asma y corticoesteroides
16
DOI:10.1542/peds.2007-3273 2009;123;353-366 Pediatrics Gary Rachelefsky and Risk Inhaled Corticosteroids and Asthma Control in Children: Assessing Impairment http://www.pediatrics.org/cgi/content/full/123/1/353 located on the World Wide Web at: The online version of this article, along with updated information and services, is rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk publication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly by on March 14, 2010 www.pediatrics.org Downloaded from
-
Upload
fiona-truvill -
Category
Documents
-
view
219 -
download
0
Transcript of asma y corticoesteroides

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 1/16
DOI: 10.1542/peds.2007-32732009;123;353-366Pediatrics
Gary Rachelefskyand Risk
Inhaled Corticosteroids and Asthma Control in Children: Assessing Impairment
http://www.pediatrics.org/cgi/content/full/123/1/353located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. Alland trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk publication, it has been published continuously since 1948. PEDIATRICS is owned, published,PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 2/16
REVIEW ARTICLE
Inhaled Corticosteroids and Asthma Control inChildren: Assessing Impairment and RiskGary Rachelefsky, MD, FAAP
Executive Care Center for Asthma, Allergy, and Respiratory Diseases, Geffen School of Medicine at UCLA, Los Angeles, California
The author has indicated he has no nancial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.To review the use of inhaled corticosteroids on asthma control in children byusing the new therapeutic paradigm outlined in the Expert Panel Report 3: Guidelinesfor the Diagnosis and Management of Asthma .
METHODS.A systematic review of the literature was performed by using the Medlineand Embase databases (January 1996 to October 2007).
RESULTS.A total of 18 placebo-controlled, clinical trials in 8000 children (aged 0–17years) with asthma met the criteria for evaluating monotherapy with inhaled corti-costeroids: 13 double-blind studies of inhaled corticosteroids versus placebo and 5controlled studies that compared inhaled corticosteroids to a nonsteroid antiinam-matory agent. The ndings can be summarized as follows: (1) Compared withplacebo, inhaled corticosteroid treatment was associated with reductions in both theimpairment and risk domains. (2) Improvements in impairment and risk observedwith inhaled corticosteroids were generally greater than those observed with non-steroid antiinammatory comparator medications. (3) Inhaled corticosteroids werewell tolerated. (4) Small reductions in growth rates were evident when comparedwith placebo and/or comparator nonsteroid antiinammatory medication use in thelong-term ( 1-year) studies, but when measured, the reductions diminished withtime.
CONCLUSIONS.Treatment with inhaled corticosteroids improves the asthma-control do-mains of impairment and risk in children. Differences in study protocols makedetailed comparisons difcult. Specic needs for additional trials include (1) morestudies using appropriate indicators for impairment (eg, rescue-medication use;symptoms scores; asthma/episode-free days) and risk (eg, forced expiratory volumein 1 second in children who can perform spirometry; exacerbations requiring oralcorticosteroids; urgent care usage) and (2) more studies evaluating adolescents; themajority of the data reported were for children up to the age of 12 years, and data foradolescents are often lost (either grouped with adults [eg, studies in patients 12years old] or not included [eg, studies of school-aged children 12 years old]).Attention should be given to standardizing variables that will permit comparison ofoutcomes between trials. Pediatrics 2009;123:353–366
THE NATIONAL HEART, Lung, and Blood Institute of the National Institutes ofHealth recently released an update of the US asthma clinical practice guidelines,
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma 1 (EPR3).This new document incorporates an evidence-based assessment of former guidelinesand current literature in revising the recommendations for practice.
