Interesting case orthokorat clavical fracture
38
Interesting case นพท. วิชญุตร์ ภูมิวัฒน์ ชั้นปีที่ 6 วิทยาลัยแพทยศาสตร์พระมงกุฎเกล้า
Transcript of Interesting case orthokorat clavical fracture
Interesting case
นพท. วิชญตุร์ ภมิูวฒัน์ ชัน้ปีที่ 6
วิทยาลยัแพทยศาสตร์พระมงกฎุเกล้า
History
• Case ผู้ ป่วยชายไทย อาย ุ27 ปี U/D old pulmonary TB
• CC : MC ล้ม 10 ชัว่โมง PTA
• Primary survey– A : patent airway, no C spine tender
– B : equal breath sound, no tachypnea
– C : vital sign stable, no external active bleed
– D : ผู้ ป่วยเป็นใบ้และหหูนวกแตก่ าเนิด E4V5M6 pupil 3 mm RTLBE
– E : no life-threatening wound
History
• Secondary survey– A : pyrazinamide
– M : ไมมี่ประวตัิยาเดิม ตอนนีไ้มมี่ยาท่ีใช้ประจ า
– P : old pulmonary TB รับยา รพ.โชคชยั on ยา 12/57 – 05/58
– L : NPO time 08:30 น. (2 hr)
– E : 10 hr PTA ขบัรถจกัรยานยนต์ ขบัรถล้มเอง ไมส่ลบ ไมส่วมหมวกนิรภยั ตวัด้านขวาและขาขวาลงพืน้ มีอาการปวดไหลข่วา ยกแขนไมข่ึน้เน่ืองจากปวด มีแผลถลอกตามร่างกาย ไป รพช. On arm sling ก่อนสง่ตอ่มาท่ีรพ.มหาราช
Physical examination
• Vital sign : BT 35.9 BP 127/63 PR 87 RR 20• GA : an adult Thai man, good consciousness, deaf, • HEENT : not pale conjunctivae, anicteric sclerea• Heart : normal S1S2, no murmur• Lung : equal breath sound, no adventitious sound• Abd : soft, not tender, no palpable mass• Ext : affected part• Neuro : motor grade V all, sensory intact

Physical examination
• Affected part– Tender at right proximal to middle clavicle area
