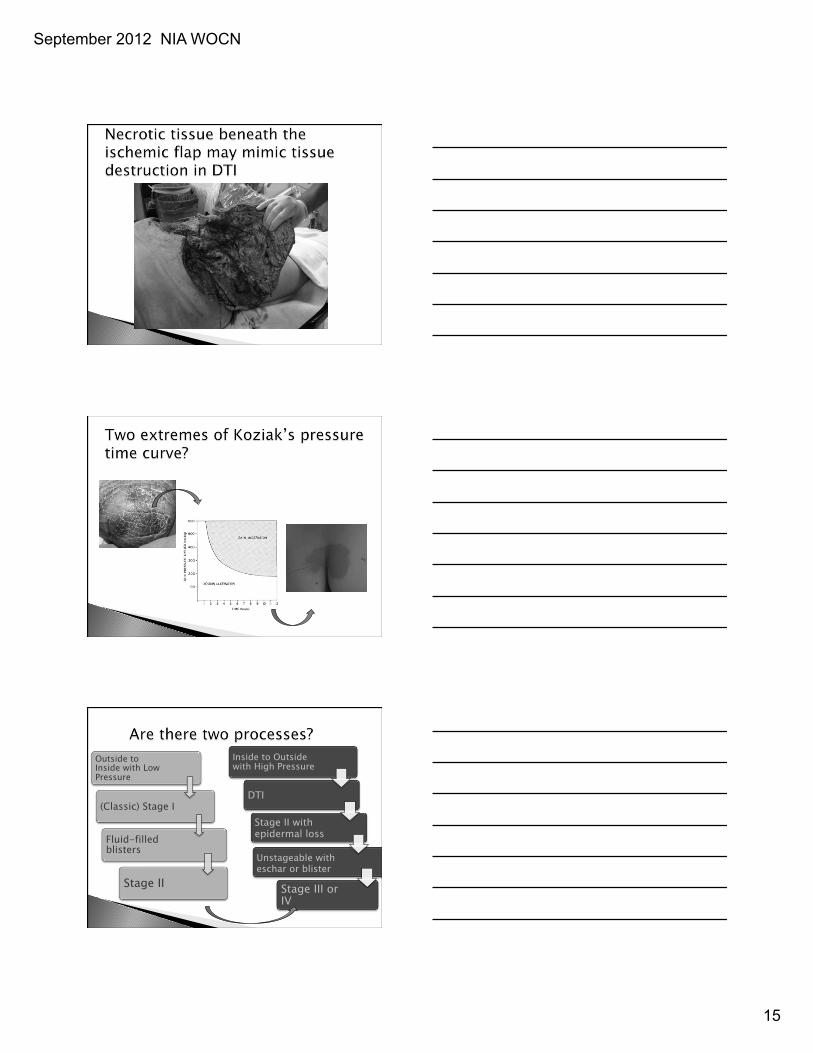
} Koziak’s model shows ulcers developing in 2 hours at 600 mmHg pressure
} And ulcers developing after 10 hours at 200 mg Hg pressure
} Are these ulcers different?
} Starts with 3 hours of ischemia ◦ Irreversible after 6
hours } Elevations in CPK ◦ Variant of
rhabdomyolysis
} Model of DTI development created from a real patient who was unconscious on a cell phone for 3 days
} The simulated DTI appeared in muscle tissue in proximity to the bone after approximately 1.5 h, and within less than 10 additional minutes it reached the muscle–fat boundary.
� Linder-Ganz, 2009
September 2012 NIA WOCN
8
} An event of confinement always preceded the first notation of purple skin by 48 hours
} Within 48 hours of the identification of purple skin, blisters were noted from epidermal sloughing ◦ Thin blisters, not fluid filled ◦ Often called “Stage II” pressure ulcers
Black, Berke, 2005
} Area sustaining highest pressures is infarcted } Surrounded by rings of ischemic and injured
