EffectorRegulatoryTCellsReflecttheEquilibrium between ...Immunology,World Premier International...
7
Cancer Immunology Miniatures Effector Regulatory T Cells Reflect the Equilibrium between Antitumor Immunity and Autoimmunity in Adult T-cell Leukemia Hiroshi Ureshino 1 , Takero Shindo 1 , Hiroyoshi Nishikawa 2 , Nobukazu Watanabe 3 , Eri Watanabe 3 , Natsuko Satoh 3 , Kazutaka Kitaura 4,5 , Hiroaki Kitamura 1 , Kazuko Doi 6 , Kotaro Nagase 7 , Hiromi Kimura 7 , Makoto Samukawa 8 , Susumu Kusunoki 8 , Masaharu Miyahara 9 , Tadasu Shin-I 10 , Ryuji Suzuki 4 , Shimon Sakaguchi 2 , and Shinya Kimura 1 Abstract The regulatory T cells (Treg) with the most potent immuno- suppressive activity are the effector Tregs (eTreg) with a CD45RA – Foxp3 þþ CCR4 þ phenotype. Adult T-cell leukemia (ATL) cells often share the Treg phenotype and also express CCR4. Although mogamulizumab, a monoclonal antibody to CCR4, shows marked antitumor effects against ATL and peripheral T-cell lymphoma, concerns have been raised that it may induce severe autoimmune immunopathology by depleting eTregs. Here, we present case reports for two patients with ATL who responded to mogamulizumab but developed a severe skin rash and autoimmune brainstem encephalitis. Deep sequencing of the T-cell receptor revealed that ATL cells and naturally occurring Tregs within the cell population with a Treg phenotype can be clearly distinguished according to CADM1 expression. The onset of skin rash and brainstem encephalitis was coincident with eTreg depletion from the peripheral blood, whereas ATL relapses were coincident with eTreg recovery. These results imply that eTreg numbers in the peripheral blood sensitively reflect the equilibrium between antitumor immuni- ty and autoimmunity, and that mogamulizumab might sup- press ATL until the eTreg population recovers. Close monitoring of eTreg numbers is crucial if we are to provide immunomodu- latory treatments that target malignancy without severe adverse events. Cancer Immunol Res; 4(8); 644–9. Ó2016 AACR. Introduction Human regulatory T cells (Treg) suppress immune reac- tions, including autoimmunity and antitumor immunity; therefore, inhibiting Treg activity is becoming an important focus of cancer treatment (1). Tregs are classified into several subtypes, the most suppressive being effector Tregs (eTreg), which express a CD45RA – Foxp3 þþ phenotype and the che- mokine receptor CCR4 (2, 3). Adult T-cell leukemia (ATL) is a therapy-resistant hematologic malignancy with a poor prog- nosis (4, 5). ATL occurs in about 5% of human T-lympho- tropic virus type-1 (HTLV-1) carriers, and most ATL cells express CCR4 (6, 7). ATL cells often share the Treg phenotype, i.e., CD3 þ CD4 þ CD25 þ Foxp3 þ (8, 9). Although ATL cells may be defined by their expression of CADM1 (10, 11), the overlap and differences between Tregs and ATL cells remain unclear. Mogamulizumab is a defucosylated and humanized mono- clonal antibody to CCR4 that shows marked effects against ATL (12) and peripheral T-cell lymphoma (13). It works directly by depleting tumor cells and indirectly by increasing antitumor immunity through eTreg depletion via antibody-dependent cellular cytotoxicity (3). However, it sometimes causes adverse events, including a skin rash or Stevens–Johnson syndrome (14, 15), which may be attributed to Treg depletion. However, the association between therapeutic effects, adverse events, and Treg depletion remains unclear. Here, we report on two mogamulizumab-treated ATL patients who developed severe skin rash and brainstem enceph- alitis. Deep sequence analysis of the T-cell receptor (TCR) reper- toire revealed that CADM1 expression specifies minimal residual ATL cells within the cell population with a Treg pheno- type. While the immunopathology was closely associated with eTreg depletion, ATL relapsed as eTregs recovered. Despite the fact that mogamulizumab suppresses ATL, it can induce serious 1 Department of Hematology, Respiratory Medicine and Oncology, Saga University School of Medicine, Saga, Japan. 