
Priporočila za zdravljenje primarne imunske trombocitopenije B1 2014.pdf · Rodeghiero F, et al....
22
Priporočila za zdravljenje primarne imunske trombocitopenije Barbara Skopec
Transcript of Priporočila za zdravljenje primarne imunske trombocitopenije B1 2014.pdf · Rodeghiero F, et al....
Priporočila za zdravljenje primarne imunske trombocitopenije
Barbara Skopec

Rodeghiero F, et al. Blood 2009;113:2386–93
ITP = Idiopatična trombocitopenična purpura
ITP = primarna imunska trombocitopenija
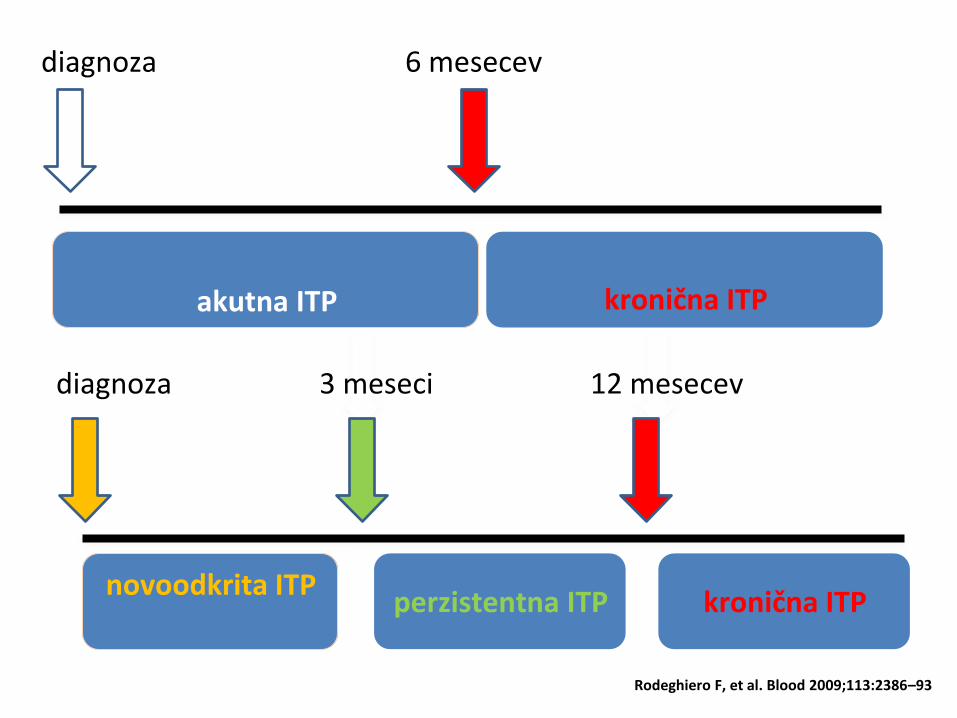
diagnoza 12 mesecev 3 meseci
novoodkrita ITP perzistentna ITP kronična ITP
Rodeghiero F, et al. Blood 2009;113:2386–93
diagnoza 6 mesecev
akutna ITP
kronična ITP
Blood 2010;115:168–186
International consensus report on the investigation and management of primary immune thrombocytopenia Provan D, Stasi R, Newland AC, Blanchette VS, Bolton-Maggs P, Bussel J.B, Chong BH, Cines DB, Gernsheimer TB, Godeau B, Grainger J, Greer I, Hunt BJ, Imbach PA, Lyons G, McMillan R, Rodeghiero F, Sanz MA, Tarantino M, Watson S, Young J and Kuter DJ
Blood 2011;117:4190–4207