tissue that is rescuable }
} Pressure creates the injury } Shear extends it to other tissue ◦ Undermining ◦ Extension
September 2012 NIA WOCN
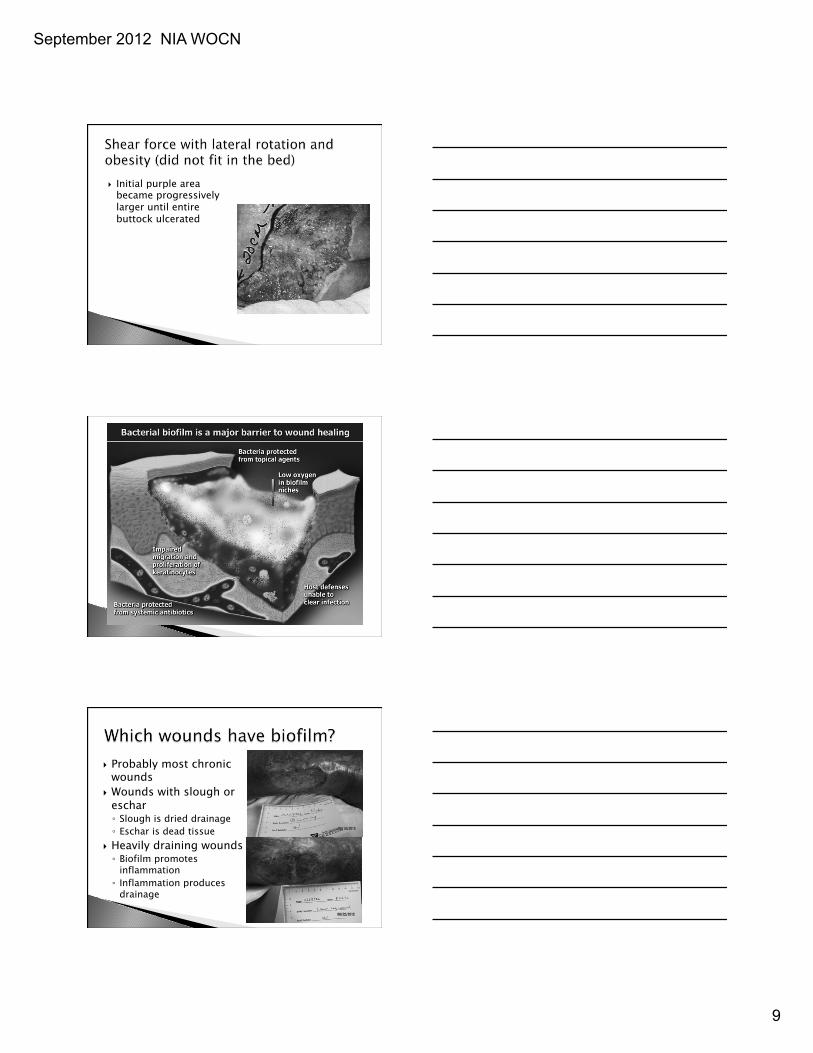
9
} Initial purple area became progressively larger until entire buttock ulcerated
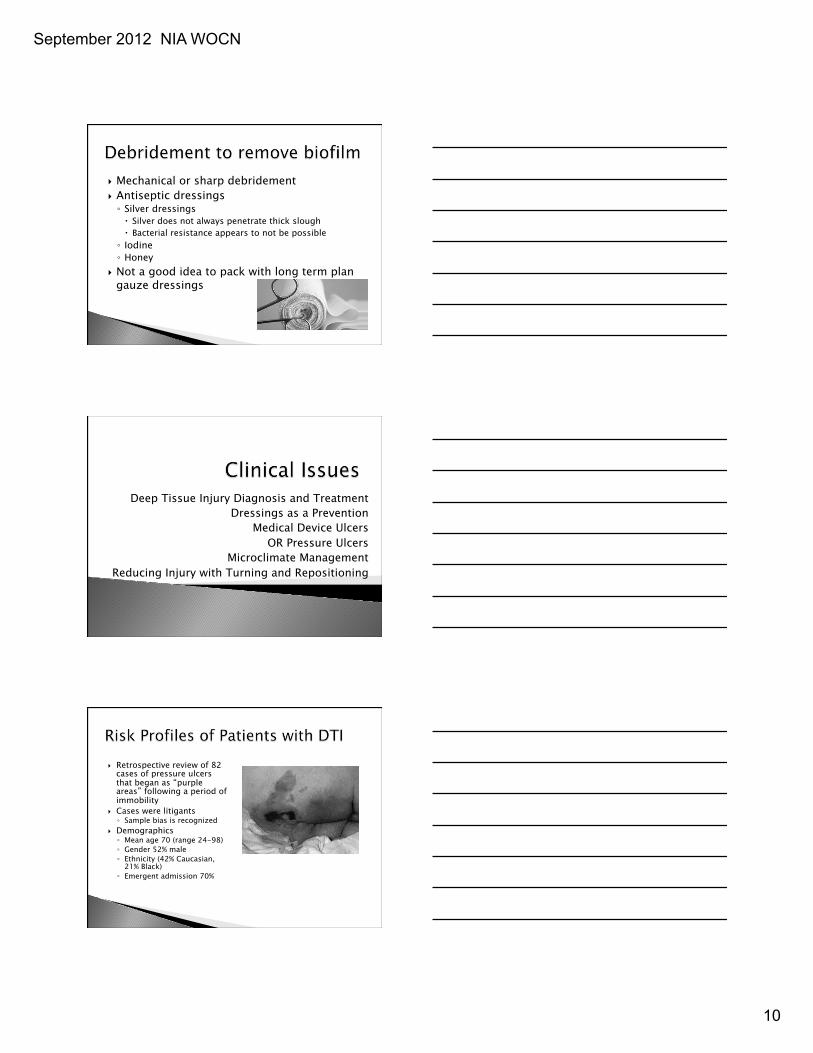
} Probably most chronic wounds
} Wounds with slough or eschar ◦ Slough is dried drainage ◦ Eschar is dead tissue
} Heavily draining wounds ◦ Biofilm promotes
inflammation ◦ Inflammation produces
drainage
September 2012 NIA WOCN
10
} Mechanical or sharp debridement } Antiseptic dressings ◦ Silver dressings � Silver does not always penetrate thick slough � Bacterial resistance appears to not be possible ◦ Iodine ◦ Honey
} Not a good idea to pack with long term plan gauze dressings
Deep Tissue Injury Diagnosis and Treatment Dressings as a Prevention
Medical Device Ulcers OR Pressure Ulcers
Microclimate Management Reducing Injury with Turning and Repositioning
