
BUKU SAKU STRATEGI KOMUNIKASI PENDIDIKAN DAN BUDAYA ANTI KORUPSI
description
KOMUNIKASI
DALAM KONTEKS BUDAYA
Oleh: Imas Rafiyah, S.Kp., MNS
Magister Peminatan Keperawatan Jiwa Fakultas Keperawatan Universitas Padjadjaran
Tujuan
Konsep dasar komunikasi dan budaya
Komunikasi western dan eastern
Komunikasi berbagai suku di Indonesia
Berkomunikasi dengan klien dengan latar belakang
berbeda
Pengembangan kemampuan seseorang dalam
berkomunikasi
DEFINISI DAN KONSEP
KOMUNIKASI DAN BUDAYA
KOMUNIKASI
BUDAYA
Cara hidup yang berkembang dan dianut oleh
sekelompok orang serta berlangsung dari generasi
ke generasi
Membentuk persepsi dan perilaku
BUDAYA
Bersifat kompleks meliputi
pengetahuan, keyakinan, seni,
moral, hukum, adat, dan
kemampuan serta kebiasaan
lainnya yang didapat
manusia sebagai anggota
masyarakat
(Tylor dikutip dalam Frisch & Frisch,
2007)
BUDAYA
Transmits meaning
Dipelajari
Disebarkan
Ever-changing
Dialogical
Mendefiniskan nilai-nilai
Mendefiniskan norma:
peran, hubungan
hak-hak dan kewajiban;
kepercayaan dan praktek atau perilaku
(Tylor dikutip dalam Frisch & Frisch, 2007)
KOMUNIKASI ANTAR BUDAYA
Komunikasi yang terjadi di antara orang-
orang yang memiliki kebudayaan yang
berbeda
BENTUK KOMUNIKASI ANTAR BUDAYA
Komunikasi antara
kelompok agama yang
berbeda
Komunikasi antara subkultur
yang berbeda.
Komunikasi antara kultur
yang dominan.
Komunikasi antara jenis
kelamin yang berbeda
KOMUNIKASI
WESTERN DAN EASTERN
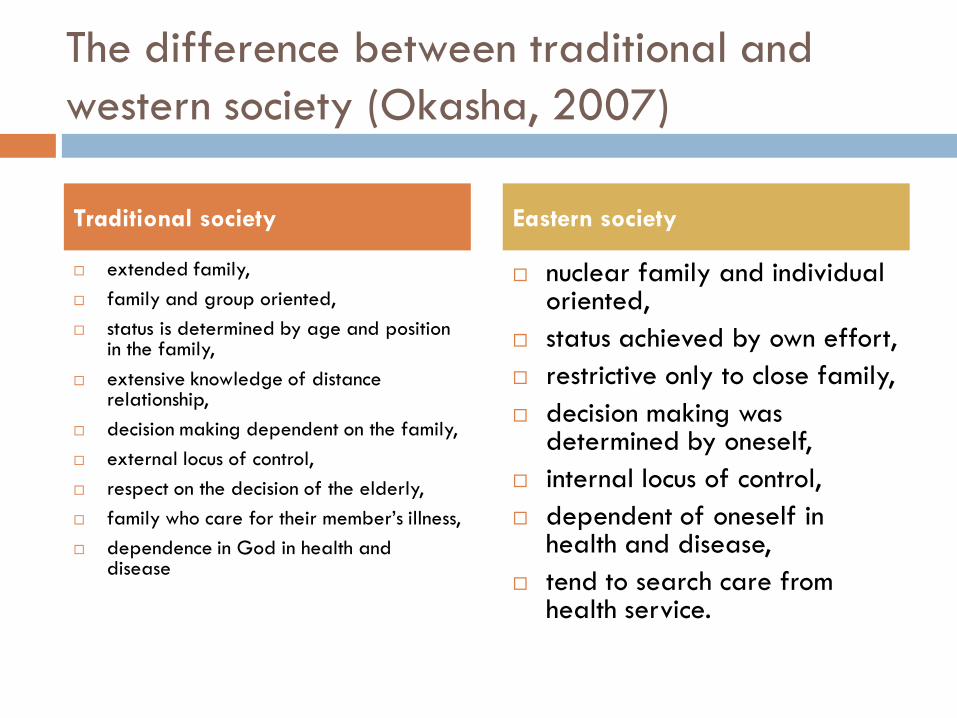
The difference between traditional and
western society (Okasha, 2007)
extended family,
family and group oriented,
status is determined by age and position in the family,
extensive knowledge of distance relationship,
decision making dependent on the family,
external locus of control,
respect on the decision of the elderly,
family who care for their member‘s illness,
dependence in God in health and disease
nuclear family and individual oriented,
status achieved by own effort,
restrictive only to close family,
decision making was determined by oneself,
internal locus of control,
dependent of oneself in health and disease,
tend to search care from health service.