2 Experimental Immunology,World Premier International Research Center, Immunol- ogy Frontier Research Center, Osaka University, Suita, Japan. 3 Labo- ratory of Diagnostic Medicine, Division of Stem Cell Therapy, Institute of Medical Science, The University of Tokyo,Tokyo, Japan. 4 Depart- ment of Clinical Immunology, Clinical Research Center for Allergy and Rheumatology, Sagamihara National Hospital, Sagamihara, Japan. 5 Repertoire Genesis, Inc., Ibaraki, Japan. 6 Department of Dermatolo- gy, Karatsu Red Cross Hospital, Karatsu, Japan. 7 Department of Der- matology, Saga University School of Medicine, Saga, Japan. 8 Depart- ment of Neurology, Kinki University School of Medicine, Sayama, Japan. 9 Department of Internal Medicine, Karatsu Red Cross Hospital, Karatsu, Japan. 10 BITS Co. Ltd., Tokyo, Japan. Note: Supplementary data for this article are available at Cancer Immunology Research Online (http://cancerimmunolres.aacrjournals.org/). Current address for Hiroyoshi Nishikawa: Exploratory Oncology Research and Clinical Trial Center, National Cancer Center, Tokyo, Japan. Corresponding Author: Takero Shindo, Saga University School of Medicine, 5-1-1 Nabeshima, Saga 849-8501, Japan. Phone: 81-952-34-2366; Fax: 81-952-34- 2017; E-mail: [email protected] doi: 10.1158/2326-6066.CIR-15-0303 Ó2016 American Association for Cancer Research. Cancer Immunology Research Cancer Immunol Res; 4(8) August 2016 644 on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303
Transcript of EffectorRegulatoryTCellsReflecttheEquilibrium between ...Immunology,World Premier International...

Cancer Immunology Miniatures
EffectorRegulatoryTCells Reflect theEquilibriumbetween Antitumor Immunity and Autoimmunityin Adult T-cell LeukemiaHiroshi Ureshino1, Takero Shindo1, Hiroyoshi Nishikawa2, Nobukazu Watanabe3,Eri Watanabe3, Natsuko Satoh3, Kazutaka Kitaura4,5, Hiroaki Kitamura1, Kazuko Doi6,Kotaro Nagase7, Hiromi Kimura7, Makoto Samukawa8, Susumu Kusunoki8,Masaharu Miyahara9, Tadasu Shin-I10, Ryuji Suzuki4, Shimon Sakaguchi2, andShinya Kimura1
Abstract
The regulatory T cells (Treg) with the most potent immuno-suppressive activity are the effector Tregs (eTreg) with aCD45RA–Foxp3þþCCR4þ phenotype. Adult T-cell leukemia(ATL) cells often share the Treg phenotype and also expressCCR4. Although mogamulizumab, a monoclonal antibodyto CCR4, shows marked antitumor effects against ATL andperipheral T-cell lymphoma, concerns have been raised thatit may induce severe autoimmune immunopathology bydepleting eTregs. Here, we present case reports for two patientswith ATL who responded to mogamulizumab but developed asevere skin rash and autoimmune brainstem encephalitis. Deepsequencing of the T-cell receptor revealed that ATL cells and
naturally occurring Tregs within the cell population with a Tregphenotype can be clearly distinguished according to CADM1expression. The onset of skin rash and brainstem encephalitiswas coincident with eTreg depletion from the peripheral blood,whereas ATL relapses were coincident with eTreg recovery.These results imply that eTreg numbers in the peripheral bloodsensitively reflect the equilibrium between antitumor immuni-ty and autoimmunity, and that mogamulizumab might sup-press ATL until the eTreg population recovers. Close monitoringof eTreg numbers is crucial if we are to provide immunomodu-latory treatments that target malignancy without severe adverseevents. Cancer Immunol Res; 4(8); 644–9. �2016 AACR.