The relative burden of asthma in relation to other chronic conditions remains high, particularly in children, despitebetter understanding of asthma, improved approaches to treatment, and modest gains in asthma morbidity. 2 Theprevalence of asthma in the United States is greater in children than in adults (8.9% vs 7.2%, 2005 data). 3 Asthmaaffects 6.5 million children (0–17 years old); 1.4 million are 5 years old. 3 Children are more likely to havesuboptimally controlled asthma as demonstrated by exacerbations and use of urgent care services. The rates ofasthma exacerbations reported in 2005 for the previous 12 months were 5.2% and 3.9% for children and adults withasthma, respectively. 3 There were 103 emergency department (ED) visits per 10 000 children compared with 50 EDvisits per 10 000 adults; hospitalization rates were 27 per 10 000 children versus 14 per 10 000 adults. Children 5years old had the highest rates: 168 ED visits and 60 hospitalizations per 10 000 children. 3 Asthma resulted in 1missed day of school for almost 13 million children (5–17 years old) in 2003. 3
www.pediatrics.org/cgi/doi/10.1542/peds.2007-3273
doi:10.1542/peds.2007-3273
Key Wordsasthma control, childhood asthma,impairment, inhaled corticosteroid,pediatric asthma, persistent asthma, risk
AbbreviationsEPR Expert Panel reportED emergency departmentICS inhaled corticosteroidmAPI modied Asthma Predictive IndexOCS oral corticosteroidFDA Food and Drug AdministrationBIS budesonide inhalation suspensionFP uticasone propionateDPI dry powder inhalerBDP beclomethasone dipropionateAE adverse eventCAMP Childhood Asthma ManagementProgramNED nedocromil sodiumSAB short-acting bronchodilatorFEV1 forced expiratory volume in 1second
bid twice dailyqd once dailySTART Steroid Treatment as RegularTherapyprn as neededSARE severe asthma-related eventLABA long-acting bronchodilator
Accepted for publication Apr 16, 2008
Address correspondence to Gary Rachelefsky,MD, FAAP, Executive Care Center for Asthma,Allergy, and Respiratory Diseases, GeffenSchool of Medicine at UCLA, 200 MedicalPlaza, Suite 140-17, Los Angeles, CA 90095.E-mail: [email protected]
PEDIATRICS (ISSNNumbers:Print, 0031-4005;Online, 1098-4275). Copyright© 2009by theAmericanAcademy of Pediatrics
PEDIATRICS Volume 123, Number 1, January 2009 353by on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 3/16
For most patients, asthma onset occurs early in life,and disease persistence is associated with recognizablerisk factors including atopic disease, recurrent wheezing,and a parental history of allergy and/or asthma. Evi-
dence indicates that therapy with current antiinamma-tory medications does not prevent progression of theunderlying disease. 1 In contrast to previous guidelinesthat focused on reducing asthma severity, the newguidelines target asthma control as the primary goal formanagement. Classifying asthma severity to initiatetreatment is differentiated from assessing asthma controlfor ongoing monitoring, and both are broken down tonewly dened domains of impairment and risk to op-erationalize therapeutic targets (Table 1). 1
The goal of asthma therapy is to achieve asthmacontrol by reducing impairment and risk on the basis ofthe criteria 1 shown in Table 2. As in previous guidelines,inhaled corticosteroids (ICSs) are the preferred class oflong-term controller medications to manage persistentasthma in all age groups. Numerous studies in childrenwith asthma have established that ICSs improve pulmo-
nary function, reduce the need for reliever medications,improve quality of life, enhance exercise tolerance, andreduce hospitalizations. 1 Thus, although early interven-tion with ICSs for childhood asthma does not alter thenatural history of asthma, these medications are impor-tant for gaining and maintaining asthma control. 1 How-ever, no review to date has examined the effect of ICSson childhood asthma in terms of impairment and risk asdened in the EPR3. The purpose of this review is toevaluate the data on ICSs in childhood asthma withspecic regard to the newly dened domains of risk andimpairment.
METHODSA systematic review of the literature was performed forrandomized, placebo-controlled studies that evaluatedmonotherapy with ICSs in children. Searches of theMedline and Embase databases (January 1996 to Octo-ber 2007) were performed by using the Medical SubjectHeadings (MeSH) terms asthma, beclomethasone dipro-pionate, budesonide, unisolide, controlled clinical tri-als, uticasone propionate, mometasone, randomized,controlled trials, and triamcinolone acetonide and thetext words childhood asthma, pediatric asthma, persis-tent asthma, and ICS. Searches were limited to humansubjects aged 0 to 17 years and English-language litera-ture.
EFFICACY OF ICSs IN CHILDRENAccording to the new guidelines, “ICSs are the mostpotent and consistently effective long-term control med-ication for asthma” for adults and children. 1 They are theonly medications consistently shown to meet the goalsof pharmacotherapy for asthma:
● control (ideally, prevent) asthma symptoms;● reverse airow obstruction;● improve quality of life; and● decrease the number and severity of asthma exacer-
bations (and associated urgent medical care).
