local anesthesia in dentistry 5 armamentarium
59
IN THE NAME OF GOD
-
Upload
- -
Category
Health & Medicine
-
view
174 -
download
7
Transcript of local anesthesia in dentistry 5 armamentarium
IN THE NAME OF GOD
اصول بی حسی موضعی در دندانپزشکی
درس جراحی نظری
دکتر سید هادی حسینی
متخصص جراحی فک و صورت
www.drhadihoseini.com
:دانلود اسالید در
http://www.slideshare.net/hadidezyan

The Armamentarium
4 PARTS:
1) The Syringe
2) The Needle
3) The Cartridge
4) Preparation

The Syringe
Standard of Care aspirating dental syringes are the standard of care due to their ability to aspirate blood if the tip of the needle is located intravascularly
ADA Standards for Injection Syringes
.1They must be durable and able to withstand repeated
sterilization without damage
2. They should be capable of accepting a wide variety of
cartridges and needles from different manufacturers and
permit repeated use
3. They should be inexpensive, self-contained, lightweight
and simple to use with one hand
4. Provide aspiration so blood can be seen through the glass
cartridge

Breech-Loading, Metallic, Cartridge-Type, Aspirating #1 Used Syringe In Dentistry
-breech loading implies that the dental cartridge is loaded from the side
-a needle is attached to the barrel of the syringe at the needle adaptor
-the needle passes into the barrel and pierces the diaphragm of the local anesthetic cartridge

Aspirating Syringe
-the needle adaptor is sometimes inadvertently
discarded along with the disposable needle
-the harpoon is a sharp tip attached to the piston
and is responsible for penetrating the thick
silicone rubber stopper (bung) at the other end
of the cartridge

- negative pressure is applied to the thumb ring by
the
administrator, if blood enters the glass local anesthetic
cartridge (carpule) then the tip of the needle is
inserted into the lumen of a blood vessel
•chrome-plated brass and stainless steel
-incidence of positive aspiration is between 10-15% for some injections
-aspiration before injection of local anesthetic is accepted in the practice of dentistry and is overlooked to a great extent
-these syringes use the elasticity of the rubber diaphragm in the anesthetic cartridge to obtain the necessary negative pressure for aspiration

-multiple aspirations are possible with very little
effort due to a small metal projection that applies
pressure to the rubber diaphragm when the thumb
ring is depressed negative pressure aspiration
-this type of aspiration is as reliable as using the
harpoon to check for blood aspiration
Self-Aspirating Syringes
-Major factor for aspiration is the gauge of the
needle being used
-Most doctors using the harpoon-type syringe, retract
the thumb ring back too far and with excessive force
which frequently disengages the harpoon from the
silicone rubber stopper of the cartridge

-1st generation self-aspirating syringes required a thumb disk
which forced the operator to remove their index and middle
fingers from the thumb ring to the thumb disk to aspirate
-2nd generation self-aspirating syringes have removed this
thumb disk
-Dentists only need to stop applying pressure to the thumb
ring for aspiration; aspiration becomes very easy to do



