
人類乳突病毒 HPV疫苗 臺南市政府衛生局合約醫療 …ED46D13B-4DA1...人類乳突病毒 HPV疫苗 臺南市政府衛生局合約醫療院所申請表 醫療院所名稱:
109
中華民國 103 年 6 月第二十四卷第三期
前 言
14.4~21.3
2,482~6,078
[1]
[2]
85,000
20
200 [3]
醫療人員手部衛生知識、態度及行為調查
臺中榮民總醫院 感染管制中心
2011 10 12
500 405 81%
10
15
88%
5 15
Pearson’s
感控雜誌 2014:24:109-121
關鍵詞:
102 4 26 102 6 15 103 4 10
1650(04) 23592525 6090

110 手部衛生知識、態度及行為調查
感染控制雜誌
[4] Pittet
12%
(
)
88%
[5]
38.7% [4]
2009
Save Lives Clean Your Hands (
)
[4]
2010 5 4
325
100 12
Hayden
[6]
5
[7]
材料及方法
2011 10 12
[8,9]
5
(Content Validity Index, CVI)
1
2
3
4
5
111陳瀅淳、施智源、傅任云婕等
中華民國 103 年 6 月第二十四卷第三期
3
3
0.8
26
KR-
20 (Kuder-Richardson-20)
Cronbach’s alpha ( )
KR-20
Cronbach’s alpha ( ) 0.7
一、醫療人員基本資料
1
二、手部衛生知識量表
26
2
2 4
7
11 1
CVI
0.98 KR-20 0.71
三、手部衛生態度量表
12 2 7 10
11 12 Likert 1~5
1 2 3
4 5
CVI 1 Cronbach’s
0.88
四、手部衛生行為量表
9
0~100%
5 2
CVI 0.96 Cronbach’s
0.91
SPSS 10.0
Mann-Whitney U test Kruskal-
Wallis test
Mann-Whitney U test
Pearson’s
結 果
500
112 手部衛生知識、態度及行為調查
感染控制雜誌
409
405
81%
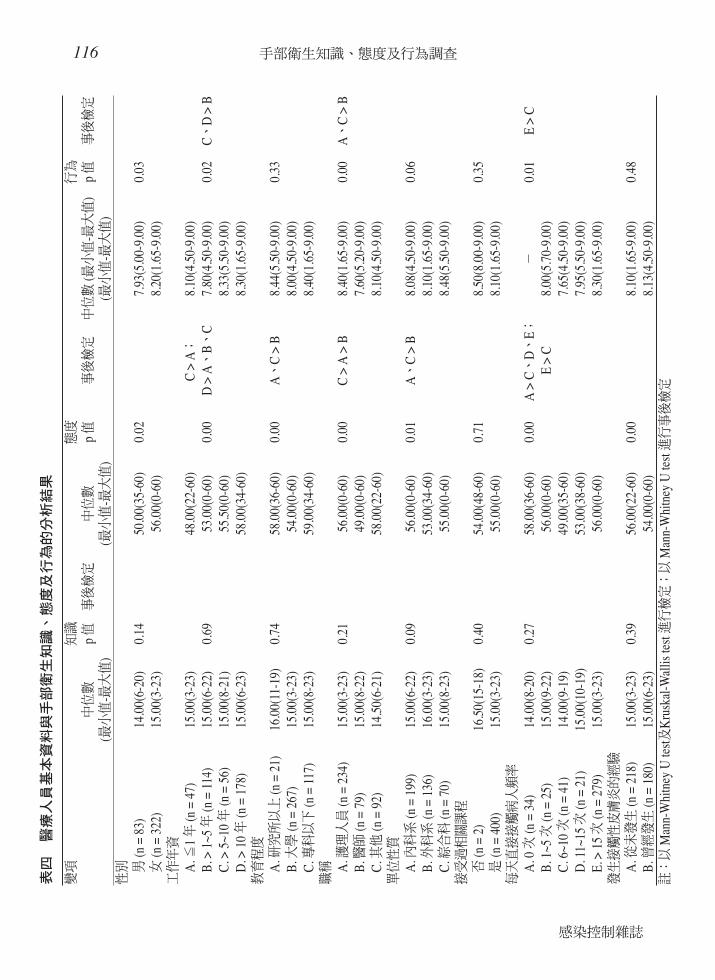