The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia Neunert C, Lim W, Crowther M, Cohen A, Solberg L. Jr and Crowther MA

Basic evaluation Tests of potential utility in the
management of an ITP patient
Tests of unproven or uncertain
benefit
•Patient history •Glycoprotein-specific antibody •TPO
•Family history
•Antiphospholipid antibodies
(including anticardiolipin and lupus
anticoagulant)
•Reticulated platelets
•Physical examination •Antithyroid antibodies and thyroid
function •PaIgG
•Complete blood count and
reticulocyte count
•Pregnancy test in women of
childbearing potential •Platelet survival study
•Peripheral blood film •Antinuclear antibodies •Bleeding time
•Quantitative immunoglobulin level
measurement* •Viral PCR for parvovirus and CMV •Serum complement
•Bone marrow examination (in
selected patients; refer to text)
•Blood group (Rh)
•Direct antiglobulin test
•H pylori†
•HIV†
•HCV†
Recommendations for the diagnosis of ITP in children and adults
Provan D et al. Blood 2010;115:168–86;
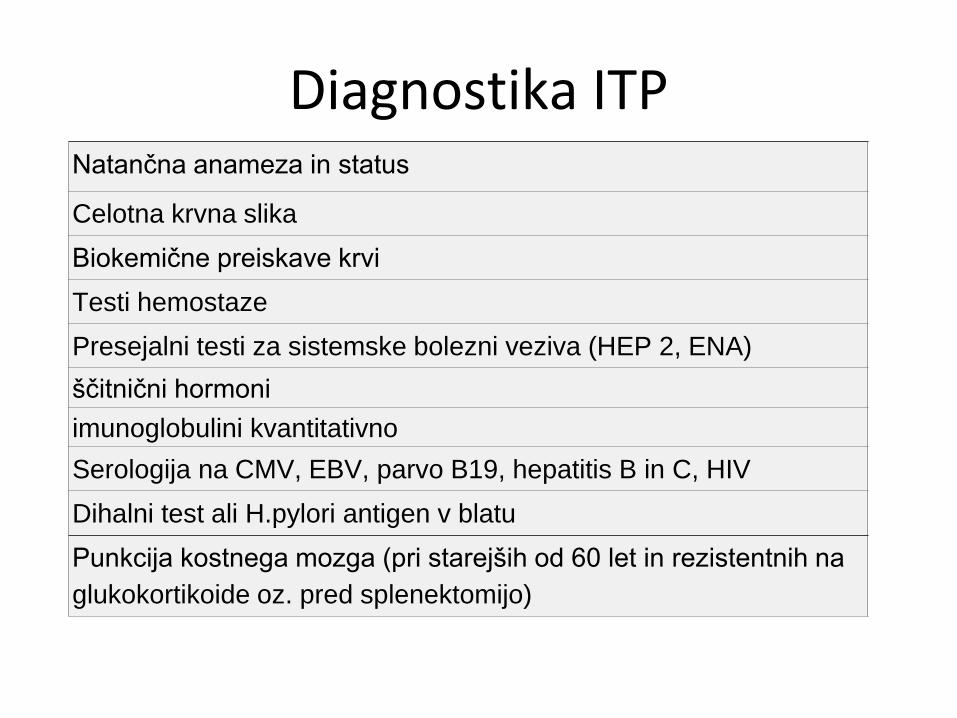
Diagnostika ITP Natančna anameza in status
Celotna krvna slika
Biokemične preiskave krvi
Testi hemostaze
Presejalni testi za sistemske bolezni veziva (HEP 2, ENA)
