Heflin Herring Infraclavicular
5
Case Report Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbow dislocation ☆ , ☆☆ We present the rst des cri ptio n of an ult ras ound -guide d infraclavicular brachial plexus block (ICB) performed by emergency physicians for reduction of an elbow dislocation. Although there is in- cre asi ng int ere st in reg ion al ane sth esi a for eme rge nc y pro ced ura l anes- the sia as a pot ent ial alternati ve to sed ati on, many eme rge ncy pro viders are justiably concerned for the potential complications and technic al dif culty. Herein, we describe in detail how to perfor m an ultrasound- guided ICB, which may be a superior alternative to interscalene or supraclavicular approaches to brachial plexus anesthesia for the arm below the midhumeral level. By moving the target injection area below the cl avic leand outof the ne ck , there is re duced systemic upt ak e of loc al ane sth eti c and red uce d ris k of loca l ane sth eti c mig rati on lea din g to unwant ed compli cationssuc h as sys temic toxi cit y, phr eni c ner ve pa- ral ysi s, and Horner syn drome.Rar e butcatast roph ic compli cat ions suc h as cer vic al spi nal cordsyrinxare avo ide d alt oget her . In add iti on, the ICB inv olv es targ etin g the bra chi al ple xus in a less ana tomi cal ly cons trai ned space and requires both less needle to nerve proximity and fewer nee- dle redirections (both procedural characteristics associated with re- duced risk of nerve injury). Elbow dislocations of the radius and ulna are best treated with timely, emergency reduction —the longer an elbow is allowed to remain dislocated, the more dif cult the reduction becomes, and risk of avascular necrosis increases. In our experience, the ultr aso und -gui ded ICB is a pote nti all y ide al tech niq ue tha t prov ide s safe, fast, effective analgesia and anesthesia for major upper extremity trauma below the midhumeral level worthy of further study in the emergency department setting. Fractures and dislocations of the upper extremity are common emerg ency department (ED) complai nts. Among those requir ing the prompt and timel y reduction are radia l and ulnar head dislocations at theelbow.Inde ed , tim e is func ti on wi th theelbo w, as de layin re duc- tion greatly increases risk of a failed reduction as well as avascular necrosis [1,2]. Pain management for procedures and major trauma to the upper extremity below the level of the midhumerus such as an elb ow dis loca tion can be achieved wit h a bra chi al ple xus block. Although the interscalene and supraclavicular brachial plexus blocks (SCB) are well known in the emergenc y setting, the ultrasound- guided infraclavicular brachial plexus block (ICB) is a potentially safer, more effective technique that has not yet described in the emergency medicine literature [3,4]. The ultrasound-guided ICB has several potential advantages vs the SCB. Several studies suggest a higher success rate for both novice and experienced providers with the ICB vs SCB [5-8]. In addition, the risk of complications such as paresthesias from needle to nerve contact, Hor ner syn drome,and phr enic ner ve par aly sis is sig ni can tly les s lik ely with the ultrasound-guided ICB than with the alternative SCB [5-9]. Potentially devastating complications related to cervical spinal cord in- jectio n are elimi nated altoge ther. The incre ased safet y and succ ess rates associated with the infraclavicular approach to brachial plexus analge- sia,it is a pote nti allyimpor tantadditi on to the eme rge ncy pro vide r'sre- gional anest hesia techn ical armame ntarium . We describe the techni que and present a case where an ultrasound-guided ICB was used as anes- thesia for a successful reduction of a posterior elbow dislocation. A 29-year-old male presented to the ED to a level complaining of left elbow pain with a shortened left forearm held in exion with a closed, prominent olecranon posterior deformity ( Fig. 1). Neurologic examin ation of the ulnar, median, and radial nerves reveale d intact function. Plain lms conrmed a posterior elbow dislocation without fracture (Fig. 2). After discussion of the risks and bene ts, patient consen t was obtaine d, and a single -injec tion ultras ound-gui ded pericoracoid ICB was performed [10]. The ultrasound-guided ICB was performed by a trainee provider (N20 blocks) supervised by an experi- enc ed p rovide r with gre ate r tha n 100 