PowerPoint-presentatie - fresubin.be · schoonschrift getoond door Mozes Ca. 1560, anoniem SK-A...
26
10/9/2018 1 Hans Van Veer, MD, FEBS-OGS Thoracale heelkunde – Slokdarmchirurgie UZ Leuven Ingrijpen op de ‘foregut’: Wat als het begin van het eetkanaal verstoord wordt? Chirurgische kijk op de ESPEN Guidelines Vraag 1: dagelijkse praktijk Ik verzorg in mijn praktijk: A. Alle soorten patiënten in het ziekenhuis B. Voornamelijk internistische patiënten C. Voornamelijk chirurgische patiënten D. Voornamelijk geriatrische patiënten
-
Upload
nguyendang -
Category
Documents
-
view
220 -
download
0
Transcript of PowerPoint-presentatie - fresubin.be · schoonschrift getoond door Mozes Ca. 1560, anoniem SK-A...

10/9/2018
1
Hans Van Veer, MD, FEBS-OGS
Thoracale heelkunde – Slokdarmchirurgie
UZ Leuven
Ingrijpen op de ‘foregut’: Wat als het begin van het eetkanaal verstoord wordt?Chirurgische kijk op de ESPEN Guidelines
Vraag 1: dagelijkse praktijk
Ik verzorg in mijn praktijk:
A. Alle soorten patiënten in het ziekenhuis
B. Voornamelijk internistische patiënten
C. Voornamelijk chirurgische patiënten
D. Voornamelijk geriatrische patiënten

10/9/2018
2
Vraag 2: Kick-off
De ESPEN Guidelines Surgery - clinical nutrition in surgery2017…
A. zijn mij niet bekend
B. zijn mij niet bekend, maar de chirurgen in mijn ziekenhuis kennen er alles van
C. pas ik al elke dag toe in mijn klinische praktijk
De Tafelen der Wet met de tien geboden in
schoonschrift getoond door Mozes
Ca. 1560, anoniem
SK-A-4487
Rijksmuseum, Amsterdam
Outline
• Mijn leefwereld
• Overlopen 2017 guidelines
– Per Vraag (excl transplantation)
– Met bijhorende recommendations
• Kritische reflecties met huidige praktijk (in bijzonder in context van ERAS)
– Lower gut
– Upper gut

10/9/2018
3
LEEFWERELD
Leefwereld

10/9/2018
4
“Is’t kanker, dokter?”
Voorkeuren toegang
Right thoracotomy,
laparotomy, cervical anastomosis, gastric tube
Left thoracoabdominal,
cervical anastomosis, gastric tube
Left thoracoabdominal, thoracic
anastomosis, gastrectomy + Roux en Y
carina
cardia
Linker thoracofrenolaparotomie