} Retrospective review of 82 cases of pressure ulcers that began as “purple areas” following a period of immobility
} Cases were litigants ◦ Sample bias is recognized
} Demographics ◦ Mean age 70 (range 24-98) ◦ Gender 52% male ◦ Ethnicity (42% Caucasian,
21% Black) ◦ Emergent admission 70%
September 2012 NIA WOCN
11
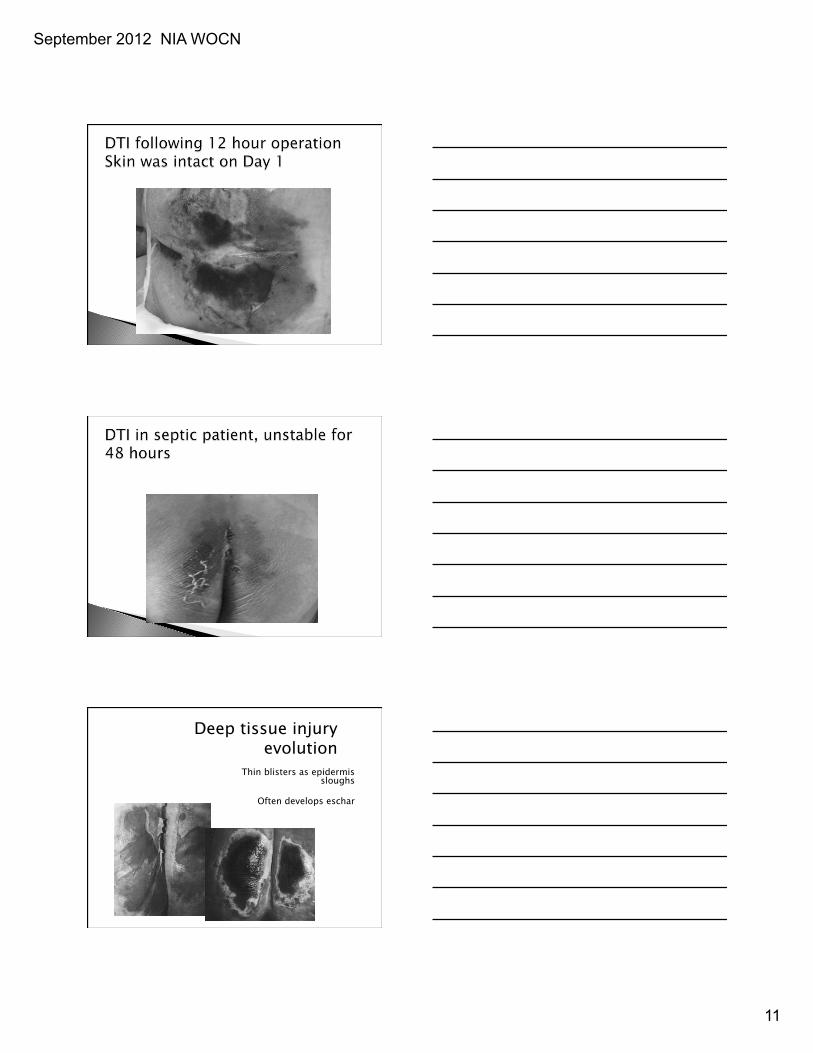
Deep tissue injury evolution
Thin blisters as epidermis sloughs
Often develops eschar
September 2012 NIA WOCN
12
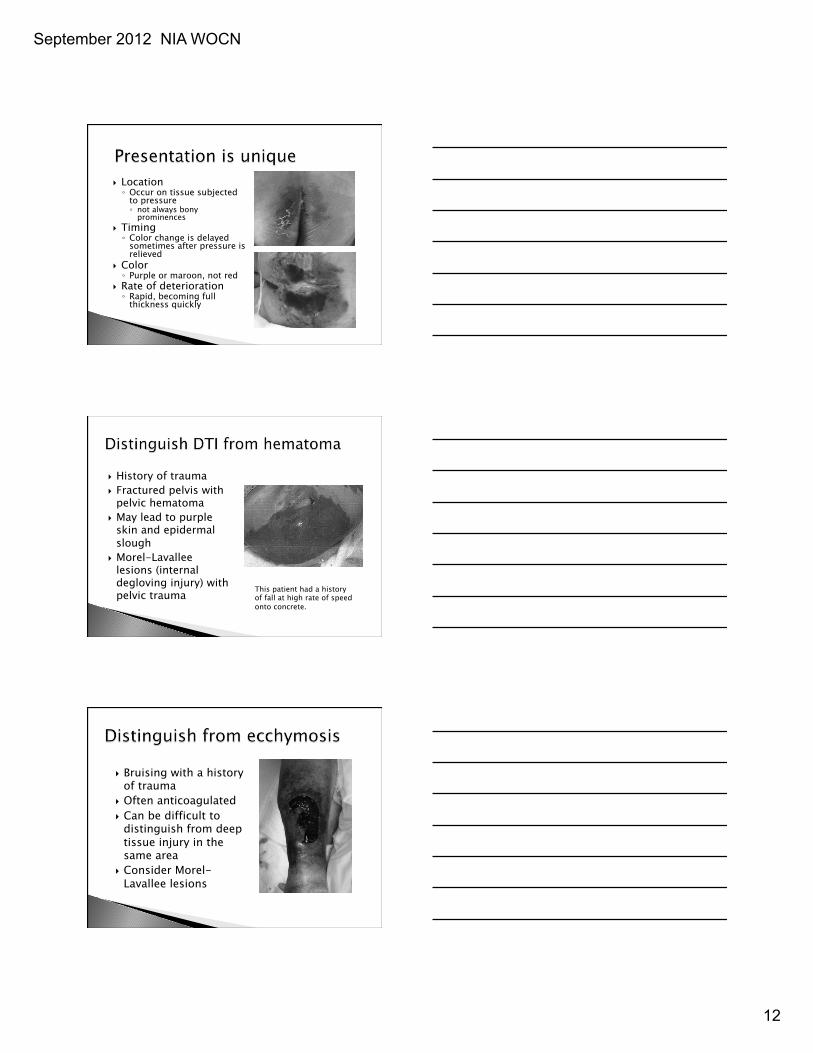
} Location ◦ Occur on tissue subjected
to pressure ◦ not always bony
prominences } Timing ◦ Color change is delayed
sometimes after pressure is relieved
} Color ◦ Purple or maroon, not red
} Rate of deterioration ◦ Rapid, becoming full
thickness quickly
} History of trauma } Fractured pelvis with
pelvic hematoma } May lead to purple
skin and epidermal slough
} Morel-Lavallee lesions (internal degloving injury) with pelvic trauma This patient had a history
of fall at high rate of speed onto concrete.
