A FOGLALKOZTATÁSBŐVÍTÉS ATIPIKUS FORMÁI ATYPICAL FORMS OF EMPLOYMENT EXPANSION
Upload
emily-eresumaCategory
view
87download
0description
Morning Report May 20, 2015
Valerie Riss, MD/MPH
HPI: Previously healthy 5yo F admitted with unilateral cervical
lymphadenitis. 12 days prior to admission developed dry cough 4 days prior to admission developed low grade fever (99-101),
nausea/emesis, neck stiffness, 2 days prior to admission developed worsening left neck pain
associated with drooling, decreased appetite, decreased range of motion.
Went to PCP, noted to be febrile to 102 with left cervical lymphadenopathy, and sent her to ED.
ED: Met shock protocol (tachycardia, tachypnea, fever, hypertensive), received fluid boluses x 2, ibprofen and CTX (2g) heart rate decreased from 155 to 110. CXR normal. Neck CT showed left anterior and posterior cervical lymphadenitis without abscess. Started on Unasyn (1200mg q6) and toradol and admitted.
Case Presentation
Admission PE: Vitals on admission to floor HD1: T 36.9, HR 114, RR 40, BP: 117/72,
95% on RA Gen: Tired, uncomfortable appearing HEENT: No conjunctival injection, TMs fine, could not open mouth due to
pain, no red/cracked lips. Enlarged and “exquisitely” tender L anterior cervical node, able to move neck through full range of motion
CV: RRR, normal S1/S2, 1/6 SEM at LUSB, no gallop, cap refill < 3 sec Lungs: breathing comfortably, clear lungs Abdomen: Tender to palpation in RUQ and epigastrum, but soft, no
masses, no hepatospenomegaly Extremities: warm and well perfused, no swelling Skin: Erythema over left neck and face, otherwise no rash, no jaundice Neuro: tired, but alert and responsive, grossly normal strength and
tone, symmetric movement of all extremities, CNs grossly intact but not specifically examined
Case Presentation
Overnight HD1 – 2: HR 130s-140s, climbed to 160s with lactate 1.6, preserved bp
HD2: In am noted to be tachycardic up to 160 with preserved blood pressure. 20/kg bolus was given (60/kg over approx 12 hours), approximately ¾ of the way through on re-checking patient noted new S3, new JVD, and hepatomegaly. Fluid bolus stopped. Good mentation, reasonable urine output. HRs did not decrease from fluid bolus.
Additional symptoms noted HD2: abdominal pain and distension, in particular RUQ
Case Presentation
PMH: Had croup 12/2014 and stayed overnight in ED No chronic medical conditions T&A 10/2014 Meds: No home meds, no antibiotics prior to admissionAllergies: NKDAImmunizations: UTD, seasonal flu vaccine receivedFamily History: negative for recurrent infections, MRSA.
Brother with history of SVT s/p ablation. No history of congenital heart disease, other history of arrhythmia, heart failure, SIDS, or sudden death.
Social history: Lives with parents and 2 older brothers, in kindergarten. Has one dog, one cat. No recent travel.
Case Presentation
CBC w/diff: WBC 25.6 (Bands 8%, Neut 83%, Lymph 5%, Mono 4%), Hgb 12.5, Hct 36.7, Plts 313,
Na 134, K 4.4, CO2 20, Glucose 76, iCa 1.23, lactate 1.6
CBG: 7.34/35/25/19/-6 ESR: 93 CRP: 11.8 VRP: negative
Admission Labs
Previously healthy 5yo female presenting on HD2 with unilateral cervical lymphadenitis, not responding to Unasyn, in compensated shock with symptoms of fluid overload, leukocytosis, elevated inflammatory markers, and RUQ pain in the setting of 12 days of cough and 4 days of low grade fever, nausea and vomiting.