Pressure Syringes-PDL (intraligamentary) injections make it
possible to achieve single tooth pulpal
anesthesia in the mandible when, in the past,
complete IANB was necessary
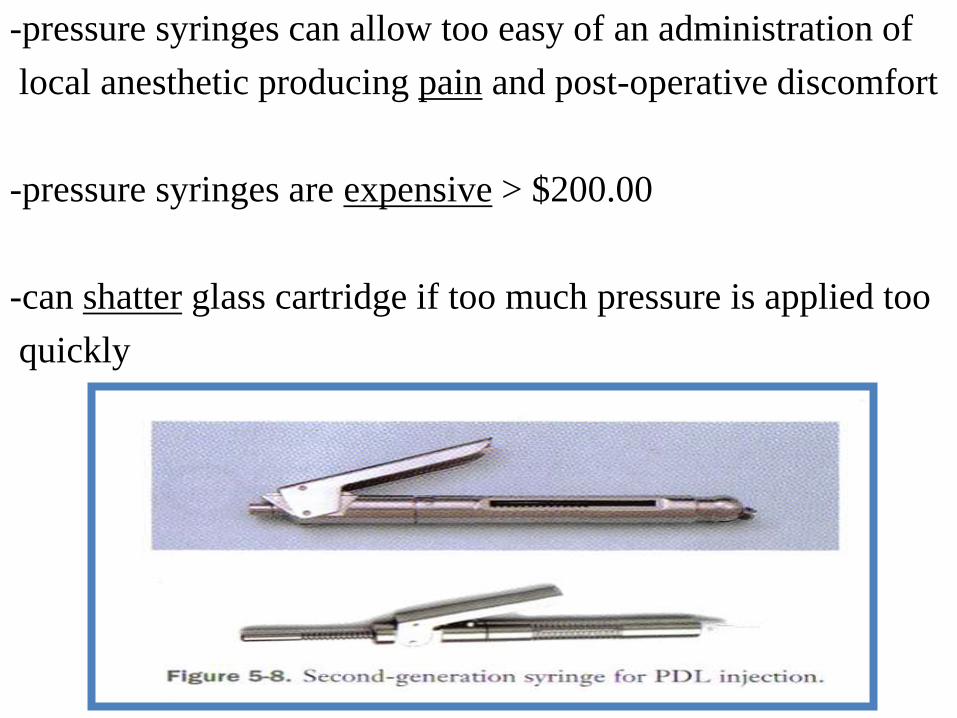
-pressure syringes can allow too easy of an administration of
local anesthetic producing pain and post-operative discomfort
-pressure syringes are expensive > $200.00
-can shatter glass cartridge if too much pressure is applied too
quickly
2000 psi Jet Syringes ($1,600)
-needle-less injection
-liquids forced through very small openings, called
jets, at very high pressure can penetrate skin or intact
mucous membrane
-Syrijet is the most popular used today
-Syrijet holds any 1.8 ml cartridge of local anesthetic

-Syrijet is calibrated to deliver .05 to .2 ml of solution at
2000 psi; traditional syringes deliver 600 psi maximum
-primary use is to obtain topical anesthesia before using a
needle
-regional nerve blocks/supraperiosteal injections are still necessary
-topical anesthetics provide the same effect at a fraction of
the cost
-patients complain of soreness where the 2000 psi hit their
tissue

Safety Syringe
-Aspiration is possible
-some brands come with an autoclavable
plunger and disposable self-contained
injection unit
-all dental safety syringes are made to be single use items
-sliding the index and middle finger forward against
the front collar of the guard makes the needle “safe”
by sliding a protective plastic sheath over the
needle tip that locks into place
-more expensive than reusable syringe units
-large disadvantage arises when it comes to re-
injecting; complication ensues due to the needle
tips newly acquired safety coping

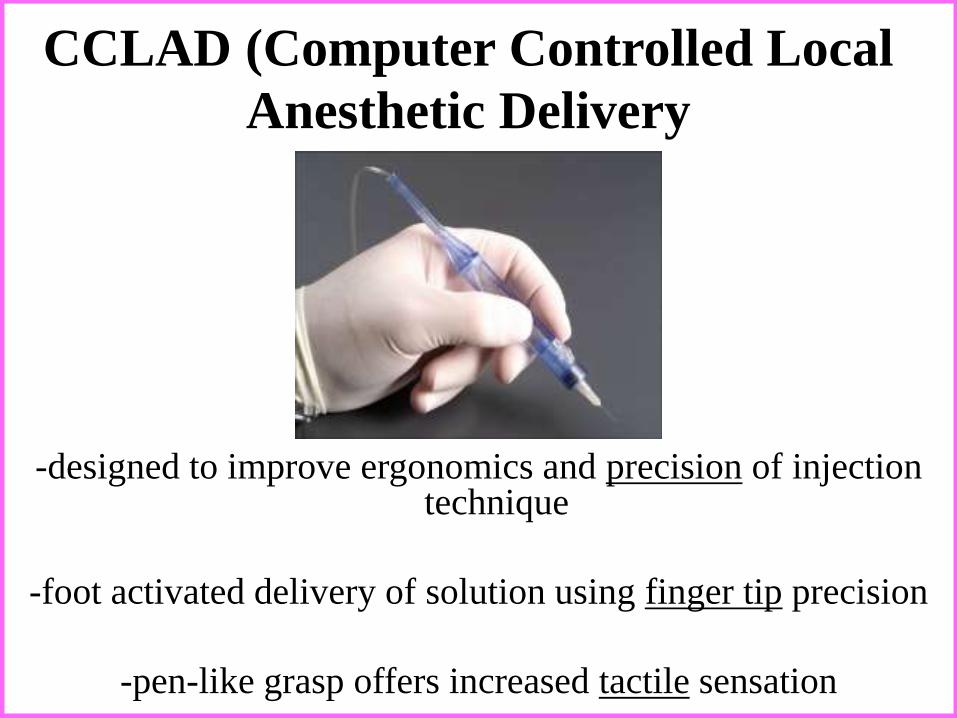
CCLAD (Computer Controlled Local
Anesthetic Delivery
-designed to improve ergonomics and precision of injection technique
-foot activated delivery of solution using finger tip precision
-pen-like grasp offers increased tactile sensation