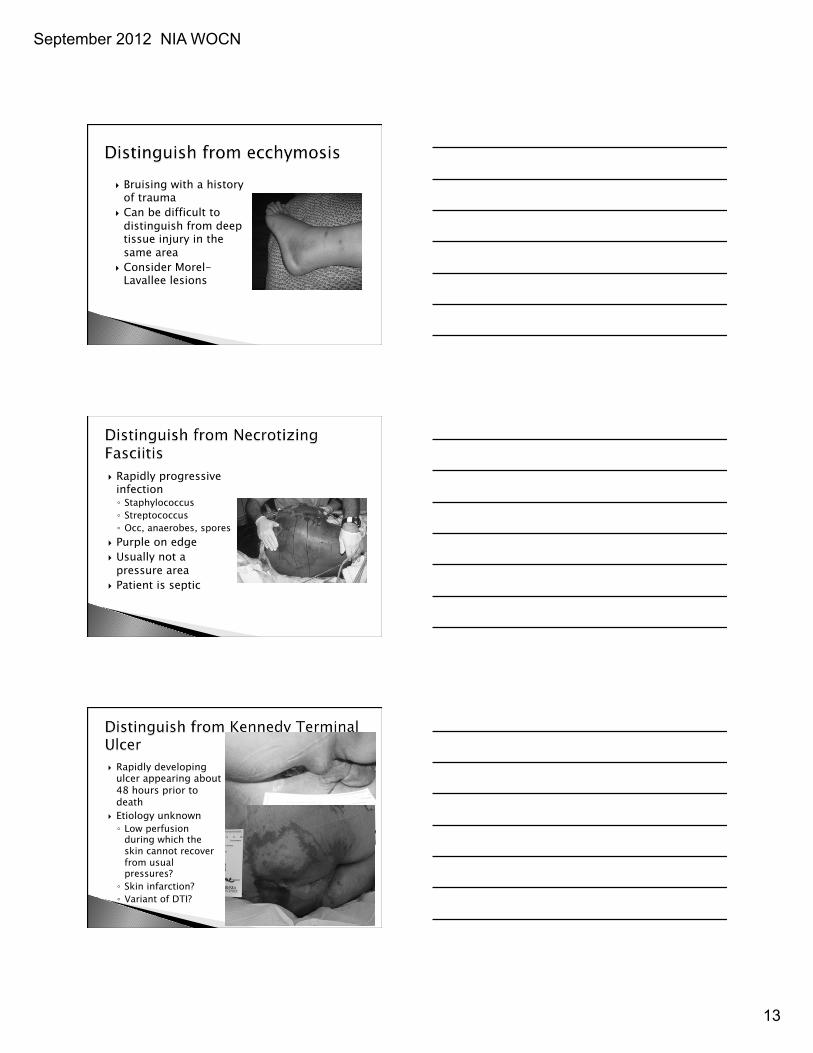
} Bruising with a history of trauma
} Often anticoagulated } Can be difficult to
distinguish from deep tissue injury in the same area
} Consider Morel-Lavallee lesions
September 2012 NIA WOCN
13
} Bruising with a history of trauma
} Can be difficult to distinguish from deep tissue injury in the same area
} Consider Morel-Lavallee lesions
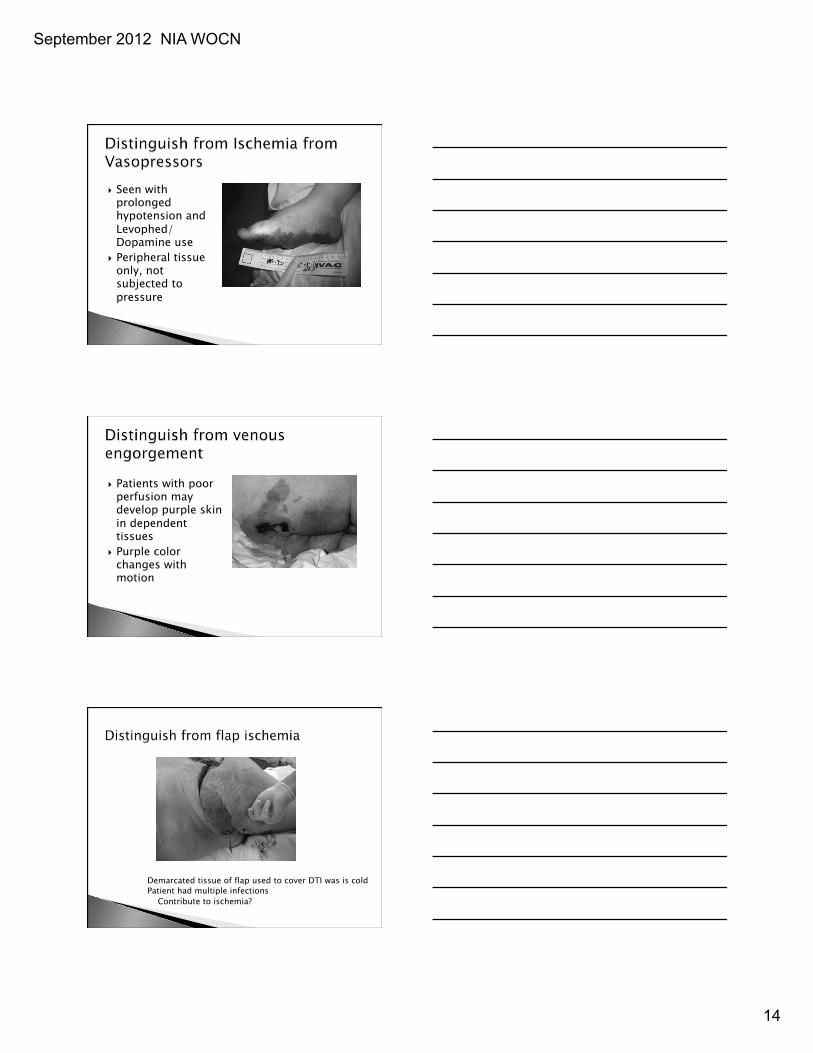
} Rapidly progressive infection ◦ Staphylococcus ◦ Streptococcus ◦ Occ, anaerobes, spores
} Purple on edge } Usually not a
pressure area } Patient is septic
} Rapidly developing ulcer appearing about 48 hours prior to death
} Etiology unknown ◦ Low perfusion
during which the skin cannot recover from usual pressures? ◦ Skin infarction? ◦ Variant of DTI?