– Stepping at right proximal to middle clavicle area
– Skin dimple seen at right proximal to middle clavicle area
– limit ROM of right shoulder due to pain
– Intact neurovascular

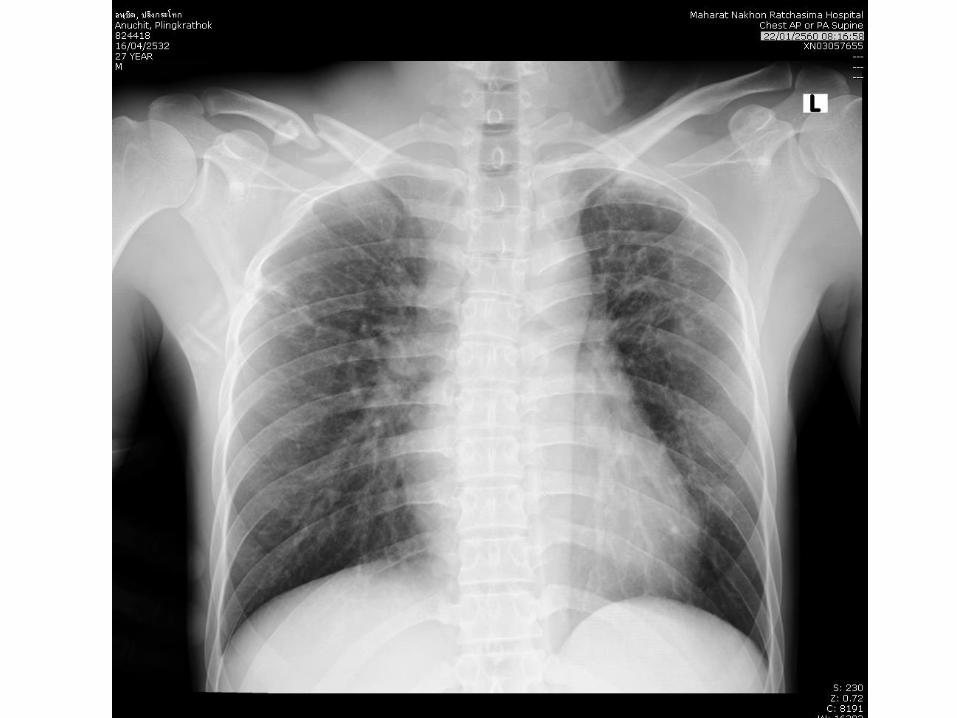
Diagnosis
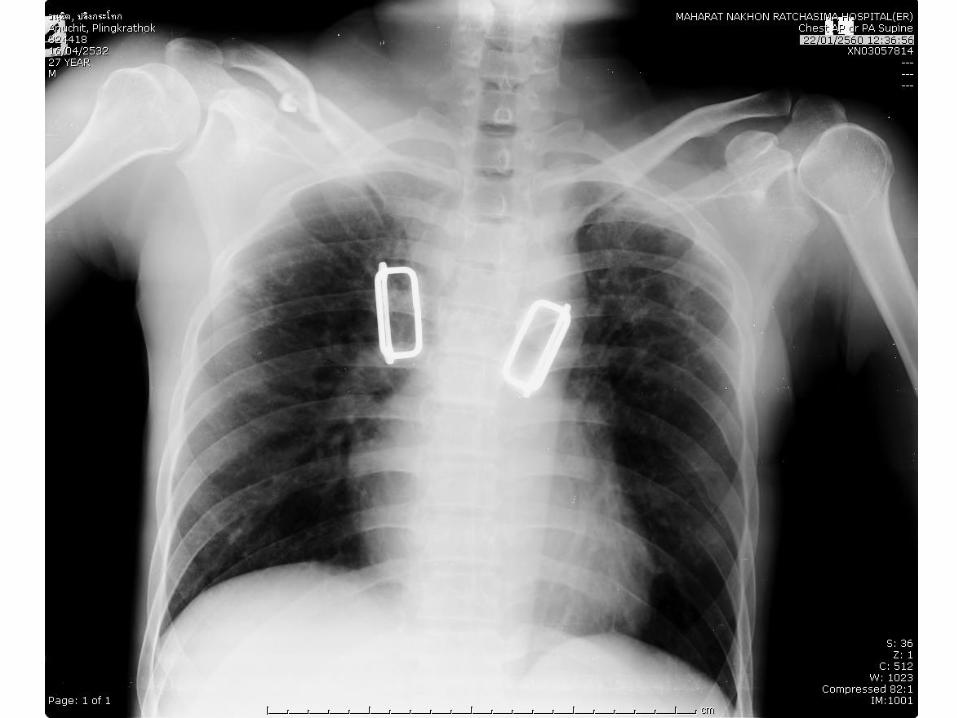
• Closed fracture at middle third of right clavicle

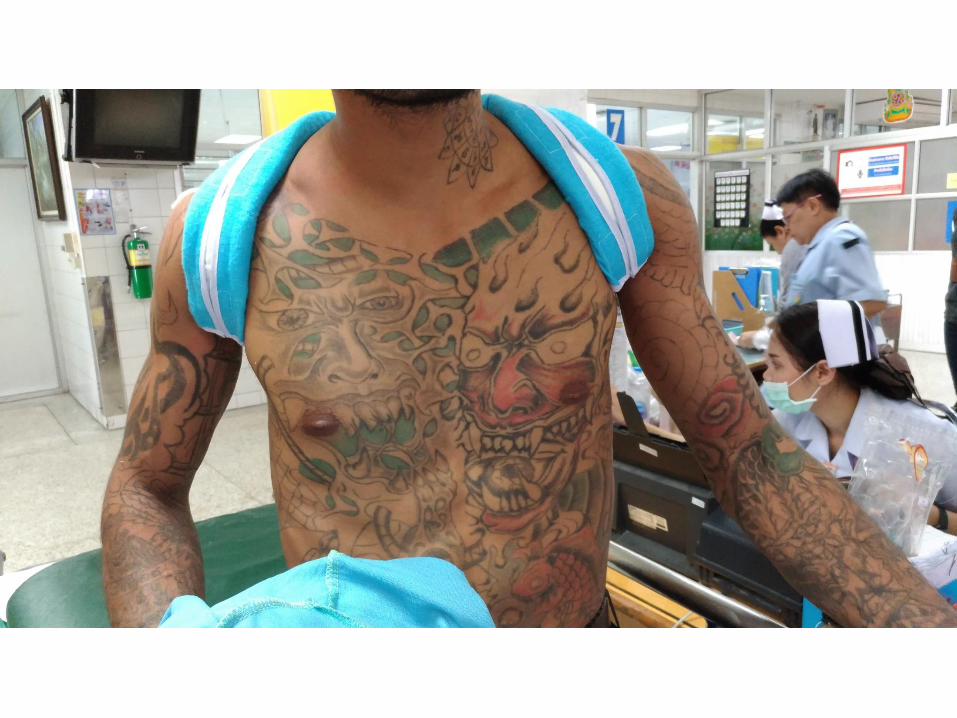
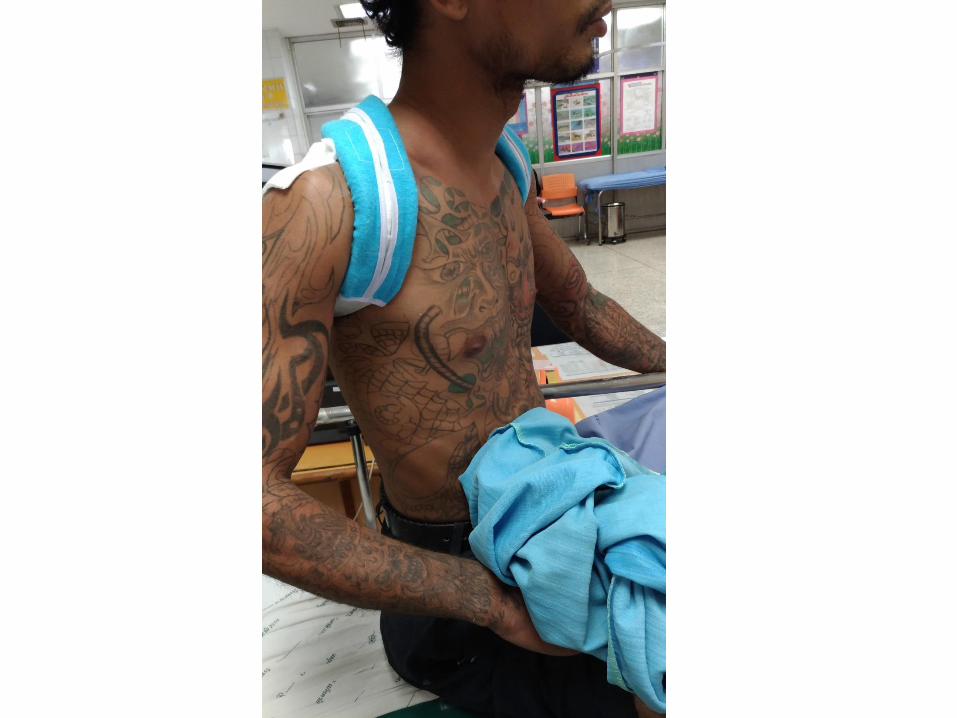
Treatment
• Figure of eight splint
• D/C
• F/U 30/1/60 (1 week)– Advice ใส ่Figure of eight ตลอดเวลาจนถงึวนันดั
– HM• Paracetamol 500 mg oral prn q 6 hr

Mini reviewClavicle fracture
Epidemiology
• 2.6% of all fractures
• 69% in middle third
• 28% in distal third
• 2.8 – 9.3% in proximal third
• Peak incidence in children and young adults