ščitnični hormoni
imunoglobulini kvantitativno
Serologija na CMV, EBV, parvo B19, hepatitis B in C, HIV
Dihalni test ali H.pylori antigen v blatu
Punkcija kostnega mozga (pri starejših od 60 let in rezistentnih na
glukokortikoide oz. pred splenektomijo)
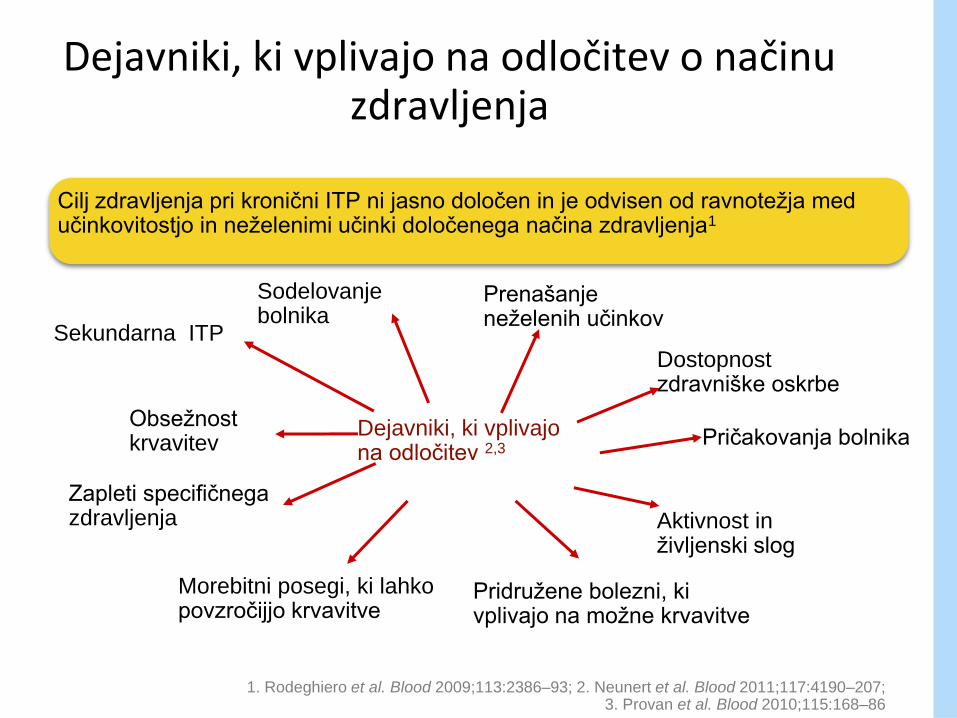
Cilj zdravljenja pri kronični ITP ni jasno določen in je odvisen od ravnotežja med učinkovitostjo in neželenimi učinki določenega načina zdravljenja1
Dejavniki, ki vplivajo na odločitev o načinu zdravljenja
1. Rodeghiero et al. Blood 2009;113:2386–93; 2. Neunert et al. Blood 2011;117:4190–207; 3. Provan et al. Blood 2010;115:168–86
Obsežnost krvavitev
Pridružene bolezni, ki vplivajo na možne krvavitve
Zapleti specifičnega zdravljenja Aktivnost in
življenski slog
Prenašanje neželenih učinkov
Morebitni posegi, ki lahko povzročijjo krvavitve
Dostopnost zdravniške oskrbe
Pričakovanja bolnika
Sodelovanje bolnika
Dejavniki, ki vplivajo na odločitev 2,3
Sekundarna ITP
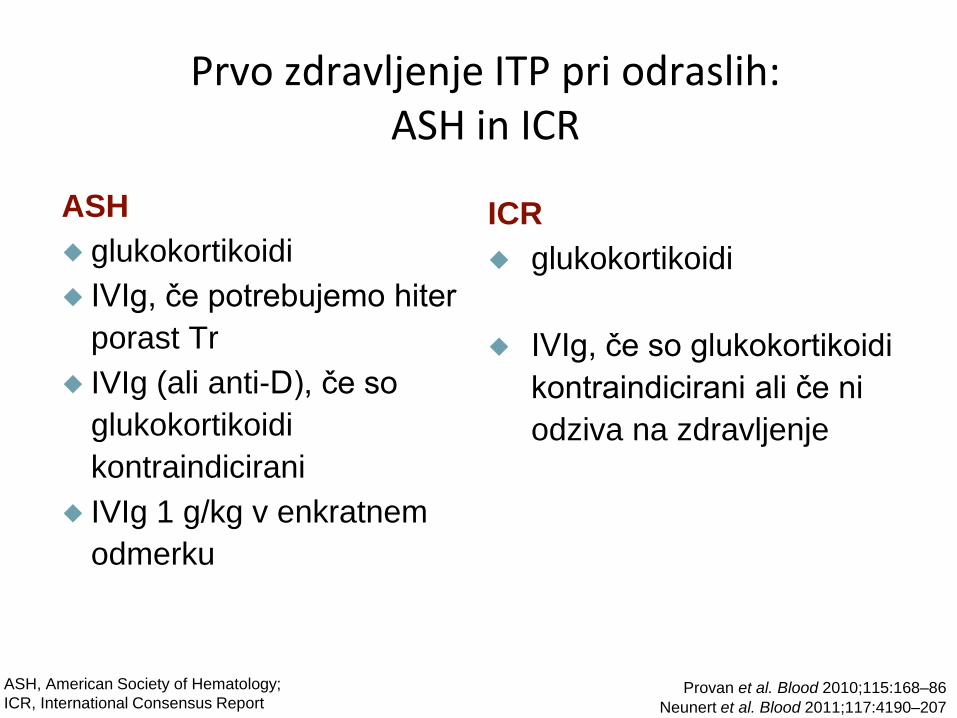
Prvo zdravljenje ITP pri odraslih: ASH in ICR
ASH
glukokortikoidi
IVIg, če potrebujemo hiter
porast Tr
IVIg (ali anti-D), če so
