Jurding Mata
53
Pathogenesis and Clinical Implications of Optic Disk Hemorrhage in Glaucoma Pembimbing : Prof. Dr. dr. H.H.B. Mailangkay, Sp. M Oleh : Daniela A. (2012-061- 001) Argya Ayu P. (2012-061- 002) Christine V. (2012-061- 003) Tony (2012-061-004)
-
Upload
christine-verina -
Category
Documents
-
view
22 -
download
0
description
Jurnal Reading Oftalmologi
Transcript of Jurding Mata
-
Pathogenesis and Clinical Implications of Optic Disk Hemorrhage in Glaucoma
Pembimbing :Prof. Dr. dr. H.H.B. Mailangkay, Sp. M
Oleh :
Daniela A. (2012-061-001)
Argya Ayu P. (2012-061-002)
Christine V. (2012-061-003)
Tony (2012-061-004)
-
Introduction
1st reported by Bjerrum et al reported with term Glaucoma Hemorrhagicum1970, revisited by Drance et al splinter hemorrages in open angle glaucoma patientsInvestigated the association between disk hemorrhages and glaucomatous damageToday (widely accepted) : disk hemorrhages = 1 of most important risk factor developing and progression of glaucoma and ocular hypertension -
Prevalence and Incindence
Disk hemorrhage in normal population = 0 1,4%Disk hemorrhage in glaucoma or ocular hypertension patients = 2 33,4%Therefore more commonly occurs in glaucoma or ocular hypertensive eyesCan also be found in case of subclinical structural loss of retinal nerve fiber layer (RNFL) thicknessNormal patients need to be evaluated with caution -
Open Angle Glaucoma: Normal tension vs. High tension
Based on data resulted from methodological difference disk hemorrhage more prevalent in open glaucoma with normal tension (NTG)
The prevalence in NTG = 20.5% 33.3%,
In HTG = 8.3% 17.6%
Therefore, 2 to 5 times more frequent in NTG than in HTG
Suh and Park NTG (33.3% prevalence) and HTG patients (17.6% prevalences)
Furthermore, overall probability reached 45.5% in NTG and 23.2% in HTG
Suggesting, found in up to half of eyes with NTG and about a quarter of those with HTG
-
Angle-closure Glaucoma
Disk hemorrhage prevalence of primary angle-closure glaucoma ranged between 0.5% and 5.7%Lan et al disk hemorrhage in primary angle-closure glaucoma to be associated with progression of glaucomatous optic neuropathy & visual field defects -
Differential Diagnosis
Can also occured in:
Posterior vitreous detachment
Optic disk drusen
Vascular occlusive disease of the retina
Non-glaucomatous optic neuropathies
Also correlated with:
Diabetes and hypertension
Leukemia
SLE
Can be distinguished from ocular or systemic condition by = absence of any sign of papillitis or presence of vitreoretinal abnormalities, or non-glaucomatous optic neuropathy
-
Appearance and Location
Typically splinter-shaped (thin and oriented perpendicular to the disk margin)If extravasation is abundant flame- or fan-shapedThese are result of the orientation of the RNFL axonsOptic disk hemorrhages located on the optic disk margin (laminar or prelaminar tissue), cross the optic disk margin, or on the peripapillary retinaIf hemorrhages is at the lamina cribosa level close relation to the location of the lamina cribosa pores tissue remodelling change in pore morphology -
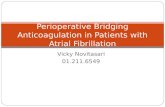
59-year-old male, open-angle glaucoma with normal tension patient had two episodes (A, C ) of disk hemorrhage in the inferotemporal area of the lamina cribrosa within a 1-year period. After absorption of the disk hemorrhage, a clear laminar pore was observed in the area where the hemorrhage occurred (B, D). Visual eld progression in the corresponding region of disk hemorrhages was noted in the deviation plot (E, F)
-
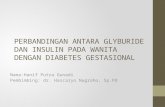
A 54-year-old female, open-angle glaucoma with normal tension patient had two episodes (B, C ) of disk hemorrhage in the temporal (B) and inferior (C ) areas of the lamina cribrosa within a 20-month period. Compared with the pre-hemorrhage photograph (A) of the areas of the proximal portions of the hemorrhages, the lamina cribrosa pores became prominent (D, black circles) after absorption of the hemorrhages, indicating that there must have been a tissue remodeling process around the pores. Visual eld progression in the corresponding region of disk hemorrhages was noted in the pattern deviation plot (E, F)
-
A 60-year-old male, open-angle glaucoma with normal tension patient showed a change in the lamina cribrosa pores (inside of the circle) near the area of the disk hemorrhage. The pores became more prominent (A, B)
- Peripapillary usually associated with RNFL defectA recent study lamina cribrosa type is signicantly more common in myopic eyesMost often located in the inferotemporal & superotemporal area of optic disk (FACT: early glaucomatous optic disk change typically develop there)
-
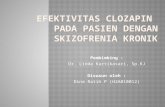
A peripapillary-type disk hemorrhage was found on the border of the inferotemporal wedge-shaped retinal nerve ber layer (RNFL) defect in a 58-year-old female open-angle glaucoma with normal tension (NTG) patient (A). Another 60-year-old female NTG patient with superotemporal and inferotemporal RNFL defects showed a peripapillary-type disk hemorrhage on the border of the inferotemporal RNFL defect (B).