One-liner
InfectiousBacterial lymphadenitis:
Staph (rarely MRSA)GASGBSOral anaerobic pathogens
Viral lymphadenitis:CMVEBV
TBTularemiaNon-tuberculous mycobacteriaHIV TularemiaToxoplasmosisSyphillisCat Scratch
GI:CholecystitisCholedocolythiasis
Rheum:Connective Tissue DisorderKawasakiLupusJIAKikuchi-Fujimoto syndromePFAPA
Hem/Onc:LymphomaLeukemiaHLH (hemophagocytic lymphocytosis)Thyroid tumorSuperior mediastinal tumor
CV:AVM (could explain right sided overload with boluses)MyocarditisDilated cardiomyopathy
Differential Diagnosis
HD2:BNP – 758CBG: 7.35/35/45/19/-5UA (clean catch): spec grav > 1.030, 1+ ketones, neg nitirites, neg hgb, trace protein, neg LE, 2 WBC, 0 RBC 1 epi, negative bacteriaRFP: Na 140, K 4.7, Cl 114, CO2 12, BUN 13, Creat 0.58, Alb 2.8, Ca 9.2, Phos 3.9 HD 4:CMP: Na 140, K 3.9, Cl 111, CO2 18, BUN 8, Creat 0.42, Ca 8.6, Prot 5.7, Alb 2.7, TB 0.4, Alk Phos 226, ALT 216, AST 194
Trends:WBC: 25.6 (HD1), 19.7 (HD5), 11.1 (HD8)Hg: 12.5 -> 9.5 -> 9.2Plts: 313 -> 277 -> 358CRP: 11.8-> 11.7 -> 8.8
Labs
ID labs: C.diff negative EBV negative CMV negative Toxoplasmosis: negative HIV negative Cat scratch Abs
(IgG/IgM) negative PPD 0mm Mycoplasma antibodies:
negative
Labs continuedHem/onc labs:
PT/INR: 15.6/1.3 Uric acid/LDH:
normal Ferritin: 241 – mildly
elevated Rheum labs:
ANA negative CPK normal C3/C4: normal
KUB on HD2: non-obstructive bowel gas pattern with possible mild ileus.
Echo on HD2: Dilated right atrium and right ventricle with flow reversal in the descending and abdominal aorta. Trace tricuspid valve insufficiency, trivial pericardial effusion
Hospital Course
HD3 – HRs increased, BPs decreased -> PICU, started on milrinone for a few hrs -> floor HD4
ID, Rheum, Cardiology consulted, lots of work up ensued
Repeat echo HD7 following rheum consult Echo HD7: Dilated distal RCA, posterior descending
artery dilatation mild, mild tricuspid valve regurg, dilated right atrium, dilated right ventricle, normal left ventricular size and function, small posterior pericardial effusion, at least moderate right pleural effusion
Follow up echo at 6 weeks – persistent right coronary artery dilatation, Z-score 1.42
Hospital Course
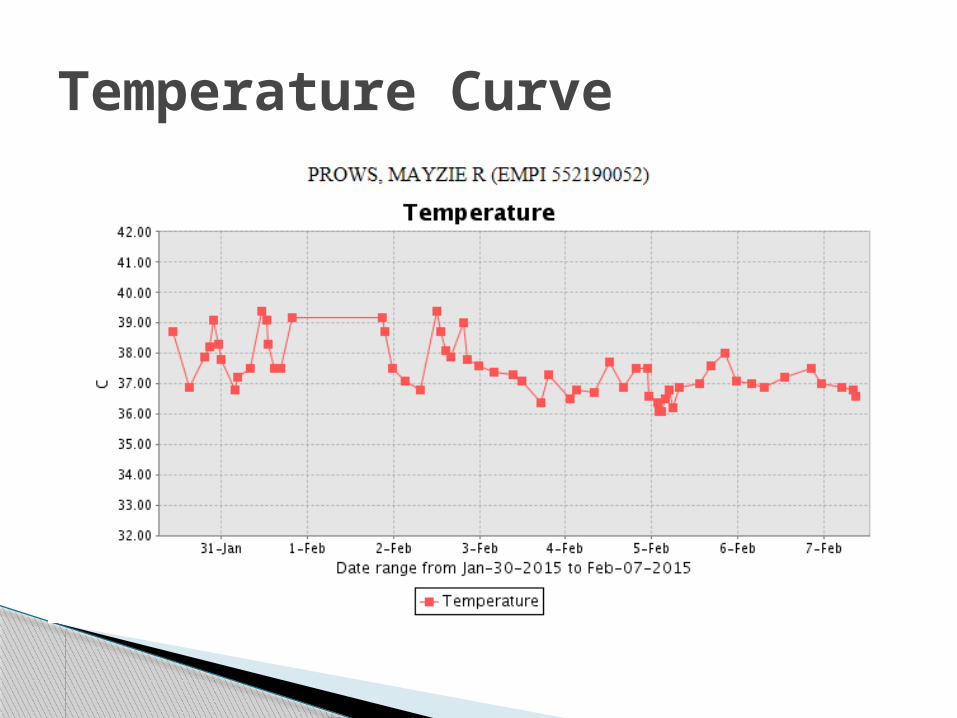
Temperature Curve
WHAT??