blo cks exp eri enc e. A line ar tra ns- duce r wasplac ed 2 cm infe ri or and 2 cm me di al to the cora co id process in the paras agi ttal plan e; the brachia l ple xus was vis ualized at the lev el of cor ds, adja ce nt to the axi lla ry arte ry (Fi g. 3). A 30- mm 22- gauge blu nt tipped block needle was advanced under ultrasound-guidance in the para sag itta l pla ne fro m cep ha lad to cau dad toward the post eri or/ dor sal aspect of the axill ary ar tery; 25 mL of me pivaca ine 1.5% was inject ed in small aliquots after negativ e aspiration just deep to the axillar y artery, obtaining the “double bubble” sign as local anesthetic spread in the periplexus space [10] (Figs. 4 and 5). Twenty minutes later, the elbow was easily and painlessly reduced without complications ( Fig. 2). The patient experienced no dyspnea or othe r clinical sign of pneum othorax or phrenic paralysis. Management of painful fracture dislocations is common in the ED. In adults, the elbow is the most commonly dislocated joint after the shoul der a nd the most common di sloca tion in p ediatr ics [1,2]. Regional anesth esia presents a practi cal, ef cient option for analgesia and ane sthe sia tha t is avai lable urgent ly at beds ide as alte rna tive to deep sedation. Indeed, regional anesthesia is a particularly attractive opti on in the inc rea singly common opi oid tole rant pati ent with increa sed risk for sedatio n-rela ted compli cations [4]. Although the ultrasound-guided ICB is potentially the safest, easiest to learn, and most rel iabl e bra chi al ple xus blo ck, it has pre vio usl y not bee n des cri bed in emergency medicine. American Journal of Emergency Medicine xxx (2015) xxx–xxx ☆ Previous presentations: none. ☆☆ S ources of support: none. 0735-6757/© 2015 Elsevier Inc. All rights reserved. Contents lists available at ScienceDire ct American Journal of Emergency Medicine j o u r na l h omepag e : www.elsevier.com/locate/ajem Pl ea se ci te this ar tic le as : Hein T, et al, Ult ras oun d-gu ided inf rac lav icu lar brachial ple xus blo ck for eme rge ncy man age men t of a pos ter ior elb ow dislocation, Am J Emerg Med (2015), http://dx.doi.org/10.1016/j.ajem.2015.06.019
-
Upload
andrew-herring -
Category
Documents
-
view
217 -
download
0
Transcript of Heflin Herring Infraclavicular

8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 14
Case Report
Ultrasound-guided infraclavicular brachial plexus block for emergency
management of a posterior elbow dislocation
We present the 1047297rst description of an ultrasound-guided
infraclavicular brachial plexus block (ICB) performed by emergency
physicians for reduction of an elbow dislocation Although there is in-
creasing interest in regional anesthesia for emergency procedural anes-
thesia as a potential alternative to sedation many emergency providers
are justi1047297
ably concerned for the potential complications and technicaldif 1047297culty Herein we describe in detail how to perform an ultrasound-
guided ICB which may be a superior alternative to interscalene or
supraclavicular approaches to brachial plexus anesthesia for the arm
below the midhumeral level By moving the target injection area
below the clavicle and outof the neck there is reduced systemic uptake
of local anesthetic and reduced risk of local anesthetic migration leading
to unwanted complications such as systemic toxicity phrenic nerve pa-
ralysis and Horner syndrome Rare but catastrophic complications such
as cervical spinal cordsyrinxare avoided altogether In addition the ICB
involves targeting the brachial plexus in a less anatomically constrained
space and requires both less needle to nerve proximity and fewer nee-
dle redirections (both procedural characteristics associated with re-
duced risk of nerve injury) Elbow dislocations of the radius and ulna
are best treated with timely emergency reductionmdashthe longer an
elbow is allowed to remain dislocated the more dif 1047297cult the reduction
becomes and risk of avascular necrosis increases In our experience
the ultrasound-guided ICB is a potentially ideal technique that provides
safe fast effective analgesia and anesthesia for major upper extremity
trauma below the midhumeral level worthy of further study in the
emergency department setting
Fractures and dislocations of the upper extremity are common
emergency department (ED) complaints Among those requiring
the prompt and timely reduction are radial and ulnar head dislocations
