DEMAM N RUAM.pptx
67
Exanthematous Fever Ratna MS, Irene Ratridewi Huwae 1
-
Upload
farrah-sayed -
Category
Documents
-
view
221 -
download
0
Transcript of DEMAM N RUAM.pptx
Pediatric Rash
Exanthematous FeverRatna MS, Irene Ratridewi Huwae11TerminologiMacule lesi datar, berbentuk lingkaran, perubahan warnaPapule lesi elevasi, kecil, solidNodule lesi elevasi, besar, solid, palpablePlaque lesi luas yang sedikit meningkatBlister lesi elevasi, berisi cairanUlcer lesi depressed, epitel permukaan hilangAtrophy lesi depressed, epitel permukaan intakCrust campuran sisik dan serum, dg cairan kekuningan pd permukaan lesiPetechiae lesi non raised, merah-kehitaman, non blanchable
22Microbial Diseases of the Skin
33PendekatanRiw. penyakit/ penyakit penyerta, imunisasiGx prodormalKarakteristik ruam (lokasi & penyebaran)Gx patognomonik/ ciri tertentuLab44Klasifikasi~ Gb ruam :Kelompok makulopapularKelompok papulovesikular~ Etiologi55DDx Maculopapular Rash RubellaRubeolaScarlet feverKawasaki diseaseSecondary syphilisDrug eruptionCoxsackie virusECHO virusAdenovirusInfectious mononucleosisParvovirusMeningococcemiaToxoplasmosisSerum sicknessRickettsial disease (eg, Rocky Mountain Spotted fever)Roseola66Summary of Paediatric Skin Rashes: Adapted from Paediatric Handbook 6th Ed. Royal Children's Hospital, Melbourne
77EtiologiInfeksiVirus: Classic viral exanthem: Measles, Rubella, VZV, Parvovirus, RoseolaOthers:, HSV, EBV, HBV, Enterovirus, DengueBacteria: Scarlet fever, Staph infection (sepsis, 4S,toxic shock syndrome), Meningococcemia, typhoidMycoplasmaRickettsial infectionNon InfeksiAllergy: Food, drug, toxin, serum sicknessUncertain cause: Kawasaki disease88Campak / MeaslesMeasles virus: RNA, genus Morbilivirus, family ParamyxoviridaeAirborne transmission Winter seasonOnly human reservior99Manifestasi KlinisIncubation: 8-12 hr, rata2 kontak rash 14 days, range 7-18 hr. Prodromal period: demam 2-4 hr + 3CcoughcoryzaconjunctivitisKoplik spotRash: erythematous maculopapular rashWajah seluruh tubuh dlm 72 jamWajah dan badan: >>>pneumoniaConvalescenceBatuk 1 mgg1010
1111DiagnosisDemographic dataRiw contactS/S3C, Koplik spot,Rash appears before defervescenceInvestigationCBC: lymphocyte predominationserology: CF, HI, ELISACXR: perihilar peribronchial infiltration1212KomplikasiPneumoniaOtitis mediaDiarrheaMeningoencephalitisCroupSubacute sclerosing panencephalitis (SSPE)
1313TreatmentSupportive and SymptomaticVit A supplementation6 mo-2 yr hospitalized with measles and complication> 6 mo who have risk for severe measles and vit A deficiency:immunodef, vitamin A def, impaired intestinal absorption, malnutrition, recent immigration from high mortality rated due to measlesAntibiotic for superimposed bacterial infection1414RubellaRNA virus: Family Togaviridae, genus RubivirusIP: 14-21 daysInfectivity: 7 days before 5 days after onset of rash1515Manifestasi KlinisProdromal period 1-5 daysMP rash for < 3 daysLN at postauricular and cervical areaCBC: normal rangeDx: viral isolationSerologic test: CF, HI, IgM ELISA
1616
1717RubellaComplicationarthritisthrombocytopeniameningoencephalitisTreatment: supportiveIsolation: droplet precaution for 7 days after onset of rash, contact precaution for congenital rubella until > 1 yr-oldPrevention: immunization
1818Varicella/ ChickenpoxVZV, HHV-3: Transmissionairbornecontact vesicular fluidvertical transmissionIncubation period: 14-16 days, (10-21days)Infectivity: winter seasonMost contagious: 1-2 days before onset of rash until crusting of lesion.
