Keratocones et implants phaques
16
KERATOCONES et IMPLANTS PHAQUES Dr CHACHIA.N 2 ème journées d’automne ASTOC KERATOCONE 22octobre 2016
-
Upload
nejib-chachia -
Category
Health & Medicine
-
view
55 -
download
0
Transcript of Keratocones et implants phaques

KERATOCONES et IMPLANTS PHAQUES
Dr CHACHIA.N2 ème journées d’automne ASTOC
KERATOCONE 22octobre 2016
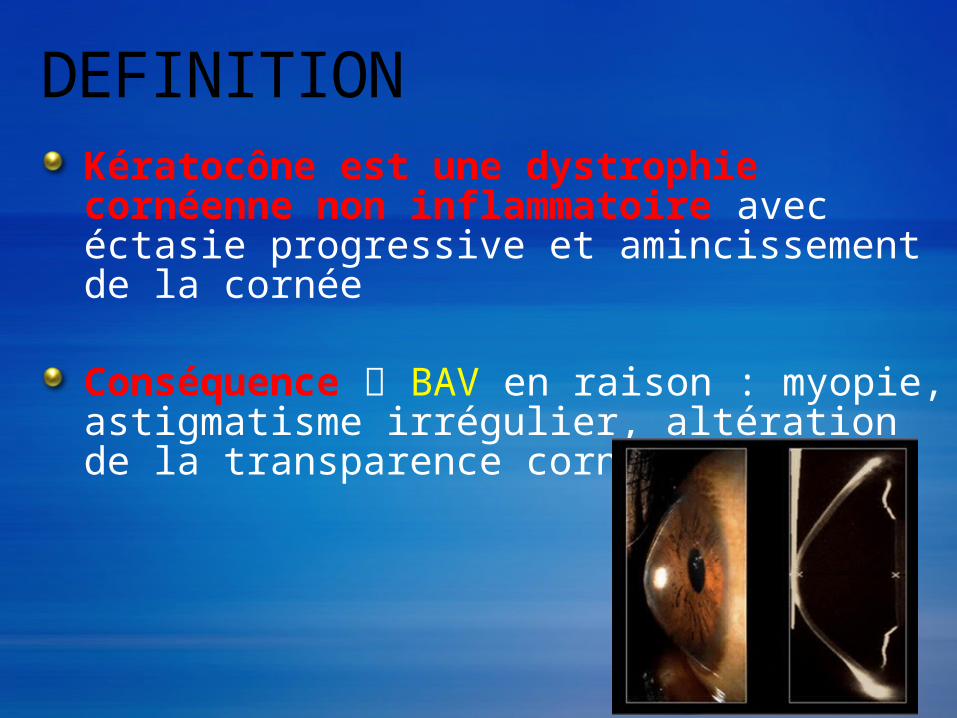
DEFINITIONKératocône est une dystrophie cornéenne non inflammatoire avec éctasie progressive et amincissement de la cornée
Conséquence BAV en raison : myopie, astigmatisme irrégulier, altération de la transparence cornéenne
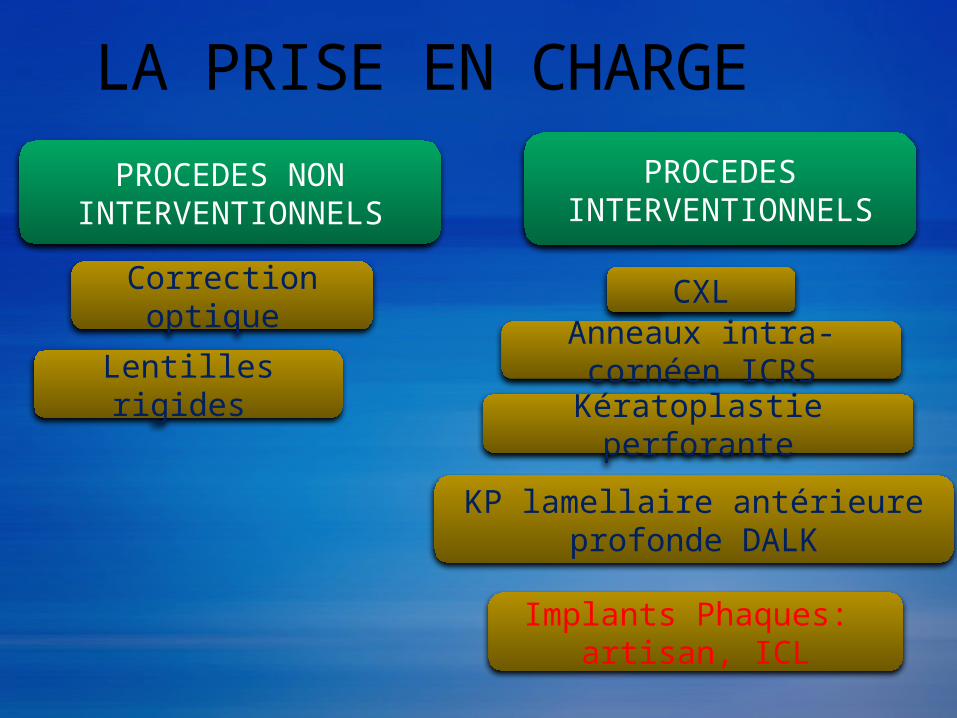
LA PRISE EN CHARGEPROCEDES NON
INTERVENTIONNELS
Correction optique
Lentilles rigides