Traditional society Eastern society
KOMUNIKASI BERBAGAI SUKU
DI INDONESIA
Suku Bangsa di Indonesia
By ethnicity there are approximately 300 ethnic group and by mother tongue they can be grouped in eight largest ethnicity including:
1. Javanese (52.1%) in Central and east Java,
2. Sundanese (19.3%) in West Java,
3. Minang (3.5%) in West Sumatra,
4. Maduranese (2.9%) in Madura island,
5. Banjar (2.4%) in Kalimantan,
6. Batak (2.3%) in North Sumatra,
7. Buginese (1.8%) in South Sulawesi, and
8. Balinese (1.7%) in Bali.
Five recognized religions in Indonesia including Islam (87%), Protestant (6.5%), Catholic (3.6%), Hindu (1.5%), and Buddhism (data not available)
(Hidayat, 2002).
Suku Sunda
Close relationship among neighboring families (Guinesas cited in Zevalkink et al., 1999).
Believe on value ―silih asih, silih asah, silih asuh‖, it means that people should care, love and guide each other (Suryani, n.d).
Social activities that are commonly done by women, those are volunteer for public health center, Islamic organization or ―pengajian‖, and rotating saving association or ―arisan‖. These activities can be the activities for making relationship or making relax (Niehof, 1998).
Budaya Sunda
Good health, economic security, and the well being of
loved ones, are considered enough for satisfaction.
illness is caused by inner imbalance that influence
functioning of the mind. They describe ―inner‖ as hawa
nafsu (climate of feeling),this climate is influenced by up
and down feeling rhythm, for example, anger is caused
by hot feeling
Muslim-Sundanese believes to ―ulama” (Islamic religious
functionaries) as local healers
(Horikoshi-Koe, 1979).
Budaya Sunda
mother is mostly primary caregiver for children.
(Adimihardja & Utja as cited in Zevalkink et al., 1999)
People help to others, particularly mother to her
children and it should be given voluntarily (Suryani, n.d).
Economic stress is also found in most Sundanese family.
Instable income and permanent job are rare in
Sundanese families(Chase-Lansdale & Owen, Gecas,
Greenberger, O‘Neill & Nagel as cited in Zevalkink et
al., 1999).
BERKOMUNIKASI DENGAN KLIEN
DENGAN LATAR BELAKANG BERBEDA
Nursing theory
MADELEINE LEININGER‘S CULTURE CARE: DIVERSITY
AND UNIVERSALITY THEORY
Pentingnya Memahami Budaya dalam
Komunikasi Keperawatan
Era globalisasi----banyak klien dari budaya
berbeda
Memahami klien-----membangun trust
Mengidentifikasi cultural need klien
Mencapai tujuan asuhan keperawatan dengan
cultural strategies
Intercultural caring (Wickberg & Eriksson, 2008)
Patients and nurses with different cultural backgrounds meet in nursing care that is not always experienced as caring.
The patients‘ expectations might not be met
Nurses feel frustrated when language problems, different cultural values and beliefs and lack of support and resources interfere with nursing care
The world is becoming more multicultural, and there are patients from different cultures in almost allcountries.
SETTING
KLINIK KOMUNITAS
Pengkajian Terkait Budaya
Suku bangsa, jenis kelamin, usia, agama, pendidikan, status ekonomi
Komunikasi: verbal dan non verbal
Bahasa
Pakaian dan penampilan
Makanan dan kebiasaan makan
Waktu
Penghargaan dan pengakuan
Hubungan
Nilai dan norma
Rasa kenyamanan diri dan ruang
Proses mental dan belajar
Kepercayaan dan sikap
Hambatan Komunikasi Terkait Budaya
Bahasa
Kebiasaan dan pola perilaku
Persepsi
Stereotip budaya
Cultural Miscommunication
Vokal
Pakaian
Gesture
Kontak mata
Jarak
Sentuhan
Diam
Perilaku sosial
Orientasi waktu
Patients’ Transcultural Needs and
Carers’ Ethical Responses (Dogan, Tschudin, Hot &Özkan)
This study was carried out in Göttingen, Germany.
Fifty Turkish people (described as patients) were asked about the care they had received from German health care personnel, and 50 German nurses and 50 German physiotherapists were questioned about care they had given to Turkish patients.
Significant findings were the needs of the Turkish patients for goodcommunication, physical contact and understanding of their culture-based expressions of illness.
The German nurses and physiotherapists expressed the need for language barriers to be minimized and for education in the specific culture of Turkish patients.
Suggestions for better transcultural health care paradigms are made for relating to patients from different cultures
Student nurses’ experiences of communication in
cross-cultural care encounters (Jirwe, Gerrwish, emami, 2010)
Aim : To explore student nurses‘ experiences of communication in cross-cultural care encounters.