1919Manifestasi KlinisProdromal period: 2-3 hrGeneralized, pruritic, vesicular rash 250-500 lesions skin, oral mucosaComplicationHerpes Zoster, ShinglesCongenital varicella: Scar, limb, ocular, CNS defectBacterial infectionSevere chickenpoxCNS: encephalitis, cerebellar ataxia, Reyes Syndrome
2020
2121
2222Diagnosis & Differential DiagnosisDiagnosisS/S Tzanck smear: multinucleated giant cellDifferential DiagnosisImpetigo contagiosaEnterovirus: HFMDHSV2323TreatmentSupportive and symptomaticantipruritic drugfor severe case: ACV, famciclovir, valacyclovirIsolation: Airborne and contact isolation 1-2 days before rash until crusting of all lesion.PreventionImmunization
2424Hand-foot-mouth Diseasecoxackie virus type 16 (A 16) most common, other include A5, A7, A9, A10, B2, B5(31) and enterovirus 71Fever, sore throat, droolingDDx from Herpes gingivostomatitisSelf-limited, symptomatic treatment2525HFMD
2626
2727Roseola InfantumExanthem subitum3 mo- 3 yr. (6 mo-1 yr)HHV-6,7: DNA virus, HerpesviridaeUncertain incubation period (9-10 days)
2828Manifestasi Klinis High fever 39-41 c for 3-4 daysnonspecific symptombulging AFfebrile convulsionMP Rash after defervescenceCBC: normal range of WBC, lymphocyte predominated2929
3030TreatmentSymptomatic and supportiveIsolation: standard precautionPrevention: No vaccination
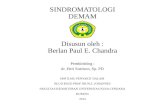
3131Erythrema infectiosum (Fifth Dz)Parvovirus (PV) B19 Family Parvoviridae 3-15 yearDroplet transmissionIncubation period: 4-14 daysS/S: lowgrade fever, constitutional symptoms, arthralgiaClassical 3 phasesSunburn-like rash both cheek (classic slapped-cheek appearance) 2-4 Day 1-4 after facial rash macular to morbiliform eruption at extremities (extensor surface) Lacy pattern: some w/o classic slapped-cheek pattern3232
3333
3434MeningococcemiaN meningitidis: GNDC, bean shapeManifestasi klinis :acute febrile illnesspetechiae, hemorrhagic manifestation: purpura fulminanrapid progressive with HT or comameningoencephalitisDiagnosis: gram stain, antigen detection, buffy coat smear and cultureTreatment: penicillin, CTX, CRO3535
3636Scarlet feverGAS or S aureusAcute febrile illness dg:Sore throatGooseflesh or coarse sand-paper rash within 12-48 jam Pressure area: axilla, groin >>>Pastias lineStrawberry tongue Pustule (Staph scarlet)Deskuamasi akhir mgg I3737
3838Scarlet fever
3939Scarlet fever
4040Scarlet fever
4141Staphylococcal scalded skin syndrome (SSSS/4S) Staphylococcus toxigenic strain phage group 2 epidemolytic toxin A and B Local inf. purulent conjunctivitis, otitis media, nasopharyngeal infectionDemam, Makulopapular rash / erythroderma, dg periorificial + flexural accentuasi dg Nikolski sign4242(if the skin is rubbed firmly, causing separation at the dermo-epidermal junction ).
4343Impetigo contagiosa
4444
DHF
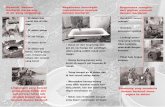
4545Rose spot in Typhoid Fever
4646Thai Tick Typhus
4747Kawasaki DiseaseFever > 5 days with 4/5 of the following criteriabilateral nonpurulent conjunctival injectionChange of mucosa of oropharynxChanges of peripheral extremitiesRashCervical adeonopathyIllness not explained by other known disease processCoronary arteritis
4848
4949
5050
5151Terima kasih5252ReferensiBarinaga, J. L., & Skolnik, P. R. (2005). Clinical presentation and diagnosis of measles, from http://uptodateonline.com.Charters, K. G. (2003). Nursing informatics, outcomes, and quality improvement. AACN Clinical Issues: Advanced Practice in Acute & Critical Care., 14(3), 282-294.Cohen, B. A., & Lehmann, C. U. (2005). Dermatlas.Org, from http://dermatlas.med.jhmi.edu/derm/.Mengert, T., Eisenberg, M. S., & Copass, M. K. (1996). Emergency medical therapy (4th ed.). Philadelphia: W.B.Saunders.