PROCEDES INTERVENTIONNELS
CXL
Kératoplastie perforante
KP lamellaire antérieure profonde DALK
Anneaux intra-cornéen ICRS
Implants Phaques: artisan, ICL
GENERALITESo KERATOCONE s ’accompagne d’une amétropie
sphéro-cylindrique +/-majeure,
o Implants Phaques, sphériques ou toriques: alternative thérapeutique intéressante dans le kératocône,
o Indication discuté cas par cas,
o Principe: PLUS DE SPHERES ET MOINS DE CYLINDRES A CORRIGER
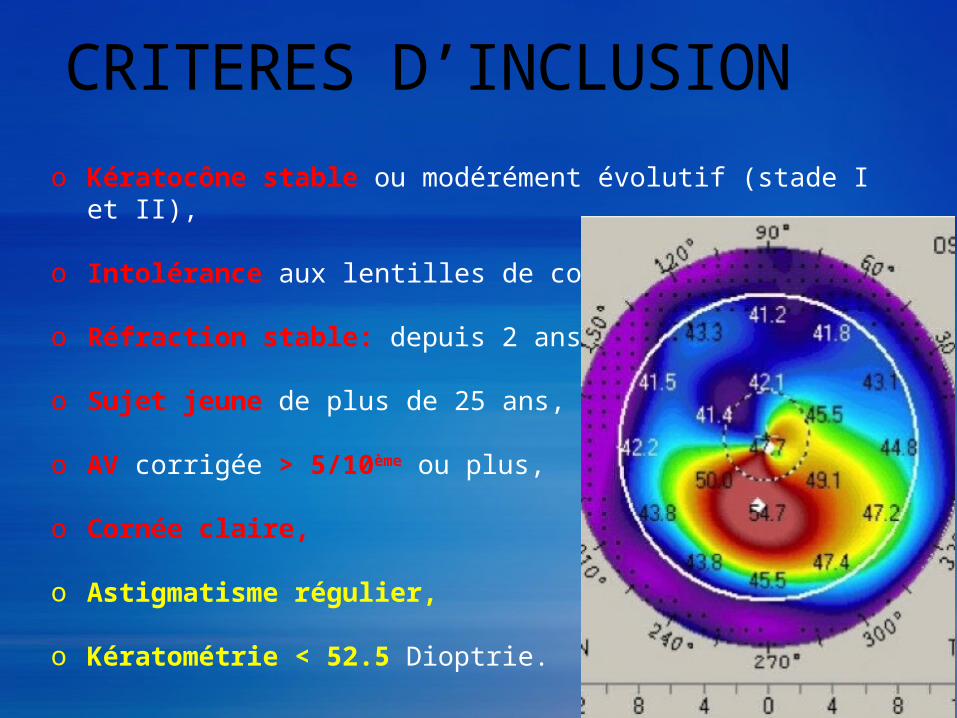
CRITERES D’INCLUSIONo Kératocône stable ou modérément évolutif (stade I et II),
o Intolérance aux lentilles de contact,
o Réfraction stable: depuis 2 ans,
o Sujet jeune de plus de 25 ans,
o AV corrigée > 5/10ème ou plus,
o Cornée claire,
o Astigmatisme régulier,
o Kératométrie < 52.5 Dioptrie.