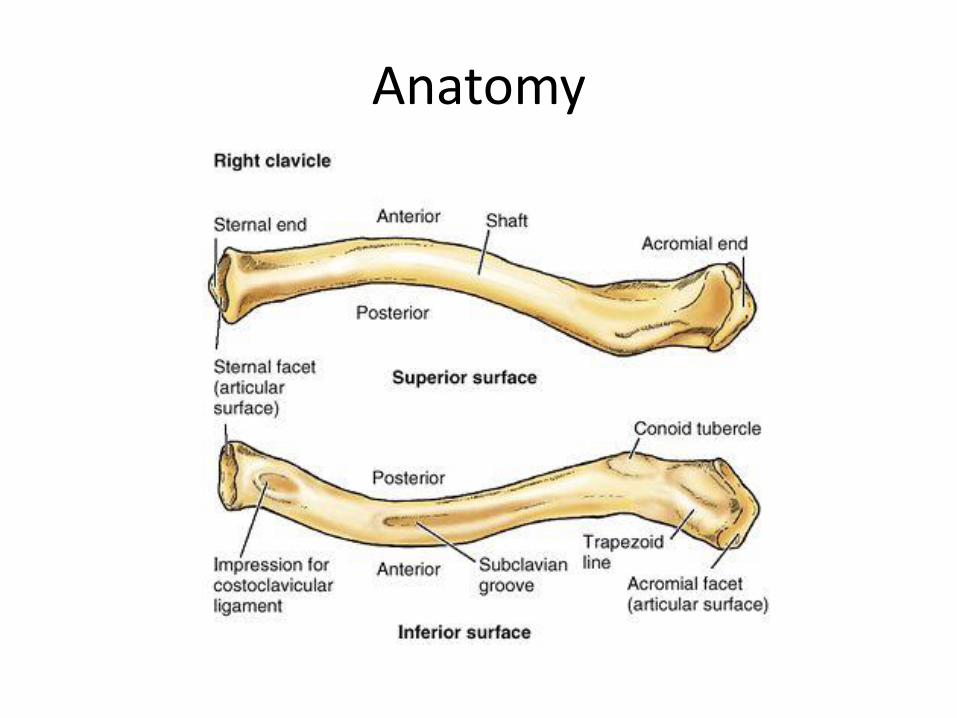
Anatomy
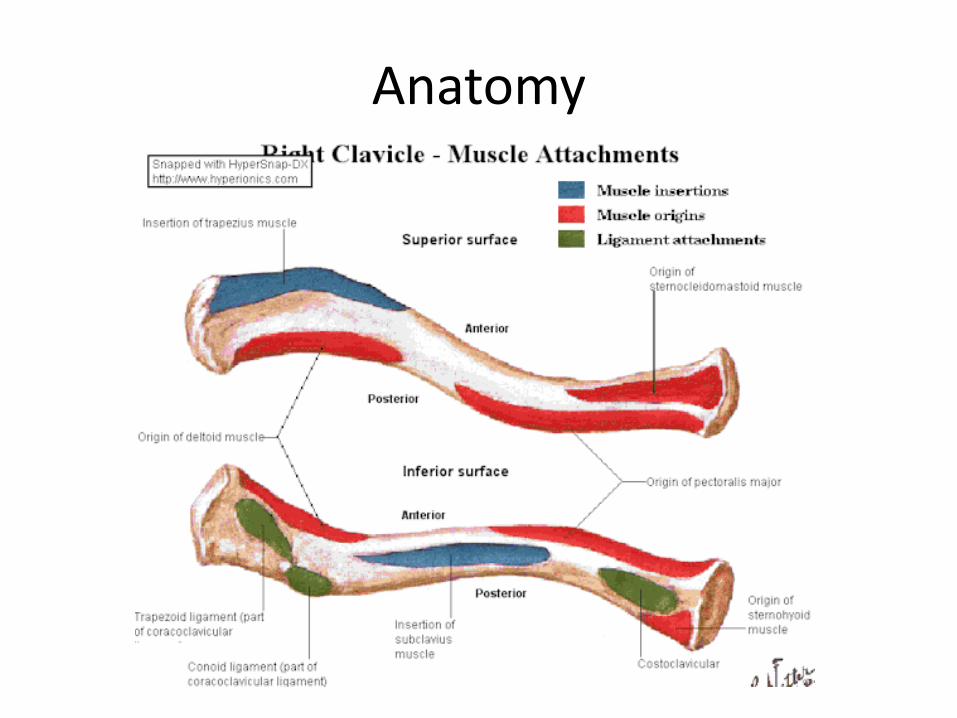
Anatomy
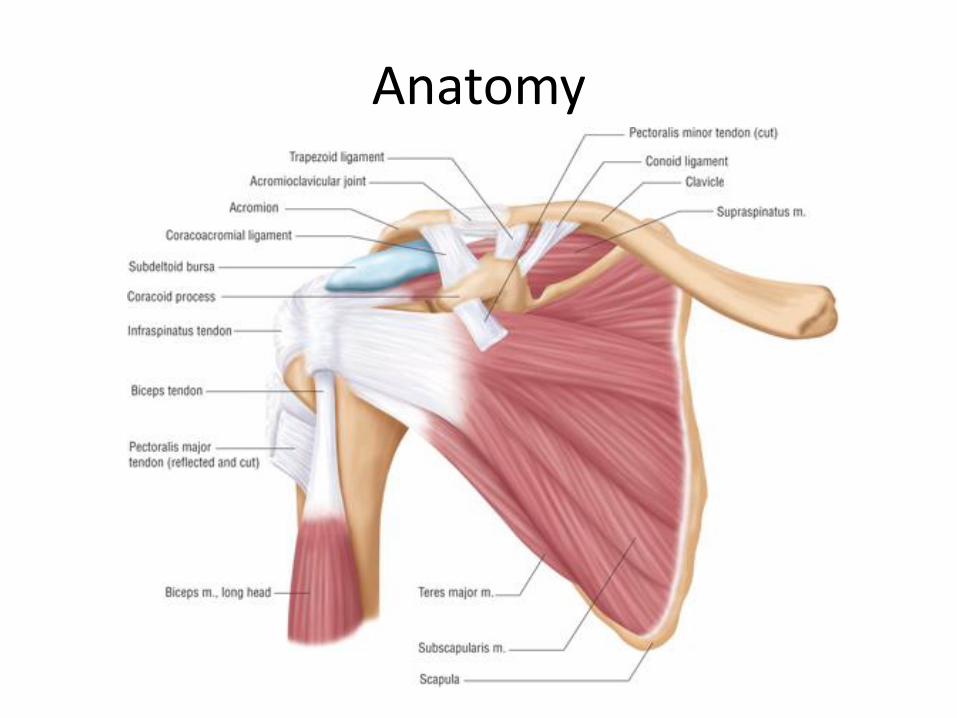
Anatomy
Mechanism of injury
• Fall onto shoulder 87%
– Traffic accident
– sport
• Direct injury to clavicle
– Falling object
– assault
Classification
• Allman classification– 3 groups based on location
• Group I : fractures of the middle third most common
• Group II : fractures of the distal third Neer classification• Group III : fractures of the proximal third

Allman classification
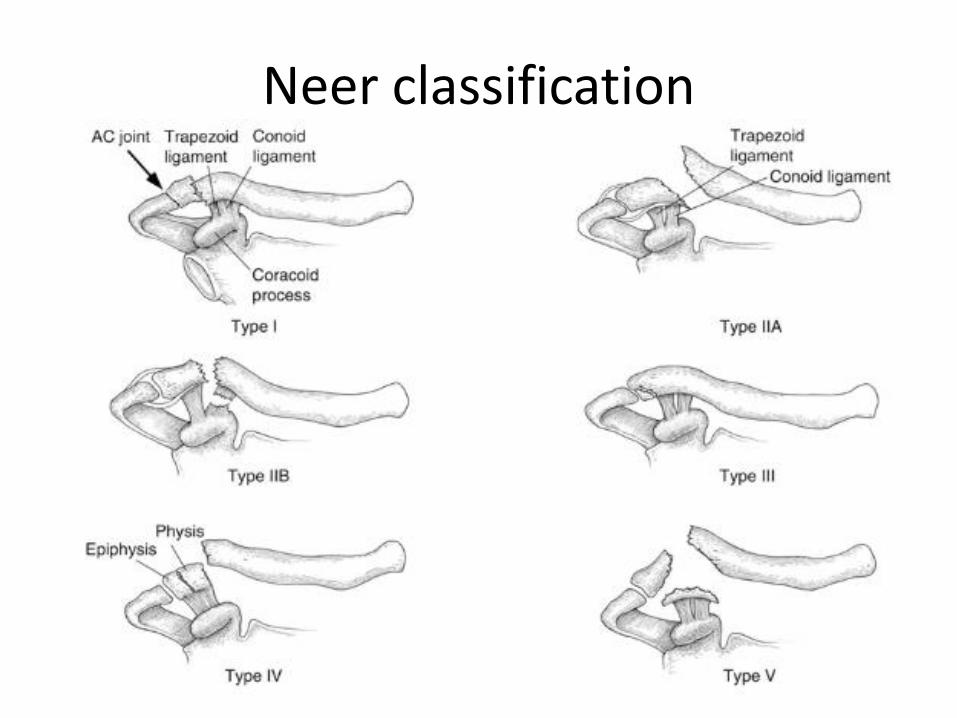
Neer classification
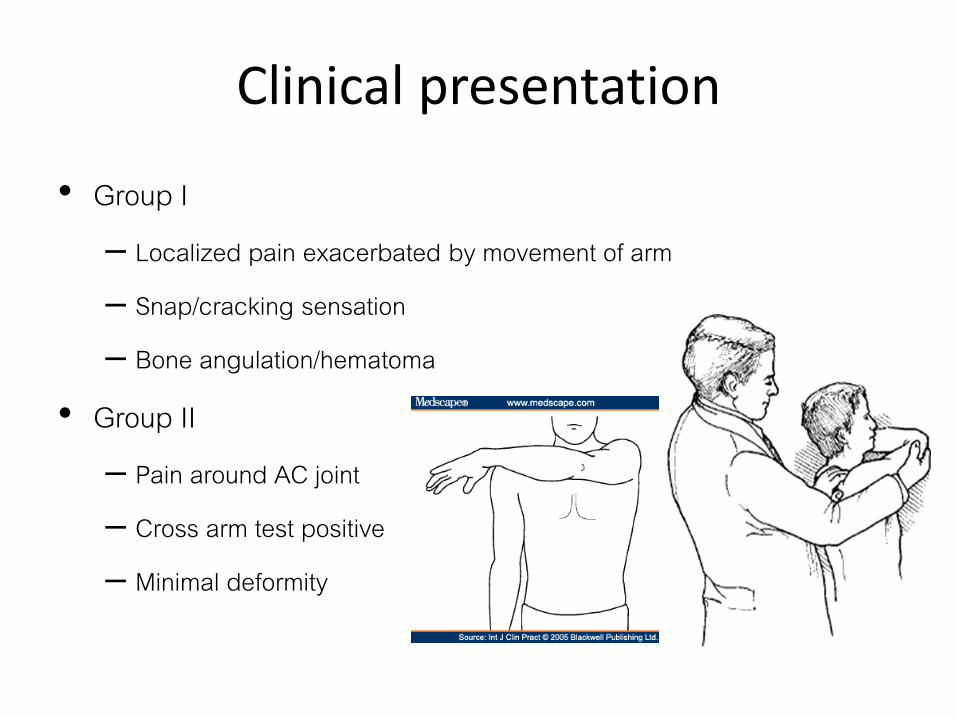
Clinical presentation
• Group I– Localized pain exacerbated by movement of arm
– Snap/cracking sensation