一、醫療人員基本資料
405
322 (79.5%) >
10 174 (43.0%)
> 1~5 109 (26.9%)
267
(65.9%) 117
(28.9%)
234 (57.8%) 79
(19.5%)
92
(22.7%)
400 (98.8%)
> 15 279
(68.9%) 34
(8.4%)
180 (44.4%)
二、醫療人員手部衛生知識現況
14.8 1~26
( )
三、醫療人員手部衛生態度現況
51.9 12~60
( )
四、醫療人員手部衛生行為現況
7.9 1.07~9
80% ( )
五、醫療人員基本資料與手部衛生知
識、態度及行為的變異數分析
10
10 ( )
5 10
1
113陳瀅淳、施智源、傅任云婕等
中華民國 103 年 6 月第二十四卷第三期
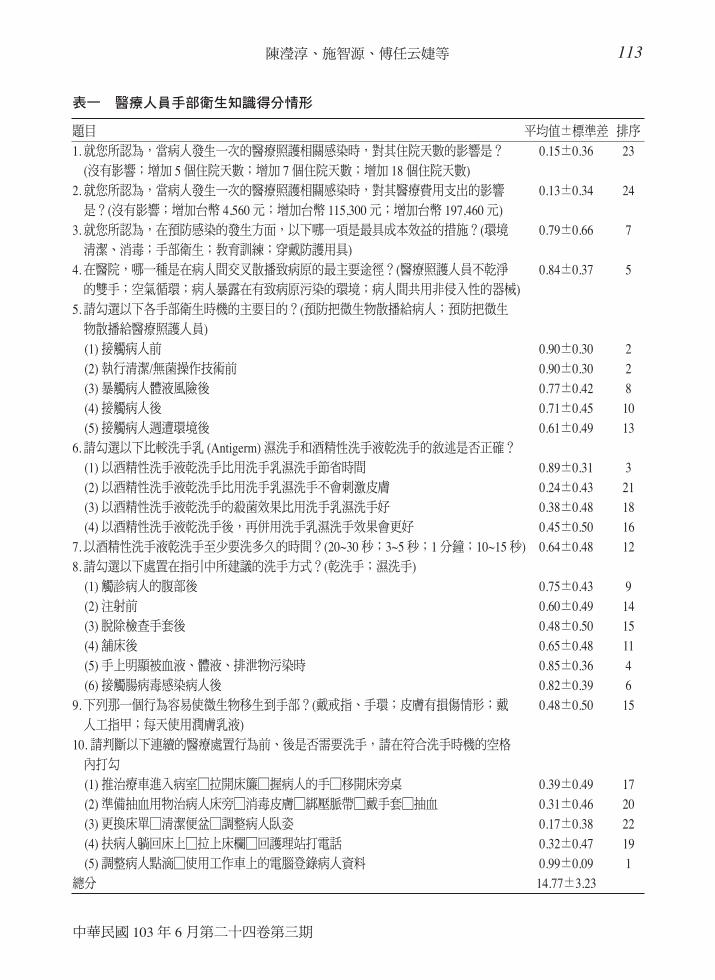
表一 醫療人員手部衛生知識得分情形
題目 平均值±標準差 排序
1. 就您所認為,當病人發生一次的醫療照護相關感染時,對其住院天數的影響是? 0.15±0.36 23
(沒有影響;增加 5 個住院天數;增加 7 個住院天數;增加 18 個住院天數)
2. 就您所認為,當病人發生一次的醫療照護相關感染時,對其醫療費用支出的影響 0.13±0.34 24
是?(沒有影響;增加台幣 4,560 元;增加台幣 115,300 元;增加台幣 197,460 元)
3. 就您所認為,在預防感染的發生方面,以下哪一項是最具成本效益的措施?(環境 0.79±0.66 7
清潔、消毒;手部衛生;教育訓練;穿戴防護用具)
4. 在醫院,哪一種是在病人間交叉散播致病原的最主要途徑?(醫療照護人員不乾淨 0.84±0.37 5
的雙手;空氣循環;病人暴露在有致病原污染的環境;病人間共用非侵入性的器械)
5. 請勾選以下各手部衛生時機的主要目的?(預防把微生物散播給病人;預防把微生
物散播給醫療照護人員)
(1) 接觸病人前 0.90±0.30 2
(2) 執行清潔/無菌操作技術前 0.90±0.30 2
(3) 暴觸病人體液風險後 0.77±0.42 8
(4) 接觸病人後 0.71±0.45 10
(5) 接觸病人週遭環境後 0.61±0.49 13
6. 請勾選以下比較洗手乳 (Antigerm) 濕洗手和酒精性洗手液乾洗手的敘述是否正確?