CRITERES D’EXCLUSIONo Kératocône stade III ou IV,
o Sujet jeune de moins de 22 ans,
o Profondeur de CA <2.8 mm (ICL) et 3 mm (Artisan),
o Pachymétrie< 400µm,
o Densité endothéliale<2000cellules/mm²,
o Pathologies du segment antérieur (cataracte, glaucome, uvéite…), segment postérieur (DR, DMLA…),Pathologie générale.
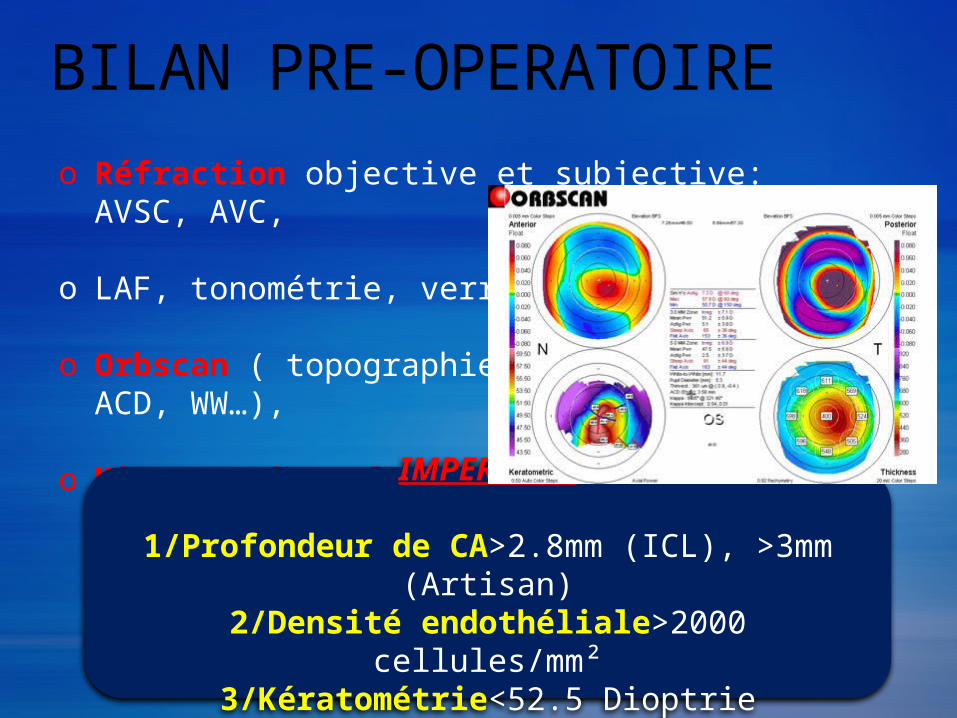
BILAN PRE-OPERATOIREo Réfraction objective et subjective: AVSC, AVC,
o LAF, tonométrie, verre à 3 miroirs …
