INTERESTING CASE - medkorat.in.th new.pdf•Present illness : 3 days pta...
53
INTERESTING CASE ENDOCRINE DEPARTMENT
Transcript of INTERESTING CASE - medkorat.in.th new.pdf•Present illness : 3 days pta...

INTERESTING CASE
ENDOCRINE DEPARTMENT
CASE ผ ปวยชายอาย 18 ป อาชพ สามเณร ภมล าเนา อ าเภอ ล าปลายมาศ จงหวด บรรมย
Chief complaint : เกรงกระตกทงตว 4 hr pta

• Present illness : 3 days pta ไมฉนอาหารจากเดมทฉน 2 มอ คอมอเชาและมอกลางวน เนองจากอยากลดความอวน ระหวางนดมแตน าอดลม น าสมขวด ชาเขยวรสหวานบรรจขวด วนละประมาณ 4-5 ขวด หวน าบอย สงเกตวาปสสาวะบอยกวาปกต สเหลองใส ไมมปสสาวะขด มลกมาปสสาวะตอนกลางคน น าหนกลง 3 กโลกรมในชวง 1 เดอน
• 2 days pta ยงคงไมรบประทานอาหาร ดมแตน า เรมมอาการไข ครนเนอครนตวตลอดทงวน ไมมหนาวสน มอาการปวดศรษะรวมดวย เปนๆหายๆ ปวดตอๆทขมบทงสองขาง ไมมราวไปไหน ไมสมพนธกบไอจามเบง ไมมเหนภาพซอนหรอตามว ไมมแขนขาออนแรงครงซก มคลนไสอาเจยน หลายครง ออกมาเปนน า ไมมปวดทอง ไมมถายเหลว ไมมปสสาวะขด ระหวางนปฏบตกจวตรประจ าวนไดตามปกต ไมไดไปรกษาทไหน
• 4 Hr pta มอาการพดจาสบสน พดไมรเรอง หลงจากนนเพอนสามเณรเหนนอนซม ปลกไมตน และมอาการตวเกรงกระตก นาน 2 นาท ไมมตาเหลอกคาง ไมมปสสาวะหรออจจาระราด อาการเกรงกระตกหยดไดเอง หลงมอาการไมตน จงไดน าคนไขสง โรงพยาบาล

Personal history
• ไมมโรคประจ าตวใดมากอน ไมดมเหลาสบบหร
• ไมไดใชยาใดประจ า
• ไมดมเหลาหรอสบบหร
• ไมเคยไดรบอบตเหตทศรษะ
• ไมเคยผาตด
• ปกตฉนอาหาร สองมอตอวน มอเชาและมอกลางวนเปนขาว 2-3 ทพพ และกบขาวทไดบณฑบาต ระหวางวนดมน าอดลม ตอนเยนดมน าอดลม
Family history
• บดามารดาไมมโรคประจ าตว
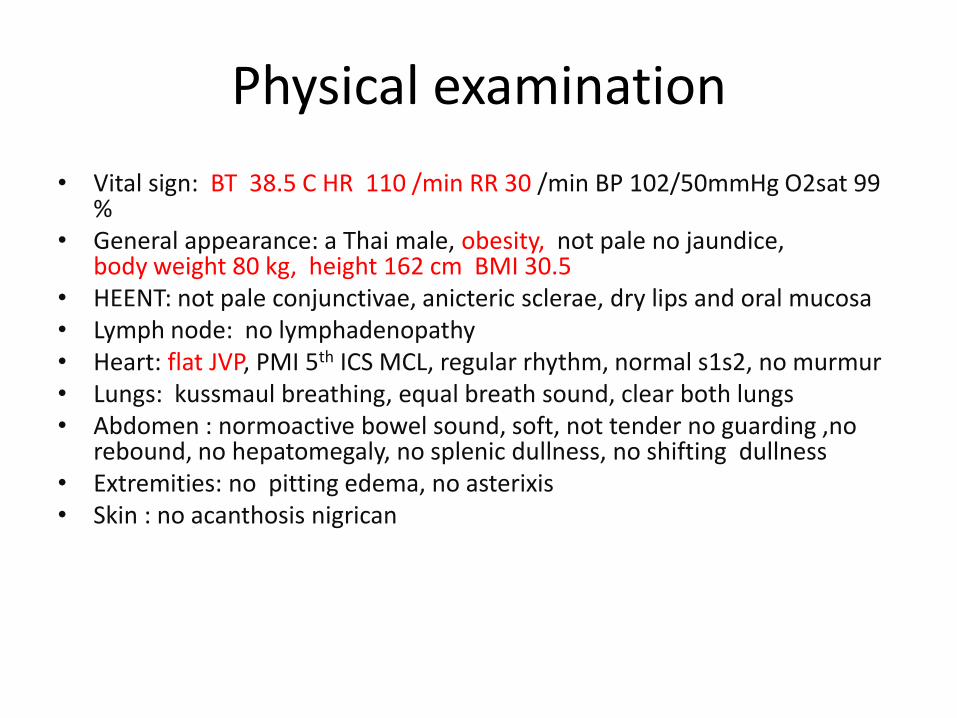
Physical examination
• Vital sign: BT 38.5 C HR 110 /min RR 30 /min BP 102/50mmHg O2sat 99 %
• General appearance: a Thai male, obesity, not pale no jaundice, body weight 80 kg, height 162 cm BMI 30.5
• HEENT: not pale conjunctivae, anicteric sclerae, dry lips and oral mucosa• Lymph node: no lymphadenopathy• Heart: flat JVP, PMI 5th ICS MCL, regular rhythm, normal s1s2, no murmur• Lungs: kussmaul breathing, equal breath sound, clear both lungs• Abdomen : normoactive bowel sound, soft, not tender no guarding ,no
rebound, no hepatomegaly, no splenic dullness, no shifting dullness• Extremities: no pitting edema, no asterixis• Skin : no acanthosis nigrican