September 2012 NIA WOCN
14
} Seen with prolonged hypotension and Levophed/ Dopamine use
} Peripheral tissue only, not subjected to pressure
} Patients with poor perfusion may develop purple skin in dependent tissues
} Purple color changes with motion
Demarcated tissue of flap used to cover DTI was is cold Patient had multiple infections Contribute to ischemia?
September 2012 NIA WOCN
15
Outside to Inside with Low Pressure
(Classic) Stage I
Fluid-filled blisters
Stage II
Inside to Outside with High Pressure
DTI Stage II with epidermal loss Unstageable with eschar or blister
Stage III or IV
September 2012 NIA WOCN
16
} Relieve pressure completely from areas likely to have DTI ◦ Side to side turning ◦ Support surfaces ◦ Heels in boots
} Relieve pressure from all purple skin
} Building evidence for MIST therapy ◦ Honaker, 2011
} No evidence today to support: ◦ Early debridement ◦ HBO
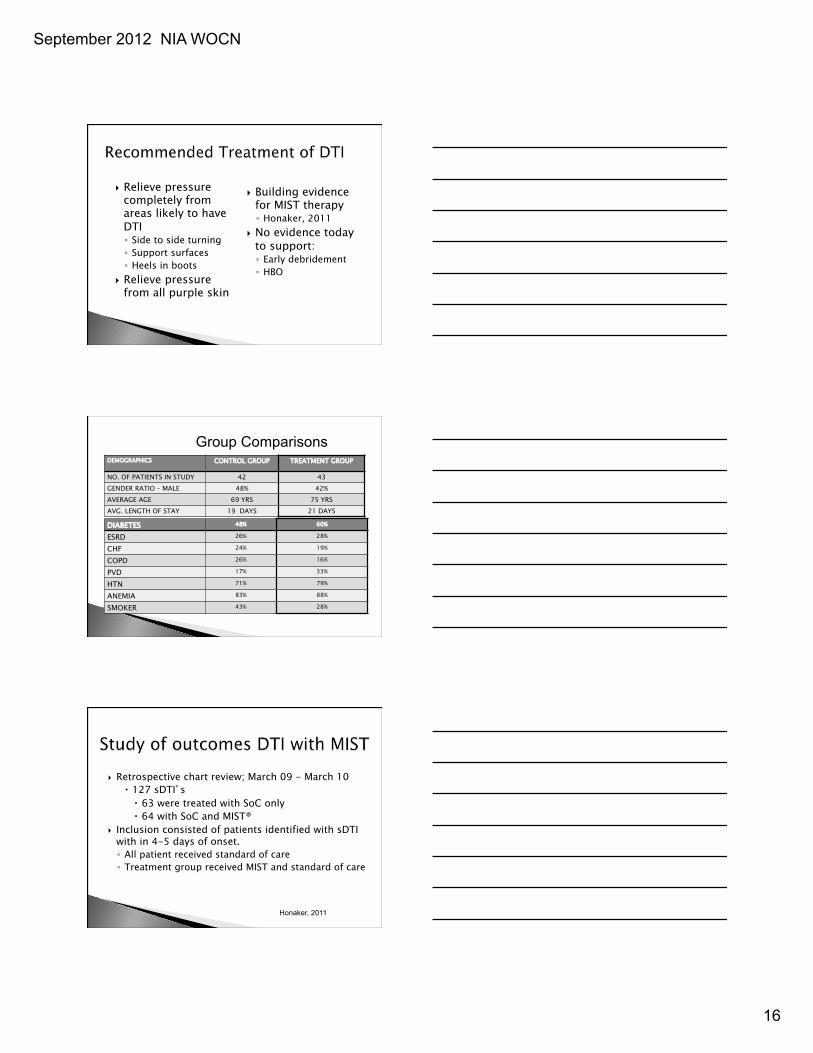
DEMOGRAPHICS CONTROL GROUP TREATMENT GROUP
NO. OF PATIENTS IN STUDY 42 43 GENDER RATIO – MALE 48% 42% AVERAGE AGE 69 YRS 75 YRS AVG. LENGTH OF STAY 19 DAYS 21 DAYS
DIABETES 48% 60%
ESRD 26% 28%
CHF 24% 19%
COPD 26% 16%
PVD 17% 33%
HTN 71% 79%
ANEMIA 83% 88%
SMOKER 43% 28%
Group Comparisons
} Retrospective chart review; March 09 - March 10 � 127 sDTI’s � 63 were treated with SoC only � 64 with SoC and MIST®
} Inclusion consisted of patients identified with sDTI with in 4-5 days of onset. ◦ All patient received standard of care ◦ Treatment group received MIST and standard of care
Honaker, 2011
September 2012 NIA WOCN
17
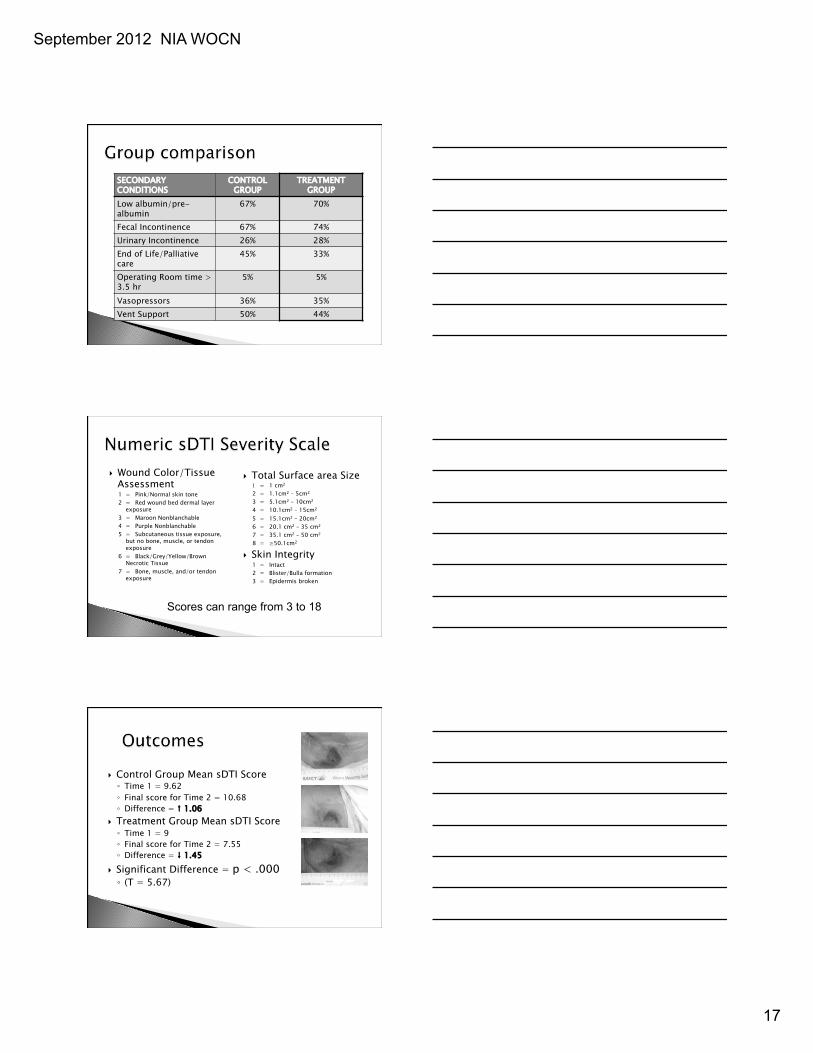
SECONDARY CONDITIONS
CONTROL GROUP
TREATMENT GROUP
Low albumin/pre-albumin
67% 70%
Fecal Incontinence 67% 74% Urinary Incontinence 26% 28% End of Life/Palliative care
45% 33%
Operating Room time > 3.5 hr
5% 5%
Vasopressors 36% 35% Vent Support 50% 44%
} Wound Color/Tissue Assessment 1 = Pink/Normal skin tone 2 = Red wound bed dermal layer
exposure 3 = Maroon Nonblanchable 4 = Purple Nonblanchable 5 = Subcutaneous tissue exposure,
but no bone, muscle, or tendon exposure
6 = Black/Grey/Yellow/Brown Necrotic Tissue
7 = Bone, muscle, and/or tendon exposure