– Bone angulation/hematoma
• Group II– Pain around AC joint
– Cross arm test positive
– Minimal deformity
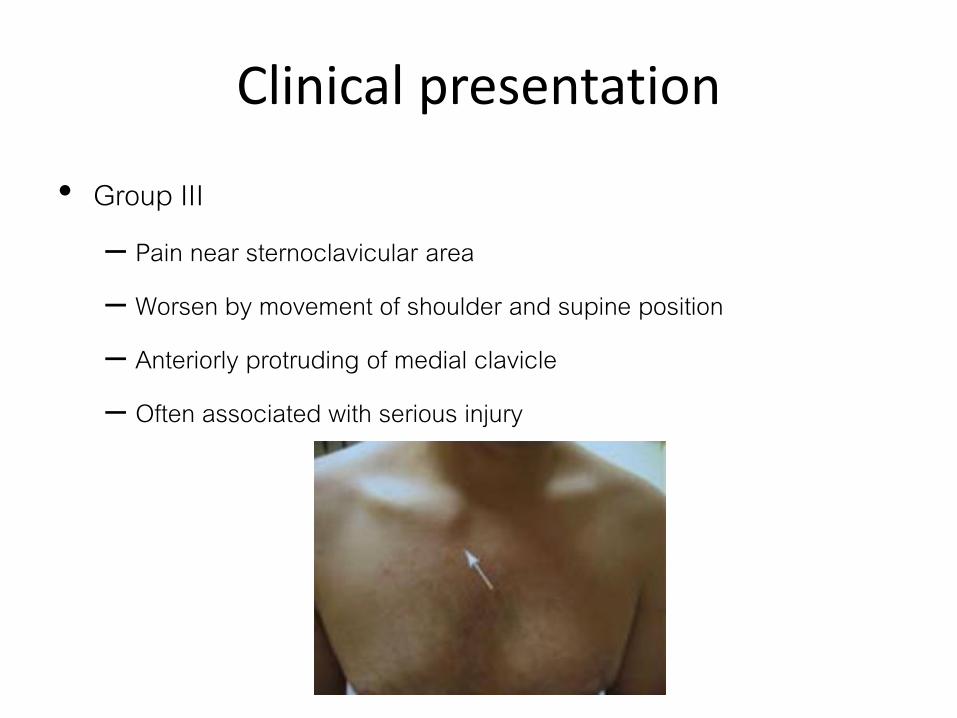
Clinical presentation
• Group III– Pain near sternoclavicular area
– Worsen by movement of shoulder and supine position
– Anteriorly protruding of medial clavicle
– Often associated with serious injury

Investigation
• Imaging– Radiographs
• AP view of bilateral shoulders – to measure clavicular shortening
• 45° cephalic tilt superior/inferior displacement• 45° caudal tilt AP displacement
– CT • may help evaluate displacement, shortening, comminution, articular
extension, and nonunion• useful for medial physeal fractures and sternoclavicular injuries

Investigation