at theelbowIndeed time is function with theelbow as delayin reduc-
tion greatly increases risk of a failed reduction as well as avascular
necrosis [12] Pain management for procedures and major trauma to
the upper extremity below the level of the midhumerus such as an
elbow dislocation can be achieved with a brachial plexus block
Although the interscalene and supraclavicular brachial plexus blocks
(SCB) are well known in the emergency setting the ultrasound-
guided infraclavicular brachial plexus block (ICB) is a potentially safer
more effective technique that has not yet described in the emergency
medicine literature [34]
The ultrasound-guided ICB has several potential advantages vs the
SCB Several studies suggest a higher success rate for both novice and
experienced providers with the ICB vs SCB [5-8] In addition the risk
of complications such as paresthesias from needle to nerve contact
Horner syndrome and phrenic nerve paralysis is signi1047297cantly less likely
with the ultrasound-guided ICB than with the alternative SCB [5-9]Potentially devastating complications related to cervical spinal cord in-
jection are eliminated altogether The increased safety and success rates
associated with the infraclavicular approach to brachial plexus analge-
siait is a potentiallyimportantaddition to the emergency providersre-
gional anesthesia technical armamentarium We describe the technique
and present a case where an ultrasound-guided ICB was used as anes-
thesia for a successful reduction of a posterior elbow dislocation
A 29-year-old male presented to the ED to a level complaining of
left elbow pain with a shortened left forearm held in 1047298exion with a
closed prominent olecranon posterior deformity (Fig 1) Neurologic
examination of the ulnar median and radial nerves revealed intact
function Plain 1047297lms con1047297rmed a posterior elbow dislocation without
fracture (Fig 2) After discussion of the risks and bene1047297ts patient
consent was obtained and a single-injection ultrasound-guided
pericoracoid ICB was performed [10] The ultrasound-guided ICB was
performed by a trainee provider (N20 blocks) supervised by an experi-
enced provider with greater than 100 blocks experience A linear trans-
ducer wasplaced 2 cm inferior and 2 cm medial to the coracoid process
in the parasagittal plane the brachial plexus was visualized at the level
of cords adjacent to the axillary artery (Fig 3) A 30-mm 22-gauge blunt
tipped block needle was advanced under ultrasound-guidance in the
parasagittal plane from cephalad to caudad toward the posteriordorsal
aspect of the axillary artery 25 mL of mepivacaine 15 was injected in
small aliquots after negative aspiration just deep to the axillary artery
obtaining the ldquodouble bubblerdquo sign as local anesthetic spread in the
periplexus space [10] (Figs 4 and 5) Twenty minutes later the elbow
was easily and painlessly reduced without complications (Fig 2) The
patient experienced no dyspnea or other clinical sign of pneumothorax
or phrenic paralysis
Management of painful fracture dislocations is common in the ED
In adults the elbow is the most commonly dislocated joint after the
shoulder and the most common dislocation in pediatrics [12] Regional
anesthesia presents a practical ef 1047297cient option for analgesia and
anesthesia that is available urgently at bedside as alternative to
deep sedation Indeed regional anesthesia is a particularly attractive
option in the increasingly common opioid tolerant patient with
increased risk for sedation-related complications [4] Although the
ultrasound-guided ICB is potentially the safest easiest to learn and
most reliable brachial plexus block it has previously not been described
in emergency medicine
American Journal of Emergency Medicine xxx (2015) xxxndashxxx
Previous presentations none Sources of support none
0735-6757copy 2015 Elsevier Inc All rights reserved
Contents lists available at ScienceDirect
American Journal of Emergency Medicine
j o u r n a l h o m e p a g e w w w e l s e v i e r c o m l o c a t e a j e m
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019
8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 24
The ultrasound-guided ICB is an important alternative to
interscalene and supraclavicular techniques for emergency providers
who use brachialplexus anesthesia in their practice[3] Bene1047297ts include
reduced incidence of complications such as paresthesias (needle-to-