IntroductionHuman regulatory T cells (Treg) suppress immune reac-
tions, including autoimmunity and antitumor immunity;therefore, inhibiting Treg activity is becoming an importantfocus of cancer treatment (1). Tregs are classified into several
subtypes, the most suppressive being effector Tregs (eTreg),which express a CD45RA–Foxp3þþ phenotype and the che-mokine receptor CCR4 (2, 3). Adult T-cell leukemia (ATL) is atherapy-resistant hematologic malignancy with a poor prog-nosis (4, 5). ATL occurs in about 5% of human T-lympho-tropic virus type-1 (HTLV-1) carriers, and most ATL cellsexpress CCR4 (6, 7). ATL cells often share the Treg phenotype,i.e., CD3þCD4þCD25þFoxp3þ (8, 9). Although ATL cells maybe defined by their expression of CADM1 (10, 11), the overlapand differences between Tregs and ATL cells remain unclear.
Mogamulizumab is a defucosylated and humanized mono-clonal antibody to CCR4 that shows marked effects against ATL(12) and peripheral T-cell lymphoma (13). It works directly bydepleting tumor cells and indirectly by increasing antitumorimmunity through eTreg depletion via antibody-dependentcellular cytotoxicity (3). However, it sometimes causes adverseevents, including a skin rash or Stevens–Johnson syndrome(14, 15), which may be attributed to Treg depletion. However,the association between therapeutic effects, adverse events, andTreg depletion remains unclear.
Here, we report on two mogamulizumab-treated ATLpatients who developed severe skin rash and brainstem enceph-alitis. Deep sequence analysis of the T-cell receptor (TCR) reper-toire revealed that CADM1 expression specifies minimalresidual ATL cells within the cell population with a Treg pheno-type. While the immunopathology was closely associated witheTreg depletion, ATL relapsed as eTregs recovered. Despite the factthat mogamulizumab suppresses ATL, it can induce serious
1Department of Hematology, Respiratory Medicine and Oncology,Saga University School of Medicine, Saga, Japan. 2ExperimentalImmunology,World Premier International Research Center, Immunol-ogy Frontier Research Center, Osaka University, Suita, Japan. 3Labo-ratory of Diagnostic Medicine, Division of Stem Cell Therapy, Instituteof Medical Science, The University of Tokyo, Tokyo, Japan. 4Depart-ment of Clinical Immunology, Clinical Research Center for Allergy andRheumatology, Sagamihara National Hospital, Sagamihara, Japan.5Repertoire Genesis, Inc., Ibaraki, Japan. 6Department of Dermatolo-gy, Karatsu Red Cross Hospital, Karatsu, Japan. 7Department of Der-matology, Saga University School of Medicine, Saga, Japan. 8Depart-ment of Neurology, Kinki University School of Medicine, Sayama,Japan. 9Department of Internal Medicine, Karatsu Red Cross Hospital,Karatsu, Japan. 10BITS Co. Ltd., Tokyo, Japan.
Note: Supplementary data for this article are available at Cancer ImmunologyResearch Online (http://cancerimmunolres.aacrjournals.org/).
Current address for Hiroyoshi Nishikawa: Exploratory Oncology Research andClinical Trial Center, National Cancer Center, Tokyo, Japan.
CorrespondingAuthor:Takero Shindo, SagaUniversity School ofMedicine, 5-1-1Nabeshima, Saga 849-8501, Japan. Phone: 81-952-34-2366; Fax: 81-952-34-2017; E-mail: [email protected]
doi: 10.1158/2326-6066.CIR-15-0303
�2016 American Association for Cancer Research.
CancerImmunologyResearch
Cancer Immunol Res; 4(8) August 2016644
on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303

immunopathology by depleting eTregs and itmight suppress ATLuntil eTreg recovery.
Materials and MethodsPeripheral blood mononuclear cells (PBMC) were collected
from the patients and sorted into specific cell fractions usinga FACSAria cell sorter (Becton Dickinson). Sequencing of theTCRa/bwas performed at Repertoire Genesis Incorporation usingthe unbiased gene amplification method with Adaptor-LigationPCR (Supplementary Table S1). About 103 to 104 valid reads weregenerated (Supplementary Table S2). Bioinformatics analysis wasthen performed using the repertoire analysis software, RepertoireGenesis (RG), provided by Repertoire Genesis Incorporation. RGassigns TRV and TRJ alleles to queries and then generates CDR3sequences,finally aggregating their combination patterns.Out-of-frame sequences were excluded from the analyses. The details ofthese analyses have beendescribed previously (16). All the studiesusing patient samples were performed in accordance with theguidelines set out in the Declaration of Helsinki and wereapproved by the Institutional Review Board.