-flow rates of solution delivery are computer
controlled and remain consistent
operator is able to focus attention on the position of
the needle tip while the motor of the machine delivers
local anesthetic at a preprogrammed rate of flow
50 Dentists were injected with traditional syringes and
The Wand; 48 of 50 Dentists preferred to be injected
again themselves with The Wand due to a reported
threefold decrease in the interpretation of pain
The Wand
-The Wand is less threatening to the patients visually
-allows two rates of delivery:
1) Slow: .5 ml/minute
2) Fast: 1.8 ml/minute
-releasing the foot rheo-stat will tell the machine to aspirate automatically; the aspiration cycle is approximately 4.5 seconds

-extremely high pressure in non-resilient
tissues cause (traditional syringe)
moderate/severe pain in most patients
The Wand eliminates a lot of this
discomfort by maintaining constant
pressure delivery of the solution
-less painful PDL, palatal, attached gingiva
injections

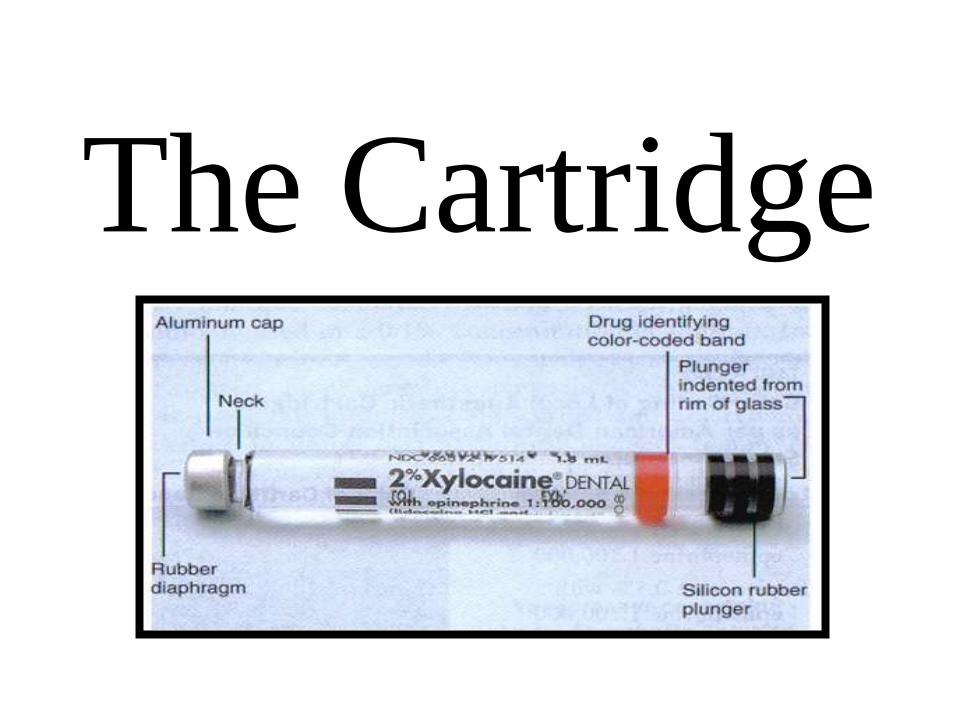
The Cartridge
Components of the CartridgeThe 1.8 ml dental cartridge consists of four parts:
1) Cylindrical glass tube
2) Stopper (Plunger, Bung)
3) Aluminum Cap
4) Diaphragm
Carpule = registered trade name for the dental cartridge introduced by Cooke-Waite laboratories
in 1920