glukokortikoidi
kontraindicirani
IVIg 1 g/kg v enkratnem
odmerku
ICR
glukokortikoidi
IVIg, če so glukokortikoidi
kontraindicirani ali če ni
odziva na zdravljenje
ASH, American Society of Hematology;
ICR, International Consensus Report Provan et al. Blood 2010;115:168–86
Neunert et al. Blood 2011;117:4190–207

Drugo zdravljenje ITP pri odraslih : ASH and ICR
ASH
zdravila
TPO-R agonisti za rezistentne in
neprimerne za splenektomijo
TPO-R agonisti za
nesplenektomirane, s tveganjem za
krvavitev po eni liniji zdravljenja
Rituximab za rezistentne s
tveganjem za krvavitev
Kirurško zdravljenje
splenektomija
ICR
zdravila
TPO-R agonisti
Rituximab
Ostala imunosupresivna
zdravila
ciklosporin
Kirurško zdravljenje
splenektomija
Provan et al. Blood 2010;115:168–86 Neunert et al. Blood 2011;117:4190–207
ASH, American Society of Hematology;
ICR, International Consensus Report
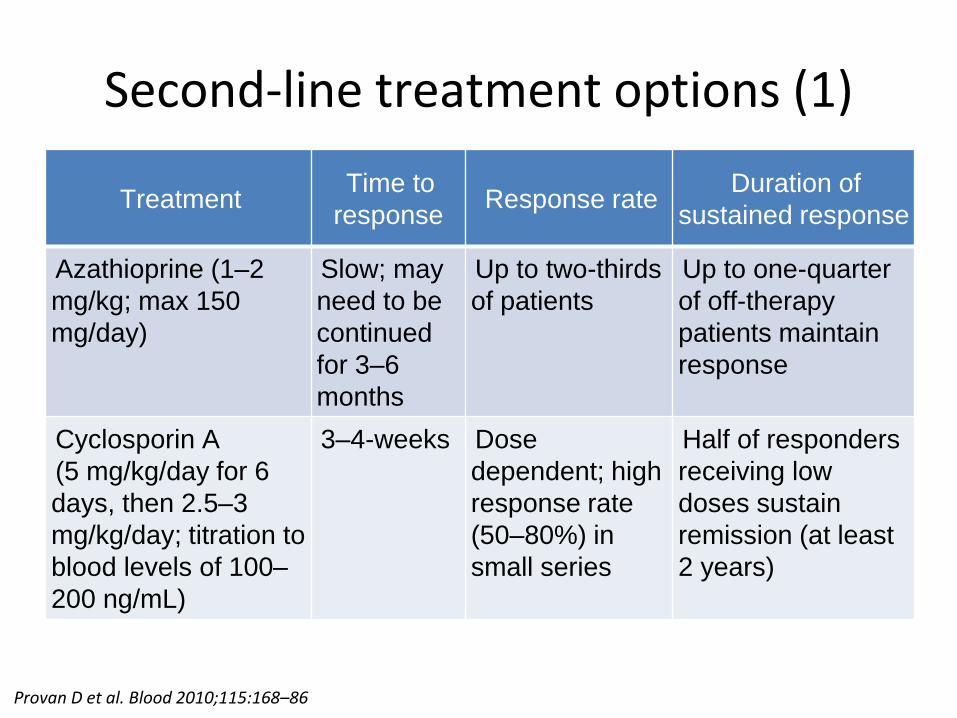
Second-line treatment options (1)
Treatment Time to
response Response rate
Duration of
sustained response
Azathioprine (1–2
mg/kg; max 150
mg/day)
Slow; may
need to be
continued
for 3–6
months
Up to two-thirds
of patients
Up to one-quarter