10/9/2018
5
Linker thoracofrenolaparotomie

10/9/2018
6
buismaag
3-Hole esophagectomy: R thoracotomie, laparotomie + cervicotomie
10/9/2018
7
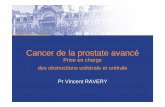
Totale gastrectomie: ROUX-en-Y
Can we do better?
The Minimally Invasive Way ?
VATS 4 ports
Laparoscopy 5 ports
Neck anastomosis
Luketich, Ann Surg 2003
VAT(thoracoscopic)S & laparoscopic MIE
10/9/2018
8
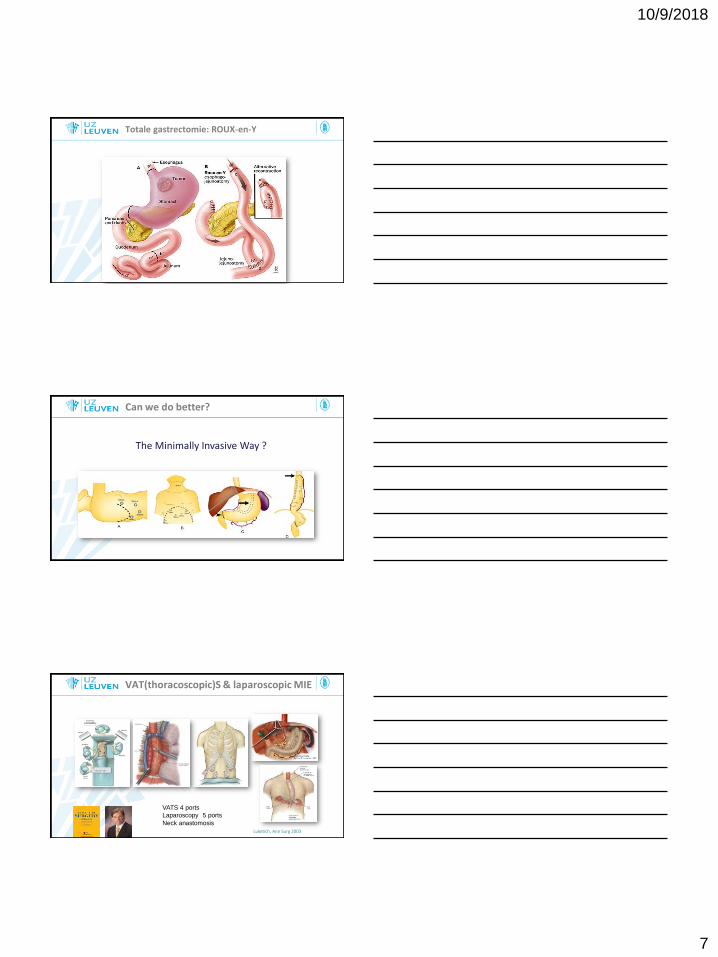
Prone Positioning
• Single lumen tube ± bronchial block
• Cave: urgent thoracotomy
Abdomen free
Rotation till 45°
Single lumen tube ± bronchial block
Cave: urgent thoracotomy
Ports placement
• High enough (dissection top of chest)
• Two ribs between each port (triangle)
Left hand
Stapling/
retraction
12 mmCamera
12 mm
Right hand
Hook coagulator
5 mm
Assistant
Suction/
Retraction
5 mm
Horizontal anatomy
subcarinal
esophagus
R Bronchus
trachea

10/9/2018
9
Bilateral vagotomy
• Gastroparesis delayed gastric emptying
• Pyloric stenosis delayed gastric emptying
• Disturbance upper GI pacemaker
• Dumping syndrome (or -like symptoms)
Case presentation - Esophageal Cancer 25
Normal esophagus Vagotomised Gastric tube
UES
a
p
e
r
i
s
t
a
l
s
i
s
Postop nutritional plan
Case presentation - Esophageal Cancer 26
Statlock + suturewing
Close to entry
BACK TO THE

10/9/2018
10
Work 2017
update of the
• 2006 ESPEN Guideline for Enteral Nutrition:Surgery and Transplantation
• 2009 ESPEN Guideline for Parenteral Nutrition: Surgery
• 2003 Guideline of the German Society for Nutritional Medicine (DGEM) Clinical Nutrition in Surgery
Kurt Boeykens, pm
Very specific…
Setup of evidence