Case Presentations and ResultsCase 1
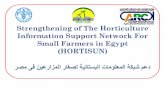
A 77-year-old man with acute ATL received mogamulizumab.Although ATL cells immediately disappeared from the peripheralblood, he developed severe skin eruptions that required long-termcorticosteroid therapy. Histopathologic examination of the skinlesions revealed a marked dermal cellular infiltrate comprisingmainly CD8þ T-cell–dominant lymphocytes and some eosino-phils, without ATL cells (Supplementary Fig. S1A–S1K). A smallpercentage of CD3dimCD4þCADM1þCD7� cells (P3 cells) stillremained in the peripheral blood on day 234 after the patientstarted mogamulizumab (Fig. 1A). TCRa repertoire analyses ofthe sorted cells revealed that these cellswere exclusively clonalATLcells: clone 1, TRAV9-2/J31, with CDR3 sequence CAPKN-NARLMF; and clone 2, TRAV13-1/J4, with CDR3 sequenceCAAIPWGYNKLIF (Fig. 1A). While the skin eruption was active,CD3þCD4þCD45RA–Foxp3þþ eTregs almost disappeared (Fig.1B and C: day 213). When the eTregs recovered, the ATL cellpopulation (CD4þCADM1þCD7– cells) gradually increased (Fig.1B: days 282 and 325). The severity of the skin eruption wasclosely associated with the percentage of eTregs (Fig. 1C). Theeruptionwasmild on day 192 (%eTreg 2.12%) but became severeon day 213 (%eTreg 0.55) before resolving on day 282 (%eTreg5.93). Notably, the percentage of ATL cells spontaneously fluc-tuated from day 325 through day 438, which might reflecttransient anti-ATL immunity. However, the patient's ATL clini-cally relapsed as multiple mediastinal lymphadenopathy, whichrequired further treatment on day 430. This time, mogamulizu-mab had little effect. Following several courses of cytotoxicchemotherapy, the patient died on day 644. Simultaneous stain-ing for Foxp3 and CADM1 revealed that the Foxp3þ cell popu-lation contained both CADM1-positive and -negative cells, withthe former gradually becoming predominant during relapse (Fig.1D). TCRa/b and CDR3 sequencing of CADM1-positive and-negative CD3þCD4þCD25þþ cells collected on day 417 revealedthat CADM1-positive cells exclusively contained one of the twoATL clones (Fig. 1A and E). Although CADM1-negative cells werepredominantly TRAV9-22/J22 (Fig. 1E), they had diverse CDR3sequences (Fig. 1E) and TRBV/J patterns (Fig. 1F), meaning that
they were not clonal. These results show that, even among cellswith the Treg phenotype, ATL and non-ATL cells can be distin-guished according to CADM1 expression.
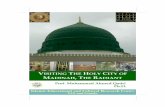
Case 2A 66-year-old man with acute ATL received mogamulizumab.
Despite the rapid disappearance of the ATL cells from the periph-eral blood, he developed a severe skin rash on the trunk (Fig. 2A).Skin biopsy and immunohistochemical staining revealed bothCD4 andCD8 T-cell infiltration of the dermal layer, but no ATL orFoxp3þ cells were detected (Supplementary Fig. S2A–S2F). At thattime, Foxp3þ Tregs (especially CD3þCD4þCD45RA–Foxp3þþ
eTregs) were depleted in the peripheral blood (Fig. 2C: days121 and 149 after mogamulizumab administration).