of off-therapy
patients maintain
response
Cyclosporin A
(5 mg/kg/day for 6
days, then 2.5–3
mg/kg/day; titration to
blood levels of 100–
200 ng/mL)
3–4-weeks Dose
dependent; high
response rate
(50–80%) in
small series
Half of responders
receiving low
doses sustain
remission (at least
2 years)
Provan D et al. Blood 2010;115:168–86

Second-line treatment options (2) Treatment
Time to
response Response rate
Duration of
sustained response
Cyclophosphamide
(1–2 mg/kg orally
daily, at least 16
weeks; or 0.3–1 g/m2
IV every 2–4 weeks,
1–3 doses)
1–16
weeks
14–85% Up to 50%
Danazol (200 mg 2–
4 times daily)
3–6 months 67% complete
or partial
response
46% in remission
at median of 119
(±45) months;
mean duration of
therapy 37 months
Dapsone (75–100
mg)
3 weeks Up to 50% Up to two-thirds of
responders off
therapy
Provan D et al. Blood 2010;115:168–86
Provan D et al. Blood 2010;115:168–86
Treatment Time to
response Response rate
Duration of
sustained response
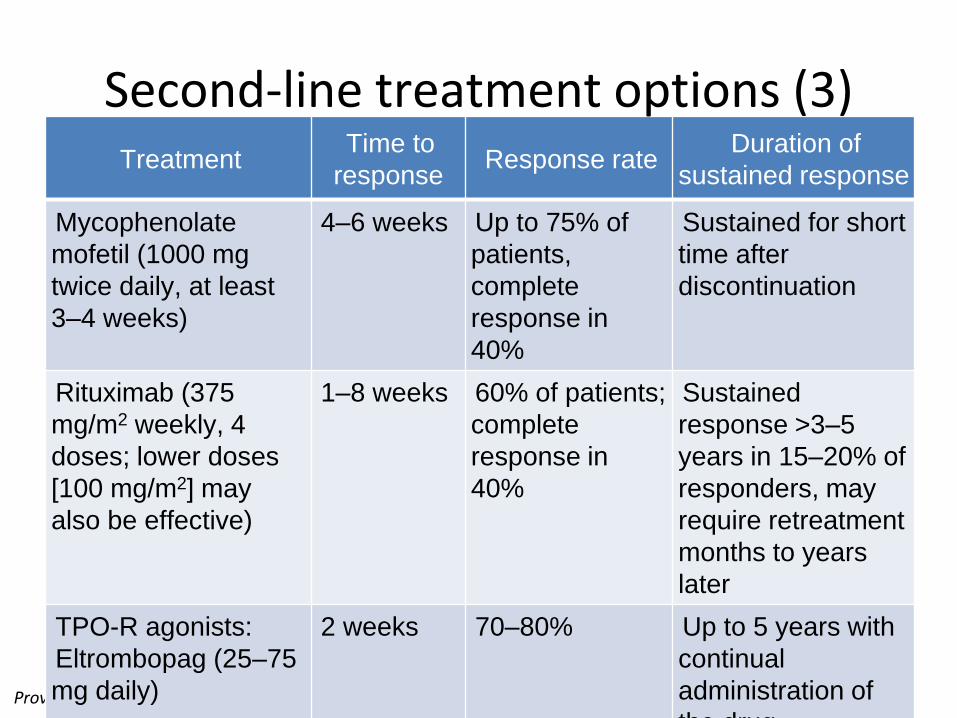
Mycophenolate
mofetil (1000 mg
twice daily, at least
3–4 weeks)
4–6 weeks Up to 75% of
patients,
complete
response in
40%
Sustained for short