} Total Surface area Size 1 = 1 cm2 2 = 1.1cm2 – 5cm2 3 = 5.1cm2 – 10cm2 4 = 10.1cm2 – 15cm2 5 = 15.1cm2 – 20cm2 6 = 20.1 cm2 – 35 cm2 7 = 35.1 cm2 – 50 cm2 8 = ≥50.1cm2
} Skin Integrity 1 = Intact 2 = Blister/Bulla formation 3 = Epidermis broken
Scores can range from 3 to 18
} Control Group Mean sDTI Score ◦ Time 1 = 9.62 ◦ Final score for Time 2 = 10.68 ◦ Difference = ↑ 1.06
} Treatment Group Mean sDTI Score ◦ Time 1 = 9 ◦ Final score for Time 2 = 7.55 ◦ Difference = ↓ 1.45
} Significant Difference = p < .000 ◦ (T = 5.67)
September 2012 NIA WOCN
18
} Scott Triggers (Suzie Scott-Williams, 2011) ◦ ASA score 3 or higher ◦ Age over 62 ◦ Albumin less than 2.5
} Add in length of time planned for surgery over 3 hours (NPUAP, 2009)
} Evaluate OR table cover ◦ If 2” elastic foam with cover may not be
adequate ◦ Replace with 3-4 inches of visco-elastic foam
} Consensus Group Examined Literature on Dressings to Reduce Pressure, Shear and Friction
} Group members from EU, US and Australia } Examined bench data from Evan Call lab on
dressings reducing � pressure by dispersing it � shear by absorbing it into layers of dressing � friction by slick outer surface � microclimate by absorbing sweat
} Brindle: PrU rate lower in OR (2012) Brindle: PrU rate lower in ICU (2010) Chaiken: PrU rate fell from 13.8-1.8 in ICU (2012) Cherry: ICU rate fell to 0 (2012)
September 3 2012
September 2012 NIA WOCN
19
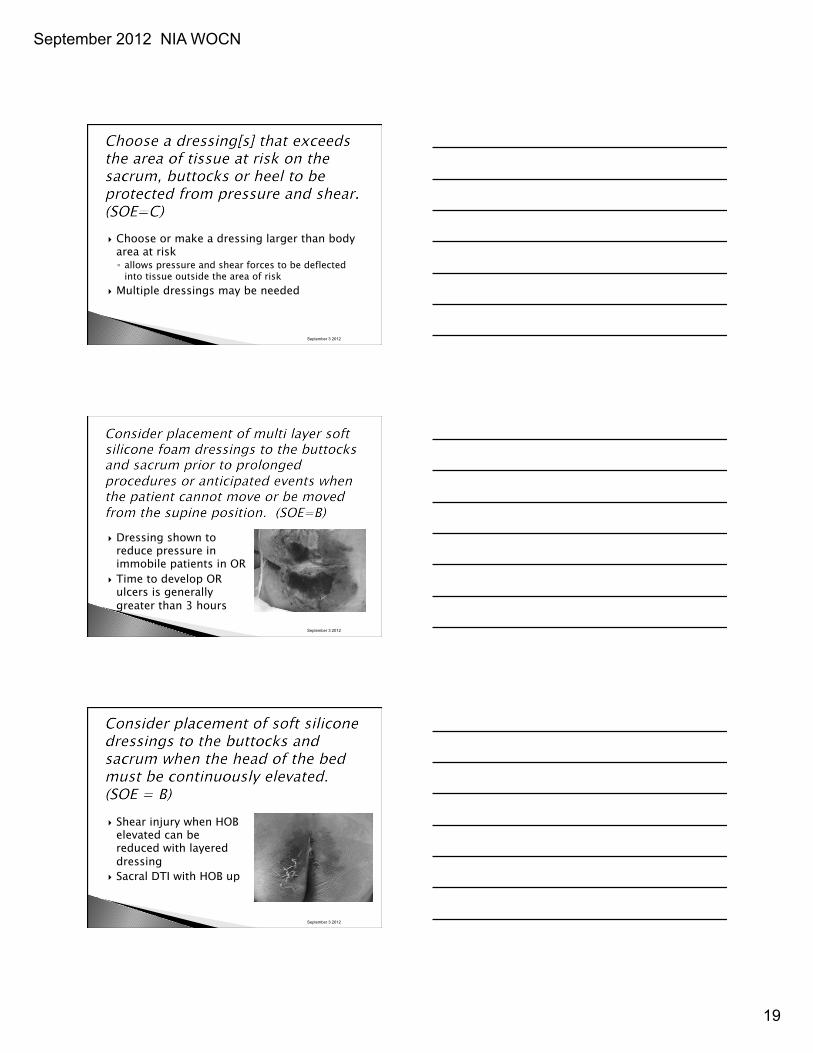
} Choose or make a dressing larger than body area at risk ◦ allows pressure and shear forces to be deflected
into tissue outside the area of risk } Multiple dressings may be needed
September 3 2012
} Dressing shown to reduce pressure in immobile patients in OR
} Time to develop OR ulcers is generally greater than 3 hours
September 3 2012
} Shear injury when HOB elevated can be reduced with layered dressing
} Sacral DTI with HOB up
September 3 2012
September 2012 NIA WOCN
20
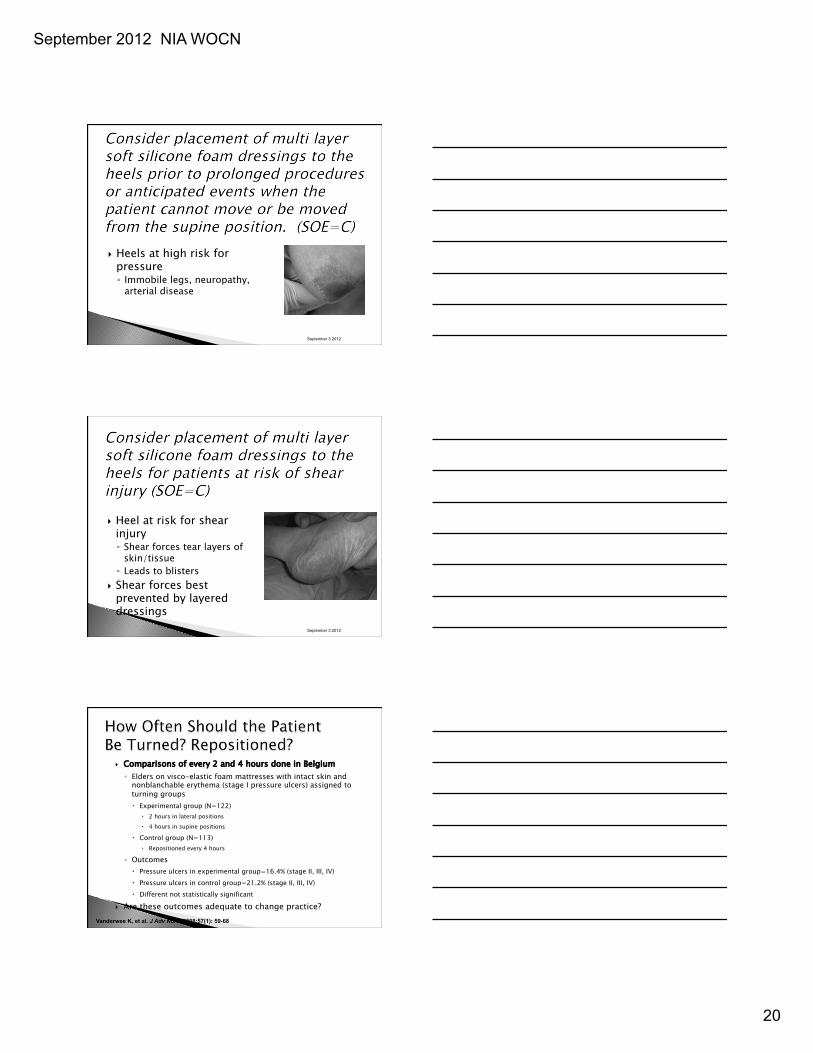
} Heels at high risk for pressure ◦ Immobile legs, neuropathy,
arterial disease
September 3 2012
} Heel at risk for shear injury ◦ Shear forces tear layers of
skin/tissue ◦ Leads to blisters