-
Timing, Duration and Recurrence
Frequently increase from ealry stage of glaucoma to the moderate stage decrease as the disease progress to advanced stageDisk hemorrhage = transient, Persisting weeks several months (most disappearing within 2 months of onset) -
Detection Methods
Often missed therefore, careful examination is necessary
Methods = ophthalmoscopy and stereophotography
Studies better detected using stereoscopic disk photography than by clinical examination
In Ocular Hypertension Treatment Study (OHTS) only seen on disk photograph
Several studies (including the Early Manifest Glaucoma Trial (EMGT)) clinical and photographic detection meets good agreement (range 55 61%)
This suggest can be found in both methods (for prognostic importance, both detection should be used)
-
Pathogenesis and Clinical Implications of Optic Disk Hemorrhage in Glaucoma
-
Pathogenesis
Associated pressure around the optic nerve headDisk hemorrhage does not develop in all patients with open angle glaucoma or ocular hypertensionThe pathogenesis remains unclearThere are four biomechanical forces influencing the lamina cribrosa and surrounding tissue:intraocular pressure (IOP),Cerebrospinal fluid pressure,arterial pressure, andvenous pressure - Intraocular pressure and cerebrospinal fluid pressureDisk hemorrhage is not dependent on the IOP. Disk-hemorrhage prevalence in NTG to be higher than that in HTG.Studies by Healy et al and Kitazawa et al show that the prevalence of disk hemorrhage in ocular hypertension was similar to that in normotensive eyes from the general population.
- Kitazawa et als study : compared two types of glaucoma
patients, bleeders (those who tend to develop disk hemorrhage),
andnon-bleeders (those who do not tend to develop disk hemorrhage),
and found that bleeders eyes bleed and rebleed despite IOP
reduction by anti-glaucoma treatment, especially among NTG
patients.
The recent EMGT study also showed that the occurrence of optic disk hemorrhage did not change after administration of IOP lowering medication
- Miyake et al, studying both a NTG group and a HTG group, found that the incidence of disk hemorrhage decreased after trabeculectomy in both populations.Incidences of disk hemorrhage decreased 33% 6% among HTG patients 42% 23% in NTG patients.HTG eyes with higher postoperative IOP exhibited a much greater incidence of disk hemorrhage than did the lower postoperative IOP group. Also, a recent review of the OHTS revealed that IOP reduction reduced the risk of disk hemorrhage, suggesting a close relationship between IOP and optic disk hemorrhage.
- The lamina cribrosa, an important structure for elucidating the biomechanical background of disk hemorrhage, consists of 6-10 layers of connective tissue sheets, each sheet containing between 200 and 400 pores.The lamina cribrosa reportedly acts as a barrier effecting a translaminar pressure gradient between cerebrospinal fluid pressure and IOP. In a recent study the lamina cribrosa was significantly thinner in NTG patients with disk hemorrhage than in those without. A thinner lamina cribrosa provides less connective tissue support to the axons, thus resulting in steeper translaminar pressure gradients and high IOP related stress on the optic nerve head.
- Moreover, disk hemorrhage develops commonly in superior and inferior areas of the lamina cribrosa that contain large pores with less connective tissued areas that are more susceptible to mechanical damage.This suggests that disk hemorrhage correlates with IOP-related mechanical properties. Certainly, the lamina cribrosa is not a static, but a dynamic, structure that pulsates with the beating of the heart and blood pressure variations.IOP variations, for example, exaggerate backward bowing of the lamina cribrosa, during which a shearing stress on the nerves and capillaries is applied at the level of the lamina cribrosa pores.Notably, one study suggested that stretching of the anterior capillaries consequent upon posterior bowing of the laminar cribrosa causes disk hemorrhage.Another suspected, but little understood, cause of disk hemorrhage done that also acts by way of the translaminar pressure gradients cerebrospinal fluid pressure. Further studies are warranted.