-Rubber stopper should be lightly indented
-Flush or extruded stoppers: don’t use
-Aluminum cap holds the diaphragm in position
-Diaphragm is latex rubber through which the needle
penetrates the cartridge (no allergies ever reported)
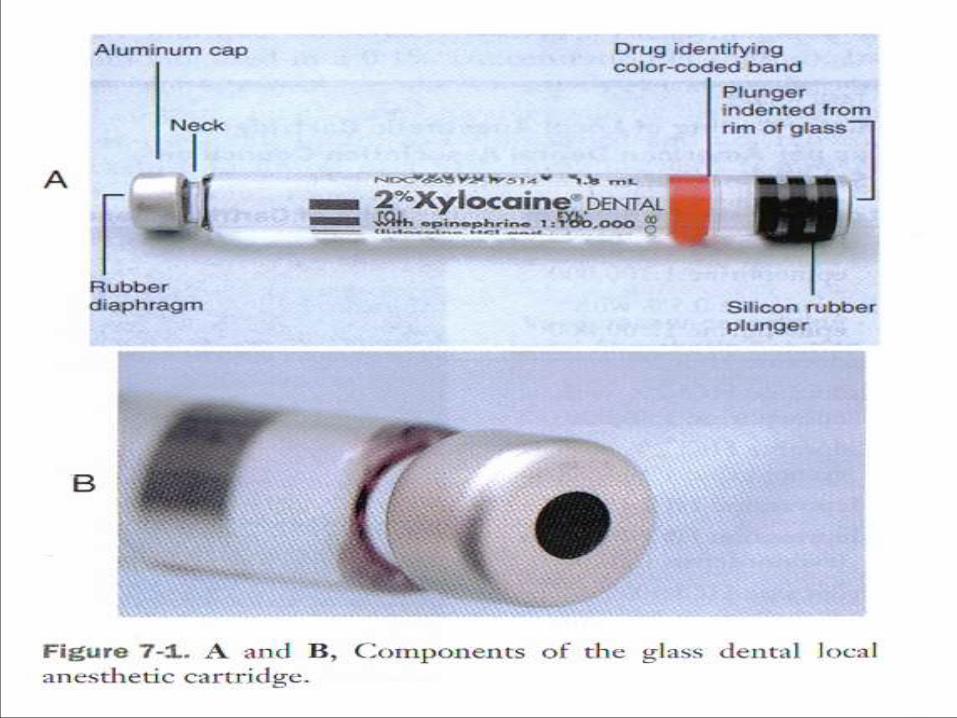
Parts of the Cartridge
-Liquid can diffuse through the diaphragm and contaminate the local anesthetic solution(alcohol common culprit)
-Mylar plastic label surrounds glass with content information and color coded band to identify the anesthetic


Composition of Local Anesthetic Cartridge

What is in the Cartridge?
-Local Anesthetic: provides anesthesia; resists heat
-Sodium Chloride: produces isotonicity with body tissue
-Sterile Water: provides volume only
-Vasopressor: increases safety, duration and depth of anesthetic
-Sodium (meta) Bisulfite: antioxidant (preservative)
-Methylparaben: bacteriostatic agent and antioxidant
-only found in multi-dose drugs, ointments, creams
-bacteriostatic, fungistatic and antioxidant
-removed due to single use and paraben allergies

Care and Handling-local anesthetic drug is stable and can be sterilized, heated, autoclaved, or boiled
without being broken down
-problem is that the diaphragm and vasopressor is heat labile and can easily be broken
down, so cartridges should not be autoclaved
-“blister packs” should be stored at room temperature and in the dark
-bacterial cultures taken off newly opened “blister packs” produce no bacterial growth
when cultured
-cartridges are ready to be used when removed from the package there is no need to
rub the diaphragm with alcohol
-cartridges should not be permitted to soak in alcohol or other sterilizing solutions
because the diaphragm will allow diffusion
Cartridge Warmers
-cartridge warmers are not necessary; the patient cannot
discern between warmed and room temperature local
anesthetic
-patients do not complain of the local anesthetic solution
feeling cold upon injection
-local anesthetics that are warmed too much, i.e., > 80 F will
be described as too hot or burning upon injection
-local anesthetic warmers are deceptive if they claim that the
injection will be less painful if the anesthetic is warmed

ProblemsBubble In The Cartridge: 1-2 mm bubble can be found in the
cartridge which is nitrogen gas that is inserted into the
cartridge when it is sealed to keep oxygen out; avoids
oxygen oxidizing the vasopressor
Extruded Stopper: liquid was frozen at some point leading to
extrusion sterile environment of the solution can no longer
be guaranteed; it only takes one day for alcohol to diffuse
through the diaphragm; alcohol is neurolytic and can cause
extended lengths of parasthesia; do not soak cartridges in
alcohol

