





Languages
Pages
Legal

Pathogenesis and Clinical Implications of Optic Disk Hemorrhage in Glaucoma
Pembimbing :Prof. Dr. dr. H.H.B. Mailangkay, Sp. M
Oleh :
Daniela A. (2012-061-001)
Argya Ayu P. (2012-061-002)
Christine V. (2012-061-003)
Tony (2012-061-004)
Introduction
1st reported by Bjerrum et al reported with term Glaucoma Hemorrhagicum1970, revisited by Drance et al splinter hemorrages in open angle glaucoma patientsInvestigated the association between disk hemorrhages and glaucomatous damageToday (widely accepted) : disk hemorrhages = 1 of most important risk factor developing and progression of glaucoma and ocular hypertensionPrevalence and Incindence
Disk hemorrhage in normal population = 0 1,4%Disk hemorrhage in glaucoma or ocular hypertension patients = 2 33,4%Therefore more commonly occurs in glaucoma or ocular hypertensive eyesCan also be found in case of subclinical structural loss of retinal nerve fiber layer (RNFL) thicknessNormal patients need to be evaluated with cautionOpen Angle Glaucoma: Normal tension vs. High tension
Based on data resulted from methodological difference disk hemorrhage more prevalent in open glaucoma with normal tension (NTG)
The prevalence in NTG = 20.5% 33.3%,
In HTG = 8.3% 17.6%
Therefore, 2 to 5 times more frequent in NTG than in HTG
Suh and Park NTG (33.3% prevalence) and HTG patients (17.6% prevalences)
Furthermore, overall probability reached 45.5% in NTG and 23.2% in HTG
Suggesting, found in up to half of eyes with NTG and about a quarter of those with HTG
Angle-closure Glaucoma
Disk hemorrhage prevalence of primary angle-closure glaucoma ranged between 0.5% and 5.7%Lan et al disk hemorrhage in primary angle-closure glaucoma to be associated with progression of glaucomatous optic neuropathy & visual field defectsDifferential Diagnosis
Can also occured in:
Posterior vitreous detachment
Optic disk drusen
Vascular occlusive disease of the retina
Non-glaucomatous optic neuropathies
Also correlated with:
Diabetes and hypertension
Leukemia
SLE
Can be distinguished from ocular or systemic condition by = absence of any sign of papillitis or presence of vitreoretinal abnormalities, or non-glaucomatous optic neuropathy
Appearance and Location
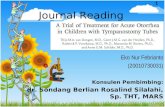
Typically splinter-shaped (thin and oriented perpendicular to the disk margin)If extravasation is abundant flame- or fan-shapedThese are result of the orientation of the RNFL axonsOptic disk hemorrhages located on the optic disk margin (laminar or prelaminar tissue), cross the optic disk margin, or on the peripapillary retinaIf hemorrhages is at the lamina cribosa level close relation to the location of the lamina cribosa pores tissue remodelling change in pore morphology59-year-old male, open-angle glaucoma with normal tension patient had two episodes (A, C ) of disk hemorrhage in the inferotemporal area of the lamina cribrosa within a 1-year period. After absorption of the disk hemorrhage, a clear laminar pore was observed in the area where the hemorrhage occurred (B, D). Visual eld progression in the corresponding region of disk hemorrhages was noted in the deviation plot (E, F)
A 54-year-old female, open-angle glaucoma with normal tension patient had two episodes (B, C ) of disk hemorrhage in the temporal (B) and inferior (C ) areas of the lamina cribrosa within a 20-month period. Compared with the pre-hemorrhage photograph (A) of the areas of the proximal portions of the hemorrhages, the lamina cribrosa pores became prominent (D, black circles) after absorption of the hemorrhages, indicating that there must have been a tissue remodeling process around the pores. Visual eld progression in the corresponding region of disk hemorrhages was noted in the pattern deviation plot (E, F)
A 60-year-old male, open-angle glaucoma with normal tension patient showed a change in the lamina cribrosa pores (inside of the circle) near the area of the disk hemorrhage. The pores became more prominent (A, B)
A peripapillary-type disk hemorrhage was found on the border of the inferotemporal wedge-shaped retinal nerve ber layer (RNFL) defect in a 58-year-old female open-angle glaucoma with normal tension (NTG) patient (A). Another 60-year-old female NTG patient with superotemporal and inferotemporal RNFL defects showed a peripapillary-type disk hemorrhage on the border of the inferotemporal RNFL defect (B).