nerve contact during the procedure) phrenic paralysis and Horner syn-drome easy positioning and technical simplicity and reduced systemic
absorption of local anesthetic [35-11] Rates of pneumothorax for the
ultrasound-guided ICB are also very low Some providers may be con-
cerned with depth of the target spacemdashapproximately 3 to 4 cmmdashin
most patients however this has not been shown to slow or complicate
the procedure [5-9] We chose 15 mepivacaine because it has a rapid
onset (10-20 minutes) with 2 to 3 hours of dense surgical anesthesia
followed by up to 8 hours of analgesia withexcellent safety record com-
parable with that of lidocaine
The ultrasound-guided ICB single-injection technique described
aims to producea shallowsaucer-shaped spread of local anesthetic pos-
teriordorsal to the axillary artery which is visualized as a ldquodouble bub-
blerdquo sign on ultrasound (Fig 5) This simple technique has been shown
to have superior rates of success among novice and experienced pro-viders with fewer complications [710] In emergency medicine simpli-
1047297ed techniques are particularly important given the intermittent nature
of procedural practice and multiple simultaneous responsibilities placed
on emergency providers while working The role of ultrasound-guided
ICB as an alternative to SCB or sedation warrants further study
Thomas He1047298in MD
Terry Ahern MD
Highland Hospitalndash Alameda Health System Oakland CA
Andrew Herring MD
Highland Hospitalndash Alameda Health System Oakland CA
University of California San Francisco San Francisco CA
Corresponding author 1411 East 39th St Oakland CA 94602Tel +1 510 437 4564 fax +1 510 437 8322
E-mail address andrewaherringgmailcom
httpdxdoiorg101016jajem201506019
References
[1] Mehta JA Bain GI Elbow dislocations in adults and children Clin Sports Med 200423(4)609ndash27 [ix]
[2] Lattanza LL Keese G Elbow instability in children Hand Clin 200824(1)139ndash52
[3] Fredrickson MJ Wolstencroft P Evidence-based medicine supports ultrasound-guided infraclavicular block over the corner pocket supraclavicular technique RegAnesth Pain Med 201136(5)525ndash6
[4] Stone MB Wang R Price DD Ultrasound-guided supraclavicular brachial plexusnerve block vs procedural sedation for the treatment of upper extremity emergen-cies Am J Emerg Med 200826(6)706ndash10
[5] Mariano ER Sandhu NS Loland VJ Bishop ML Madison SJ Abrams RA et al A ran-domized comparison of infraclavicular and supraclavicular continuous peripheralnerve blocks for postoperative analgesia Reg Anesth Pain Med 201136(1)26ndash31
[6] Koscielniak-Nielsen ZJ Frederiksen BS Rasmussen H Hesselbjerg L A comparison of ultrasound-guided supraclavicular and infraclavicular blocks for upper extremitysurgery Acta Anaesthesiol Scand 200953(5)620ndash6
[7] Fredrickson MJ Patel A Young S Chinchanwala S Speed of onset of ldquocorner pocketsupraclavicularrdquo and infraclavicular ultrasound guided brachial plexus block arandomised observer-blinded comparison Anaesthesia 200964(7)738ndash44
[8] McCartney CJ Lin L Shastri U Evidence basis for the use of ultrasound for upper-extremity blocks Reg Anesth Pain Med 201035(2 Suppl)S10ndash5
[9] Yazer MS Finlayson RJ Tran de QH A randomized comparison betweeninfraclavicular block and targeted intracluster injection supraclavicular block RegAnesth Pain Med 201540(1)11ndash5
[10] Tran DQ Charghi R Finlayson RJ The double bubble sign for successfulinfraclavicular brachial plexus blockade Anesth Analg 2006103(4)1048ndash9
[11] Rettig HC Lerou JG Gielen MJ Boersma E Burm AG The pharmacokinetics of ropivacaine after four different techniques of brachial plexus blockade Anaesthesia200762(10)1008ndash14
Fig 2 Plain 1047297lms showing posterior dislocation of both the radial and ulnar head before
reduction (top panel) and after successful reduction (bottom panel)
Fig 1 Left elbow posterior dislocation before reduction
2 T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019
8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 34
Fig 3 Setup andneedle approach for the ultrasound-guided ICB A The patient is positioned supine the operator is at thehead of thebed with an unobstructed lineof sight to the ultra-
sounddisplaynearthe patientswaist B A linearor small footprintcurvilinearprobeis placed in theparasagittal plane justmedial tothe coracoid processand inferiorto theclavicleAt this