Burning On Injection
1) Normal response to the pH of the drug
2) Cartridge contains sterilizing solution
3) Overheated cartridge (local anesthetic warmer)
4) Cartridge containing a vasopressor (decreased pH)
5) Vasopressor decreases the pH from 5.5 (plain) to 3.3 – 4.0
6) Sodium Bisulfite Sodium Bisulfate (much more acidic)
7) -ite -ate occurs by oxidation after local anesthetic expiration
-with the addition of silicone as a lubricant around the stopper instead of
paraffin this is not a problem anymore

Cracked Cartridge Glass
-there is no need to hit the thumb ring with excessive
force when engaging the stopper with the harpoon
-controlled pressure with the palm of the hand will
provide adequate engagement
-some have a tendency to engage the harpoon too
aggressively which is a bad habit that leads to
cracked glass cartridges


Additional Armamentarium
1) Topical Antiseptic: betadine or thimerosal; 8% of
Dentists use it and is considered optional; eliminates
post-injection infections
2) Topical Anesthetic: disguises the initial introduction of
the needle into the tissues when applied for a minimum
of 1 minute; if left for 2 to 3 minutes, profound topical
anesthesia is achieved; studies have shown that less than
10 seconds does not provide any more anesthesia than
placebo

The Needle
-most needles are stainless steel and disposable
-reusable needles have no place in the practice of Dentistry
-plastic hubs are not pre-threaded; metal hubs are pre-threaded
-a needle whose point is more centered on the long axis will have less deflection upon entry into soft tissues than a beveled needle

All needles have these components in common:
1) Bevel: point or tip of needle; long, medium and short
2) Shaft: long portion of the needle(diameter of lumen)
3) Hub: plastic/metal piece that attaches the needle to the syringe
4) Cartridge Penetrating End: perforates the diaphragm of the cartridge

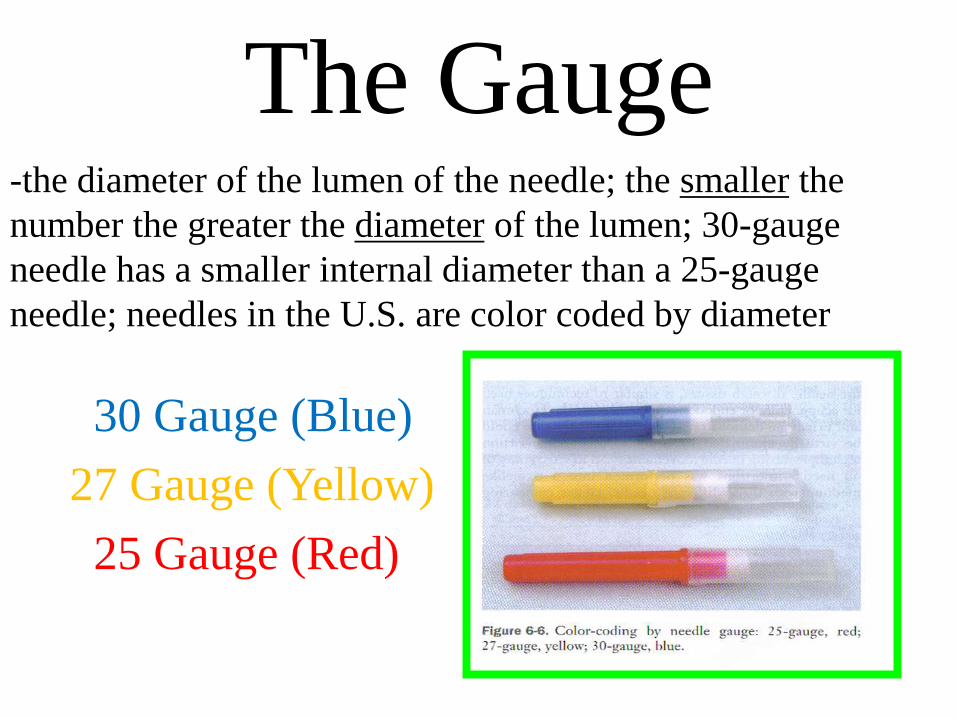
The Gauge-the diameter of the lumen of the needle; the smaller the
number the greater the diameter of the lumen; 30-gauge
needle has a smaller internal diameter than a 25-gauge
needle; needles in the U.S. are color coded by diameter
30 Gauge (Blue)
27 Gauge (Yellow)
25 Gauge (Red)

-Dentists think that using smaller gauge needles
will result in a less traumatic injection
experience by the patient which is false
-In 1972, Hamburg proved that patients could
not differentiate between 23, 25, 27 and
30-gauge needles

