Manajemen Tatalaksana Arbovirus
61
MANAJEMEN DENGUE DAN CHIKUNGUNYA ANGGRAINI ALAM Dept. IK Anak RSUP Dr. Hasan Sadikin/FK Unpad
description
Presentasi ini berisi manajemen tatalaksana arbovirus
Transcript of Manajemen Tatalaksana Arbovirus

MANAJEMEN DENGUE DAN CHIKUNGUNYA
ANGGRAINI ALAMDept. IK Anak RSUP Dr. Hasan Sadikin/FK Unpad



Dengue Virus DEN-1Kimura & Hotta, 1943Sabin & schlesinger, 1945(Haw-Den-1) as a prototype
DEN-2Isolates from New GuineaNew Guinea C (NG”C”-DEN-2) as prototype
DEN-3From patient with hemorrhagic disease in Manila, 1956
DEN-4From patient with hemorrhagic disease in Manila, 1956
Purdue univ computer illustration

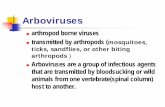
Virus Dengue Serotype at 19 cities in Indonesia (2003-2005)
D2,3
D2,3,4
D2,4
D1,2,4
D1,2
D2
D2
D3
D1,3
D4,3
D3,2
D2,3,4
D2 D2,4
D2,4,3 D2 D2

INDONESIA’S SEROTYPE
DEN-1 : 8% DEN-2 : 65% DEN-3 : 15% DEN-4 : 12%
AryatiTropical Disease Unair/Bagian Patologi Klinik FK Unair-RSU dr Soetomo


Grafik 2. Jumlah kasus DBD dan CFR di regional Asia Tenggara 2006-2008
Sumber WHO 2009
Case 2006
Case 2007 Case 2008
140000 9
CfR% 2006
8 120000
CfR% 2007
CfR% 2008
7 100000
6
80000 5
4 60000
3 40000
2
20000 1
0 0
Country

0
50
100
150
200
250
300
350
400
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
1968
1969
1970
1971
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
KASUS
TAHUN
Grafik 3 Jumlah Kasus & Kab/Kota Terjangkit DBD Per Tahun di Indonesia Tahun 1968-2009 (22 Juli 2009) sumber Dirjen PPL DEPKES 2009
KASUS KAB/KOTA TERJANGKIT
KAB/KOTA

Mortalitas DHF di RSHS 2007 s/d 2010

Demam Dengue
Hari sakit
emp
Time of fever defervescence(Saat suhu reda)
Suhu reda, klinis membaik, nafsu makan membaik

Demam Berdarah Dengue
Hari sakit
emp
Klinis memburuk, lemah, gelisah, tangan kaki dingin, nafas cepat, diuresis berkurang, tidak ada nafsu makan
Fase syokFase demam Fase konvalesens
Time of fever Time of fever defervescencedefervescence


Pearls in Diagnosis (1)
In a child with acute onset of high fever:
flushed face without coryza, with petechiae and/or Torniquet test (+) suggest the possibility of dengue infection.
TT (+) together with WBC < 5,000 /mm3: 60-70% PPV for diagnosis dengue /DHF (day 2-3 fever)
If Hepatomegaly (+) increases the possibility of DHF

Torniquet testWidely divergent and probably
reflect inter-observer variability as well as the day of illness
TT was positive in: 46% four days, 56% three days 67% two days, 78% one day before defervescence and in 90% on the day of
defervescence

A drop in platelet counts concurrently with rising Hct (> 20%) confirms diagnosis of DHF and signals the need for intervention therapy
A drop in WBC (leukopenia) with decrease in PMN and a relative increase in lymphocyte (+ atypical lymphocyte) predict the end of febrile period (24 hrs before temp drop) in DHF

The presence of pleural effusion and ascites support the diagnosis of DHF/DSS cases
in whom rising Hct is less than 20% (mostly due to early volume replacement or bleeding)

FOTO RONTGEN TORAKS RLD
Posisi anak saat pengambilan foto
Hasil yang didapat

Vaughn DW, Green S, Kalayanarooj S, et al. Dengue in the early febrilephase: viremia and antibody responses. J Infect Dis 1997; 176:322-30.
CENTERS FOR DISEASE CONTROLAND PREVENTION
AB
PEI = A/B x 100
Pleural Effusion IndexPleural Effusion Index

ULTRASONOGRAFI TORAKS tranversal
Efusi pleura kananEfusi pleura kanan

ULTRASONOGRAFI abdomen
Dinding kandung empedu menebal

Pitfalls in Diagnosis (1)
No or low index of suspicion for dengue/DHF lead to delay or misdiagnosis.
Although the incidence of DHF is high in older children (5-9 and 10-15 years), DHF can occur in younger infants, even newborn (from vertical transmission)
Failure to appreciate the value of tourniquet test and routine WBC which help screening dengue from non-dengue in early febrile phase