The patient also developed neurologic symptoms, includingptosis, diplopia, and hearing loss. MRI of the brain on day 149revealed a high-intensity area in the brainstem on diffusion-weighted images and fluid attenuated inversion recoveryimages (FLAIR; Fig. 2B: day 149). Tests of the cerebrospinalfluid revealed a mild increase in protein levels (62 mg/dL), butan absence of ATL cells. Anti-ganglioside GM2 IgM was detectedin the serum, and intrathecal administration of methotrexateand cytarabine did not improve the neurologic symptoms;therefore, the patient was diagnosed with autoimmune brain-stem encephalitis. After steroid pulse and high-dose immuno-globulin therapy followed by prednisolone administration, theneurologic symptoms completely resolved and the high-inten-sity area on brain MRI disappeared (Fig. 2B: day 219).
Two months later, the patient developed progressive drowsi-ness. Brain MRI revealed a broad high-intensity area in the rightfrontal and temporal lobes on FLAIR; no abnormal signals weredetected in the brainstem (Fig. 2B: day 270). Steroid pulse andhigh-dose immunoglobulin therapy did not improve the symp-toms, and biopsy of the frontal lobe revealed diffuse infiltrationby atypical CD3þCD4þCD25þ lymphocytes (Supplementary Fig.S2G–S2L) with monoclonal integration of HTLV-1; therefore, adiagnosis of ATL with central nervous system involvement wasmade. Notably, eTregs in the peripheral blood had recovered atthat time (Fig. 2C: day 275) and Foxp3þ cellswere focally detectedin the brain (Supplementary Fig. S2M). The CD4þFoxp3þ T cellsin peripheral blood were negative for CADM1 (Fig. 2C: day 275),indicating that they were not ATL cells, but naturally occurringTregs. High-dose methotrexate/cytarabine and mogamulizumabameliorated the symptoms, andboth the abnormality detectedonMRI and the CD4þCD45RA�Foxp3þþ cells in the peripheralblood rapidly disappeared (Fig. 2C: day 310). At the time of thestudy, the patient showed no signs of ATL relapse.
DiscussionBased on our sequencing and phenotypic analyses of these two
patients over time, we can come to some conclusions about theoverlap and differences between ATL cells with the Treg pheno-type and non-leukemia "true" eTregs. As these two populationsshare the same phenotype of CD3þCD4þCD25þFoxp3þ, it isactually difficult to discriminate between them. Given that ATLcells share the clonal TCR rearrangements, deep sequencinganalysis of TCRa/b chains and CDR3 diversity confirmed that theCD3þCD4þCADM1þCD7– cells were exclusively ATL cells.Among cells with the Treg phenotype, only the CADM1þ cellsshared the same clonality as ATL cells. The data suggest that ATL
Effector Regulatory T Cells in ATL
www.aacrjournals.org Cancer Immunol Res; 4(8) August 2016 645
on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303

cells with the Treg phenotype have a different cellular origin fromthat of naturally occurring Tregs, and that transition between thetwo subsets is unlikely. CADM1-negativeCD3þCD4þCD25þ cells
appeared clonal in terms of Va and Ja chain combinations(TRAV9-2/J22; Fig. 1E), but not in terms of the b chain (Fig.1F); the meaning of this observation remains unclear.
Figure 1.
Clinical course of case 1. A, TCRa V and J assignment and sequencing of the CDR3 region from whole PBMCs on day 234 after the start of mogamulizumab therapy(top row) and sorted cells based on high-resolution flow cytometry (bottom row). CADM1–CD7þ cells (P1: 64.9%), CADM1dimCD7þ cells (P2: 6.0%), CADM1þCD7– cells(P3 3.9%), and CADM1dimCD7� cells (P4 6.2%) were sorted from the total CD4þ T-cell population before analysis. Regarding TCR repertoire analysis, the upper 3Dgraphs show TRAV/J clones according to their percentage, and the lower tables show the ten major clones in each cell population. The two columnsand bars highlighted in yellow (TRAV9-2/J31) and brown (TRAV13-1/J4) indicate ATL clones. B, high-resolution flow cytometric detection of eTregs (top row:CD45RA�Foxp3þþ) and ATL cells (middle and bottom rows: CD3dimCADM1þCD7–) among the CD4þ T-cell population in peripheral blood. Numbers representthe percentage of eTreg cells (top row), CD4þ T cells (middle row), and CADM1þCD7� cells (bottom row). C, time course of skin eruptions. D, flow cytometricanalysis of CADM1-positive and -negative cells within the CD3þCD4þFoxp3þ cell population. E and F, TCRa/b V and J assignment and sequencing of theCDR3 region in sorted CADM1-positive and -negative cells with the Treg phenotype (CD3þCD4þCD25þ). Days are counted from start of mogamulizumab treatment.