position the pectoralis major and minor muscles are identi1047297ed with the axillary vein and artery underneath The brachial cords of the plexus clustered around the artery
3T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019
8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 44
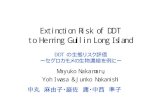
Fig 5 Con1047297rmation of ultrasound-guided infraclavicular brachial plexus injection with
ldquodouble bubblerdquo sign The dashed line outlines the axillary artery as the top ldquobubblerdquo
the accumulating local anesthetic after injection posteriordorsal to the artery is the sec-
ond ldquo
bubblerdquo
Fig 4 Ultrasound-guidedinfraclavicularbrachial plexus injection A The needle is advanced
in the parasagittal plane from toward the posteriordorsalaspect of the axillary artery Local
anesthetic is seen to 1047298owing between the axillary artery and the intercostal muscles
4 T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019

8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 24
The ultrasound-guided ICB is an important alternative to
interscalene and supraclavicular techniques for emergency providers
who use brachialplexus anesthesia in their practice[3] Bene1047297ts include
reduced incidence of complications such as paresthesias (needle-to-
nerve contact during the procedure) phrenic paralysis and Horner syn-drome easy positioning and technical simplicity and reduced systemic
absorption of local anesthetic [35-11] Rates of pneumothorax for the
ultrasound-guided ICB are also very low Some providers may be con-
cerned with depth of the target spacemdashapproximately 3 to 4 cmmdashin
most patients however this has not been shown to slow or complicate
the procedure [5-9] We chose 15 mepivacaine because it has a rapid
onset (10-20 minutes) with 2 to 3 hours of dense surgical anesthesia
followed by up to 8 hours of analgesia withexcellent safety record com-
parable with that of lidocaine
The ultrasound-guided ICB single-injection technique described
aims to producea shallowsaucer-shaped spread of local anesthetic pos-
teriordorsal to the axillary artery which is visualized as a ldquodouble bub-
blerdquo sign on ultrasound (Fig 5) This simple technique has been shown
to have superior rates of success among novice and experienced pro-viders with fewer complications [710] In emergency medicine simpli-
1047297ed techniques are particularly important given the intermittent nature
of procedural practice and multiple simultaneous responsibilities placed
on emergency providers while working The role of ultrasound-guided
ICB as an alternative to SCB or sedation warrants further study
Thomas He1047298in MD
Terry Ahern MD
Highland Hospitalndash Alameda Health System Oakland CA
Andrew Herring MD
Highland Hospitalndash Alameda Health System Oakland CA
University of California San Francisco San Francisco CA
Corresponding author 1411 East 39th St Oakland CA 94602Tel +1 510 437 4564 fax +1 510 437 8322
E-mail address andrewaherringgmailcom
httpdxdoiorg101016jajem201506019
References
[1] Mehta JA Bain GI Elbow dislocations in adults and children Clin Sports Med 200423(4)609ndash27 [ix]
[2] Lattanza LL Keese G Elbow instability in children Hand Clin 200824(1)139ndash52
[3] Fredrickson MJ Wolstencroft P Evidence-based medicine supports ultrasound-guided infraclavicular block over the corner pocket supraclavicular technique RegAnesth Pain Med 201136(5)525ndash6
[4] Stone MB Wang R Price DD Ultrasound-guided supraclavicular brachial plexusnerve block vs procedural sedation for the treatment of upper extremity emergen-cies Am J Emerg Med 200826(6)706ndash10
[5] Mariano ER Sandhu NS Loland VJ Bishop ML Madison SJ Abrams RA et al A ran-domized comparison of infraclavicular and supraclavicular continuous peripheralnerve blocks for postoperative analgesia Reg Anesth Pain Med 201136(1)26ndash31
[6] Koscielniak-Nielsen ZJ Frederiksen BS Rasmussen H Hesselbjerg L A comparison of ultrasound-guided supraclavicular and infraclavicular blocks for upper extremitysurgery Acta Anaesthesiol Scand 200953(5)620ndash6
[7] Fredrickson MJ Patel A Young S Chinchanwala S Speed of onset of ldquocorner pocketsupraclavicularrdquo and infraclavicular ultrasound guided brachial plexus block arandomised observer-blinded comparison Anaesthesia 200964(7)738ndash44
[8] McCartney CJ Lin L Shastri U Evidence basis for the use of ultrasound for upper-extremity blocks Reg Anesth Pain Med 201035(2 Suppl)S10ndash5