time after
discontinuation
Rituximab (375
mg/m2 weekly, 4
doses; lower doses
[100 mg/m2] may
also be effective)
1–8 weeks 60% of patients;
complete
response in
40%
Sustained
response >3–5
years in 15–20% of
responders, may
require retreatment
months to years
later
TPO-R agonists:
Eltrombopag (25–75
mg daily)
2 weeks 70–80% Up to 5 years with
continual
administration of
the drug
Second-line treatment options (3)
Provan D et al. Blood 2010;115:168–86
Treatment Time to
response Response rate
Duration of
sustained response
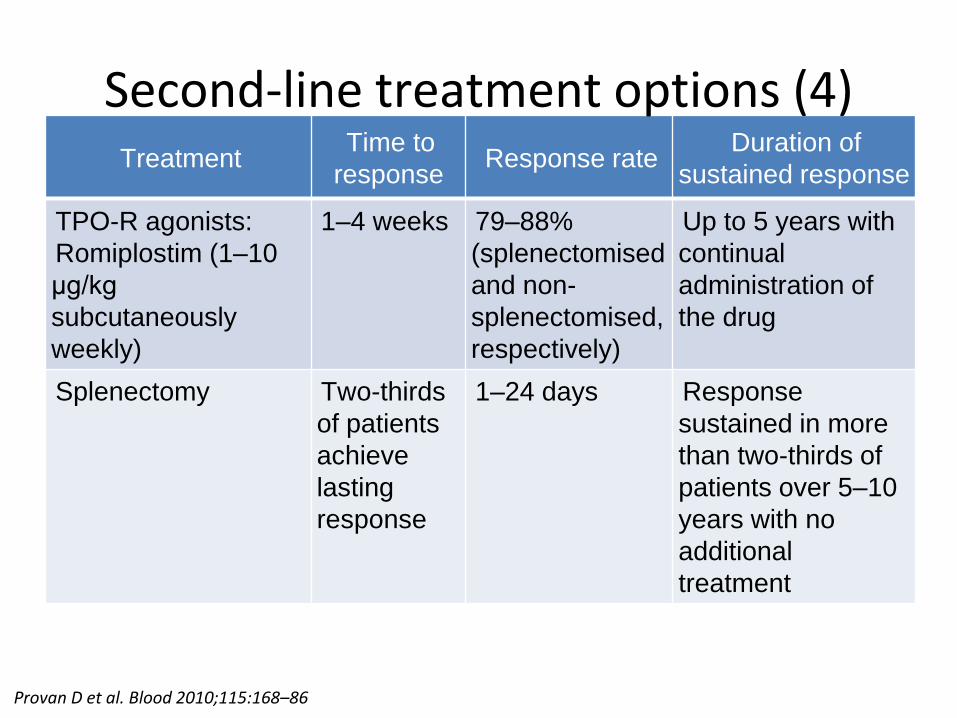
TPO-R agonists:
Romiplostim (1–10
µg/kg
subcutaneously
weekly)
1–4 weeks 79–88%
(splenectomised
and non-
splenectomised,
respectively)
Up to 5 years with
continual
administration of
the drug
Splenectomy Two-thirds
of patients
achieve
lasting
response
1–24 days Response
sustained in more
than two-thirds of
patients over 5–10
years with no
additional
treatment
Second-line treatment options (4)
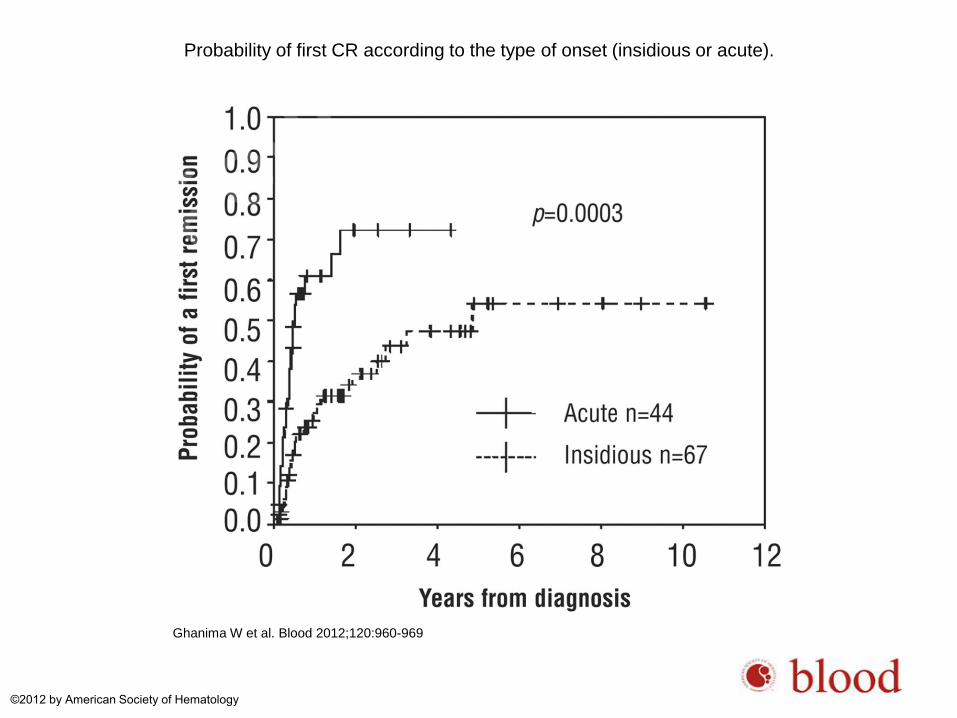
Probability of first CR according to the type of onset (insidious or acute).
Ghanima W et al. Blood 2012;120:960-969
©2012 by American Society of Hematology