10/9/2018
11
Work 2017
By means of
• Literature search
• Drafts
• Delphi process
recommendations from experts
evidence grading
Work 2017
Vraag 3: wiskunde
De 2017-ESPEN guidelines zijn gebaseerd op
A.85% evidence level A
B.65% evidence level A
C.45% evidence level A
D.25% evidence level A
10/9/2018
12
Vraag 3: wiskunde
De 2017-ESPEN guidelines zijn gebaseerd op
A.85% evidence level A
B.65% evidence level A
C.45% evidence level A
D.25% evidence level A
GPP
0
B
A
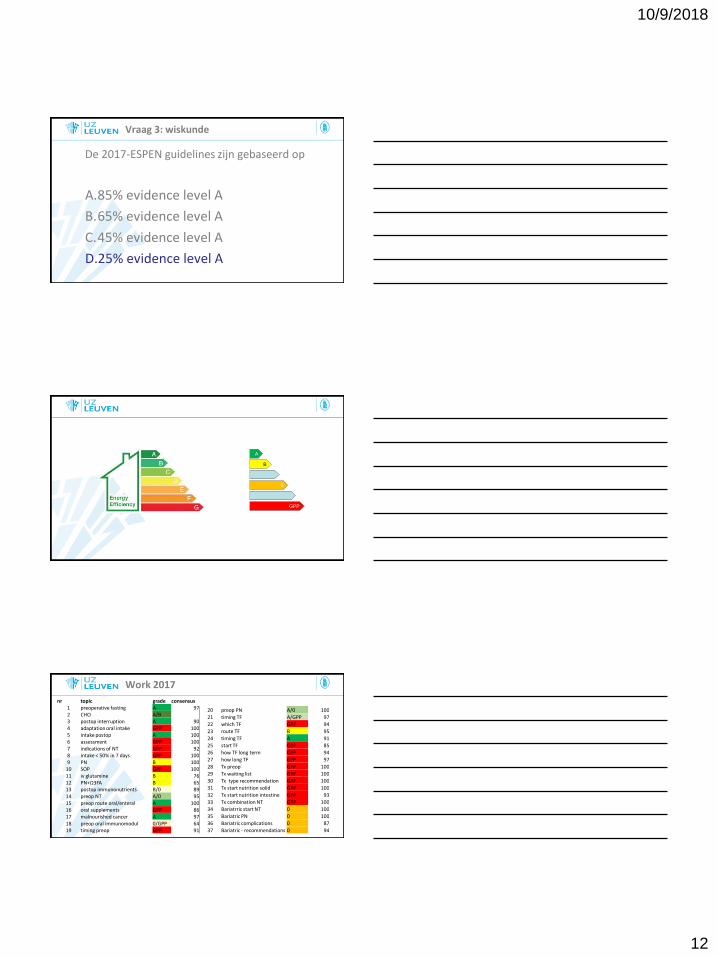
Work 2017
nr topic grade consensus1 preoperative fasting A 972 CHO A/B3 postop interruption A 904 adaptation oral intake GPP 1005 intake postop A 1006 assessment GPP 1007 indications of NT GPP 928 intake < 50% in 7 days GPP 1009 PN B 100
10 SOP GPP 10011 iv glutamine B 7612 PN+Ω3FA B 6513 postop immunonutrients B/0 8914 preop NT A/0 9515 preop route oral/enteral A 10016 oral supplements GPP 8617 malnourished cancer A 9718 preop oral immunomodul 0/GPP 6419 timing preop GPP 91
20 preop PN A/0 100
21 timing TF A/GPP 97
22 which TF GPP 94
23 route TF B 95
24 timing TF A 91
25 start TF GPP 85
26 how TF long term GPP 94
27 how long TF GPP 97
28 Tx preop GPP 100
29 Tx waiting list GPP 100
30 Tx type recommendation GPP 100
31 Tx start nutrition solid GPP 100
32 Tx start nutrition intestine GPP 93
33 Tx combination NT GPP 100
34 Bariatrric start NT 0 100
35 Bariatric PN 0 100
36 Bariatric complications 0 87
37 Bariatric - recommendations 0 94

10/9/2018
13
Preface/voorbeschouwing
• Insulin resistance
• Functional recovery
– < tolerance of oral food intake
– < restored GI motility <> ileus
– < mobilization
• Inflammatory “turning point”
– Effect on albumin
1 Is preoperative fasting necessary?
Recommendation 1:
• Preoperative fasting from midnight is unnecessary in most patients. Patients undergoing surgery, who are considered to have no specific risk of aspiration, shall drink clear fluids until two hours before anaesthesia. Solids shall be allowed until six hours before anaesthesia (BM, IE, QL).
Grade of recommendation A - strong consensus (97% agreement)
A