(1) 以酒精性洗手液乾洗手比用洗手乳濕洗手節省時間 0.89±0.31 3
(2) 以酒精性洗手液乾洗手比用洗手乳濕洗手不會刺激皮膚 0.24±0.43 21
(3) 以酒精性洗手液乾洗手的殺菌效果比用洗手乳濕洗手好 0.38±0.48 18
(4) 以酒精性洗手液乾洗手後,再併用洗手乳濕洗手效果會更好 0.45±0.50 16
7. 以酒精性洗手液乾洗手至少要洗多久的時間?(20~30 秒;3~5 秒;1 分鐘;10~15 秒) 0.64±0.48 12
8. 請勾選以下處置在指引中所建議的洗手方式?(乾洗手;濕洗手)
(1) 觸診病人的腹部後 0.75±0.43 9
(2) 注射前 0.60±0.49 14
(3) 脫除檢查手套後 0.48±0.50 15
(4) 舖床後 0.65±0.48 11
(5) 手上明顯被血液、體液、排泄物污染時 0.85±0.36 4
(6) 接觸腸病毒感染病人後 0.82±0.39 6
9. 下列那一個行為容易使微生物移生到手部?(戴戒指、手環;皮膚有損傷情形;戴 0.48±0.50 15
人工指甲;每天使用潤膚乳液)
10. 請判斷以下連續的醫療處置行為前、後是否需要洗手,請在符合洗手時機的空格
內打勾
(1) 推治療車進入病室□拉開床簾□握病人的手□移開床旁桌 0.39±0.49 17
(2) 準備抽血用物治病人床旁□消毒皮膚□綁壓脈帶□戴手套□抽血 0.31±0.46 20
(3) 更換床單□清潔便盆□調整病人臥姿 0.17±0.38 22
(4) 扶病人躺回床上□拉上床欄□回護理站打電話 0.32±0.47 19
(5) 調整病人點滴□使用工作車上的電腦登錄病人資料 0.99±0.09 1
總分 14.77±3.23
114 手部衛生知識、態度及行為調查
感染控制雜誌
6
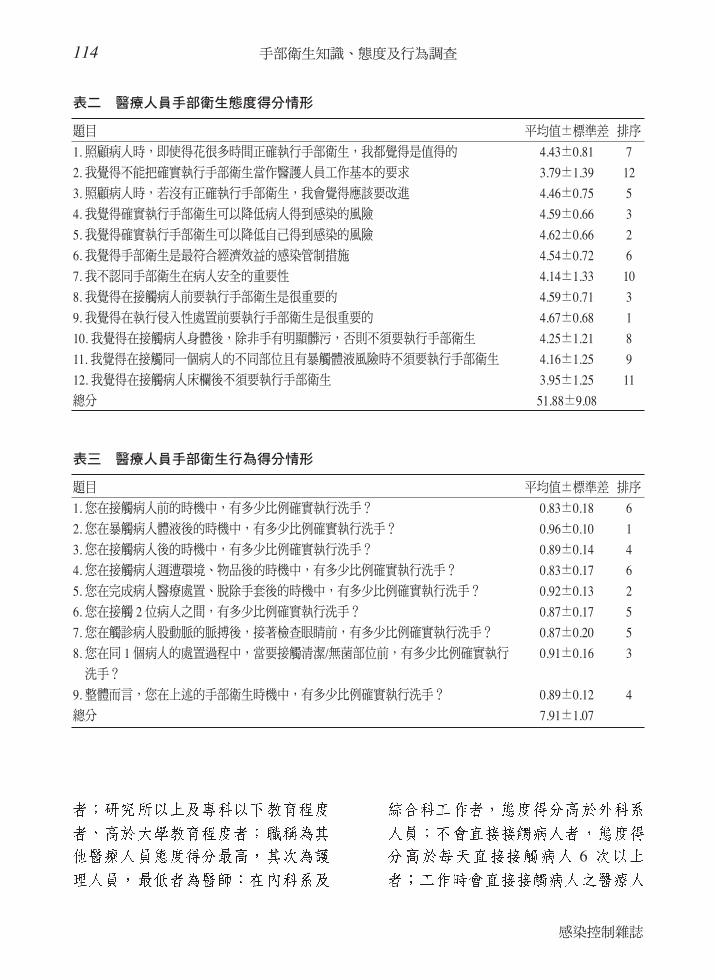
表二 醫療人員手部衛生態度得分情形
題目 平均值±標準差 排序
1. 照顧病人時,即使得花很多時間正確執行手部衛生,我都覺得是值得的 4.43±0.81 7
2. 我覺得不能把確實執行手部衛生當作醫護人員工作基本的要求 3.79±1.39 12
3. 照顧病人時,若沒有正確執行手部衛生,我會覺得應該要改進 4.46±0.75 5
4. 我覺得確實執行手部衛生可以降低病人得到感染的風險 4.59±0.66 3
5. 我覺得確實執行手部衛生可以降低自己得到感染的風險 4.62±0.66 2
6. 我覺得手部衛生是最符合經濟效益的感染管制措施 4.54±0.72 6
7. 我不認同手部衛生在病人安全的重要性 4.14±1.33 10
8. 我覺得在接觸病人前要執行手部衛生是很重要的 4.59±0.71 3
9. 我覺得在執行侵入性處置前要執行手部衛生是很重要的 4.67±0.68 1
10. 我覺得在接觸病人身體後,除非手有明顯髒污,否則不須要執行手部衛生 4.25±1.21 8