In the step-care approach to therapy, ICSs are the main-stay of treatment for all patients with persistent asthma(Fig 1, steps 2–6). Treatment for adolescents (12–18years old) is the same as for adults; changes to thealgorithm are shown for children 12 years old. Table 3shows the currently available ICSs indicated for use inchildren in the United States.
The broad action of ICSs on airway inammation andassociated clinical markers in asthma is well documentedand beyond the scope of this article. 4–7
Most of the clinical benets observed with ICS treat-ment in children occur at low doses. However, similar toadults, the dose response to ICSs in children may varyaccording to the clinical outcome (eg, improvement inlung function, prevention of exacerbations) and patientcharacteristics. Children with more severe asthma mayrespond to higher doses, whereas those with mild ormoderate asthma usually show a plateauing of effect atlow and medium doses. 8–11 Nonetheless, stepping up the
TABLE 1 Some KeyTermsUsed to Dene thePatient With AsthmaRegardless of Age 1
Term Denition
Severity The intrinsic intensity of asthma pathology, which is measuredmost easily and directly before a patient starts long-termcontrol therapy (ie, before a patient is being treated)
Control The degree to which the manifestations of asthma(symptoms, functional impairments, risks of AEs) areminimized and the goals of therapy are met
Impairment The frequency and intensity of symptoms and functionallimitations that the patient is experiencing or has recentlyexperienced
Risk The likelihood of asthma exacerbations, progressive decline inlung function (or, for children, reduced lung growth), oradverse effects from medication
TABLE 2 Criteria for Achieving Asthma Control by Targeting theDomains of Impairment andRisk 1
Asthma-ControlDomain
Criteria
Reducing impairment Prevent chronic and troublesome symptoms (eg,coughing or breathlessness in the daytime,nighttime, after exertion)
Infrequent use ( 2 d/wk) of inhaled SAB forquick relief of symptoms
Maintain (near) “normal” pulmonary functionMaintain normal activity levels (including
exercise, other physical activity, attendance atwork or school)
Meet patients’ and families’ expectations of andsatisfaction with asthma care
Reducing risk Prevent recurrent exacerbations of asthma;minimize ED visits, urgent care visits,hospitalizations
Prevent progressive loss of lung function (forchildren, prevent reduced lung growth)
Provide optimal pharmacotherapy with minimal(ideally, no) adverse effects
354 RACHELEFSKYby on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 4/16
ICS dose may provide added clinical benet for somechildren with mild or moderate asthma during exacer-bations or seasonal increases in symptom severity (eg, toallergens, respiratory viruses). 1 This “exible dose ap-proach” to treatment suggests that ICS therapy may beincreased temporarily in response to some index ofworsening asthma, usually an increase in symptoms,nighttime awakenings, decrease in peak ow rate, or useof rescue medications; it remains subject to continuedstudy and discussion. 12–15 In the future, such dose adjust-
ments may be based on measurement of a simple bi-omarker of airway inammation in children; sputumeosinophils and exhaled nitric oxide are being studiedbut require further validation. 16,17
USING ICSs IN INFANTS AND YOUNG CHILDREN ( < 5 YEARSOLD)As in older children and adults, the use of ICSs in infantsand young children is directed toward symptom control,preventing exacerbations, and improving the child’s
Intermittentasthma
Consult with asthma specialist if step 3 care or higher is required.Consider consultation at step 2.
STEP 1PREFERRED
SABA prn
STEP 2
PREFERRED
Low-dose ICS
ALTERNATIVE
Montelukast or cromolyn
STEP 3PREFERRED
Medium-doseICS
STEP 4
PREFERRED
Medium-doseICS
andeither
or LABA
STEP 5
PREFERRED
High-doseICS
andeither
montelukastor
LABA
STEP 6
PREFERRED
High-dose ICS
andeither
montelukastor
LABA
andoral corti-costeroids
FOR ALL PATIENTS and AT ALL STEPS:Education and environmental control
• Quick-relief medication: SABA prn for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at20-min intervals as needed. Short course of oral corticosteroids may be needed.
• Caution: Increasing of β-agonist or use >2 times per wk for symptoms control indicates inadequate control and the need to stepup treatment.