} Shear forces best prevented by layered dressings
September 3 2012
} Comparisons of every 2 and 4 hours done in Belgium ◦ Elders on visco-elastic foam mattresses with intact skin and
nonblanchable erythema (stage I pressure ulcers) assigned to turning groups � Experimental group (N=122)
� 2 hours in lateral positions � 4 hours in supine positions
� Control group (N=113) � Repositioned every 4 hours
◦ Outcomes � Pressure ulcers in experimental group=16.4% (stage II, III, IV) � Pressure ulcers in control group=21.2% (stage II, III, IV) � Different not statistically significant
} Are these outcomes adequate to change practice? Vanderwee K, et al. J Adv Nurs. 2008;57(1): 59-68
September 2012 NIA WOCN
21
} Back injury very common in healthcare workers ◦ 1/3 of back injuries are due to moving patients
� Nurses aides, orderlies and attendants are number 2 in the top 10 occupations for back injury
◦ In 2009, there were 25,160 on-the-job injuries � 60% required 5 days off; 12% required 8 days off
� Nurses use 30% more sick leave annually due to back pain
} The cost of on-the-job musculoskeletal injury is high ◦ $20 billion on worker’s compensation ◦ $100 billion on indirect costs
American Nursing Association. http://www.anasafepatienthandling.org/Main-Menu/SPH-Background /Background.aspx. Accessed May 15. Bureau of Labor and Statistics. http://www.bls.gov/news.release /archives/osh2_11202008.pdf. Accessed May 15. Bureau of Labor and Statistics. http://www.bls.gov/news. release/archives/osh2_11092010.pdf. Accessed May 15. Occupational Safety and Health Administration. http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_id=205&p_table=SPEECHES. Accessed May 16.
} If turning takes 5 minutes per turn x 12 turns per day =1 hr ◦ In acute care, RN=$38 per day per patient ◦ In a 200 bed hospital, turning half the patients=$3800
for salary if alone � How many patients can be turned alone? � How many patients can be turned in 5 minutes?
} Considered a pressure ulcer
} If cartilage is visible or palpable } Stage IV
} Mucous membrane ulcers are not staged
September 2012 NIA WOCN
22
} General care items ◦ Bedpans ◦ Foley tubing ◦ NG tubes ◦ Bed trash ◦ Suture