Ureshino et al.
Cancer Immunol Res; 4(8) August 2016 Cancer Immunology Research646
on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303

Figure 2.
Clinical course of case 2.A, sequential emergence of symptoms followed by improvement: ptosis, diplopia, hearing loss, skin rash, and drowsiness. Administration oftherapeutic reagents is also shown: mogamulizumab (Moga), prednisolone (PSL), methylprednisolone (mPSL), intravenous immunoglobulin (IVIG), andmethotrexate/cytarabine (MTX/AraC). B, representative MRI of the brain. Diffusion-weighted images (DWI) are shown in the top row, and FLAIR images in thebottom row. The high-intensity area in the right frontal lobe on the day 314 DW image indicates hematoma after the biopsy. C, the expression of CD45RA, Foxp3,CADM1, and CD7 by peripheral blood CD3þCD4þ T cells was repeatedly analyzed by flow cytometry. In the top row, the numbers indicate the percentage ofCD45RA�Foxp3þþ cells (eTregs). In the bottom row, CD7�CADM1þ cells represent ATL cells. Days are counted from start of mogamulizumab treatment.
Effector Regulatory T Cells in ATL
www.aacrjournals.org Cancer Immunol Res; 4(8) August 2016 647
on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303

The frequency of eTregs was closely associated with adverseevents and ATL relapses. Depletion of eTregs was coincident withsevere skin rash and autoimmune brainstem encephalitis, suggest-ing that depletion of eTregs causes severe autoimmunity. On theother hand, eTregs recovery was coincident with ATL relapse. Inaddition, at the time case 1 relapsed, CADM1–Foxp3þ cells (nat-urally occurring Tregs) reappeared first, followed by the re-appear-ance of CADM1þFoxp3þ cells (ATL cells), which then graduallybecamedominant (Fig. 1D). These observations raise a hypothesisthat mogamulizumab suppresses ATL until eTreg recovery, whichweakens anti-ATL immunity and results in relapse of ATL.
Treg deficiency induces a severe autoimmune pathology calledIPEX (immune dysregulation, polyendocrinopathy, enteropathy,and X-linked) syndrome (17, 18), whereas abundant Tregs intumor tissues are associated with a poor prognosis (19, 20);however, it is unclear whether the percentage of Tregs in theperipheral blood has an inverse impact on immunopathology(21–23). This may be because the Foxp3þ cell population con-tains some non-Treg cells (CD45RA�Foxp3dim cells) that do nothave suppressive activity (2). We found that the depletion andrecovery of eTregs in the peripheral blood, but not that of thewhole Treg population, were coincident with adverse events andATL relapse, respectively.
In conclusion, the eTreg population reflects the equilibriumbetween antitumor immunity and autoimmunity. Currently,many monoclonal antibodies that increase antitumor immunity(including immune checkpoint blockers) are approved for clinicaluse (24). Although these reagents enable deep suppression ofTregs or enhancement of antitumor immunity, they may increasethe risk of severe autoimmune disease. To optimize the effects(and avoid serious adverse events) of the currently availablemonoclonal antibodies thatmodulate antitumor immunity, close
observation and analyses of the correlation between eTreg num-bers, antitumor immunity, and autoimmunity are warranted.
Disclosure of Potential Conflicts of InterestS. Kimura reports receiving honoraria for service on the speakers bureau for
Bristol-Myers Squibb. No potential conflicts of interest were disclosed by theother authors.