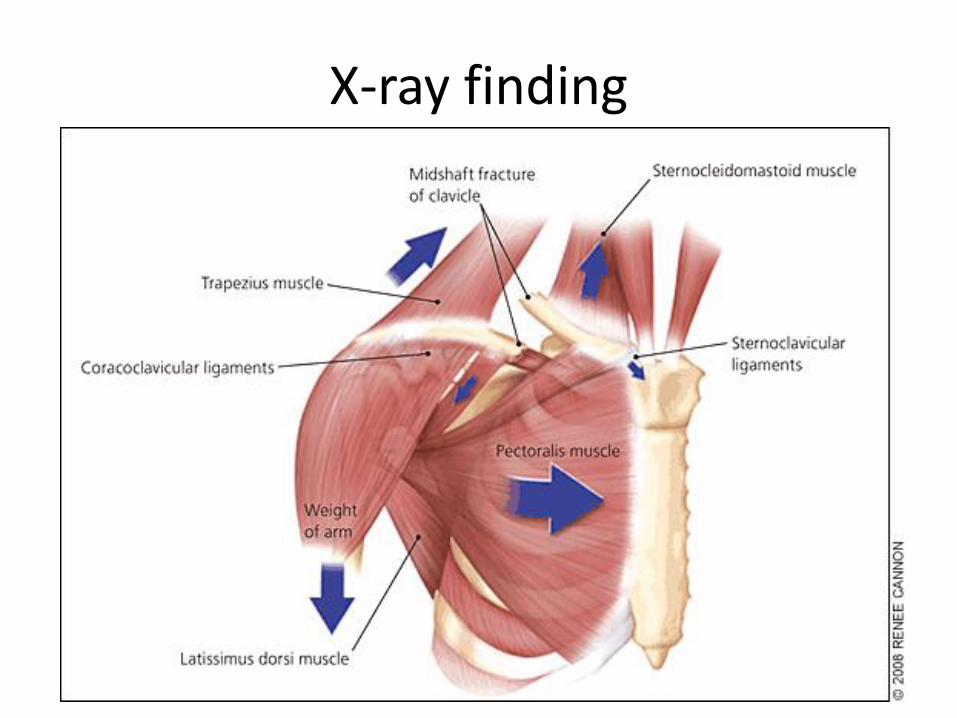
X-ray finding
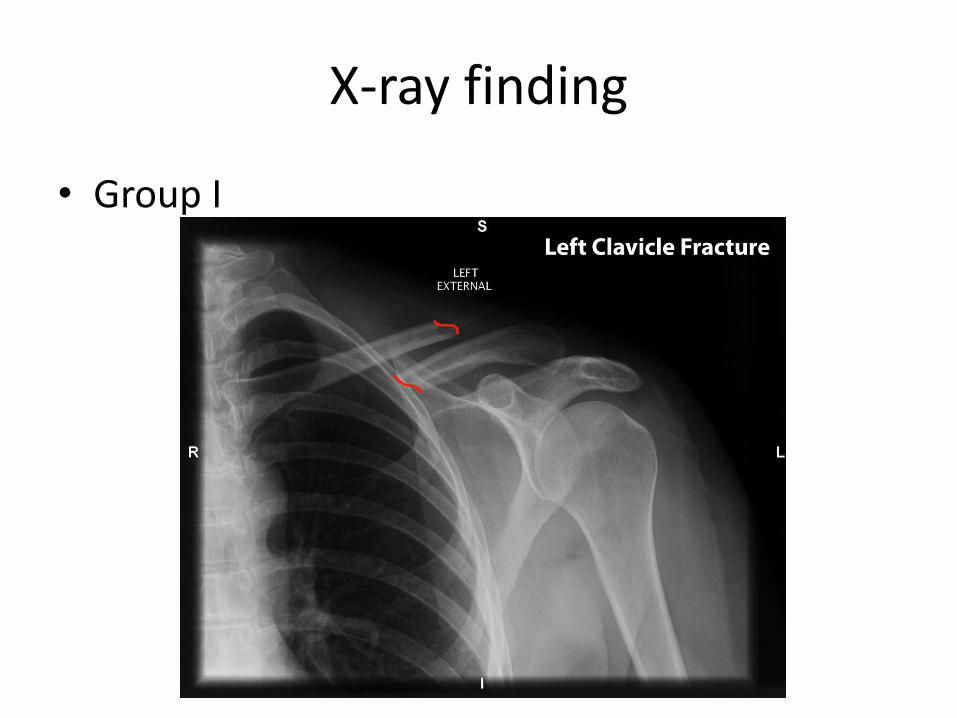
X-ray finding
• Group I

X-ray finding
• Group II

X-ray finding
• Group III
Complication
• Malunion most common• Nonunion (if fail to heal after 4 – 6 mo)
• Pneumothorax
• Subclavian vessels/carotid A. compression or laceration
• Brachial plexus injury
• Post-traumatic arthritis
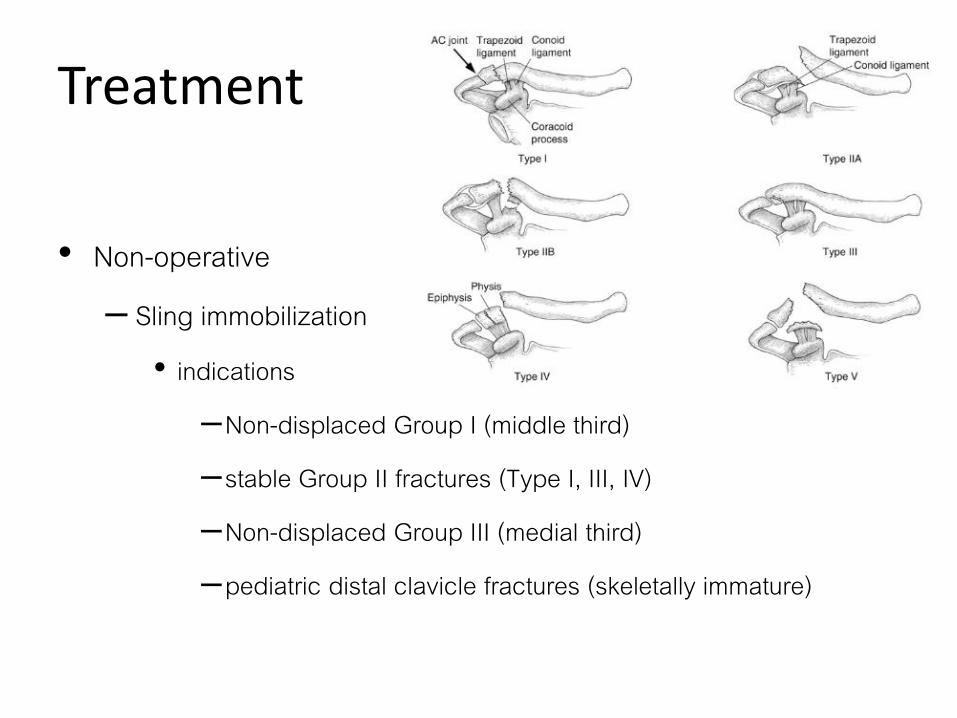
Treatment
• Non-operative– Sling immobilization
• indications
–Non-displaced Group I (middle third)
–stable Group II fractures (Type I, III, IV)
–Non-displaced Group III (medial third)
–pediatric distal clavicle fractures (skeletally immature)

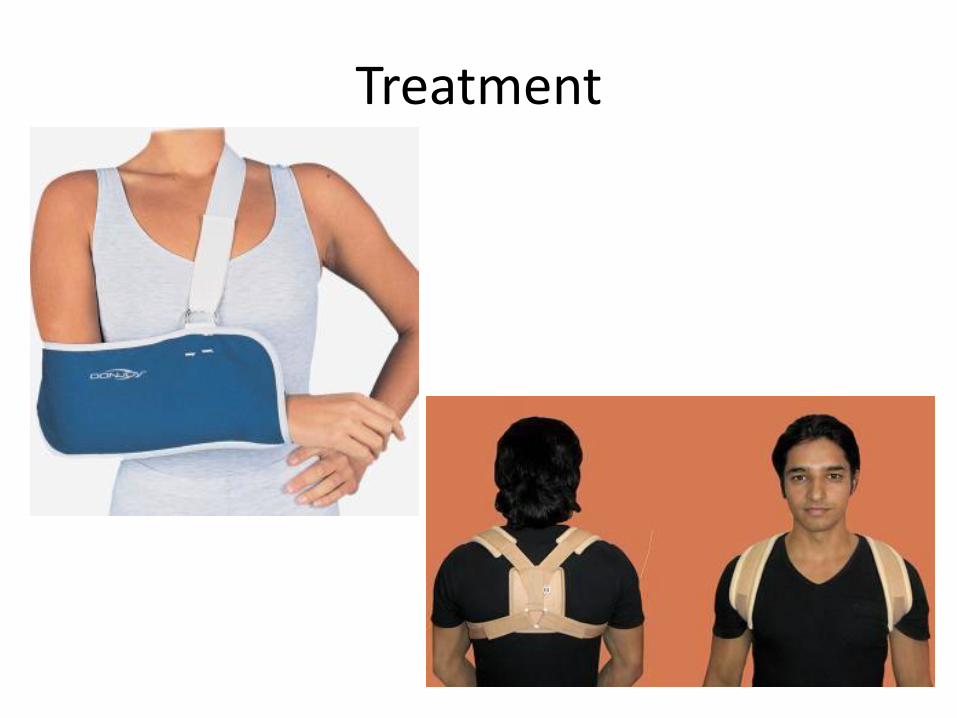
Treatment
• Sling immobilization– Arm sling or figure-of-eight splint