10/9/2018
14
2. Is preoperative carbohydrate metabolic preparation of the elective patient usefull?
Recommendation 2:
• Oral preoperative CHO treatment (instead of overnight fasting) the night before and two hours before surgery should be administered (QL).
• To impact postoperative insulin resistance and hospital length of stay, preoperative carbohydrates can be considered in patients undergoing major surgery (0) (BM, HE).
Consensus Conference: Grade of recommendation A/B
CAVE Not with DM
CAVE weak evidence cfr. Br J Surg. 2017 Feb;104(3):187-197.B
3. postop interruption of oral intake generally necessary after surgery?
Recommendation 3:
• In general, oral nutritional intake shall be continued after surgery without interruption (BM, IE).
Grade of recommendation A - strong consensus (90% agreement)
A
3. postop interruption of oral intake generally necessary after surgery?
Recommendation 4:
• It is recommended to adapt oral intake according to individual tolerance and to the type of surgery carried out with special caution to elderly patients
Grade of recommendation GPP - strong consensus (100% agreement)
GPP
10/9/2018
15
3. postop interruption of oral intake generally necessary after surgery?
Recommendation 5:
• Oral intake, including clear liquids, shall be initiated within hours after surgery in most patients.
Grade of recommendation A - strong consensus (100% agreement)
Evidence available for colonic surgery…
So far no data for esophagectomy…
A
4.1. When is nutritional assessment and therapy indicated in the surgical patient?
Recommendation 6:
• It is recommended to assess the nutritional status before and after major surgery.
Grade of recommendation GPP - strong consensus (100%agreement)
GPP
4.1. When is nutritional assessment and therapy indicated in the surgical patient?
Recommendation 7:
Perioperative nutritional therapy (NT) is indicated:
• malnutrition and pt at nutritional risk.
• unable to eat for more than 5 days perioperatively.
• expected to have low oral intake and who cannotmaintain above 50% of recommended intake for more than 7 days.
In these situations, it is recommended to initiate NT. Grade of recommendation GPP - strong consensus (92% agreement)
GPP

10/9/2018
16
4.1. When is nutritional assessment and therapy indicated in the surgical patient?
Recommendation 7:
NT via Enteral route except:
• Intestinal obstructions or ileus,
• Severe shock
• Intestinal ischaemia
• High output fistula
• Severe intestinal haemorrhage
4.1. When is nutritional assessment and therapy indicated in the surgical patient?
Recommendation 8:
• i.c.o. oral/ enteral intake alone <50% of caloric requirement for more than 7 days, a combination of enteral and parenteral nutrition isrecommended (GPP).
PN asap when contraindication for EN • e.g. intestinal obstruction (A)
Grade of recommendation GPP/A - strong consensus (100% agreement)
GPP A
4.1. When is nutritional assessment and therapy indicated in the surgical patient?
Recommendation 9:
• For administration of parenteral nutrition an all-in-one (threechamber bag or pharmacy prepared) should be preferred instead of multibottle system (BM, HE)
Grade of recommendation B - strong consensus
(100% agreement)
B
10/9/2018
17
4.1. When is nutritional assessment and therapy indicated in the surgical patient?
Recommendation 10:
• Standardised operating procedures (SOP) for nutritional support are recommended to secure an effective nutritional support therapy.
Grade of recommendation GPP - strong consensus (100%agreement)
GPP
4.2. Indication for supplementing IV glutamine?
Recommendation 11:
• Parenteral glutamine supplementation may be considered in patients who cannot be fed adequately enterally and, therefore, require exclusive PN (0) (BM, HE)
Grade of recommendation B - consensus (76%agreement)
Currently, no clear recommendation for oral glutamin suppB
4.2. Indication for supplementing oral glutamine?
Currently, no clear recommendation for oral glutamin supp

