Chirurgia d’Urgenza & Trauma Center: A Che Punto Siamo...2019/10/14 · 1 Tecnico Rian....
47
Chirurgia d’Urgenza & Trauma Center: A Che Punto Siamo ? M. Chiarugi, MD, FACS Chirurgia d’Urgenza Universitaria e Trauma Center AOUP-Pisa
Transcript of Chirurgia d’Urgenza & Trauma Center: A Che Punto Siamo...2019/10/14 · 1 Tecnico Rian....

Chirurgia d’Urgenza & Trauma Center: A Che Punto Siamo ?M. Chiarugi, MD, FACS
Chirurgia d’Urgenza Universitaria e Trauma Center AOUP-Pisa

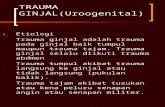
Geographic variations in
MVC-mortalityBaker et al, 1987
MVC mortality (per 100 000 persons)
2.5
558
Population density (persons/sq mile)
64000
0.2
Esmerelda, NV versus Manhattan, NY

Trauma System
◼Sistema organizzato in grado di dare unaadeguata ed efficace rispostamultidisciplinare al paziente traumatizzato:– in una area geografica definita– In grado di offrire servizi sanitari “full-range”– a tutti I pazienti traumatizzati– Integrato con sistemi pubblici di educazione, prevenzione e
sorveglianza
◼Benefits– migliora l’outcome dei traumatizzati con lesioni severe– riduce l’impatto anche economico dei decessi e disabilità per
trauma– migliora l’efficacia dei componenti del sistema (feed-back positivo)

Landmark Paper
Trauma Mortality in Orange County: The Effect of Implementation of Regional Trauma System
Cales RH. Ann Emerg Med. 1984; 13:1-10

The Goals of a Trauma System
➢ Prevent as many injuries as possible
➢ Get the severely injured patient to
the best source of care as quickly as possible
➢ Immediate response/care at the scene
➢ Rapid transport from the scene to a
qualified trauma hospital
➢ Qualified trauma hospitals capable of delivering immediate medical care and ongoing treatment for the injured


An organized Trauma System links the necessary resources to maximize patient recovery
• A trauma system includes:– EMS interventions– Emergency department
interventions– Intensive and surgical in-hospital
care– Rehabilitation– Social services– Injury prevention– Research– Education– Disaster Planning

Trauma Is Still a Surgical Illness

Trauma philosophy
o Trauma patient: the most likely patient to suffermistakeso No medical history, working against time
o The least likely patient to survive mistakeso Limited physiological reserve
o Small mistakes: heavy price
o Trauma team works /reducing in-hospital preventabledeaths
o Every minute counts!
o A trauma surgeon doesn’t walk: he/she runs!
o The more you know about trauma the more you worry!
o Never hesitate to ask for help!

The 3-D Trauma SurgeonPutting Brain in Gear before Knife in Motion
(from Hirshberg & Mattox “Top-Knife”, 2005)
o Procedures span from head to toe
o Sterility is a luxury in severe hemorrhagic shock
o Always prep for a worst-case scenario
o Know the key maneuver and pitfall in every operative step
o Avoid flailing; learn to deal with technical failure
o Simplify complex tactical situations
o Know when to bailing out
o Be able to choose a definitive repair option the fail well
o Stay well ahead of the operation
o Damage control is the great equalizer of trauma surgery


Trauma Surgery: Fatti• Interventi per lesioni regione anteriore collo, torace, addome,
grossi vasi
• Tendenza alla riduzione ferite penetranti
• Espansione dei trattamenti non chirurgici
• Radiologia interventistica e procedure endoscopiche
• Riduzione carico interventi chirurgici
• Sostenibilità economica
• Minore interesse specializzandi per trauma surgery/ trauma surgeons shortage
Chirurgia d’Urgenza Università di Pisa-AOUP

Challenges in Trauma Training
• Trauma cases per year declined from 78 in 1990 to 38 in 2010;
• Laparotomy 9.97 in 1990 to 4.85 cases/resident 2010 (Patel M, et al
J Surg Res 2012)
• 55 residency graduates: 3.4 spleen procedures, 2.4 liveroperations;
• Resuscitative thoracotomy;
• Definitive Surgical Trauma Care (DSTC);
• Advanced Trauma Operative Management (ATOM) Course;
• Adanced Surgical Skills for Exposure in Trauma (ASSET) Course
• University of Southern California (USC) Course
Chirurgia d’Urgenza Università di Pisa-AOUP