•Step up if needed
(first, checkadherence,
environmentalcontrol and
comorbidconditions)
Step downif possible
(and asthma iswell-controlled
at least 3mo)
ASSESSCONTROL
FOR ALL PATIENTS and AT ALL STEPS:• Education and environmental control• Quick-relief medication: SABA prn for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at
20-min intervals as needed. Short course of oral corticosteroids may be needed.• Caution: Increasing of β-agonist or use >2 times per wk for symptoms control indicates inadequate control and the need to step
up treatment.
•Step up if needed
(first, checkadherence,
environmentalcontrol andcomorbid
conditions)
Step downif possible
(and asthma iswell-controlled
at least 3mo)
ASSESSCONTROL
Intermittentasthma
Persistent asthma: daily medicationConsult with asthma specialist if step 4 care or higher is required.
Consider consultation at step 3.
STEP 1
PREFERRED
SABA prn
STEP 2
PREFERRED
Low-dose ICSALTERNATIVE
LTRA,cromolyn,
nedocromil or theophylline
STEP 3
PREFERRED
Medium-doseICS
or
low-dose ICS+ LABA,LTRA, or
theophylline a
STEP 4
PREFERRED
Medium-doseICS + LABA
ALTERNATIVE
medium-doseICS + either
LTRA or theophyllline a
STEP 5PREFERRED
High-dose ICS+ LABAb
andomalizumab
may be
considered for patients whohave allergies c
STEP 6
PREFERRED
High-dose ICS+ LABAb
+ oralcorticosteroid
andomalizumab
may beconsidered for patients who
have allergies c
A
B
FIGURE 1A, Stepwise approach for managing asthma in patients 0 to 4 years of age.1 B, Stepwise approach for managing asthma in patients 5 years of age.1 a Zileuton may be considered inpatients 7 to 12 years old;b alternative in patients 5 to 11 years old: high-dose ICS plus either leukotriene receptor antagonist (LTRA) or theophylline;c 12 years old or older. (Adapted
fromNationalAsthma Educationand PreventionProgram.ExpertPanelReport3: Guidelinesforthe Diagnosisand Managementof Asthma.Bethesda,MD:NationalInstituteofHealth,2007[Tables 41a and 41b].)
PEDIATRICS Volume 123, Number 1, January 2009 355by on March 14, 2010www.pediatrics.orgDownloaded from
8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 5/16
(and family’s) quality of life. Treatment with ICSs shouldnot be initiated or prolonged to alter the progression orunderlying severity of asthma. 1
Data on the use of ICSs to treat asthma in young
children, particularly infants, are limited. Most treat-ment recommendations are based on expert opinion andextrapolations from studies in older children and adults. 1
The most common symptoms of asthma in this popula-tion are wheeze and cough, which are frequently asso-ciated with other conditions. 18–20 A diagnostic trial ofICSs is recommended if asthma is suspected.
A predictive clinical index (the modied Asthma Pre-dictive Index [mAPI]) to identify children 3 years oldwho might be at high risk for developing asthma hasbeen developed and validated on the basis of data fromthe Tucson Children’s Respiratory Study. 18,21 In pre-school-aged children a positive mAPI was associatedwith 4 severe wheezing episodes requiring use of oralcorticosteroids (OCSs) in 12 months and increased hos-pitalizations and urgent care visits for asthma. 21,22 Therecommendation of the EPR3 regarding which youngchild is appropriate for ICS therapy builds on the mAPI(Table 4).
ICSs approved by the Food and Drug Administration(FDA) in the United States for young children ( 5 yearsold) include budesonide inhalation suspension (BIS),which is approved for children as young as 12 months,and uticasone propionate (FP) dry powder inhaler(DPI) and hydrouoroalkane formulations, which areapproved for children as young as 4 years. Beclometha-sone dipropionate (BDP) hydrouoroalkane is only ap-
proved for children aged 5 years. Although not ap-proved for young children and there are no dataregarding dosing, efcacy, or safety in this population,many pediatricians will use a diagnostic trial of any of
these ICSs as they deem necessary. Figure 2 presents analgorithm for a diagnostic trial of ICSs in infants andyoung children.