Authors' ContributionsConception and design: T. Shindo, S. KimuraDevelopment of methodology: H. Nishikawa, N. Watanabe, R. Suzuki,S. SakaguchiAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): H. Ureshino, T. Shindo, H. Nishikawa, E. Watanabe,N. Satoh, K. Kitaura,H. Kitamura, K.Doi, K.Nagase,M. Samukawa, S. Kusunoki,M. Miyahara, R. SuzukiAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): T. Shindo, H. Nishikawa, N. Watanabe, K. Nagase,T. Shin-IWriting, review, and/or revision of the manuscript: H. Ureshino, T. Shindo,M. Samukawa, S. Kusunoki, S. KimuraAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): E. Watanabe, N. SatohStudy supervision: S. SakaguchiOther (patient treatment): K. Nagase
AcknowledgmentsThe authors thank Dr. Ayumi Uchibori (Kyorin University) for analysis of
paraneoplastic neurological syndrome–related antibodies.The costs of publication of this articlewere defrayed inpart by the payment of
page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received December 10, 2015; revised March 24, 2016; accepted April 19,2016; published OnlineFirst May 23, 2016.
References1. Nishikawa H, Sakaguchi S. Regulatory T cells in cancer immunotherapy.
Curr Opin Immunol 2014;27:1–7.2. Miyara M, Yoshioka Y, Kitoh A, Shima T, Wing K, Niwa A, et al.
Functional delineation and differentiation dynamics of human CD4þT cells expressing the FoxP3 transcription factor. Immunity 2009;30:899–911.
3. SugiyamaD,NishikawaH,Maeda Y,NishiokaM, Tanemura A, Katayama I,et al. Anti-CCR4 mAb selectively depletes effector-type FoxP3þCD4þregulatory T cells, evoking antitumor immune responses in humans. ProcNatl Acad Sci U S A 2013;110:17945–50.
4. Tsukasaki K, Hermine O, Bazarbachi A, Ratner L, Ramos JC, HarringtonWJr, et al. Definition, prognostic factors, treatment, and response criteria ofadult T-cell leukemia-lymphoma: A proposal from an international con-sensus meeting. J Clin Oncol 2009;27:453–9.
5. Uchiyama T, Yodoi J, Sagawa K, Takatsuki K, Uchino H. Adult T-cellleukemia: Clinical and hematologic features of 16 cases. Blood 1977;50:481–92.
6. Ishida T, Utsunomiya A, Iida S, Inagaki H, Takatsuka Y, Kusumoto S, et al.Clinical significance of CCR4 expression in adult T-cell leukemia/lympho-ma: Its close association with skin involvement and unfavorable outcome.Clin Cancer Res 2003;9:3625–34.
7. Yoshie O, Fujisawa R, Nakayama T, Harasawa H, Tago H, Izawa D,et al. Frequent expression of CCR4 in adult T-cell leukemia andhuman T-cell leukemia virus type 1-transformed T cells. Blood 2002;99:1505–11.
8. Matsubara Y, Hori T, Morita R, Sakaguchi S, Uchiyama T. Delineation ofimmunoregulatory properties of adult T-cell leukemia cells. Int J Hematol2006;84:63–9.
9. Shimauchi T, Kabashima K, Tokura Y. Adult T-cell leukemia/lymphomacells from blood and skin tumors express cytotoxic T lymphocyte-associ-
ated antigen-4 and Foxp3 but lack suppressor activity toward autologousCD8þ T cells. Cancer Sci 2008;99:98–106.
10. Kobayashi S, Nakano K, Watanabe E, Ishigaki T, Ohno N, Yuji K, et al.CADM1 expression and stepwise downregulation of CD7 are closelyassociated with clonal expansion of HTLV-I-infected cells in adult t-cellleukemia/lymphoma. Clin Cancer Res 2014;20:2851–61.
11. Kobayashi S, Watanabe E, Ishigaki T, Ohno N, Yuji K, Nakano K, et al.Advanced human T-cell leukemia virus type 1 carriers and early-stage indolent adult T-cell leukemia-lymphoma are indistinguishablebased on CADM1 positivity in flow cytometry. Cancer Sci 2015;106:598–603.
12. Ishida T, Joh T, Uike N, Yamamoto K, Utsunomiya A, Yoshida S, et al.Defucosylated anti-CCR4 monoclonal antibody (KW-0761) for relapsedadult T-cell leukemia-lymphoma: A multicenter phase II study. J ClinOncol 2012;30:837–42.