Neurological examination
• Mental status : drowsiness
• No Stiffness of neck
• Cranial nerves
– Cranial nerve II: Pupil 2 mm ,react to light both eyes
– Cranial nerve III, IV, VI : doll eys positive (horizontal and vertical)
– Cranial nerve V: cannot evaluate
– Cranial nerve VII: no facial palsy
– Cranial nerve VIII: cannot evaluate
– Cranial nerve IX,X: gag reflex present
– Cranial nerve Xll: cannot evaluate
Neurological examination
• Moter power : at least grade IV all extremity
• Deep tendon reflex: 2+ all
• Clonus: negative bilateral
• Babinski: absent bilateral
Problem list

Lab investigation
CBC
serum ketone
Blood chemistry
Liver function test
UA
Chest xray
Arterial blood gas
Hemoculture
FBS
Lipid profile
Blood sugar

Blood sugar
• Sugar : 1370mg/dL

Arterial blood gas
Bar Pres : 760.0mmHg
pH : 7.000. N : 7.35 - 7.45
PCO2 : 11.0mmHg N : 32 - 46
PO2 : 118mmHg N : 74 - 108
HCO3 : mmol/L N : 21 - 29
HCO3 <3.0 T-CO2 : mmol/L N : 19 - 31
BEb : mmol/L N : 0.95 - 1.25
BEef : mmol/L N : -2 - +2
SBC : mmol/L N : 18 - 22
sO2 CT : % N : 92 - 96