Larger gauge needles have advantages over smaller gauge needles:
(1less deflection of the needle tip results ingreater accuracy
2) less chance of needle breakage (separation)
3) easier aspiration of blood through the larger lumens
4) undetectable pain differences between 25 and30-gauge needles

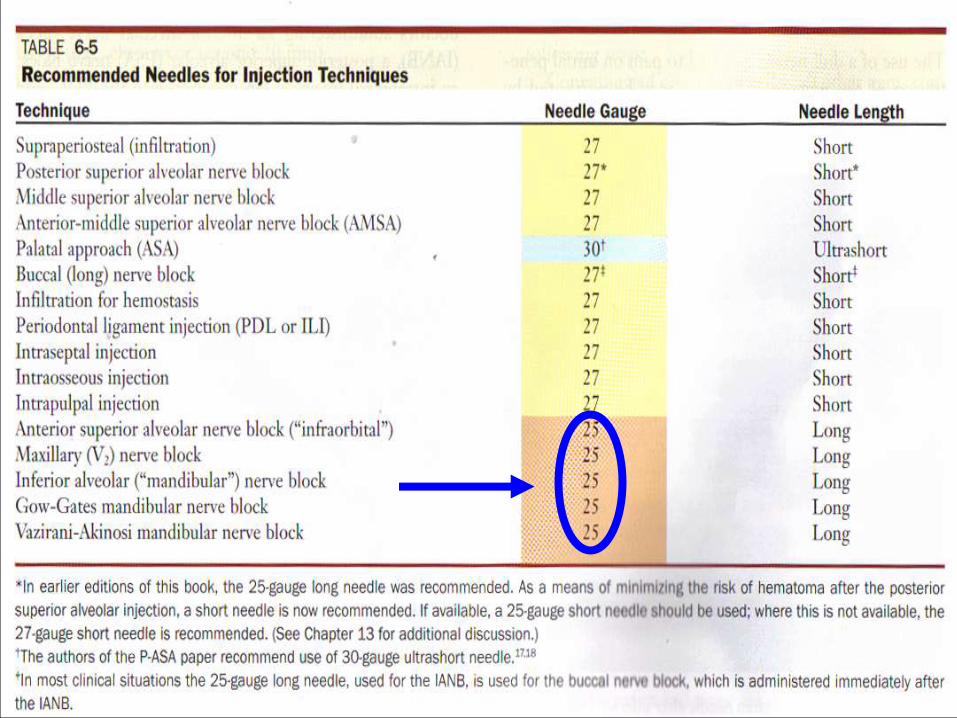
-25 gauge is the needle of choice for injections that
have a high potential for a positive aspiration
(PSA, IANB and Mental Block)
-30-gauge needles are not recommended for any
specific injection
Rotational Insertion Technique
(minimizes deflection)
Bi-rotational insertion technique
the operator rotates the needle in a back-and-forth rotational movement while advancing the needle through the tissues; traditional hand-held syringes cannot be rotated in this manner, however, The Wand can be rotated in this fashion results in less deflection, less force is needed for needle penetration

Length-there are three lengths to dental needles: long, shortand ultrashort
-average length of short needles: 20 mm (hub to tip)
-average length of long needles: 32 mm (hub to tip)
-needles should not be inserted to the hub unless absolutely necessary for the success of the injection
-hub is the most common area for breakage because this area has the highest level of stress
-when a needle is separated the elastic properties of the tissues permit a rebound effect that completely covers the needle (buries it)
-25 gauge long needle is the only needle any Dentist needs to perform any dental injections per Malamed(25 or 27-gauge short possible too)


Problems-Stainless steel needles dull after 3-4 penetrations into soft tissue causing more pain/post-operative discomfort; change your needle
-If needles are to be penetrated into soft tissue more than 5 mm then the needle should not be bent; bending needles weaken them
-No attempt should be made to change the direction of a needle when it is embedded into tissue; you should remove the needle and reinsert it completely
-Of 60 needles that separated and lead to litigation, 59 of them were 30-gauge short needles(probably inserted too far and above rules broken)

Separated Needle

Problems-Pain on withdrawal of needle could be due to “fishhook”
barbs due to errors in manufacturing or too hard contact
against bone
-Needle should be recapped immediately after it is withdrawn
from a patients mouth; avoids unintentional sticks
-Never put an uncapped needle on the tray for yourself or
someone else to inadvertently be stuck; always recap the
needle after you have given any injection