11. 我覺得在接觸同一個病人的不同部位且有暴觸體液風險時不須要執行手部衛生 4.16±1.25 9
12. 我覺得在接觸病人床欄後不須要執行手部衛生 3.95±1.25 11
總分 51.88±9.08
表三 醫療人員手部衛生行為得分情形
題目 平均值±標準差 排序
1. 您在接觸病人前的時機中,有多少比例確實執行洗手? 0.83±0.18 6
2. 您在暴觸病人體液後的時機中,有多少比例確實執行洗手? 0.96±0.10 1
3. 您在接觸病人後的時機中,有多少比例確實執行洗手? 0.89±0.14 4
4. 您在接觸病人週遭環境、物品後的時機中,有多少比例確實執行洗手? 0.83±0.17 6
5. 您在完成病人醫療處置、脫除手套後的時機中,有多少比例確實執行洗手? 0.92±0.13 2
6. 您在接觸 2 位病人之間,有多少比例確實執行洗手? 0.87±0.17 5
7. 您在觸診病人股動脈的脈搏後,接著檢查眼睛前,有多少比例確實執行洗手? 0.87±0.20 5
8. 您在同 1 個病人的處置過程中,當要接觸清潔/無菌部位前,有多少比例確實執行 0.91±0.16 3
洗手?
9. 整體而言,您在上述的手部衛生時機中,有多少比例確實執行洗手? 0.89±0.12 4
總分 7.91±1.07
115陳瀅淳、施智源、傅任云婕等
中華民國 103 年 6 月第二十四卷第三期
15
6~10
5
1
5
15
6~10 ( )
六、醫療人員手部衛生的知識、態度
與行為之相關性
Pearson’s
( = 0.18 p <
0.05) ( = 0.27
p < 0.05) (
0.3 )
( = 0.01 p
> 0.05)
( )
討 論
98.8%
57%
1~4
51.9
116 手部衛生知識、態度及行為調查
感染控制雜誌
表四
醫
療人
員基
本資
料與
手部
衛生
知識
、態
度及
行為
的分
析結
果
變項
知識
態度
行為
中位
數p
值事
後檢
定中
位數
p 值
事後
檢定
中位
數(最
小值
-最大
值)
p 值
事後
檢定
(最小
值-最
大值
)(最
小值
-最大
值)
(最小
值-最
大值
)性
別 男(n
= 8
3)14
.00(
6-20
)0.
1450
.00(
35-6
0)0.
027.
93(5
.00-
9.00
)0.
03女
(n =
322
)15
.00(
3-23
)56
.00(
0-60
)8.
20(1
.65-
9.00
)工
作年
資A
. ≦1
年(n
= 4
7)15
.00(
3-23
)48
.00(
22-6
0)C
> A
;8.
10(4
.50-
9.00
)B
. > 1
~5 年
(n =
114
)15
.00(
6-22
)0.
6953
.00(
0-60
)0.
00D
> A
、B
、C
7.80
(4.5
0-9.