Serum ketone and osmolarity
Ketone-S : 142.2mg/dL N : 0.2 - 2.8
Osmolarity : 419mOSMOL/Kg N:289-308
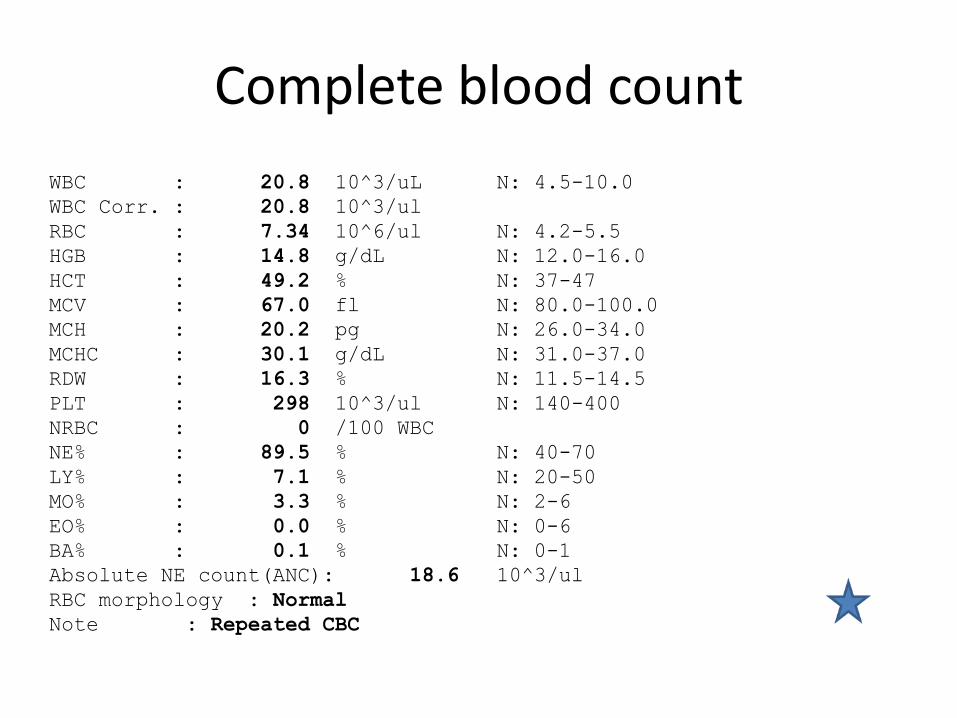
Complete blood count
WBC : 20.8 10^3/uL N: 4.5-10.0
WBC Corr. : 20.8 10^3/ul
RBC : 7.34 10^6/ul N: 4.2-5.5
HGB : 14.8 g/dL N: 12.0-16.0
HCT : 49.2 % N: 37-47
MCV : 67.0 fl N: 80.0-100.0
MCH : 20.2 pg N: 26.0-34.0
MCHC : 30.1 g/dL N: 31.0-37.0
RDW : 16.3 % N: 11.5-14.5
PLT : 298 10^3/ul N: 140-400
NRBC : 0 /100 WBC
NE% : 89.5 % N: 40-70
LY% : 7.1 % N: 20-50
MO% : 3.3 % N: 2-6
EO% : 0.0 % N: 0-6
BA% : 0.1 % N: 0-1
Absolute NE count(ANC): 18.6 10^3/ul
RBC morphology : Normal
Note : Repeated CBC
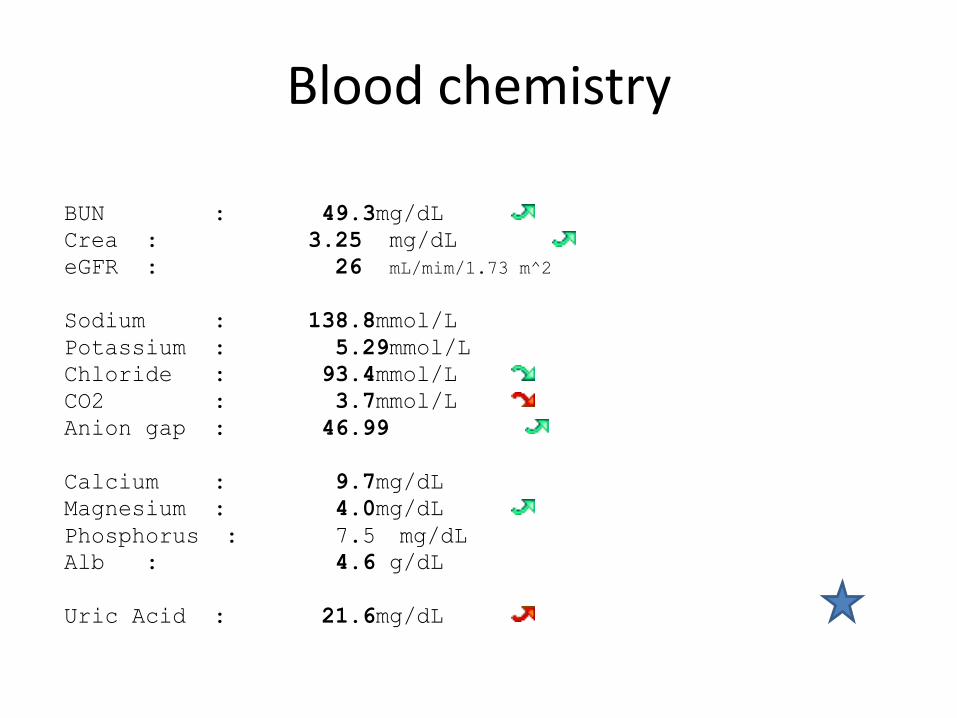
Blood chemistry
BUN : 49.3mg/dL
Crea : 3.25 mg/dL
eGFR : 26 mL/mim/1.73 m^2
Sodium : 138.8mmol/L
Potassium : 5.29mmol/L
Chloride : 93.4mmol/L
CO2 : 3.7mmol/L
Anion gap : 46.99
Calcium : 9.7mg/dL
Magnesium : 4.0mg/dL
Phosphorus : 7.5 mg/dL
Alb : 4.6 g/dL
Uric Acid : 21.6mg/dL