Birth & Essential Components Acute Care Surgery (ACS)
❑ Trauma surgeons shortage
❑ Increasing specialization in the field of general surgery
❑ Complexity of the critical illness affecting emergency general surgery patients
❑ American College of Surgeons and American Association for the Surgery of Trauma training programs in Acute Care Surgery
❑ ACS 2005
▪ Trauma
▪ Emergency Surgery
▪ Critical Care

Emergency General Surgery (EGS) Facts
❑11% of surgical admission;
❑50% of surgical mortality;
❑Likelihood of postoperative death 8 times more thanelective surgery;
❑50% of patients undergoing EGS will developcomplications;
❑15% will be readmitted within 30 days of theirsurgery;
❑Increasing elederly population, increasing EGS.
adapted from Scott JW et al JAMA Surgery 2016;151 (6):1-7



Respect to non –RSCL benefits for:▪ Severe sepsis / septic shock patients▪ Male patients▪ Age > 70 yrs.▪ Multiple co-morbidities▪ Acidosis and elevated lactate▪ Avoid unplanned re-explorations wich occurred in 50%
of patients with severe sepsis/septic shockwhonderwent fascia closure at primary intervention


▪ Complications of medical or surgical care more frequent diagnosisthan bowel obstruction,acute cholecystitis, and appendicitiscombined;
▪ 10% of general surgery (nontrauma) admissions/consults for surgical rescue from a major complications;
▪ On average 1 patient/day seen requiring surgical rescue;
▪ More than 80% require an operation;
▪ 50% from other in-hospital services (majority surgical), 25% from the region, 25% own service.
J Trauma Acute Care Surg 2015;79(2):327

Evolving Concept of Acute Care Surgery
• ACS 2005▪ Trauma▪ Emergency Surgery▪ Critical Care
• ACS 2015▪ Trauma▪ Emergency Surgery▪ Critical Care▪ Elective Surgery▪ Surgical Rescue
A. Peitzman et al. J Trauma Acute Care Surg 2015;79(2):327

Where Are We Now and Where Are We Going?

Istituzione Sistema Integrato Assistenza al Trauma
➢ Network Ospedali➢ Centro Traumi Alta Specializzazione
(CTS)
➢ Centro Traumi di Zona (CTZ)
➢ Pronto Soccorso Traumi (PST)
➢ Volumi ricovero
➢ Concentazione di pazienti = esito migliore

Rete Emergenza
3.752.000 abitanti
PST = 12 (5)
CTZ = 14 (1 con NCH) (4)
CTS = 3 + 1 Pediatrico (1)

Trauma Center di Area Vasta Nord Ovest presso l’AOUP


Trauma Team


Centralizzazione politraumada Ospedale spoke a Trauma
Center AOUP
Richiesta di trasferimento c/o Trauma Center AOUP chiamando il PS AOUP al
numero unico dedicato 050 994660
Medico P.S. periferico
Diagnostica per immagini
Valutazione parametri per trasferimento
Medico P.SAOUP
Allertamento•Trauma Team•Specialista di riferimento
Medico P.S AOUP
Nessun trasferimento
no
sì
arrivo in P.S. Rivalutazione
necessità intervento?Trauma Team/Specialista di riferimento
Trasferimento in S.O.
Rianimatore P.S
Trattamento chirurgicoChirurgo/
anestesista P.S /S.O. spec.
Ricovero in ambiente intensivo
RIANIMAZIONE P.S.
Ricovero in sub intensivo
RIANIMAZIONE P.S./ SUB specialistica riferimento
sì no
Osservazione e nuova diagnosticaRianimazione P.S.
Rivalutazione:Intervento?Specialista riferimento
Rinvio all’ospedale
di provenienza
sì
no
Centralizzazione secondaria da
centro “spoke”
a Trauma Center
di paziente
con trauma in codice rosso
DGRT n°
1380/2016
Centralizzazione secondaria politraumada Ospedale spoke a Trauma Center AOUP
Richiesta di trasferimento c/o Trauma Center AOUP chiamando il PS AOUP al
numero unico dedicato 050 994660
Medico P.S. periferico
Diagnostica per immagini
Valutazione parametri per trasferimento
Medico P.S. AOUP
Allertamento•Trauma Team•Specialista di riferimento
Medico P.S AOUP
Nessun trasferimento
no
sì
arrivo in P.S. Rivalutazione
necessità intervento?Trauma Team/Specialista di riferimento
Trasferimento in S.O.
Rianimatore P.S
Trattamento chirurgicoChirurgo/
anestesista P.S /S.O. spec.
Ricovero in ambiente intensivo
Rianimazione P.S.
Ricovero in sub intensivo
RIANIMAZIONE P.S./ SUB specialistica riferimento
sì no
Osservazione e nuova diagnosticaRianimazione P.S.
Rivalutazione:Intervento?Specialista riferimento
Rinvio all’ospedale
di provenienza
sì
no
2. Centralizzazione secondaria
paziente traumatizzato da centro
“spoke”a Trauma Center con
richiesta attraverso numero
dedicato
DGRT n°
1380/2016

aAzienda Ospedaliero Universitaria Pisana
5,5
5,44
6,7
22,6
21
2,4 2,51,4
2,5
0
5
10
15
20
25
2018 2019
Surgical Procedures (%)
NCH
Ch. Generale
Ch. Ortopedica
Maxillo-facial
Combined procedures