• have no differences in healing times, healing rates, and alignment at final follow-up
– Adjust q 7 – 10 days
– After 3-4 weeks begin gentle range of motion exercises
Treatment

Treatment
• Operative (should refer)– open reduction internal fixation indications
• absolute – unstable Group II fractures (Type IIA, Type IIB, Type V) – open fracture– displaced fracture with skin tenting – subclavian artery or vein injury– floating shoulder (clavicle and scapula neck fracture)– symptomatic nonunion– posteriorly displaced Group III fracture– displaced Group I (middle third) with >2cm shortening
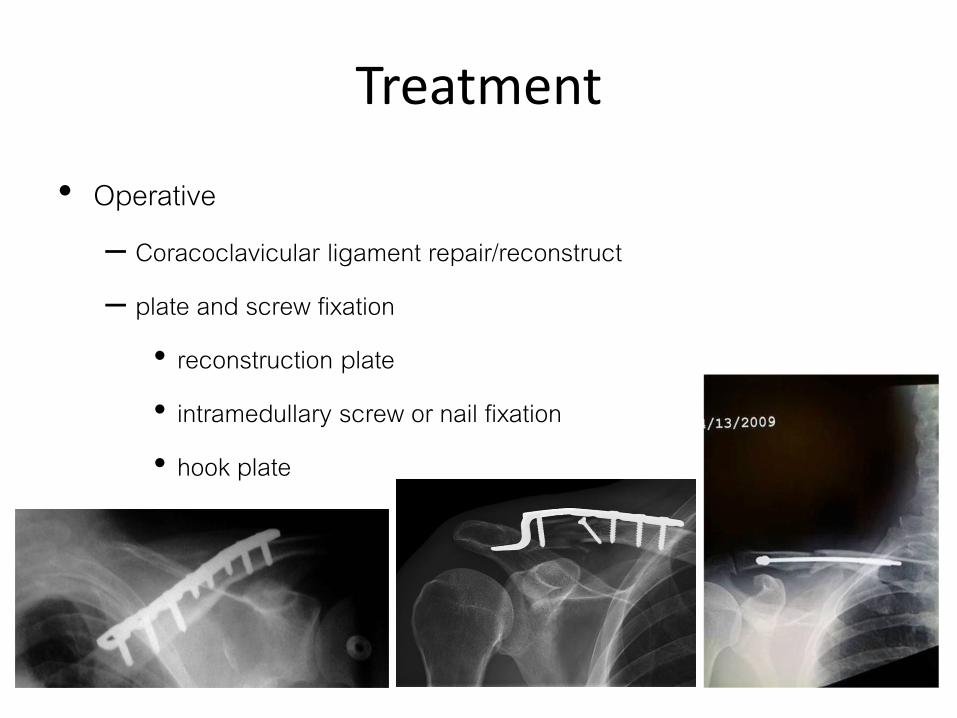
Treatment
• Operative– Coracoclavicular ligament repair/reconstruct
– plate and screw fixation
• reconstruction plate
• intramedullary screw or nail fixation
• hook plate

Surgical complication
• hardware prominence• superior plates increased irritation• neurovascular injury (3%)
– superior plates associated with increased risk of subclavian vessels penetration– subclavian thrombosis
• nonunion (1-5%) • infection (~4.8%) • mechanical failure (~1.4%)• pneumothorax• adhesive capsulitis
Return to work and sport
• In general– 6 – 8 weeks
• Distal clavicle fracture return to pre-injury level sooner– 4 – 6 weeks
• Should avoid contact sport and strenuous activity until 4 weeks after clinical healing– Required 8 – 12 weeks before returning to contact sport
– Should remove hardware before playing