o Orbscan ( topographie, pachymétrie, ACD, WW…),
o Microscopie spéculaire,
IMPERATIFS
1/Profondeur de CA>2.8mm (ICL), >3mm (Artisan)
2/Densité endothéliale>2000 cellules/mm²3/Kératométrie<52.5 Dioptrie
TECHNIQUE OPERATOIRE
POSITION DES IOL TORIQUES Incision sur l’axe le plus bombé++ Marquage pré-opératoire, Positionnement pré-opératoire
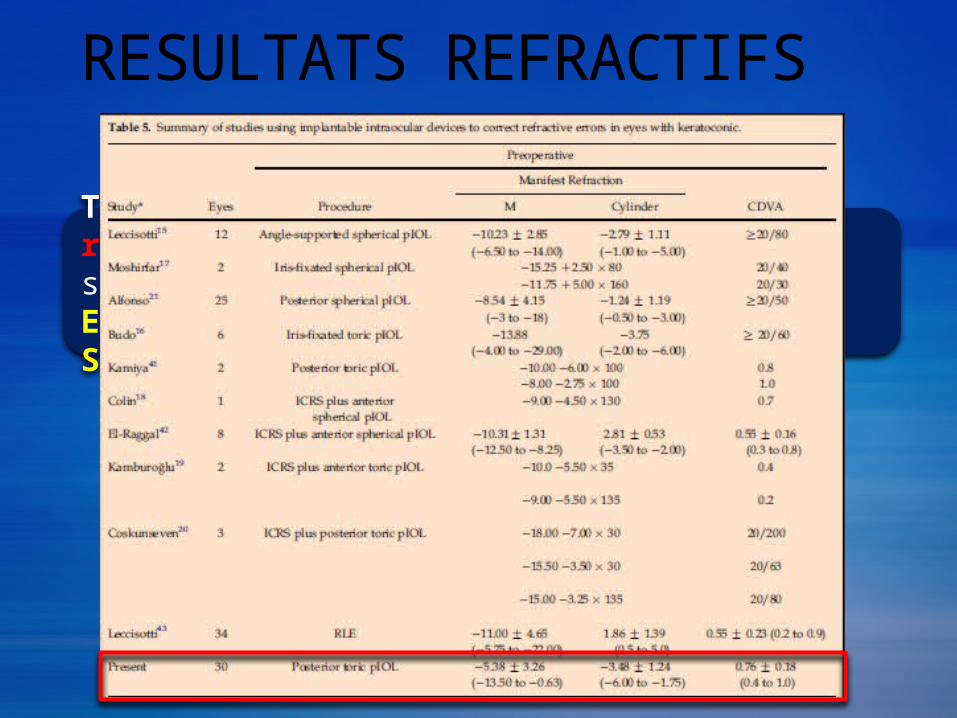
RESULTATS REFRACTIFS