13. Ogura M, Ishida T, Hatake K, Taniwaki M, Ando K, Tobinai K, et al.Multicenter phase II study of mogamulizumab (KW-0761), a defucosy-lated anti-cc chemokine receptor 4 antibody, in patients with relapsedperipheral T-cell lymphoma and cutaneous T-cell lymphoma. J Clin Oncol2014;32:1157–63.
14. Ishida T, Ito A, Sato F, Kusumoto S, Iida S, Inagaki H, et al. Stevens-JohnsonSyndrome associated with mogamulizumab treatment of adult T-cellleukemia/lymphoma. Cancer Sci 2013;104:647–50.
15. Yoshie O,Matsushima K. CCR4 and its ligands: from bench to bedside. IntImmunol 2015;27:11–20.
16. Kitaura K, Fujii Y, Hayasaka D, Matsutani T, Shirai K, Nagata N, et al. Highclonality of virus-specific T lymphocytes defined by TCRusage in the brainsof mice infected with West Nile virus. J Immunol 2011;187:3919–30.
17. Chatila TA, Blaeser F, Ho N, Lederman HM, Voulgaropoulos C, Helms C,et al. JM2, encoding a fork head-related protein, is mutated in X-linked
Cancer Immunol Res; 4(8) August 2016 Cancer Immunology Research648
Ureshino et al.
on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303

autoimmunity-allergic disregulation syndrome. J Clin Invest 2000;106:R75–81.
18. Hori S,Nomura T, Sakaguchi S.Control of regulatory T cell developmentbythe transcription factor Foxp3. Science 2003;299:1057–61.
19. Curiel TJ, Coukos G, Zou L, Alvarez X, Cheng P, Mottram P, et al.Specific recruitment of regulatory T cells in ovarian carcinoma fostersimmune privilege and predicts reduced survival. Nat Med 2004;10:942–9.
20. Ishida T, Ishii T, Inagaki A, Yano H, Komatsu H, Iida S, et al. Specificrecruitment of CC chemokine receptor 4-positive regulatory T cells inHodgkin lymphoma fosters immune privilege. Cancer Res 2006;66:5716–22.
21. Arimoto K, Kadowaki N, Ishikawa T, Ichinohe T, Uchiyama T. FOXP3expression in peripheral blood rapidly recovers and lacks correlation with
the occurrence of graft-versus-host disease after allogeneic stem cell trans-plantation. Int J Hematol 2007;85:154–62.
22. Clark FJ, Gregg R, Piper K, Dunnion D, Freeman L, Griffiths M, et al.Chronic graft-versus-host disease is associated with increased numbersof peripheral blood CD4þCD25high regulatory T cells. Blood2004;103:2410–6.
23. Zorn E, Kim HT, Lee SJ, Floyd BH, Litsa D, Arumugarajah S, et al.Reduced frequency of FOXP3þ CD4þCD25þ regulatory T cells inpatients with chronic graft-versus-host disease. Blood 2005;106:2903–11.
24. Topalian SL, Sznol M, McDermott DF, Kluger HM, Carvajal RD, SharfmanWH, et al. Survival, durable tumor remission, and long-term safety inpatients with advanced melanoma receiving nivolumab. J Clin Oncol2014;32:1020–30.
www.aacrjournals.org Cancer Immunol Res; 4(8) August 2016 649
Effector Regulatory T Cells in ATL
on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303

2016;4:644-649. Published OnlineFirst May 23, 2016.Cancer Immunol Res Hiroshi Ureshino, Takero Shindo, Hiroyoshi Nishikawa, et al. Antitumor Immunity and Autoimmunity in Adult T-cell LeukemiaEffector Regulatory T Cells Reflect the Equilibrium between
Updated version
10.1158/2326-6066.CIR-15-0303doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerimmunolres.aacrjournals.org/content/suppl/2016/05/19/2326-6066.CIR-15-0303.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/4/8/644.full#ref-list-1
This article cites 24 articles, 14 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/4/8/644To request permission to re-use all or part of this article, use this link
on April 10, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/2326-6066.CIR-15-0303