Liver function test
• Cholest : 356mg/dL
• D-BILI : 0.1mg/dL
• T-BILI : 0.6mg/dL
• SGOT (AST) : 23U/L
• SGPT (ALT) : 23U/L
• ALP : 40U/L
• TP : 8.3g/dL
• Alb : 4.6g/dL
• Globu : 3.7g/dL

Urine analysis
Color : Yellow
Appearance : Clear
Specific gravity : 1.027
pH : 5.5
Protein (Albumin) : 2+ (30-100 mg/dl)
Sugar (Glucose) : 4+ (1000-2000mg/dl)
Blood(RBC,Hb),Myoglobin : 3+ (50-250 RBC/uL
Ketone(Acetoacetic acid) : 2+ (10-50 mg/dl)
Bilirubin : Negative
Urobilinogen : Negative Leukocyte(WBC,histiocytes) : Negative Nitrite : Negative
Red blood cell(RBC) : 0-1 cell/HPF
White blood cell(WBC) : 10-20 cell/HPF Squamous epithelial cell : Negative

Cholest : 222mg/dL N : 150 - 200
Trigly : 211mg/dL N : <150
HDL-Cholest: 34mg/dL N : 32-68
LDL-Cholest : 146mg/dL N : < 150
%HbA1C_R : 12.8%

Chest x ray

Hemoculture
• Hemoculture 1: coagulase negative staphylococci
– susceptible : cloxacilllin, cefazolin
• Hemoculture 2: non fermentative bacteria
– Susceptible: amikacin, ceftazidime, ciprofloxacin

Hyperglycemic Crises in Adult Patients With Diabetes
DKA and HHS
• Two-thirds of DKA have type 1 diabetes
• Half of all deaths younger than 24 years
• In adults with DKA, the overall mortality is 1% and 5% in the elderly and in patients with concomitant illnesses
• Mortality to HHS is higher than DKA, mortality rates of 5–20%

Pathophysiology


Pathogenesis
• Insulin levels in HHS are inadequate to facilitate glucose utilization by insulin sensitive tissues but adequate to prevent lipolysis and subsequent ketogenesis

PRECIPITATING FACTORS
• Infection
• Discontinuation of or inadequate insulin therapy
• Pancreatitis
• Myocardial infarction
• Cerebrovascular accident
• Drugs that affect carbohydrate metabolism, such as corticosteroids, thiazides, sympathomimetic agents, and pentamidine
• New-onset type 1 diabetes
• An increasing number of DKA cases without precipitating cause in adolescents and adult with type 2 diabetes
HHS
• 20% have no history of diabetes, delayed recognition of hyperglycemic symptoms led to severe dehydration
• In most patients with HHS, restricted water intake is due to being bedridden is likely to result in severe dehydration and HHS
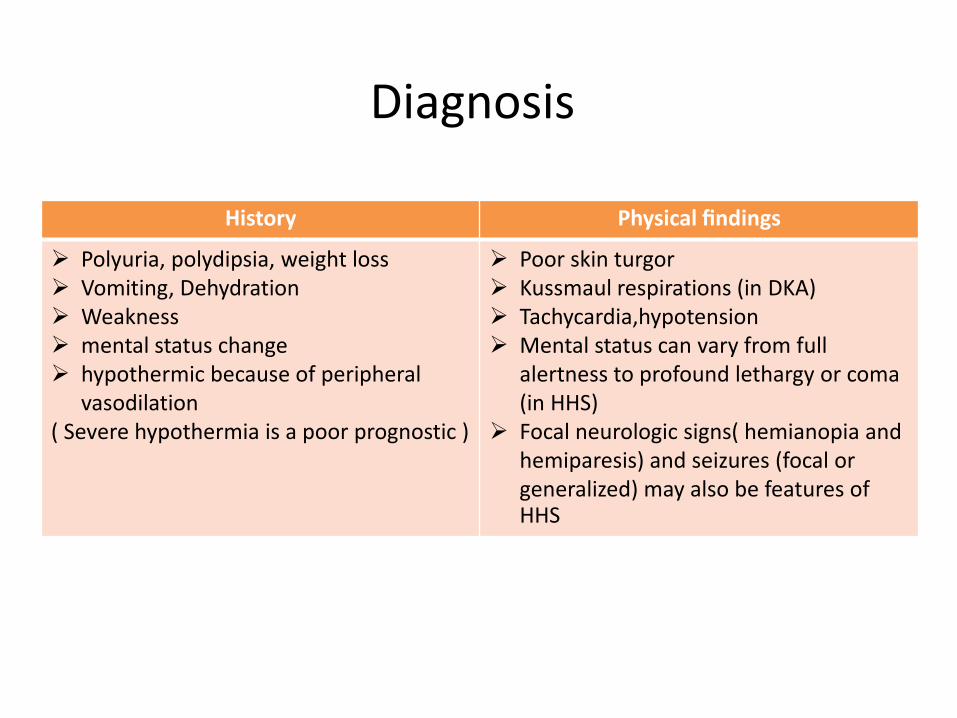
Diagnosis
History Physical findings
Polyuria, polydipsia, weight loss Vomiting, Dehydration Weakness mental status change hypothermic because of peripheral
vasodilation( Severe hypothermia is a poor prognostic )
Poor skin turgor Kussmaul respirations (in DKA) Tachycardia,hypotension Mental status can vary from full
alertness to profound lethargy or coma (in HHS)
Focal neurologic signs( hemianopia and hemiparesis) and seizures (focal or generalized) may also be features of HHS