Atypical Kawasaki
Irritability almost always present Fever comes and goes, generally > 39/40 when present America: Fever >= 5 days + 4/5 of:
◦ Bilateral bulbar conjunctival injection◦ Oral mucous membrane changes, including injected or fissured
lips, injected pharynx, or strawberry tongue◦ Peripheral extremity changes
Erythema of palms/soles Edema of hands/feet Peri-ungal desquamation
◦ Polymorphous rash◦ Cervical lymphadenopathy (at least one node > 1.5cm)
Japanese criteria – fever is one of 6 criteria, require 5/6
Typical Kawasaki
CRP > 3 and/or ESR > 40Supplemental labs: Alb <=3, anemia for
age, Increased ALT, Plts >450, WBC > 15, Urine WBC > 10
Atypical Kawasaki
Japanese MR – 8/10,000 – mortality ratio 1.25 overall, 2.35 for boys with cardiac sequlae
US – in-hospital mortality 17/10,000 Peak mortality 15-45 days (combo of bad
coronary vasculitis with thrombocytosis)
Kawasaki Disease
Most common cause of acquired heart disease in children in developed countries
Other findings: pericardial effusion, pericarditis, myocarditis, valvular incompetence, cardiac failure, MI
Hyperdynamic precordium, tachycardia, gallop rhythm, innocent flow murmur, depressed myocardial contractility, low cardiac output syndrome, EKG changes – prolonged PR, non-specific ST/T wave changes
Kawasaki and the Heart
Aneurysms, coronary arteritis, decreased left ventricular contractility, mild valvular regurgitation (primarily mitral valve), and pericardial effusion.