Tous les travaux attestent d’excellents résultats réfractifs dans le KERATOCONE stable:EFFICACITE, SECURITE, PREDICTIBILITE ET STABILITE
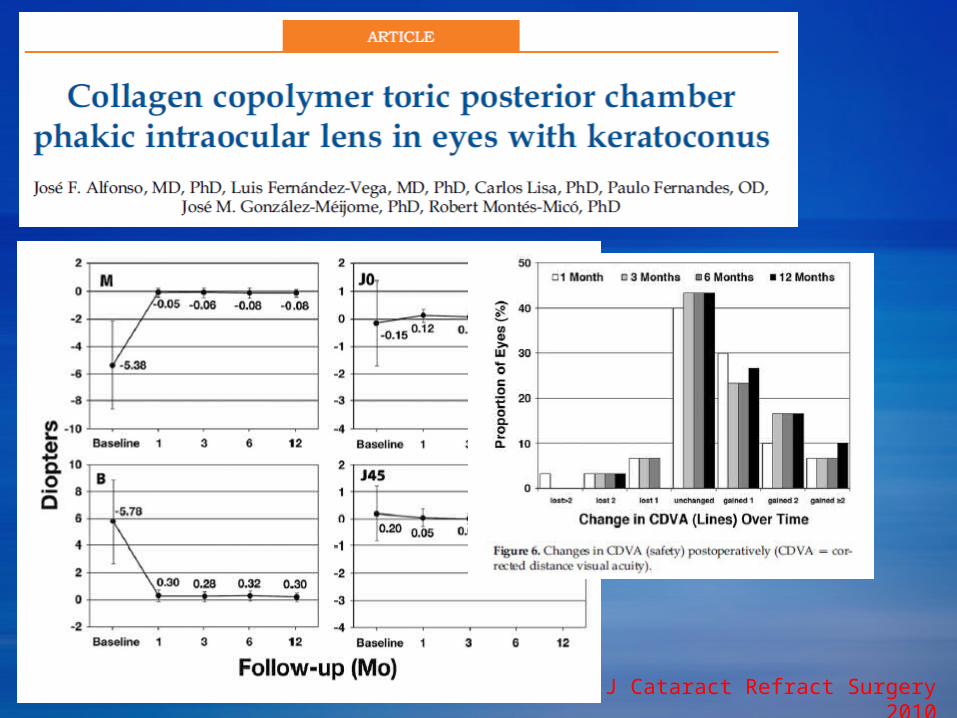
José et al. J Cataract Refract Surgery 2010
• Etude Prospective • 30 yeux (21 patients)• Sphère: -13,5 à -0,63 D• Cylindre: -1,75 à -6 D
Recul 12 mois
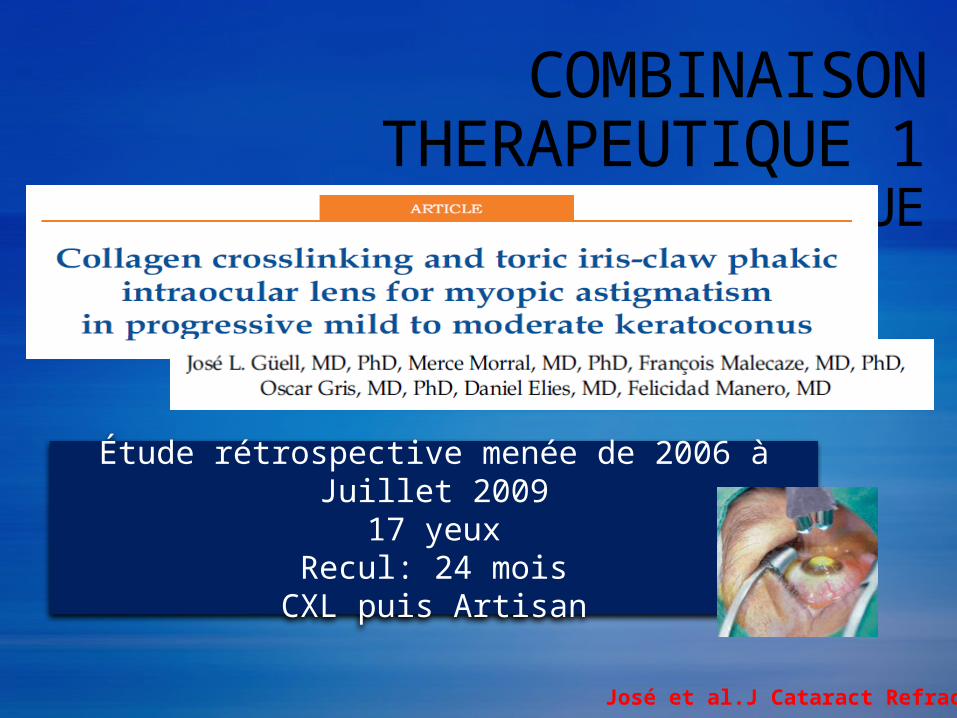
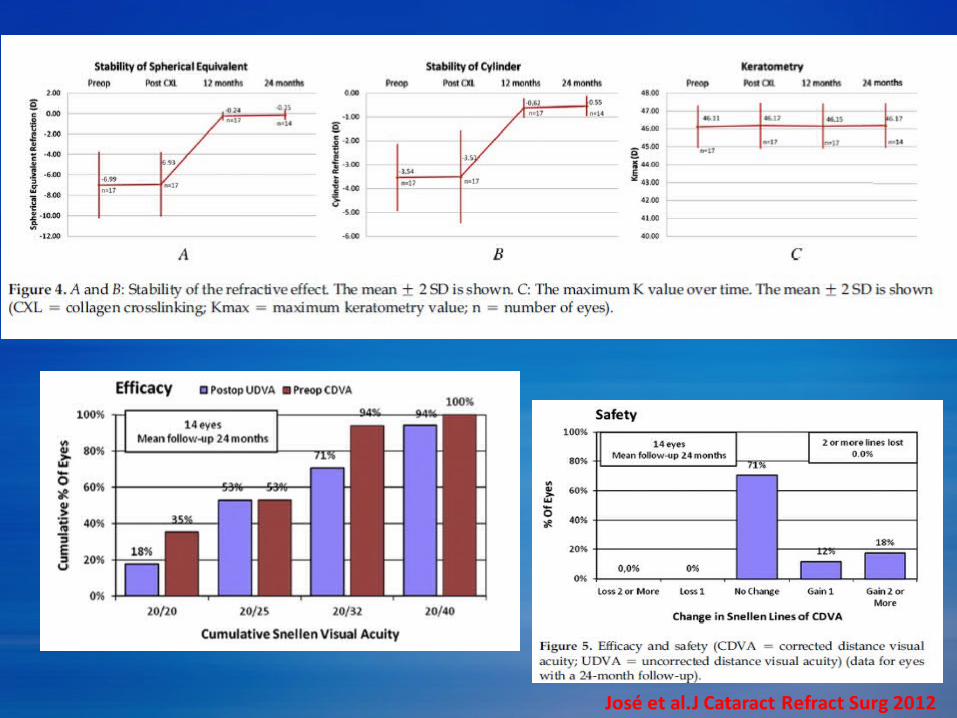
COMBINAISON THERAPEUTIQUE 1CXL et IMPLANT PHAQUE
Étude rétrospective menée de 2006 à Juillet 200917 yeux