•
Significant overlap between DKA and HHS has been reported in more than one-third of patients
Main metabolic product in ketoacidosis “serum hydroxybutyrate”
• Augmented ketonemia is performed by the nitroprusside reaction
– is highly sensitive, but it can underestimate the severity of ketoacidosis because does not recognize the presence of hydroxybutyrate

• Effective osmolality = 2 serum sodium + glucose(mg/dl)/ 18
• urea concentration is not taken into account because it Is freely permeable and its does not induce major changes in intracellular volume or osmotic gradient
• Plasma glucose levels in DKA that are independent of the severity of ketoacidosis
• “euglycemic DKA” —glucose levels< 250 mg/dl
• This could be due to
– including exogenous insulin injection en route to the hospital
– antecedent food restriction and inhibition of gluconeogenesis
– Pregnancy
– Medication : SGLT1

Concomitant labLeukoctosis(10,000-15,000) is attributed to stress and correlated to elevated levels
of cortisol and norepinephrine
Low serum sodium because of the osmotic flux of water from the intra- to the extracellular
High serum sodium indicates a rather profound degree of free water loss
High serum potassium extracellular shift of potassium
High serum phosphate insulin deficiency, hypertonicity, and increased catabolism all contribute to the movement of phosphate out of cells
Hyperamylasemia reported in 21–79% of patients with DKA there is little correlation between the presencehyperamylasemia and the presence of gastrointestinal symptoms (nausea, vomiting, and abdominal pain)
Differential diagnosis
• Starvation ketosis
• Alcoholic ketoacidosis
– Plasma glucose concentrations that range from mildly elevated (rarely 200 mg/dl) to hypoglycemia acidosis
– serum bicarbonate concentration in starvation ketosis is usually not 18 mEq/l
• High anion gap metabolic acidosis: lactic acidosis

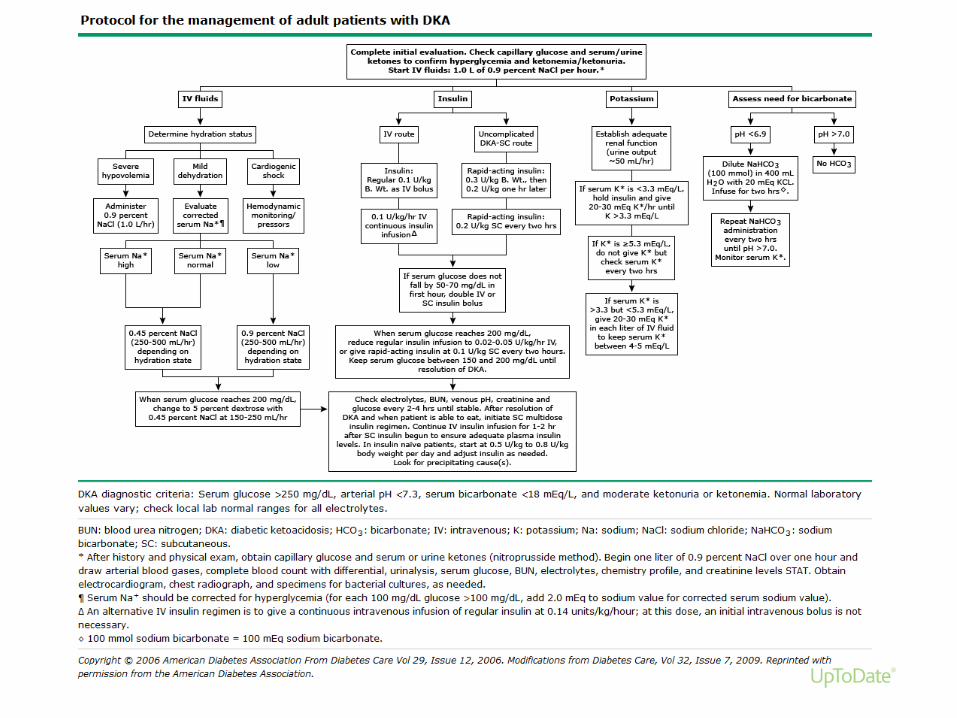
TREATMENT
• Correction of
1. Dehydration
2. Hyperglycemia
3. Electrolyte imbalances
4. Identification of precipitating events