SAFETY OF ICSs IN CHILDRENRegardless of age, few patients report serious adverseevents (AEs) with ICSs at the recommended dosages,even with long-term use. 23–26 Most clinical benet withICSs is achieved at relatively low doses, further reducingthe potential risk of AEs. 1 Nonetheless, as for any regu-larly used medication, children should be monitoredregularly for potential systemic AEs, particularly becausesome children may be more susceptible to the effects ofICSs even at conventional doses. Suggestions for reduc-ing AEs associated with ICSs are shown in Table 5.
Data on potential adverse effects of low- or medium-dose ICSs on the hypothalamic-pituitary-adrenal axis inchildren show rare events, which are usually clinicallyinsignicant. 27,28
Of greater concern has been the potential effect ofICSs on linear growth. Again, the available data for low-to medium-dose ICSs show a minimal effect on growthvelocity: a reduction of 1 cm in the rst year of treat-ment in some children. This decrease, when observed,usually does not progress over time, and long-term stud-ies have indicated that these children attain their fulladult height. 18,28–32 All children using ICSs should be
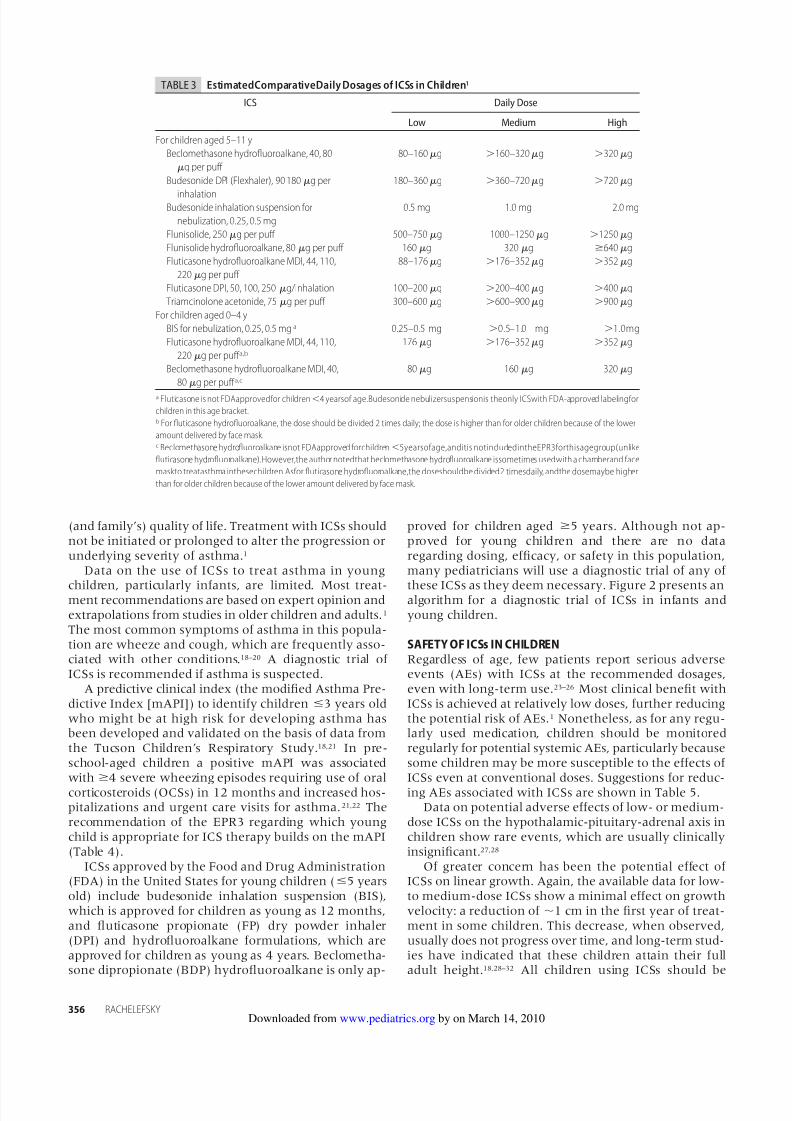
TABLE 3 EstimatedComparativeDaily Dosages of ICSs in Children 1
ICS Daily Dose
Low Medium High
For children aged 5–11 yBeclomethasone hydrouoroalkane, 40, 80
g per puff 80–160 g 160–320 g 320 g
Budesonide DPI (Flexhaler), 90180g per
inhalation
180–360 g 360–720 g 720 g
Budesonide inhalation suspension fornebulization, 0.25, 0.5 mg
0.5 mg 1.0 mg 2.0 mg
Flunisolide, 250 g per puff 500–750 g 1000–1250 g 1250 gFlunisolide hydrouoroalkane, 80 g per puff 160 g 320 g 640 gFluticasone hydrouoroalkane MDI, 44, 110,
220 g per puff 88–176 g 176–352 g 352 g
Fluticasone DPI, 50, 100, 250g/inhalation 100–200 g 200–400 g 400 gTriamcinolone acetonide, 75 g per puff 300–600 g 600–900 g 900 g
For children aged 0–4 yBIS for nebulization, 0.25, 0.5 mga 0.25–0.5 mg 0.5–1.0 mg 1.0mgFluticasone hydrouoroalkane MDI, 44, 110,
220 g per puff a,b
176 g 176–352 g 352 g
Beclomethasone hydrouoroalkane MDI, 40,80 g per puff a,c
80 g 160 g 320 g
a Fluticasone is not FDAapprovedfor children 4 yearsof age.Budesonide nebulizersuspensionis theonly ICSwith FDA-approved labelingforchildren in this age bracket.b For uticasone hydrouoroalkane, the dose should be divided 2 times daily; the dose is higher than for older children because of the loweramount delivered by face mask.c Beclomethasone hydrouoroalkane isnot FDAapproved forchildren 5yearsofage,anditis notincludedintheEPR3forthisagegroup(unlikeuticasone hydrouoroalkane).However,the author notedthat beclomethasone hydrouoroalkane issometimes usedwith a chamberand facemaskto treatasthma inthesechildren. Asfor uticasone hydrouoroalkane,the doseshouldbe divided2 timesdaily, andthe dosemaybe higherthan for older children because of the lower amount delivered by face mask.