Methods: Semi-structured interviews were undertaken a purposive sample of 10 final year students from one university in Sweden: five participants were from a Swedish background and five from an immigrant background.
Four themes were identified: conceptualizing cross-cultural care encounters, difficulties in communication, communication strategies and factors influencing communication. ‗
Cross-cultural care encounters involved patients from a different immigrant background to the nurse.
Student nurses experienced particular difficulties communicating with patients with whom they did not share a common language. This led to care becoming mechanistic and impersonal.
They were fearful of making mistakes and lacked skills and confidence in questioning patients.
Various strategies were used to overcome communication barriers including the use of relatives to interpret, nonverbal communication, gestures and artefacts.
Other factors which influenced communication included the student‘s attitude, cultural knowledge acquired through education and life experience.
Tips Komunikasi Efektif
Pengetahuan perawat tentang budaya sendiri dan
budaya lainnya
Hindari stereotiping terhadap klien
Kaji secara individual
(Frisch & Frisch, 2007)
PENGEMBANGAN KEMAMPUAN SESEORANG
DALAM BERKOMUNIKASI
Cultural Competency
Cultural competence is defined as a set of congruentbehaviors, attitudes, policies, and structures that come together in a system or agency or among professionals and enables the system, agency, or professionals to work effectively in cross cultural situations (Cross & colleagues in Flaskerud, 2007)
In these descriptions, skills, attitudes, and values are spelled out in three areas: cultural knowledge, cultural sensitivity, and collaboration with the community to be served.
(Flaskerud, 2007).
Cultural Competency
Cultural knowledge means actively learning about
the community—its ethnicities, languages, origins,
immigration or migration history, acculturation level,
economy, sources of income, family and social
structures and roles, value systems and beliefs,
education levels and literacy, geography, and
ecologic environment.
(Flaskerud, 2007).
Cultural Competency
Cultural sensitivity includes an ethic or a moral imperative to value and respect the beliefs, norms, and practices of the people to be served.
This begins with an awareness of our own cultural beliefs and practices and moves toward being non-judgmental and respectful in dealing with people whose culture is different than our own.
Culturally sensitive professionals possess capacities for warmth, empathy, and genuineness.
(Flaskerud, 2007).
Cultural Competency in Nursing
Cultural desire: want to be competent
Cultural awareness : self exploration
Cultural skill: ability to collect data
Cultural encompasses: professioanl face to face
interaction
SUATU PROSESFrisch & Frisch, 2007)
Daftar Pustaka
Dogan, H., Tschudin, V., Hot, I., & Ozkan, I. (2009). Patients‘ transcultural needs and carers‘ ethical responses. Nursing Ethics.
16(6), p. 683-696
Flaskerud, J., H. (2007). Cultural competence: What is it?. Issues in Mental Health Nursing, 28:121–123.
Hidayat, R., S. (2002, December). Women in Indonesia: Between ethnicity and religiosity. Seminar conducted at the
meeting of Women in Asia: Issues and Concerns, Chennai.
Horikoshi-Roe, H. (1979). Mental illness as a cultural phenomenon: Public tolerance and theurapeutic process among the
moslem Sundanese in West Java. Indonesia, 28, 121-138.
Jirwe, M., Gerrwish, , K., & Emami, A. (2010). Student nurses‘ experiences of communication in cross-cultural care encounters.
Scanadian Journal of Caring Sciencies, 24; 436-444.
Niehof, A. (1998). The changing lives of Indonesian women: Contained emancipation under pressure. Leiden, 2, 236-258.
Okasha, A. (2007). The individual versus the family: An Islamic and traditional societies perspective. In J. Cox., A. V.
Campbell, & B. Fulford (Eds.), Medicine of the person (pp. 110-124). Philadelphia, PA: Jessica Kingsley.
Suryani, E. (n.d). Pandangan hidup orang sunda. Retrieved January, 18, 2011 from http://resources.unpad.ac.id/unpad-
content/uploads/publikasi_dosen/ Adat&PandanganHidupOrangSunda.pdf.
Wickberg, A. & Eriksson, K. (2008). Intercultural caring – an abductive model. Scanadian Journal of Caring Sciencies 22;
485–496
Zevalkink, J., Riksen-Walraven, J. M., & Lieshout, C. F. M. Van. (1999). Attachment in Indonesian caregiving context. Social
Development, 8(1), 21-40.
TUGAS
Mahasiswa ditugaskan melakukan literatur review
tentang aplikasi praktek komunikasi terapeutik
yang peka budaya
Tugas dipresentasikan di kelas minggu depan.
TERIMAKASIH


