DKA chart
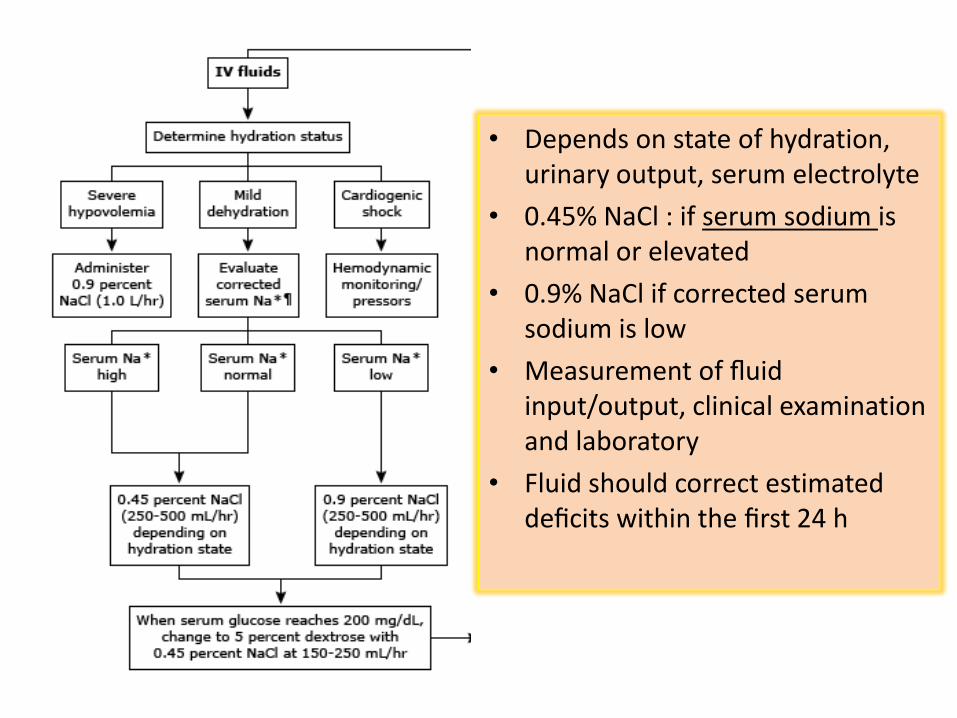
• Depends on state of hydration, urinary output, serum electrolyte
• 0.45% NaCl : if serum sodium is normal or elevated
• 0.9% NaCl if corrected serum sodium is low
• Measurement of fluid input/output, clinical examination and laboratory
• Fluid should correct estimated deficits within the first 24 h

• Hyperglycemia is corrected faster than ketoacidosis
• Mean duration until blood glucose is 250 mg/dl and ketoacidosis (pH 7.30; bicarbonate 18 mmol/l)is corrected is 6 and 12hr
• Once the plasma glucose is 200 mg/dl, 5% dextrose should be added
– until ketonemia is controlled while at the same time avoiding hypoglycemia

• Goal: decrease plasma glucose 50–75 mg/dl per hr
• If plasma glucose does not achieved
– Increased insulin infusion every hour until a steady glucose decline is achieved
Type Keep plasma glucose
DKA 150 and 200 mg/dl
HHS 250 and 300 mg/dl