[9] Yazer MS Finlayson RJ Tran de QH A randomized comparison betweeninfraclavicular block and targeted intracluster injection supraclavicular block RegAnesth Pain Med 201540(1)11ndash5
[10] Tran DQ Charghi R Finlayson RJ The double bubble sign for successfulinfraclavicular brachial plexus blockade Anesth Analg 2006103(4)1048ndash9
[11] Rettig HC Lerou JG Gielen MJ Boersma E Burm AG The pharmacokinetics of ropivacaine after four different techniques of brachial plexus blockade Anaesthesia200762(10)1008ndash14
Fig 2 Plain 1047297lms showing posterior dislocation of both the radial and ulnar head before
reduction (top panel) and after successful reduction (bottom panel)
Fig 1 Left elbow posterior dislocation before reduction
2 T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019
8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 34
Fig 3 Setup andneedle approach for the ultrasound-guided ICB A The patient is positioned supine the operator is at thehead of thebed with an unobstructed lineof sight to the ultra-
sounddisplaynearthe patientswaist B A linearor small footprintcurvilinearprobeis placed in theparasagittal plane justmedial tothe coracoid processand inferiorto theclavicleAt this
position the pectoralis major and minor muscles are identi1047297ed with the axillary vein and artery underneath The brachial cords of the plexus clustered around the artery
3T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019
8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 44
Fig 5 Con1047297rmation of ultrasound-guided infraclavicular brachial plexus injection with
ldquodouble bubblerdquo sign The dashed line outlines the axillary artery as the top ldquobubblerdquo
the accumulating local anesthetic after injection posteriordorsal to the artery is the sec-
ond ldquo
bubblerdquo
Fig 4 Ultrasound-guidedinfraclavicularbrachial plexus injection A The needle is advanced
in the parasagittal plane from toward the posteriordorsalaspect of the axillary artery Local
anesthetic is seen to 1047298owing between the axillary artery and the intercostal muscles
4 T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019

8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 34
Fig 3 Setup andneedle approach for the ultrasound-guided ICB A The patient is positioned supine the operator is at thehead of thebed with an unobstructed lineof sight to the ultra-
sounddisplaynearthe patientswaist B A linearor small footprintcurvilinearprobeis placed in theparasagittal plane justmedial tothe coracoid processand inferiorto theclavicleAt this
position the pectoralis major and minor muscles are identi1047297ed with the axillary vein and artery underneath The brachial cords of the plexus clustered around the artery
3T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019
8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 44
Fig 5 Con1047297rmation of ultrasound-guided infraclavicular brachial plexus injection with
ldquodouble bubblerdquo sign The dashed line outlines the axillary artery as the top ldquobubblerdquo
the accumulating local anesthetic after injection posteriordorsal to the artery is the sec-
ond ldquo
bubblerdquo
Fig 4 Ultrasound-guidedinfraclavicularbrachial plexus injection A The needle is advanced
in the parasagittal plane from toward the posteriordorsalaspect of the axillary artery Local
anesthetic is seen to 1047298owing between the axillary artery and the intercostal muscles
4 T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019

8202019 Heflin Herring Infraclavicular
httpslidepdfcomreaderfullheflin-herring-infraclavicular 44
Fig 5 Con1047297rmation of ultrasound-guided infraclavicular brachial plexus injection with
ldquodouble bubblerdquo sign The dashed line outlines the axillary artery as the top ldquobubblerdquo
the accumulating local anesthetic after injection posteriordorsal to the artery is the sec-
ond ldquo
bubblerdquo
Fig 4 Ultrasound-guidedinfraclavicularbrachial plexus injection A The needle is advanced
in the parasagittal plane from toward the posteriordorsalaspect of the axillary artery Local
anesthetic is seen to 1047298owing between the axillary artery and the intercostal muscles
4 T He 1047298in et al American Journal of Emergency Medicine xxx (2015) xxxndash xxx
Please cite this article as He1047298in T et al Ultrasound-guided infraclavicular brachial plexus block for emergency management of a posterior elbowdislocation Am J Emerg Med (2015) httpdxdoiorg101016jajem201506019