00)
0.02
C、
D >
BC
. > 5
~10
年(n
= 5
6)15
.00(
8-21
)55
.50(
0-60
)8.
33(5
.50-
9.00
)D
. > 1
0 年
(n =
178
)15
.00(
6-23
)58
.00(
34-6
0)8.
30(1
.65-
9.00
)教
育程
度A
. 研究
所以
上(n
= 2
1)16
.00(
11-1
9)0.
7458
.00(
36-6
0)0.
00A
、C
> B
8.44
(5.5
0-9.
00)
0.33
B. 大
學(n
= 2
67)
15.0
0(3-
23)
54.0
0(0-
60)
8.00
(4.5
0-9.
00)
C. 專
科以
下(n
= 1
17)
15.0
0(8-
23)
59.0
0(34
-60)
8.40
(1.6
5-9.
00)
職稱 A
. 護理
人員
(n =
234
)15
.00(
3-23
)0.
2156
.00(
0-60
)0.
00C
> A
> B
8.40
(1.6
5-9.
00)
0.00
A、
C >
BB
. 醫師
(n =
79)
15.0
0(8-
22)
49.0
0(0-
60)
7.60
(5.2
0-9.
00)
C. 其
他(n
= 9
2)14
.50(
6-21
)58
.00(
22-6
0)8.
10(4
.50-
9.00
)單
位性
質A
. 內科
系(n
= 1
99)
15.0
0(6-
22)
0.09
56.0
0(0-
60)
0.01
A、
C >
B8.
08(4
.50-
9.00
)0.
06B
. 外科
系(n
= 1
36)
16.0
0(3-
23)
53.0
0(34
-60)
8.10
(1.6
5-9.
00)
C. 綜
合科
(n =
70)
15.0
0(8-
23)
55.0
0(0-
60)
8.48
(5.5
0-9.
00)
接受
過相
關課
程否
(n =
2)
16.5
0(15
-18)
0.40
54.0
0(48
-60)
0.71
8.50
(8.0
0-9.
00)
0.35
是(n
= 4
00)
15.0
0(3-
23)
55.0
0(0-
60)
8.10
(1.6
5-9.
00)
每天
直接
接觸
病人
頻率
A. 0
次(n
= 3
4)14
.00(
8-20
)0.
2758
.00(
36-6
0)0.
00A
> C
、D
、E;
-0.
01E
> C
B. 1
~5 次
(n =
25)
15.0
0(9-
22)
56.0
0(0-
60)
E >
C8.
00(5
.70-
9.00
)C
. 6~1
0 次
(n =
41)
14.0
0(9-
19)
49.0
0(35
-60)
7.65
(4.5
0-9.
00)
D. 1
1~15
次(n
= 2
1)15
.00(
10-1
9)53
.00(
38-6
0)7.
95(5
.50-
9.00
)E.
> 1
5 次
(n =
279
)15
.00(
3-23
)56
.00(
0-60
)8.
30(1
.65-
9.00
)發
生接
觸性
皮膚
炎的
經驗
A. 從
未發
生(n
= 2
18)
15.0
0(3-
23)
0.39
56.0
0(22
-60)
0.00
8.10
(1.6
5-9.
00)
0.48
B. 曾
經發
生(n
= 1
80)
15.0
0(6-
23)
54.0
0(0-
60)
8.13
(4.5
0-9.