Misdiagnosis DF as DHF: not using evidence of plasma leakage
(pleural effusion/ ascites or hypoproteinemia/albuminemia)
for case definition of DHF
Over diagnosis of dengue/DHF : not using criteria for diagnosis

Misjudgement of critical stage, which could begin as early as day 3 (if fever drop on day 3).
A delay in doing the WBC, platelets and Hct determination which help predict the critical stage/shock lead to misdiagnosis and/or delay until shock occur
Delay to recognize DSS as most of them remain in good conscious and have narrowed pulse pressure (eg BP 110/90; 100/80 mmHg) without hypotension

Misdiagnosis of DHF in infants (< 1 yr) who may present with convulsion as CNS infections which may lead to unnecessary and invasive procedure (eg LP)
Failure to think of internal (concealed) bleeding that need blood transfusion because of high Hct (from plasma loss)
Failure to diagnose other associated condition that may be risk factors e.g. peptic ulcer, menstruation that may increase bleeding tendency

Rapid sero-diagnosis by ELISA may give
false negative on the first 2-3 days of fever
while the PCR is specific and sensitive but cannot differentiate DHF from DF


Pearls in Management (1)
With early clinical recognition and frequent monitoring of patient for
plasma leakage, early volume replacement when Hct rises significantly can prevent shock
and/or modify disease severity

The period of plasma leakage/shock is short.
The time that need close observation and monitoring of vital signs, Hct and urine
output is approximately 24-48 hours
A rising Hct is a good indicator for plasma loss
Hct is simple procedure for use to adjust I.V. fluid rate/volume

DSS can be succesfully resuscitated: About 60% by using crystalloid solution only 25% need colloidal and 15% need blood transfusion (+ blood
components) Children Hospital Bangkok (2002)
Pediatrics department Hasan Sadikin Hospital:
April 2005 – Maret 2006 175 DSS cases 63% crystalloid only; 13% crystalloid and
colloid 9,5% crystalloid, colloid and inotropic ( 22.5% need colloid) 4 % crystalloid and inotropic

With rapid recognition of shock and proper treatment, rapid and dramatic recovery is the rule
If shock is rapidly and appropriately managed usually there is no massive bleeding even though the platelets are lower than 50,000/mm3
Stable Hct and vital signs, diuresis, and rapid return of appetite are good indicators to stop I.V. fluid

Pitfalls in management (1)
Abuse of antibiotics when not suspicion of dengue/DHF
These unnecessary drugs use may contribute to:
increase chance for hemorrhage (aspirin,ibuprofen)
precipitate Reye syndrome (aspirin) hepatic dysfunction (acetaminophen if
overdose)

Over use of platelet transfusion as prophylaxis
for bleeding in all shock cases

Thrombocytopenia and Platelet Transfusions in DengueHaemorrhagic Fever and Dengue Shock SyndromeAlex Chairulfatah, Djatnika Setiabudi, Ridad Agoes andRobert Colebunders
In conclusion, a large number of patients with DHF/DSS in Bandung hospitals receive platelet transfusions, even if thrombocyte counts are above 25,000/ml.
This study suggests that in most DHF/DSS cases,
platelet transfusions do not influence the incidence of severe bleeding.
Treatment costs for DHF/DSS cases could be reduced if these unnecessary platelet transfusions are avoided.
Dengue Bulletin – Vol 27, 2003

PENATALAKSANAANPENATALAKSANAAN
- Terlalu dini/agresif memberi IVFDTerlalu dini/agresif memberi IVFD
- Terlambat menghentikan/ Terlambat menghentikan/
memperlambat tetesan IVFDmemperlambat tetesan IVFD
- Terlambat memberikan cairan koloid pada Terlambat memberikan cairan koloid pada kebocoran plasma yang hebatkebocoran plasma yang hebat
PENATALAKSANAANPENATALAKSANAAN
- Terlalu dini/agresif memberi IVFDTerlalu dini/agresif memberi IVFD
- Terlambat menghentikan/ Terlambat menghentikan/
memperlambat tetesan IVFDmemperlambat tetesan IVFD
- Terlambat memberikan cairan koloid pada Terlambat memberikan cairan koloid pada kebocoran plasma yang hebatkebocoran plasma yang hebat
Beberapa hal yang perlu diperhatikanBeberapa hal yang perlu diperhatikan