Priporočila za splenektomijo
• Splenektomija ima med zdravljenji 2. reda najvišji delež uspešnosti(80%) in remisije (60–70% po 5–10 letih)
• ICR in ASH jo priporočata kot zdravljenje 2.reda
• ICR priporoča odlog splenektomije do kronične faze (>12 mesecev)
• ASH predlaga zdravljenje s TPO-R agonisti in rituksimabom pred splenektomijo
Ghanima W et al. Blood 2012;120:960–9; Provan D et al. Blood 2010;115:168–86; Neunert C et al. Blood 2011;117:4190–207
Zapleti splenektomije
• Z operacijo povezana morbiditeta in mortaliteta:
– krvavitve, okužbe, peripankreatični hematom
• Povečano tveganje za nastanek VT
• Doživljenjsko povečano tveganje za sepso povzročeno z enkapsuliranimi bakterijami (pneumococci, meningococci, Haemophilus influenzae)
Ghanima W et al. Blood 2012;120:960–9
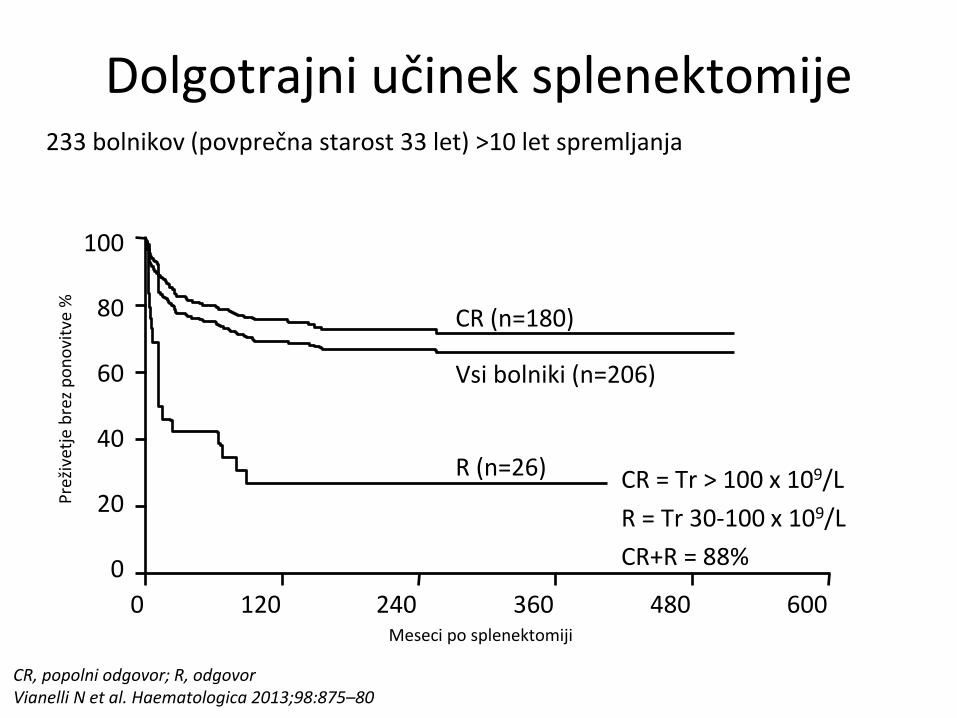
Dolgotrajni učinek splenektomije 233 bolnikov (povprečna starost 33 let) >10 let spremljanja
CR = Tr > 100 x 109/L
R = Tr 30-100 x 109/L
CR+R = 88%
Pre
žive
tje
bre
z p
on
ovi
tve
%
100
80
60
40
20
0
Meseci po splenektomiji
0 120 240 360 480 600
CR (n=180)
Vsi bolniki (n=206)
R (n=26)