00)
註:
以M
ann-
Whi
tney
U te
st及
Kru
skal
-Wal
lis te
st 進
行檢
定;
以M
ann-
Whi
tney
U te
st 進
行事
後檢
定
117陳瀅淳、施智源、傅任云婕等
中華民國 103 年 6 月第二十四卷第三期
28.5%
O’Boyle
(82%)
(70%) [10]
80%
/
57~62% [10,11]
4~14%
14~60% [12,13]
[14]
88%
/
82.3%
90%
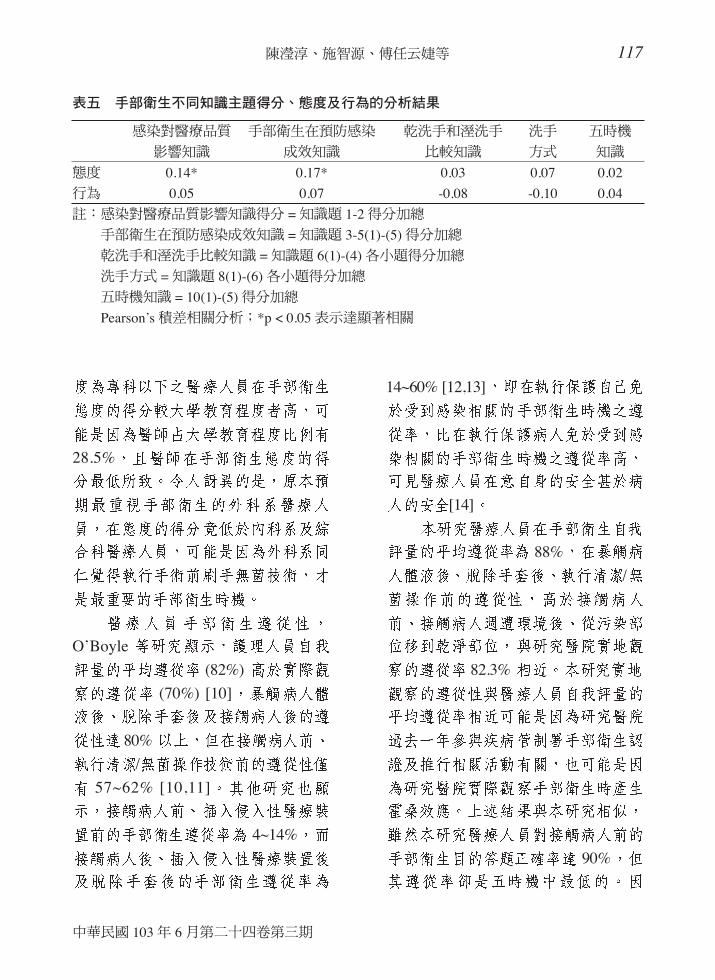
表五 手部衛生不同知識主題得分、態度及行為的分析結果
感染對醫療品質 手部衛生在預防感染 乾洗手和溼洗手 洗手 五時機
影響知識 成效知識 比較知識 方式 知識
態度 0.14* 0.17* 0.03 0.07 0.02
行為 0.05 0.07 -0.08 -0.10 0.04
註:感染對醫療品質影響知識得分 = 知識題 1-2 得分加總
手部衛生在預防感染成效知識 = 知識題 3-5(1)-(5) 得分加總
乾洗手和溼洗手比較知識 = 知識題 6(1)-(4) 各小題得分加總
洗手方式 = 知識題 8(1)-(6) 各小題得分加總
五時機知識 = 10(1)-(5) 得分加總
Pearson’s 積差相關分析;*p < 0.05 表示達顯著相關
118 手部衛生知識、態度及行為調查
感染控制雜誌
[10,14]
Tai
[11]
72%
[11]
[15-17]
[15]
(Objective Structured
Clinical Examinations, OSCEs)
[15]
Pittet
7
[18]
Buffet-Bataillon 30~40
[17] 10
15
86%
Stutz
[19]
119陳瀅淳、施智源、傅任云婕等
中華民國 103 年 6 月第二十四卷第三期
[20]
(p < 0.05)
Tai
[11]
(
)
參考文獻
1. Sheng WH, Wang JT, Lu DC, et al: Comparativeimpact of hospital-acquired infections on medicalcosts, length of hospital stay and outcomebetween community hospitals and medicalcentres. J Hosp Infec 2005;59:205-14.
2. Sheng WH, Chie WC, Chen YC, et al: Impact of
nosocomial infections on medical costs, hospitalstay, and outcome in hospitalized patients. JFormos Med Assoc 2005;104:318-26.
3. 張文瀚 (2010 年 10 月 4 日).醫院感染控制概論 . 台 灣 醫 院 感 染 管 制 學 會 網 路 . 摘 自https://www.nics.org.tw/news_upload.php?id=650-。
4. WHO (2009, January). WHO guidelines on handhygiene in health care. Available http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf.
5. Pittet D, Hugonnet S, Harbarth S, et al:Effectiveness of a hospital-wide programme toimprove compliance with hand hygiene. Lancet2000;356:1307-12.
6. Hayden MK, Bonten MJ, Blom DW, et al:Reduction in acquisition of vancomycin-resistantenterococcus after enforcement of routineenvironmental cleaning measures. Clin Infect Dis2006;42:1552-60.