Aneurysms rarely develop before day 10 Early echo findings of arteritis: perivascular
brightness, lack of tapering of the coronary arteries, decreased left ventricular contractility, mild valvular regurgitation (most commonly mitral), and pericardial effusion
Echo findings
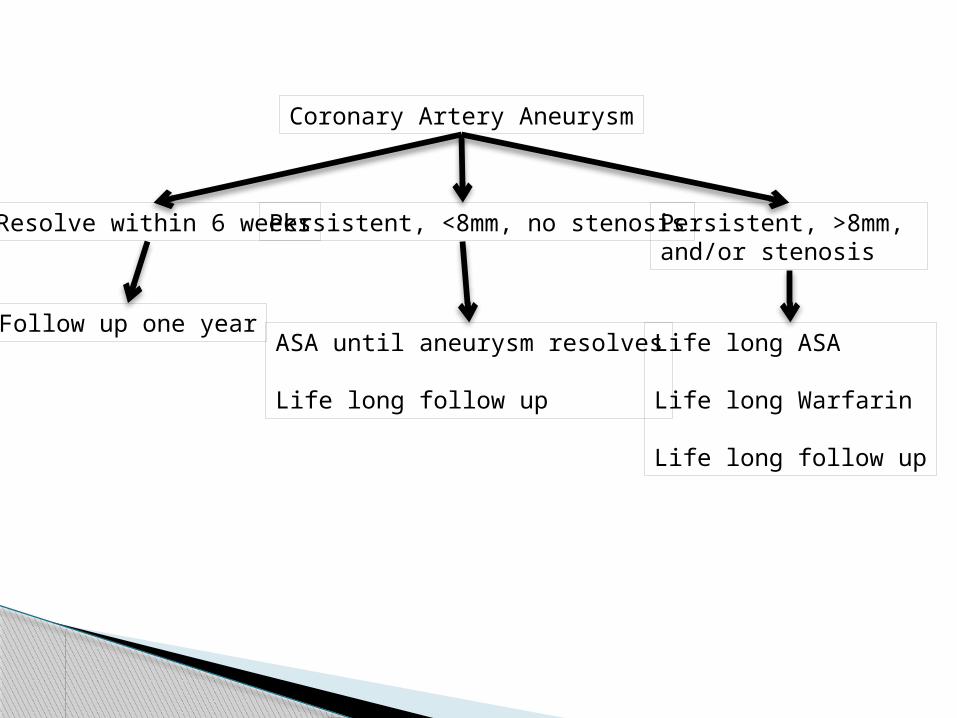
Coronary Artery Aneurysm
Resolve within 6 weeksPersistent, <8mm, no stenosis Persistent, >8mm, and/or stenosis
Follow up one year Life long ASA
Life long Warfarin
Life long follow up
ASA until aneurysm resolves
Life long follow up
ArthritisAseptic meningitisPneumonitisUveitisGastroenteritisMeatitisDysuriaOtitisGallbaldder hydrops –
15%GI ischaemia
Other weird symptomsJaundiceCN palsyRenal involvementPetechial rashShock syndromeFebrile convulsionsEncephalopathyAtaxiaMacrophage activation syndromeSIADHTransient sensorineural hearing loss
Diagnostic criteria present prior to day 5 CAA or coronary dilatation are present Persistently elevated inflammatory markers
with no other explanation
When to Treat
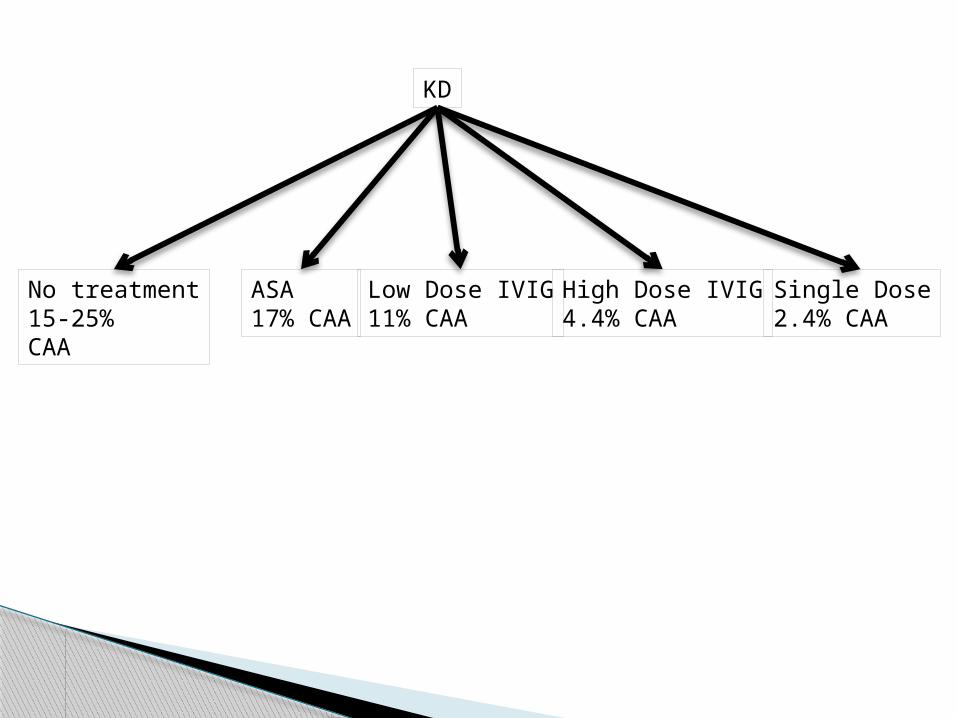
KD
No treatment15-25%CAA
ASA17% CAA
Low Dose IVIG11% CAA
High Dose IVIG4.4% CAA
Single Dose2.4% CAA
Rigors (18%) Pruritius (4%) Urticaria Nausea Hypotension Many many more
Side effects of IVIG
Persistently elevated CRP or lack of defervescence despite IVIG, liver dysfunction, hypoalbuminaemia, anemia, HLH, shock