10/9/2018
18
4.3. Indication for supplementing arginine (iv/oral)?
Currently, no clear recommendation for arginine supp
4.4. Indication for supplementing i.v. Ω3 fatty acids?
Recommendation 12:
• Postop PN+Ω3FA considered only in patients who cannot be adequately fed enterally and, therefore, require parenteral nutrition (BM, HE).
Grade of recommendation B - majority agreement (65% agreement)
B
4.5. Indication for oral/enteral immunonutrients?
Recommendation 13:
• Peri-/postop immunonutrients (arginine, omega-3-fatty acids, ribonucleotides) should be given in malnourished patients undergoing major cancer surgery (B) (BM, HE).
• currently no clear evidence for immunonutrientsexclusively in the preoperative period (0).
Grade of recommendation B/0 - consensus (89% agreement) B
10/9/2018
19
4.6. NT in the PREOP period: for who?
Recommendation 14:
• Patients with severe nutritional risk shall receive nutritional therapy prior to major surgery (A) even if operations including those for cancer have to be delayed (BM).
• A period of 7-14 days may be appropriate (0)
Grade of recommendation A/0 - consensus (95% agreement)
A
4.6. NT in the PREOP period: for who?
Recommendation 15:
• Whenever feasible, the oral/enteral route shall be preferred (A) (BM, HE, QL).
Grade of recommendation A - strong consensus (100% agreement)
Grade of recommendation A – strong consensus (100% agreement) A
4.6.2 PREOP oral/enteral supplements: when?
Recommendation 16:
• When patients do not meet their energy needs from normal food, it is recommended to encourage these patients to take oral nutritional supplements during the preoperative period unrelated to their nutritional status.
Grade of recommendation GPP - consensus (86% agreement)
GPP
10/9/2018
20
4.6.2 PREOP oral/enteral supplements: when?
Recommendation 17:
• Preoperatively, oral nutritional supplements shall be given to all malnourished cancer and high-risk patients undergoing major abdominal surgery (BM, HE). A special group of high-risk patients are the elderly people with sarcopenia.
Grade of recommendation A - strong consensus (97% agreement)
A
4.6.2 PREOP oral/enteral supplements: when?
Recommendation 18:
• Immune modulating oral nutritional supplements including arginine, omega-3 fatty acids and nucleotides can be preferred (0) (BM, HE) and administered for five to seven days preoperatively (GPP).
Grade of recommendation 0/GPP - majority agreement (64% agreement)
0
4.6.2 PREOP oral/enteral supplements: when?
Recommendation 19:
• Preoperative enteral nutrition/oral nutritional supplements should preferably be administered prior to hospital admission to avoid unnecessary hospitalization and to lower the risk of nosocomialinfections (BM, HE, QL).
Grade of recommendation GPP - strong consensus (91% agreement)
GPP

10/9/2018
21
4.7 PREOP PN supplements: when?
Recommendation 20:
• Preoperative PN shall be administered only in patients with malnutrition or severe nutritional risk where energy requirement cannot be adequately met by EN (A) (BM). A period of 7-14 days is recommended (0).
Grade of recommendation A/0 - strong consensus (100% agreement)
A
POSTOPERATIVE NUTRITION
5.1 early postoperative tube feeding (TF): who?
Recommendation 21:
• Early TF (within 24 h) shall be initiated in patients inwhom early oral nutrition cannot be started, and in whom oral intake will be inadequate (<50%) for more than 7 days.
• Special risk groups are:undergoing major head and neck or GI surgery for cancer (A) patients with severe trauma including brain injury (A) (BM)patients with obvious malnutrition at the time of surgery (A) (BM) (GPP)
Grade of recommendation A/GPP - strong consensus (97% agreement) A

10/9/2018
22
5.2 tube feeding (TF): which?
Recommendation 22:
• In most patients, a standard whole protein formula is appropriate.
• kitchen-made (blenderized) diets for tube feeding is not recommended in general.
>> tube clogging
>> infection
Grade of recommendation GPP - strong consensus (94% agreement)
GPP
5.3 tube feeding (TF): how?
Recommendation 23:
• With special regard to malnourished patients, placement of a nasojejunal tube (NJ) or needle catheter jejunostomy (NCJ) should be considered for all candidates for tube feeding undergoing major uppergastrointestinal and pancreatic surgery (BM).
Grade of recommendation B - strong consensus (95% agreement)
B
5.3 tube feeding (TF): how?
Recommendation 24:
• If tube feeding is indicated, it shall be initiated within 24 h after surgery (BM).
Grade of recommendation A - strong consensus (91% agreement)
A