Rete Emergenza
3.752.000 abitanti
PST = 12 (5)
CTZ = 14 (1 con NCH) (4)
CTS = 3 + 1 Pediatrico (1)
Comitato Strategico Rete Trauma Maggiore
• On-site visit CTS• Verifica hardware• U.O. Chirurgica dedicata = 1
Proposta:
o U.O. Trauma & Acute Care Surgery Unit /CTSo Centro Clinico Trauma Center a coordinamento chirurgico/CTS

An organized Trauma System links the necessary resources to maximize patient recovery
• A trauma system includes:– EMS interventions– Emergency department
interventions– Intensive and surgical in-hospital
care– Rehabilitation– Social services– Injury prevention– Research– Education– Disaster Planning

Chirurgia d’Urgenza & Trauma Center: A Che Punto Siamo ?



Trauma Center AOUP

Rete Trauma
Area Vasta Nord-Ovest
(AVNO)

Università di Pisa - Azienda Ospedaliera PisanaU.O. Chirurgia Generale e d’Urgenza
Sc. Specializzazione in Chir. Gen. II- Urgenza
TRAUMA TEAM
Core T.T. In House On Call
24h/24h 24h/24h Reperibilità
1 Chirurgo Ortopedico 3 Chirurghi
1 Resident Ch. Neurochirurgo2 Inf. S.O.*
1 Medico P.S. Ch. max. faciale Team Endoscopia
1 Rianimatore Oculista
1 Tecnico Rian. Otorinolaringoiatra
1 M. Radiologo Etc.
1 Tecn. Radiologo
1 Infermiere (BTLS)





Trauma Surgery: Fatti• Interventi per lesioni regione anteriore collo, torace, addome, grossi
vasi
• Gestione pazienti in Surgical Critical Care Units
• Tendenza alla riduzione ferite penetranti
• Espansione dei trattamenti non chirurgici
• Radiologia interventistica e procedure endoscopiche
• Riduzione carico interventi chirurgici
• Sostenibilità economica
• Minore interesse specializzandi per trauma surgery/ trauma surgeons shortage
Chirurgia d’Urgenza Università di Pisa-AOUP

Istituzione Sistema Integrato Assistenza al Trauma
• Network Ospedali
– Centro Traumi Alta Specializzazione (CTS)
– Centro Traumi di Zona (CTZ)
– Pronto Soccorso Traumi (PST)
• Volumi ricovero
• Concentazione di pazienti = esito migliore

CORE TRAUMA TEAM e TRAUMA TEAM ESTESO - CONFIGURAZIONE
ATTUALE
Nucleo base trauma
(CTT)
1 Chirurgo senior
1 Chirurgo
Specializzando
1 Anestesista
Rianimatore
1 Radiologo
1 Infermiere
1 Tecnico Radiologo
Presente al D.E.U. 24/24 h.
Presente al D.E.U. 24/24 h.
Presente al D.E.U. 24/24 h.*
Presente al D.E.U. 24/24 h.*
Presente al D.E.U. 24/24 h.
Presente al D.E.U. 24/24 h.*
Afferenza “in house”
(Personale di guardia)
Neurochirurgo
Ortopedico
Ch. Maxillo-faciale
Otorinolaringoiatra
Oculista
Ch. plastico-ricostr.
Internista P.S
Presente nel nosocomio 24/24 h
Presente nel nosocomio 24/24 h
Presente nel nosocomio 24/24 h
Presente nel nosocomio 24/24 h
Presente nel nosocomio 24/24 h
Presente nel nosocomio 24/24 h
Presente nel nosocomio 24/24 h
Afferenza “on call”
(Personale in
Reperibilità)
3 Chirurghi
2 Infermieri S.
Operatoria
1 Tecnico Anestesia
Reperibilità
Reperibilità
Reperibilità

Rete Emergenza
To sum-up:
3.752.000 abitanti
PS = 23
DEA 1°= 12 (1 con NCH)
DEA 2°= 3 + 1 Pediatrico
Centrali Operative 118 = 8