Timing, Duration and Recurrence
Frequently increase from ealry stage of glaucoma to the moderate stage decrease as the disease progress to advanced stageDisk hemorrhage = transient, Persisting weeks several months (most disappearing within 2 months of onset)Detection Methods
Often missed therefore, careful examination is necessary
Methods = ophthalmoscopy and stereophotography
Studies better detected using stereoscopic disk photography than by clinical examination
In Ocular Hypertension Treatment Study (OHTS) only seen on disk photograph
Several studies (including the Early Manifest Glaucoma Trial (EMGT)) clinical and photographic detection meets good agreement (range 55 61%)
This suggest can be found in both methods (for prognostic importance, both detection should be used)
Pathogenesis and Clinical Implications of Optic Disk Hemorrhage in Glaucoma
Pathogenesis
Associated pressure around the optic nerve headDisk hemorrhage does not develop in all patients with open angle glaucoma or ocular hypertensionThe pathogenesis remains unclearThere are four biomechanical forces influencing the lamina cribrosa and surrounding tissue:intraocular pressure (IOP),Cerebrospinal fluid pressure,arterial pressure, andvenous pressureThe recent EMGT study also showed that the occurrence of optic disk hemorrhage did not change after administration of IOP lowering medication
Morphologic Associations
zone perpapillary atrophy (PPA)A number of studies suggest that disk hemorrhage tends to occur in areas of the eye having the greatest zone PPA width
Morphologic Associations
RNFL and neuroretinal rim areaDisk hemorrhage has been strongly associated with:
Rim notching
Small neuroretinal rim, and
RNFL defects
RNFL defect border is an active site of damage and that its enlargement causes disruption of the capillary network, and finally, optic disk hemorrhage
Morphologic Associations
Other morphologic parametersJonas et al found that morphologic factors
not associated with disk hemorrhage:
disk size and shape,
zone PPA,
retinal vessel diameter, and
cup depth
Associated with disk hemorrhage:
Neuroretinal rim area and
zone PPA
Morphologic Associations
Other morphologic parametersFor patients with unilateral disk hemorrhage, the probability that the contralateral eye will develop optic disk hemorrhage is as high as that of the affected eye
Glaucoma Progression and Optic Disk Hemorrhage
SignificanceDisk hemorrhage is of clinical importance because its presence is an important prognostic factor for glaucoma progression
Glaucoma progression is associated with optic disk hemorrhage in both HTG patients and those suspected of it, as well as in NTG patients
Glaucoma Progression and Optic Disk Hemorrhage
Several points concerning the correlation between optic disk hemorrhage and glaucoma progression:The time relationship between glaucoma progression and disk hemorrhage
The method of detecting glaucoma progression and relationship between recurrent optic disk hemorrhage and glaucoma progression.
Glaucoma Progression and Optic Disk Hemorrhage
Glaucoma progression detected before and after optic disk hemorrhageVarious studies have addressed glaucoma progression after disk hemorrhage
Data from ocular hypertension patients with a median follow-up of more than 8 years indicate that disk hemorrhage represents an independent risk factor for HTG development, even after adjusting for other factors including corneal thickness, age, and cup:disk ratio.
Glaucoma progression detected before and after optic disk
hemorrhage
Disk hemorrhage should therefore be considered one of the risk factors for progression of ocular hypertension and warrant frequent monitoring and more aggressive treatment.
Not all patients with optic disk hemorrhage, however, show glaucoma progressionGlaucoma progression detected before and after optic disk
hemorrhage
Glaucoma progression detected before and after optic disk
hemorrhage
Glaucoma progression detected before and after optic disk
hemorrhage
Glaucoma progression detected before and after optic disk
hemorrhage
Glaucoma progression detected before and after optic disk
hemorrhage
Rapid, localized disease progression predisposes to optic disk hemorrhage, and disease progression accelerates after disk hemorrhage
So disk hemorrhage can be a marker of rapid glaucoma progression
Glaucoma progression detected before and after optic disk
hemorrhage
It remains unclear whether optic disk hemorrhage has a causative role in disease progression.
The extravasated blood is known to be neurotoxic
Recurrent Optic Disk Hemorrhage
Several studies had evaluated the relationship between glaucoma and optic disk hemorrhage:Eyes with recurrent optic disk hemorrhage had a more than two-fold greater chance of progression than single-disk hemorrhage eyes (Kim & Park et al)
Open-angle glaucoma eyes with recurrent optic disk hemorrhage had a higher cumulative probability of progression of RNFL loss than eyes with single-disk hemorrhage (Suh, et al)
Recurrent Optic Disk Hemorrhage
Conclusion:Eyes with reccurent disk hemorrhage had more rapid and extensive progression of glaucoma than those with single-disk hemorrhage
Effect of Treatment
Conclusions
Optic disk hemorrhage is more commonly detected in NTG than in HTG, but hemorrhage can also be detected in almost a quarter of HTG patients by more frequent and careful examination.The development of disk hemorrhage may be associated with the biomechanical circumstances of the lamina cribrosa and surrounding tissues, including the IOP ecerebrospinal pressure gradient, arterial pressure, and venous pressure.