7. WHO (2009, January). Guide to theimplementation of the WHO multimodal handhygiene improvement strategy. Availablehttp://www.who.int/gpsc/5may/Guide_to_Implementation.pdf.
8. WHO (2009, August). Hand hygiene knowledgequestionnaire for health-care workers. Availablehttp://www.who.int/gpsc/5may/Hand_Hygiene_Knowledge_Questionnaire.doc
9. De Wandel D, Maes L, Labeau S, et al:Behavioral determinants of hand hygienecompliance in intensive care units. Am J Crit Care2010;19:230-9.
10. O’Boyle CA, Henly SJ, Larson E: Understandingadherence to hand hygiene recommendation: thetheory of planned behavior. Am J Infect Control2001;29:352-60.
11. Tai JW, Mok ES, Ching PT, et al: Nurses andphysicians’ perceptions of the importance andimpact of healthcare-associated infections andhand hygiene: a multi-center exploratory study inHong Kong. Infection 2009;37:320-33.
12. Saba R, Inan D, Seyman D, et al: Hand hygienecompliance in a hematology unit. Acta Haematol2005;113:190-3.
13. Lankford MG, Zembower TR, Trick WE, et al:Influence of role models and hospital design onhand hygiene of healthcare workers. Emerg Infect

120 手部衛生知識、態度及行為調查
感染控制雜誌
Dis 2003;9:217-23.
14. Darawad MW, Al-Hussami M, Almhairat II, et al:Investigating Jordanian nurses’ handwashingbeliefs, attitudes, and compliance. Am J InfectControl 2012;40:643-7.
15. Jang JH, Wu S, Kirzner D, et al: Physicians andhand hygiene practice: a focus group Study. JHosp Infect 2010;76:87-9.
16. Creedon SA: Healthcare workers’ handdecontamination practices: compliance withrecommended guidelines. J Adv Nurs2005;51:208-16.
17. Buffet-Bataillon S, Leray E, Poisson M, et al:Influence of job seniority, hand hygieneeducation, and patient-to-nurse ratio on hand
disinfection compliance. J Hosp Infect2010;76:32-5.
18. Pittet D, Simon A, Hugonnet S, et al: Handhygiene among physicians: performance, beliefs,and perceptions. Ann Intern Med 2004;141:1-8.
19. Stutz N, Becker D, Jappe U, et al: Nurses’perceptions of the benefits and adverse effects ofhand disinfection: alcohol-based hand rubs vs.hygienic handwashing: a multicentrequestionnaire study with additional patch testingby the German Contact Dermatitis ResearchGroup. Br J Dermatol 2009;160:565-72.
20. 莊慧瑛,蔡鎮吉,賴重彰等:護理主管對感染管制認知、態度與行為及其相關因素探討。感控雜誌 2011;21:157-66。
121陳瀅淳、施智源、傅任云婕等
中華民國 103 年 6 月第二十四卷第三期
A Survey of Hand Hygiene Knowledge,
Attitude, and Practice among Health Care
Workers
Ying-Chun Chen, Hui-Mei Huang, Yun-Jiau Fuh Rehn, Lui-Chen Chang, Kae-Jiun Wang,
Ay-Pyng Chiou, Pei-Hsuan Huang, Meei-Fang Liu, Zhi-Yuan Shi
Department of Infection Control, Taichung Veterans General Hospital, Taichung, Taiwan
The purpose of this study was to investigate hand hygiene knowledge, attitude,practice, and related factors among health care workers. A descriptive cross-sectional and correlational study was performed at a medical center from Octoberto December 2011. In this survey, 500 health care workers were randomly selectedto participate in the study; of these, 405 (81%) completed the survey. The resultsshowed that most health care workers had insufficient hand hygiene knowledge buthad positive attitude and practice. Knowledge was not significantly affected byworker background factors. Factors that significantly affected attitude included sex,experience, level of education, profession, department, frequency of contact withpatients, and experience with dermatitis. The mean hand hygiene compliance was88% among participants. Sex, experience, profession, and frequency of patientcontact affected hand hygiene practice. Finally, positive correlations were observedbetween knowledge and attitude and between attitude and practice. Therefore, werecommend that infection control practitioners apply multi-disciplinary trainingstrategies to promote hand hygiene knowledge, practice, and attitude among healthcare workers.
Key words: Hand hygiene, knowledge, attitude, practice


