20% are resistant to IVIG Additional therapies – Steroids, TNF-alpha
inhibitors, other monoclonal Abs, plasma exchange, cytotoxic agents
Markers of high severity
Fever >= 7 days unexplained – get labs to evaluate
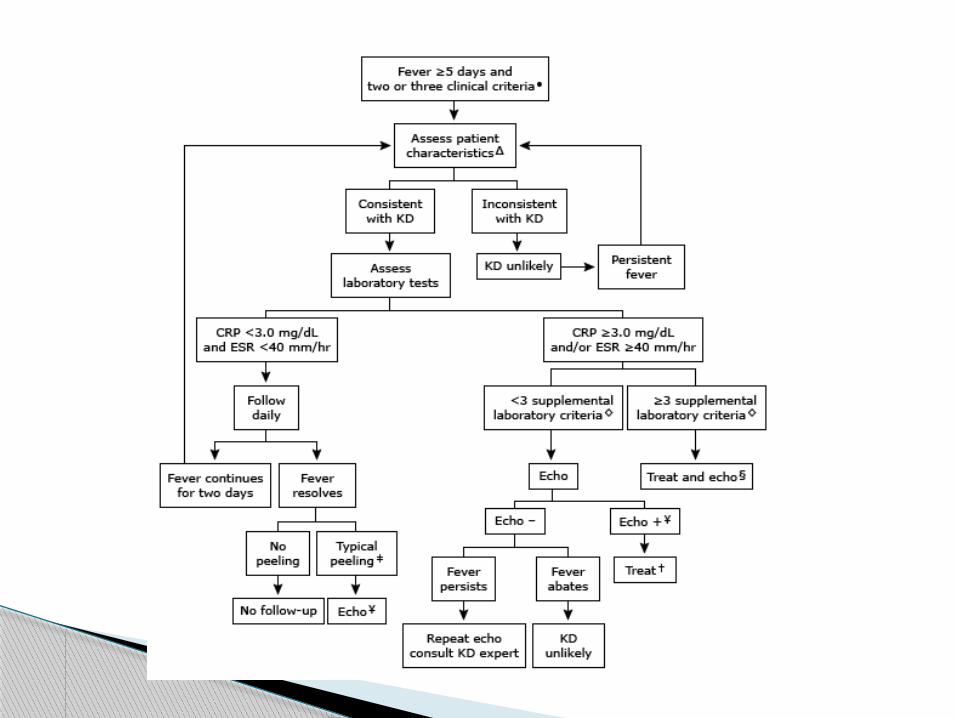
Patients of any age with unexplained fever >= 5 days and only 2-3 clinical criteria
If there is periungual desquamation after resolution of the fever in someone not meeting epidemiologic criteria for KD
When to Eval
Abdominal CT on HD 5: Mild hepatomegaly, moderate pelvic fluid, large right pleural effusion, small left pleural effusion, possible fecalith right lower abdomen
Neck ultrasound HD5: no fluid collection Echo HD7: Dilated distal RCA, posterior
descending artery dilatation mild, mild tricuspid valve regurg, dilated right atrium, dilated right ventricle, normal left ventricular size and function, small posterior pericardial effusion, at least moderate right pleural effusion
Additional Imaging
Uptodate Newberger et al. Diagnosis, Treatment and
Long-Term Management of Kawasaki Disease. Circulation 2004: 110: 2747-2771
Eleftheriou et al, Management of Kawasaki Disase. Arch Dis Child 2014; 99; 74-83
Dorongpiskitkul et al. The prevention of coronary artery aneurysm in Kawasaki disease: a meta-analysis on the efficacy of aspirin and Immunoglobulin treatment. Pediatrics 1995 Dec; 96 (6): 1057-61
References