PENATALAKSANAAN
- Terlambat memberi transfusi darah pada perdarahan masif tersembunyi
- Terlalu agresif memberi suspensi trombosit
- Terlambat/lupa memberi Oksigen pada DSS
Jangan lupa membuat laporan KDRS
PENATALAKSANAAN
- Terlambat memberi transfusi darah pada perdarahan masif tersembunyi
- Terlalu agresif memberi suspensi trombosit
- Terlambat/lupa memberi Oksigen pada DSS
Jangan lupa membuat laporan KDRSJangan lupa membuat laporan KDRSJangan lupa membuat laporan KDRS

pelaporan Isi formulir KDRS: Diserahkan 24 jam setelah penegakkan
diagnosis Memerlukan pemeriksaan laboratorium
termasuk serologi
terlambat?Perlu form TERSANGKA DBD sebagai
laporan awal

pelaporan 30% pelaporan RS di Kota Bandung
(RSHS dan RS Swasta) ke Dinkes Jabar (2003)

peralatanTensimeter dengan berbagai ukuran cuff
(3 macam), untuk: Pengukuran tekanan darah Tourniquette test
Pemeriksaan hematokrit Di puskesmas (minimal PKM DTP)


What the heck is Chikungunya?Togaviridae
alphavirusRNA virus able to
evolve rapidly and expand vector
Endemic in Africa and Asia, especially India
Vectored by Aedes species (albopictus, aegypti)

Natural cycleAedes mosquitoes
Feed in daytime Breed in stagnant
water Small puddle
Reservoir Primates Transient viremia 3-
7 days

Clinical criteria: Acute onset of fever >38.5°C and severe arthralgia/arthritis not explained by other medical conditions.
Epidemiological criteria: Residing or having visited epidemic areas, having reported transmission within 15 days prior to the onset of symptoms.
Laboratory criteria: At least one of the following tests in the acute phase:- Virus isolation.- Presence of viral RNA by RT-PCR.- Presence of virus-specific IgM antibodies in single
serum sample collected in acute or convalescent stage.- Four-fold increase in IgG values in samples
collected at least three weeks apart.
case definition

CASES CATEGORIZED Possible case: A patient meeting
clinical criteria. Probable case: A patient meeting both
the clinical and epidemiological criteria. Confirmed case: A patient meeting the
laboratory criteria, irrespective of the clinical presentation.

Algorithm for ascertainment of suspected Chikungunya case
Source: ECDC Mission Report: Chikungunya in Italy, Joint ECDC/WHO visit for a European risk assessment 17 – 21 September 2007

It may be noted that during an epidemic:
all patients need not be subjected to confirmatory tests as aboveAn epidemiological link may be enoughClinical management as of now does not differ between a probable case and a confirmed case

Clinical diseaseSignificant
morbidity, minimal mortality
Fever, rash, nausea, fatigue, arthralgia lasting days to weeks
Arthritis may be long-term sequellae

Manifestasi Klinis
WHO Guidelines for Prevention and Control of Chikungunya Fever; 2009


Complications Possible complications include gastro-
intestinal complications, cardiovascular decompensation or meningo-ecephalitis
Fatalities have been reported mainly in aged patients or where the patient’s immune system was weakened by underlying conditions

Treatment
In the absence of treatment for Chikungunya fever, focus is set on: symptomatic treatment only (non-steroid
anti-inflammatories, non-salicylic analgesics)
surveillance of the patient for complications
prevention of further transmission
In order to prevent further transmission, infected persons should avoid further mosquito bites (e.g. use of repellents or sleeping under bed nets as much as possible)

CASE MANAGEMENT
rest acetaminophen or paracetamol to relieve
fever ibuprofen, naproxen or other non-
steroidal anti-inflammatory agent (NSAID) to relieve the arthritic component
drink plenty of fluids to replenish fluid lost from sweating, vomiting, etc.
Cases that have prolonged arthralgia and joint stiffness may benefit from a regimen of graduated physiotherapy






Dengue vaccines in clinical trials
Swaminathan S, Khanna N. Current Science 2010;98(3)

Morrison et al. JID 2010:201
CYD Vaccine Trial

R.Z. Capeding et al. / Vaccine 29 (2011) 3863–3872
CYD Vaccine Trial

DENGUE VACCINES The live attenuated dengue vaccines may
eventually be licensed for human use. Current indications are that these vaccines
will need to be administered in 2 or 3 doses to achieve tetravalent seroconversion.
In dengue-endemic areas, partially seroconverted recipients are likely to face the possibility of infection before completion of the immunization schedule; it needs not only safe and efficacious, but also inexpensive
Swaminathan S, Khanna N. Current Science 2010;98(3)