- Arterial pressure and venous pressureThere might be other factors related to disk hemorrhage. Systemic arterial pressure, for example, might influence arterial pressure on the optic nerve head.Kim et al showed that for NTG patients, hypertension was the only statistically significant disk-hemorrhage risk factor among various parameters including IOP, diabetes, and aspirin use. Increased venous pressure from valsalva or head down posture also might increase the likelihood of disk hemorrhage, directly or indirectly, by way of IOP elevation through heightened episcleral venous pressure and choroidal expansion. Little is known, however, about the relationship between disk hemorrhage and the pressure in blood vessels on the optic nerve head, and further study willbe needed.
- Other factors associated with optic disk hemorrhageAlong with the four types of pressure on the optic nerve head, other vascular abnormalities, including systemic and ocular vascular diseases and primary vascular dysregulation (PVD), might also be related to disk hemorrhage.Other vascular abnormalitiesSystemic vascular abnormalities. Many studies have explored the possible association of the various systemic vascular abnormalities (including diabetes, migraine, nail bed hemorrhage, PVD, aspirin use, and platelet aggregation inhibition) with optic disk hemorrhage, though the results have been mostly inconclusive.Recently, as noted earlier, systemic hypertension was demonstrated to be an important risk factor associated with optic disk hemorrhage.
- Ocular vascular disease. Microinfarctions within the optic nerve head, retinal circulation disorder, and decrease of capillary perfusion pressure at the optic nerve head also have been evaluated. Two of these studies found a higher frequency of disk hemorrhage in patients with both branch retinal vein occlusion and NTG. This suggests that some cases of NTG, especially those involving disk hemorrhage, share a common pathophysiology with branch retinal vein occlusion.
- MiscellaneousDisk hemorrhage also is associated with advanced age and, controversially, with gender. Previous studies on open-angle glaucoma have identified a female preponderance, whereas Suh and Parks recent longitudinal study on a large population of open-angle glaucoma patients found no such sex correlation.The purported relationship between central corneal thickness and the development of disk hemorrhage in glaucoma patients is controversial
-
Morphologic Associations
zone perpapillary atrophy (PPA)A number of studies suggest that disk hemorrhage tends to occur in areas of the eye having the greatest zone PPA width
-
Morphologic Associations
RNFL and neuroretinal rim areaDisk hemorrhage has been strongly associated with:
Rim notching
Small neuroretinal rim, and
RNFL defects
RNFL defect border is an active site of damage and that its enlargement causes disruption of the capillary network, and finally, optic disk hemorrhage
-
Morphologic Associations
Other morphologic parametersJonas et al found that morphologic factors
not associated with disk hemorrhage:
disk size and shape,
zone PPA,
retinal vessel diameter, and
cup depth
Associated with disk hemorrhage:
Neuroretinal rim area and
zone PPA
-
Morphologic Associations
Other morphologic parametersFor patients with unilateral disk hemorrhage, the probability that the contralateral eye will develop optic disk hemorrhage is as high as that of the affected eye
-
Glaucoma Progression and Optic Disk Hemorrhage
SignificanceDisk hemorrhage is of clinical importance because its presence is an important prognostic factor for glaucoma progression
Glaucoma progression is associated with optic disk hemorrhage in both HTG patients and those suspected of it, as well as in NTG patients
-
Glaucoma Progression and Optic Disk Hemorrhage
Several points concerning the correlation between optic disk hemorrhage and glaucoma progression:The time relationship between glaucoma progression and disk hemorrhage
The method of detecting glaucoma progression and relationship between recurrent optic disk hemorrhage and glaucoma progression.
-
Glaucoma Progression and Optic Disk Hemorrhage
Glaucoma progression detected before and after optic disk hemorrhageVarious studies have addressed glaucoma progression after disk hemorrhage
Data from ocular hypertension patients with a median follow-up of more than 8 years indicate that disk hemorrhage represents an independent risk factor for HTG development, even after adjusting for other factors including corneal thickness, age, and cup:disk ratio.
-
Glaucoma progression detected before and after optic disk hemorrhage
Recent review found that eyes with optic disk hemorrhage manifested visual eld progression that was twice as rapid as those without.Disk hemorrhage should therefore be considered one of the risk factors for progression of ocular hypertension and warrant frequent monitoring and more aggressive treatment.