} Bedpans left under patients can create intense pressure ◦ Fatal wounds
} Strap injury from boots
} Injury to “other leg” when patient on his side
} Nerve/tendon injury when leg not maintained in neutral alignment
Prevents leg rotation

September 2012 NIA WOCN
23
} Elastic devices can impair blood flow to the legs ◦ “TED sores”? ◦ Ulcers on shin, toes,
calf } Must be removed
daily to inspect the skin
} Fit the device to the patient ◦ Measure TEDs ◦ Use proper sized boots
} Be aware of edema } Devices can be “lost”
in bariatric patient skin folds
} Remove or move device on each shift } Examine skin beneath device and do not
replace device back onto injured tissues ◦ Move ET tubes ◦ Do not tighten O2 cannulas � Secure to face ◦ Move pulse oximetry probes ◦ Splint NG tubes ◦ Remove TEDs BID
} Return devices that are defective!!
September 2012 NIA WOCN
24
} Litigation risk ◦ Increasing numbers of cases � “Never event” setting the stage for plaintiffs � Skin failure and skin changes at life’s end helping the
defense } Reducing your risk --- nothing new here ◦ Skin assessment on admission with proper
classification of wounds found ◦ Accurate risk assessment with linked interventions ◦ Assignment of upscaled beds or turning ◦ Documentation
A sloth in the wound? 3 toed?
} Check the credentials of providers } Be aware of a tendency to debride every
wound ◦ Often with a curette and topical Lidocaine � No bleeding from wound � No removal of necrotic tissue, in that healing is not
promote } CMS aware of rising charges for
débridements ◦ Some states limiting coverage
September 2012 NIA WOCN
25
} Call for podium presentations on DTI ◦ Do you have data?
Your participation in advancing the science and practice remains important
for quality patient outcomes












![4 NORMAS DE AUDITORIA [Modo de compatibilidad]...NIA 560 NIA 570 NIA 580 NIA 600 NIA 610 NIA 620 NIA 700 NIA 705 NIA 706 NIA 710 NIA 720 NIA 800 NIA 805 NIA 810 20/03/2017 7 Implicaciones](https://static.fdocument.pub/doc/165x107/61186efb5a681917227d2458/4-normas-de-auditoria-modo-de-compatibilidad-nia-560-nia-570-nia-580-nia-600.jpg)