Type Keep plasma glucose
DKA 150 and 200 mg/dl
HHS 250 and 300 mg/dl
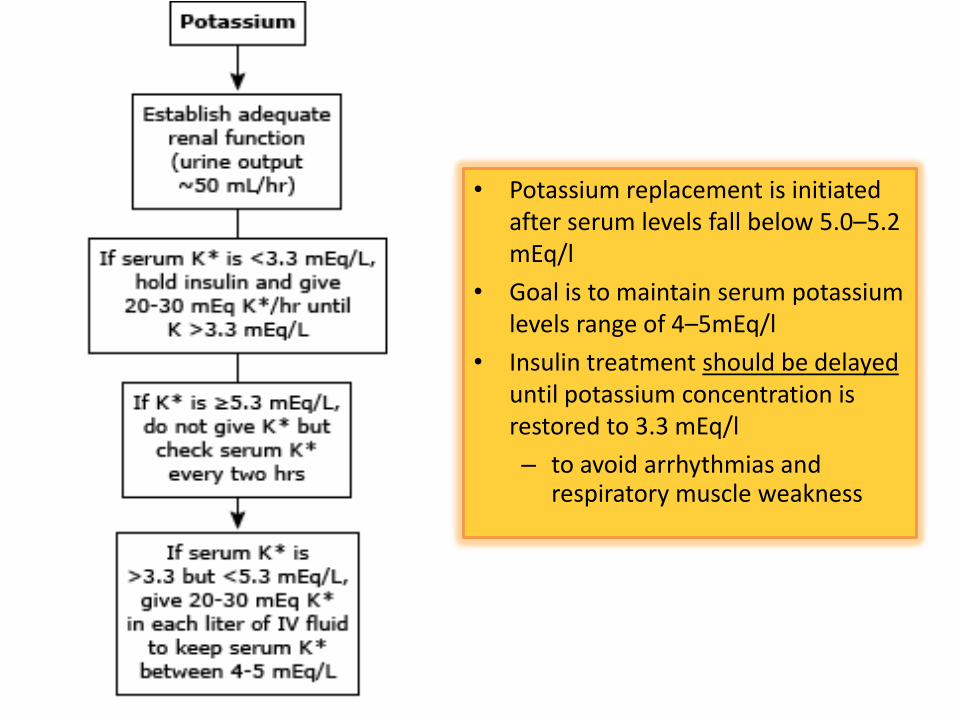
• Potassium replacement is initiated after serum levels fall below 5.0–5.2 mEq/l
• Goal is to maintain serum potassium levels range of 4–5mEq/l
• Insulin treatment should be delayed until potassium concentration is restored to 3.3 mEq/l
– to avoid arrhythmias and respiratory muscle weakness
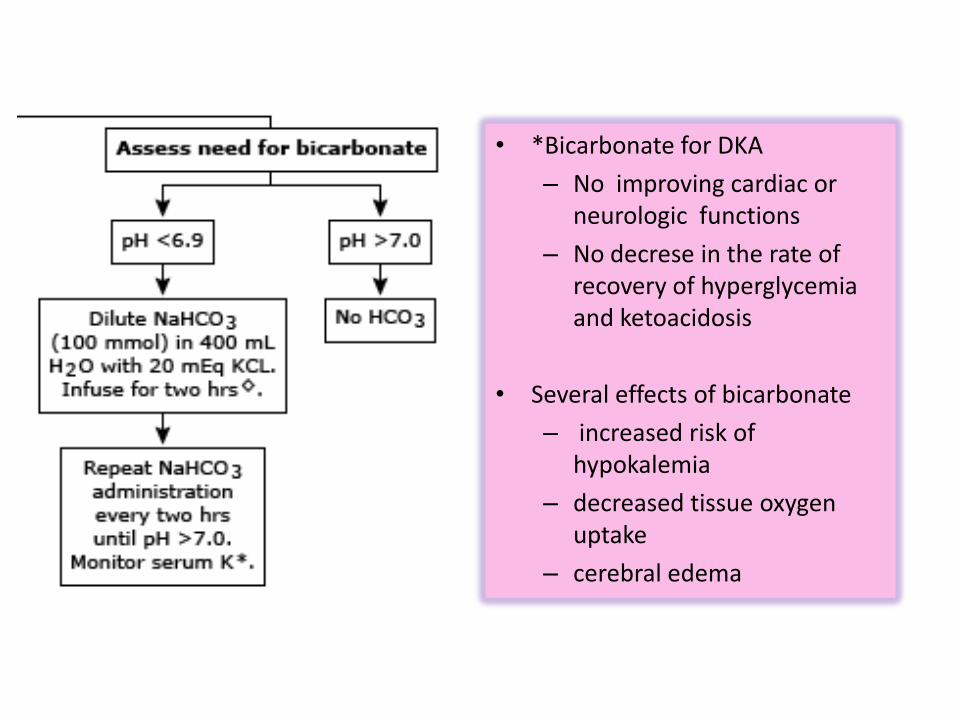
• *Bicarbonate for DKA
– No improving cardiac or neurologic functions
– No decrese in the rate of recovery of hyperglycemia and ketoacidosis
• Several effects of bicarbonate
– increased risk of hypokalemia
– decreased tissue oxygen uptake
– cerebral edema