356 RACHELEFSKYby on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 6/16
monitored by stadiometry and, if possible, measured by
the same person at each clinic visit. 1 Although no specicclinical cutoffs are provided in the EPR3, my approach inpractice is to (1) reduce the ICS dose if there is slowingof growth at the 3-month visit and the child’s asthma isstable and (2) stop ICSs and consider changing the med-ication or the device if the child is still not growing after6 months. A reduction in growth velocity also resultsfrom inadequate control of asthma. 1 Table 6 summarizesthe evidence-based ndings of the 2007 EPR3.
For children with difcult-to-control asthma, whorequire higher doses of ICSs, the use of adjunctive long-term control therapy is recommended to reduce the doseof ICSs and, thus, minimize possible dose-related long-
term effects on growth (Fig 1).1
High doses of ICSs ad-ministered for prolonged periods of time (eg, 1 year),particularly in combination with frequent courses ofOCSs, may be associated with adverse growth effects.However, the benets of early intervention with ICSs
may outweigh the potential small reduction in growthvelocity in these children (Table 6). 1,18,32
THE EFFECT OF ICSs ON THE DOMAINS OF IMPAIRMENT ANDRISK IN CHILDRENEighteen randomized, placebo-controlled studies involv-ing 8000 children (0–17 years old) met the criteria for
reviewing monotherapy with ICSs: 13 double-blindstudies of ICSs alone (Table 7) and 4 double-dummystudies comparing ICSs to a nonsteroid antiinamma-tory agent (Table 8). One study, the Childhood AsthmaManagement Program (CAMP), was a double-blindedtrial that compared nedocromil sodium (NED), budes-onide, and matched placebos and is included in Tables 7and 8. Approximately 4900 children were exposed toICSs in these studies.
In most of the studies, the children had mild or mod-erate persistent asthma as dened by symptoms, use ofshort-acting bronchodilator (SAB), and/or need for dailyasthma medications. At study entry all children wereusing 1 asthma medication, an SAB with or without acontroller medication (ICSs, cromolyn sodium). For chil-dren who were able to perform spirometry, baselineforced expiratory volume in 1 second (FEV 1 ) rangedfrom 70% to 90% predicted.
Study duration was 12 weeks, and dosing frequencyfor ICSs was twice or less daily.