Recul: 24 moisCXL puis Artisan
José et al.J Cataract Refract Surg 2012
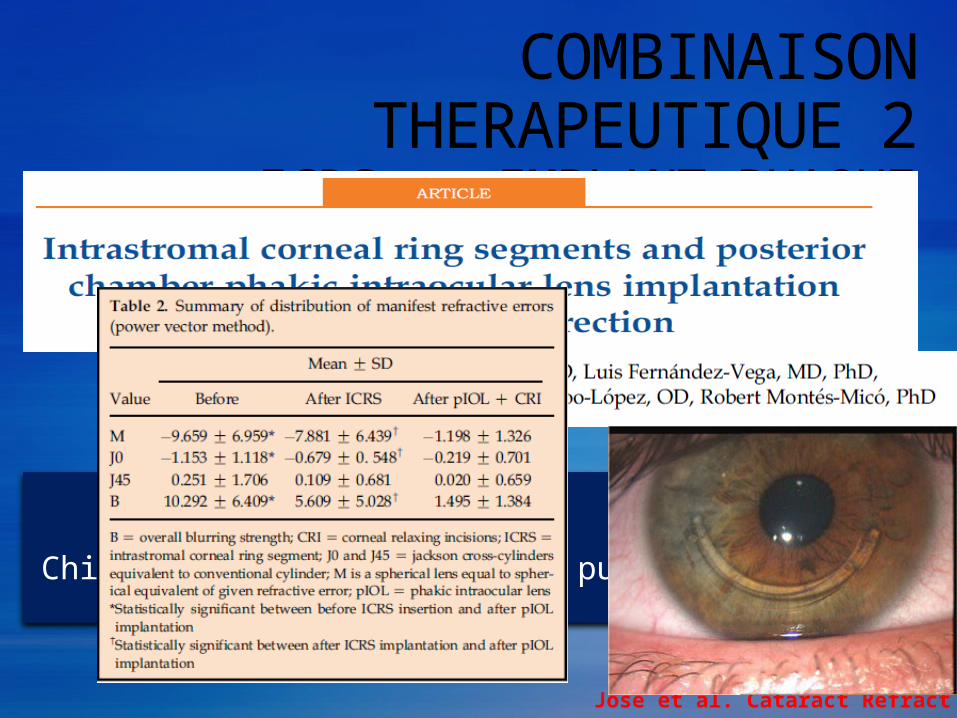
COMBINAISON THERAPEUTIQUE 2ICRS et IMPLANT PHAQUE
Étude prospective40 yeux
Chirurgie séquentielle ICRS puis ICL
José et al. Cataract Refract Surgery 2011
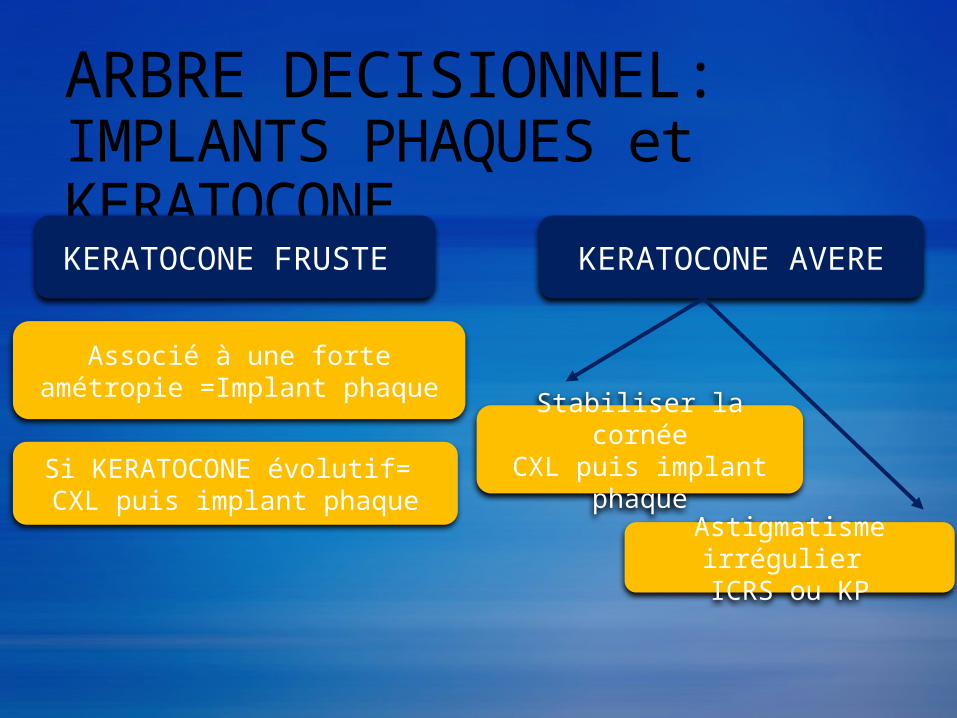
ARBRE DECISIONNEL: IMPLANTS PHAQUES et KERATOCONE
KERATOCONE FRUSTE
Associé à une forte amétropie =Implant phaque
Si KERATOCONE évolutif= CXL puis implant phaque
KERATOCONE AVERE
Stabiliser la cornéeCXL puis implant
phaqueAstigmatisme
irrégulier ICRS ou KP
TAKE HOME MESSAGE
o Une forte amétropie dans le KERATOCONE peut être axile ou de courbure
o Indication implant phaque doit être prudente: KERATOCONE stable, PLUS DE SPHERES MOINS DE CYLINDRES
o Astigmatisme irrégulier important= mauvaise indication
o Information du patient est FONDAMENTALE
o Surveillance post-opératoire du KERATOCONE est NECESSAIRE