Phosphate
• Whole body phosphate deficits in DKA that average 1.0 mmol/kg
• Phosphate concentration decreases with insulin therapy
• Careful phosphate replacement is indicated in patients with cardiac dysfunction, respiratory depression, serum phosphate <1.0 mg/dl
– 20–30 mEq/l potassium phosphate can be added to replacement fluids
• The maximal rate of phosphate is 4.5 mmol/h (1.5 ml/hofK2PO4)
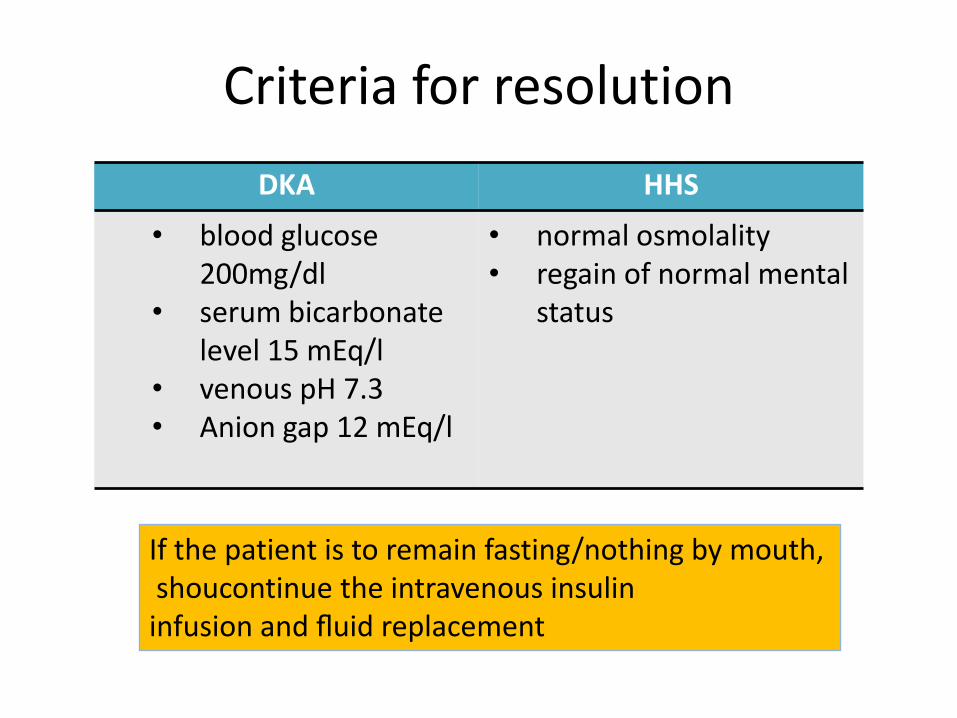
Criteria for resolution
DKA HHS
• blood glucose 200mg/dl
• serum bicarbonate level 15 mEq/l
• venous pH 7.3• Anion gap 12 mEq/l
• normal osmolality• regain of normal mental
status
If the patient is to remain fasting/nothing by mouth,shoucontinue the intravenous insulin infusion and fluid replacement

Transition to subcutaneous insulin
• Patients with known diabetes
– given insulin at the dosage they were receiving before the onset of DKA
• In insulin naïve patients
– multidose insulin regimen should be started at a dose of 0.5–0.8 units/kg/day

Complication
• Hypoglycemia
• Hypokalemia
• Hyperchloremic nonaniongap acidosis during the recovery phase caused by
– loss of ketoanions, which are metabolized to bicarbonate during the evolution of DKA
– excess fluid infusion of chloride containing fluids
• Cerebral edema (extremely rare) in adult, mortality rate of 20–40%
– Prevention might include avoidance of excessive hydration and rapid reduction of plasma osmolarity
Prevention is the best
after a short period of insulin therapy, prolonged remission is often possible, with diet or oral antihyperglycemic agents