5353Measles, Treatment and CareIsolation: Airborne Precaution1-2 day before onset of symptom or 3-5 days before onset of rash4 days after onset of rash in healthy childrenFor the duration of illness in immunocompromised pt.Isolated room (negative pressure ventilation)Prevention: immunization9-15 months4-6 years
5454Measles, Treatment and CareImmunoglobulin therapy- indicationsAll susceptible contactsInfants 5 mo. To 1 year of ageImmunocompromisedPregnant women 6 month old with unimmunized/unvaccinated
All exposed susceptible immunocompetent patients should be immunized within 72 hr and should be discharged as early as possible.
All susceptible immuocompromised patients should received IG 0.5ml.kg IM within 6 days of exposure.
5656All exposed susceptible patient who cannot be discharged should be placed in airborne precaution from day 5-21 after exposure.
All susceptible exposed staff should be excused from patient contact from day 5-21 after exposure.
Personnel who become ill should be relieved from patient contact for 4 days after rash develops.
Consider booster dose of MMR in children 4-12 year who was immunized only 1 dose.
Measles, Care of exposed person5757
Measles, Care of exposed person5858Varicella, Treatment and careOral acyclovir- indicationsHealthy nonpregnant teenagers and adultsChildren > 1 yr with chronic cutaneous or pulmonary conditionsPatients on chronic salicylate therapyPatients receiving short or intermittent courses of aerosolized corticosteroidsDose: 80 mg/kg/day in four divided doses for 5 days5959Varicella, Treatment and careVZIG (1 vial/5 kg IM) :Px on high dose steroidsImmunocompromised without a history of VaricellaPregnant womenNewborns exposed 5 days prior to birth and 2 days after deliveryNeonates born to nonimmune mothersHospitalized premature infants < 28 weeks gestation6060Identify those who are susceptible: both personel and patientimmunocompromised patientimmunocompetent patient who:< 6 month old without maternal history of chickenpox> 6 month old with unimmunized/unvaccinated
All exposed susceptible patients should be discharged as soon as possible.
All susceptible patients who cannot be discharged should be placed in airborne and contact precaution from day 8-21 after exposure.Varicella, Care of expose Person:6161All susceptible exposed staff should be excused from patient contact from day 8-21 after exposure.
Varicella immunization is recommended for susceptible staff in varicella does not develop from the exposure
Postexposure Immunization: 72 (possibly up to) 120 hr after varicella exposure to prevent or significantly modify disease.
6262Varicella, Child Care and SchoolChildren may return to school when all lesion are crusted.
For compromised children with prolonged course should excluded for the duration of the vesicular eruption.
Older children and staff members with zoster should be instructed to wash their hands if they touch potentially infectious lesion6363Case definition of Invasive Meningococcal DiseaseConfirmed case: +ve culture for N meningitidis in sterile site Presumtive: +ve Gram stain of GPDC in sterile siteProbable: +ve meningococcal antigen in sterile site with compatible clinical manifestation (purpura fulminan)
Clinical manifestation of Invasive meningococcal disease: acute toxic febrile illness, stiffneck, petechiae or purpuric spot with rapidly progress to coma, seizure or hypotension
Guideline for contact case of Meningococci6464household contactdaycare center (same bedroom) within 7 days prior to diagnosisdirect contact to oropharyngeal secretion: kiss, share toothbrush or eating utensilhealthcare worker
Routine nursing care has not increase risk of transmission: PEP is not indicated.
Indication for Postexposure Prophylaxis 6565Should begin within 24 hr. after contact.
Rifampicin 10 mkdoseoral; bid x 2 day (maximum