CR, popolni odgovor; R, odgovor Vianelli N et al. Haematologica 2013;98:875–80
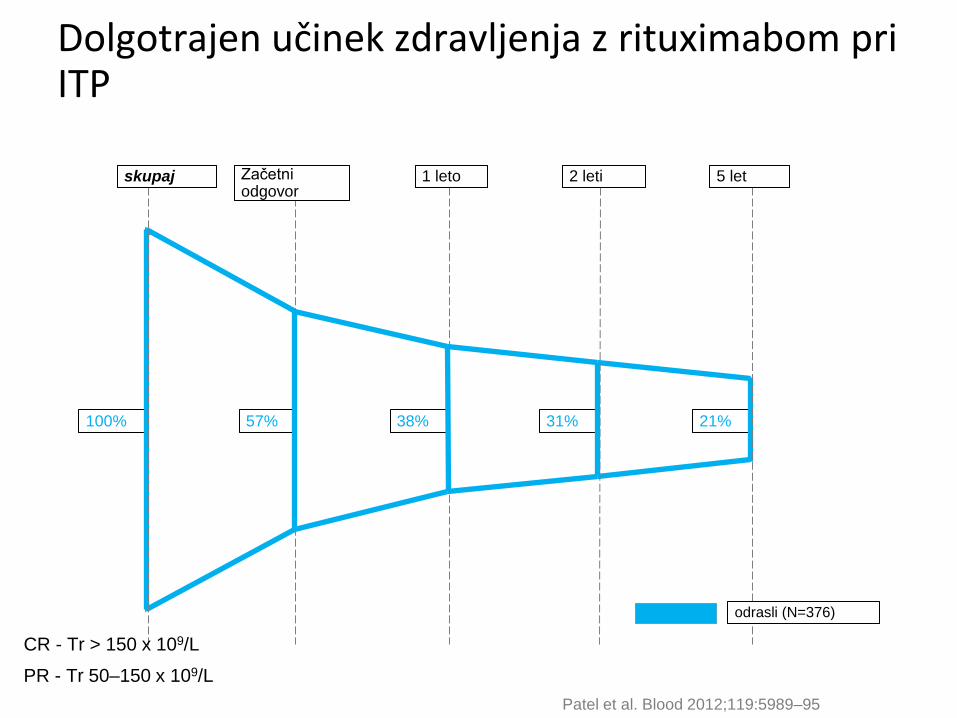
31% 100% 57% 38% 21%
odrasli (N=376)
5 let skupaj Začetni odgovor
1 leto 2 leti
Patel et al. Blood 2012;119:5989–95
Dolgotrajen učinek zdravljenja z rituximabom pri ITP
CR - Tr > 150 x 109/L
PR - Tr 50–150 x 109/L
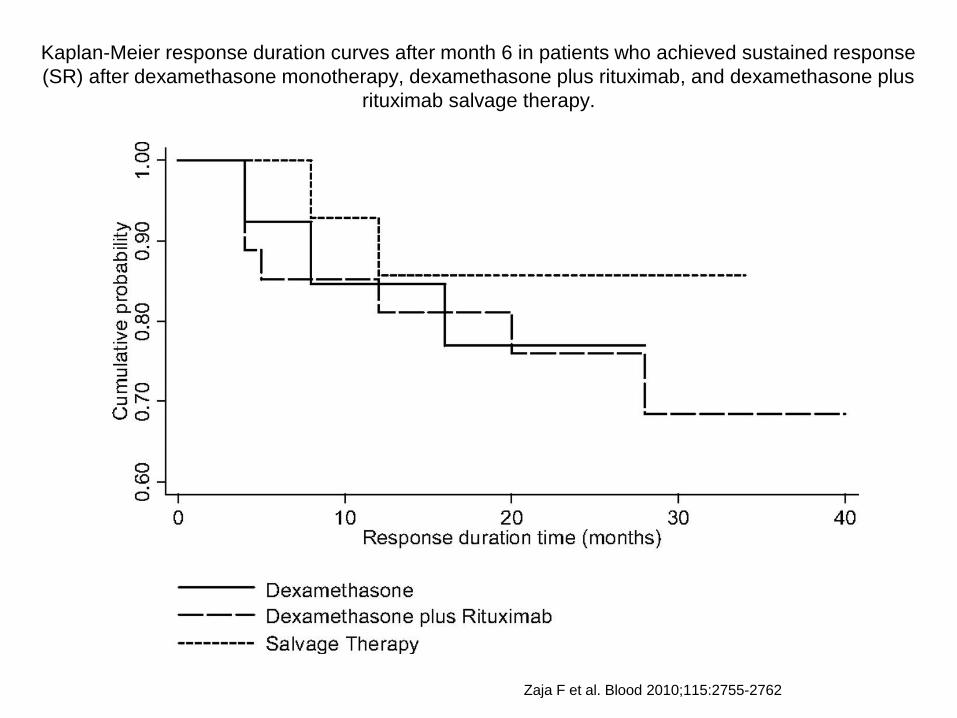
Kaplan-Meier response duration curves after month 6 in patients who achieved sustained response
(SR) after dexamethasone monotherapy, dexamethasone plus rituximab, and dexamethasone plus
rituximab salvage therapy.
Zaja F et al. Blood 2010;115:2755-2762
20
•Indicirani za zdravljenje odraslih s kronično ITP po splenektomiji, ki so odporni na druga zdravljenja (glukokortikoidi, IvIG)
•Kot druga linija zdravljenja za bolnike, pri katerih je splenektomija kontraindicirana
agonisti TPO-R
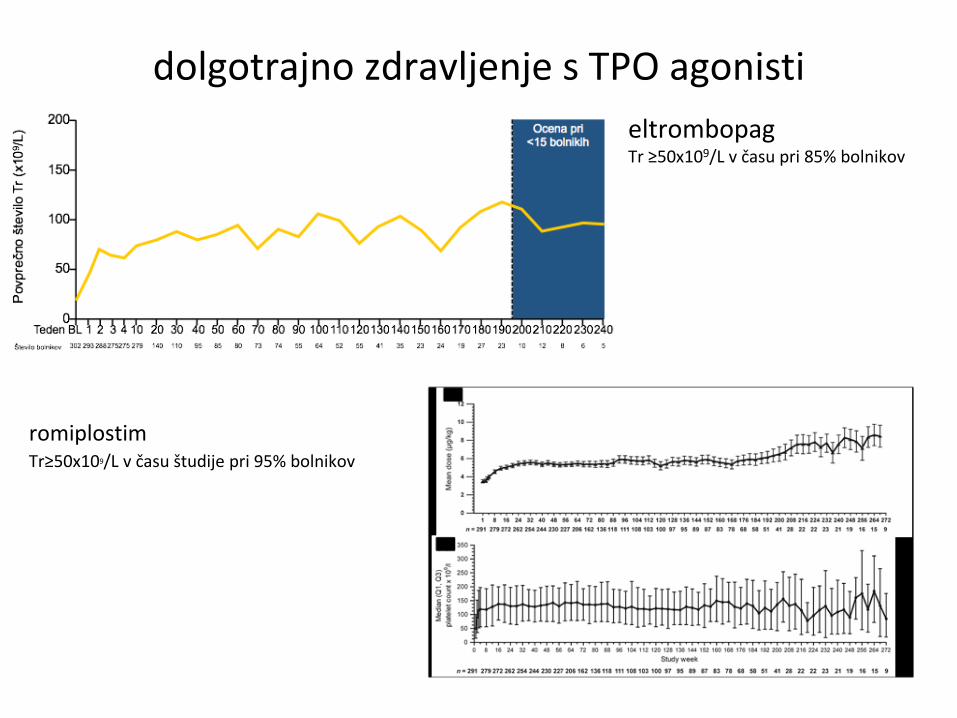
dolgotrajno zdravljenje s TPO agonisti
eltrombopag Tr ≥50x109/L v času pri 85% bolnikov
romiplostim Tr≥50x109/L v času študije pri 95% bolnikov

Naša priporočila???
• Kdaj splenektomija?
• Kdaj TPO-A?
• Kdaj rituksimab?
• Kdaj ostala imunosupresivna zdravila?


