10/9/2018
23
5.3 tube feeding (TF): how?
Recommendation 25:
• It is recommended to start tube feeding with a lowflow rate (e.g. 10 - max. 20 ml/h) and to increase the feeding rate carefully and individually due to limited intestinal tolerance. The time to reach the target intake can be very different, and may take five to seven days.
Grade of recommendation GPP - consensus (85% agreement)
GPP
5.3 tube feeding (TF): how?
Recommendation 26:
• If long term TF (>4 weeks) is necessary, e.g. in severe head injury, placement of a percutaneous tube (e.g. percutaneous endoscopic gastrostomy - PEG) is recommended.
Grade of recommendation GPP - strong consensus (94% agreement)
GPP
5.4 tube feeding (TF): how long?
Recommendation 27:
• Regular reassessment of nutritional status during the stay in hospital and, if necessary, continuation of nutrition therapy including qualified dietary counselling after discharge, is advised for patients who have received nutrition therapy perioperatively and still do not cover appropriately their energy requirements via the oral route.
Grade of recommendation GPP - strong consensus (97% agreement)GPP
10/9/2018
24
6. TRANSPLANTATION
See hidden slides
7. BARIATRIC SURGERY
7.1. when perioperative NT in bariatrics?
Recommendation 34:
• Early oral intake can be recommended after bariatric surgery.
Grade of recommendation 0 - strong consensus (100% agreement)
Recommendation 35:
• Parenteral nutrition is not required in uncomplicated bariatric surgery.
Grade of recommendation 0 - strong consensus (100% agreement) 0
0

10/9/2018
25
7.1. when perioperative NT in bariatrics?
Recommendation 36:
• In case of a major complication with relaparotomy the use of a nasojejunal tube/needle catheter jejunostomy may be considered.
Grade of recommendation 0 - strong consensus (87% agreement)
Recommendation 37:
• Further recommendations are not different from those for patients undergoing major abdominal surgery (0).
Grade of recommendation 0 - strong consensus (94% agreement) 0
0
How are we doing ourselves?
nr topic grade consensus1preoperative fasting A
2CHO A/B
3postop interruption A
4adaptation oral intake GPP
5intake postop A
6assessment GPP
7indications of NT GPP
8intake < 50% in 7 days GPP
9PN B
10SOP GPP
11iv glutamine B
12PN+Ω3FA B
13postop immunonutrients B/0
14preop NT A/0
15preop route oral/enteral A
16oral supplements GPP
17malnourished cancer A
18preop oral immunomodul 0/GPP
19timing preop GPP
20preop PN A/0
21timing TF A/GPP
22which TF GPP
23route TF B
24timing TF A
25start TF GPP
26how TF long term GPP
27how long TF GPP
28Tx preop GPP
29Tx waiting list GPP
30Tx type recommendation GPP
31Tx start nutrition solid GPP
32Tx start nutrition intestine GPP
33Tx combination NT GPP
34Bariatrric start NT 0
35Bariatric PN 0
36Bariatric complications 0
37Bariatric - recommendations 0
Conclusion
• Currently best-available evidence
• In certain areas the evidence is not strong, in some even non-existent (eg. oesophageal…)
• Inevitably, new evidence in the future will lead tostrengthening or modification of the guidelines.
• Assessment is the start, then team collaboration is the key to successful nutritional therapy.

10/9/2018
26
Vraag 4: closing games
Door de ESPEN Guidelines Surgery 2017 zal…
A. mijn klinische praktijk niet veranderen
B. mijn klinische praktijk aanpassen
C. voel ik mij geroepen om de nieuwe guidelines voor 2020 te schrijven


![· 4487 s mt eden paeroa n- 286 2 9 mar 4487 scale of chains 0643 to an of the pijiÁeÌj] tj}íem blocks i and survey. dst clearing o o. o re 0)](https://static.fdocument.pub/doc/165x107/5e3122cbf68d54366e03fdeb/4487-s-mt-eden-paeroa-n-286-2-9-mar-4487-scale-of-chains-0643-to-an-of-the-pijieoej.jpg)