Not all patients with optic disk hemorrhage, however, show glaucoma progression -
Glaucoma progression detected before and after optic disk hemorrhage
Meanwhile, the recent advent of sophisticated imaging devices, including OCT and confocal scanning laser ophthalmoscopy, has enabled early diagnosis and detection of progressive glaucomatous change.Limitation of the conventional functional and imaging devices is their delay in detecting post-hemorrhage glaucoma progression. -
Glaucoma progression detected before and after optic disk hemorrhage
Functional damage and their corresponding visual eld changes take time to develop in early-to-moderate glaucoma, and mild RNFL thinning maybe undetectable on optic disk and RNFL photographs. Conclusion: OCT and confocal scanning laser ophthalmoscopy might be more useful for detecting glaucoma progression after optic disk hemorrhage. -
Glaucoma progression detected before and after optic disk hemorrhage
Glaucoma may develop prior to detection of optic disk hemorrhage. Law et al found that all eyes with pre-existing focal rim notches showed subsequent disk hemorrhage at or adjacent to the notches after a median time to progression of 21.5 months. -
Glaucoma progression detected before and after optic disk hemorrhage
This can be explained by the fact that a neural rim notch and disk hemorrhage are different manifestations of an underlying degenerative process corresponding to a localized geographic area of the optic disk and its surroundings.Further, that expansion of the RNFL defect causes disruption of the capillary network, resulting in optic disk hemorrhage. -
Glaucoma progression detected before and after optic disk hemorrhage
Conclusion:Rapid, localized disease progression predisposes to optic disk hemorrhage, and disease progression accelerates after disk hemorrhage
So disk hemorrhage can be a marker of rapid glaucoma progression
-
Glaucoma progression detected before and after optic disk hemorrhage
It remains unclear whether optic disk hemorrhage has a causative role in disease progression.
The extravasated blood is known to be neurotoxic
-
Recurrent Optic Disk Hemorrhage
Several studies had evaluated the relationship between glaucoma and optic disk hemorrhage:Eyes with recurrent optic disk hemorrhage had a more than two-fold greater chance of progression than single-disk hemorrhage eyes (Kim & Park et al)
Open-angle glaucoma eyes with recurrent optic disk hemorrhage had a higher cumulative probability of progression of RNFL loss than eyes with single-disk hemorrhage (Suh, et al)
-
Recurrent Optic Disk Hemorrhage
Conclusion:Eyes with reccurent disk hemorrhage had more rapid and extensive progression of glaucoma than those with single-disk hemorrhage
- Hendrickx et al found that patients with HTG showed a
significant decrease in the number optic disk hemorrhages after
IOP-reducing therapy, but not NTG patientsMiyake et al demonstrated
that the frequency of disk hemorrhage decreased significantly in
both NTG and HTG patients after trabeculectomy with mitomycin C
Effect of Treatment
- EMGT study found that the presence or frequency of disk hemorrhage was not related to IOP-lowering therapy either before or after controlling for associated factors, including IOP at the baseline or during follow-upThis suggests that disk hemorrhage might not be stopped by IOP-lowering therapy and that, correspondingly, hemorrhage might not be a sign of insufficient IOP reduction
- Medeiros et al noted that IOP reduction had a beneficial effect in slowing the rates of progression of visual field loss in eyes with optic disk hemorrhagePrata et al argued that IOP reduction should not be included as a significant risk factor for visual field progression after disk hemorrhage in glaucomatous eyes, but that baseline visual field mean deviation and older age should
- A possible explanation for the discrepancy is that the study by Medeiros et al had longer mean follow-up period than that by Prata et al (8.2 years vs 3.8 years) and had a higher degree of IOP reduction (5.6 mm Hg vs 2 mm Hg) as wellTherefore, we can suppose that glaucoma progression after disk hemorrhage can be halted by a greater degree of IOP reduction and a longer follow-up period.
-
Conclusions
Optic disk hemorrhage is more commonly detected in NTG than in HTG, but hemorrhage can also be detected in almost a quarter of HTG patients by more frequent and careful examination.The development of disk hemorrhage may be associated with the biomechanical circumstances of the lamina cribrosa and surrounding tissues, including the IOP ecerebrospinal pressure gradient, arterial pressure, and venous pressure. - Most disk hemorrhages are detected within 5 years of follow-up, and half are detected within 1 year.Disk hemorrhage can be amarker of glaucoma progressionin that rapid, localized disease progression predisposes to disk hemorrhage, and the subsequent disease process is accelerated after disk hemorrhage.
- Recurrent disk hemorrhage is correlated with rapid structural progression of glaucomatous damage.IOP-lowering therapy can help to halt glaucoma progression after disk hemorrhage