Double-Blind, Placebo-ControlledStudiesA total of 6700 children received placebo ( n 2696) oran ICS ( n 4004) for 12 weeks. The ICSs includedbudesonide, 200 to 2000 g/day ( n 2941), FP, 100 to200 g/day ( n 826), or BDP hydrouoroalkane, 80 to
160 g/day ( n 237).Three studies evaluated 2 years of treatment withbudesonide ( n 1951) or FP ( n 143). 18,29,33 Five stud-ies evaluated young children and/or infants (mean age:
5 years). 18,34–37 The results were comparable to the
TABLE 4 ICSs as Asthma Controller Therapy in Infants and YoungChildren 1
Recommended for thechild who:
Has had 4 episodes of wheezing in the pastyear that lasted 1 d and affected sleepand who has either 1 of the following:
Parental history of asthmaPhysician’s diagnosis of atopic dermatitisEvidence of sensitization to aeroallergens
or 2 of the following:Evidence of sensitization to foods
4% peripheral blood eosinophiliaWheezing apart from colds
Should be considered forthe child who:
Consistently requires symptomatic treatment2 d/wk for 4 wk
Has had 2 exacerbations requiring systemiccorticosteroids within 6 mo
Has periods, or seasons, of previouslydocumented risk
Monitor child’s response to therapy4–6 wk
No clear positiveresponse
Positive responsesuggested
Diagnostic trialwith ICS
Check medicationtechnique,adherence
(parents/caregivers)
Monitor child’s response to therapy12 wk Satisfactory
Unsatisfactory
Consider alternativediagnoses/therapies
Careful step down to lowestdose to maintain control
Positive responsesuggested
FIGURE 2Algorithm for a diagnostic trial of ICSs in infants and young chil-dren ( 5 years old) with suspected asthma.1
PEDIATRICS Volume 123, Number 1, January 2009 357by on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 7/16
studies conducted in school-aged children (mean age:
5 years).Treatment with ICSs clearly improved measures of
impairment. Benets in the risk domain were also ob-served, where reported.
Impairment DomainSignicant improvements in symptoms with ICSs com-pared with placebo were evident as mean reductions insymptom scores and increased numbers of days freefrom asthma (symptoms) or “episode-free days.” 18,29,33–43
In young children ( 30 months old), signicantly lessdaytime and nighttime wheezing ( P .05 and P .01,respectively) were reported with BIS versus placebo, but
the specic scores and/or between-treatment changeswere not provided. 35 A similar population had signicantincreases in the percentage of days without cough ( P .011) or wheeze ( P .002) when treated with FP. 37
Improvements in symptoms were maintained with long-term treatment ( 2 years). 18,29,33
The symptom improvements were observed regard-less of the patient’s therapy before randomization. Insome studies, patients were allowed to use their regularasthma medications (including ICSs) up to the point ofrandomization; other studies were conducted in steroid-naive patients or required a steroid-free run-in periodbefore trial entry. In the studies reported by Baker et al 34
(1999) and Peden et al 41 (1998), children were permittedto use their regular asthma medications through therun-in period; in these studies, 31% and 45% of chil-dren used ICSs up to random assignment to BIS andFP, respectively. Shapiro et al 43 (2001) specicallyevaluated the ability of once-daily (qd) budesonide tomaintain asthma control in children who had beenpreviously receiving ICSs; all children used theirmaintenance ICSs up to random assignment, and 87%were using ICSs twice daily (bid). In most studies, allcontroller medications were withdrawn before ran-dom assignment. However, Chen et al 33 (2006) re-ported a subanalysis of data for 5- to 10-year-olds inthe Steroid Treatment as Regular Therapy (START)
trial, a 3-year study in which budesonide was added tothe usual care of patients diagnosed with mild asthmawho had not regularly used ICSs. 32,33 Added medica-tions were tracked, but changes in usual care medica-tions were not. 32,33
Concomitant with fewer symptoms, ICS use was as-sociated with signicant reductions in daily and/or as-needed (prn) SAB. 29,34,36–43 de Blic et al 35 (1996) observeda slightly shorter duration of nebulized albuterol in in-fants treated with BIS compared with placebo, but thedifference was not statistically signicant. Although useof prn SAB was not reported, young children treatedwith FP for 2 years required less added controller med-ication (montelukast [ P .001] or additional FP [ P .001]) than placebo-treated children. 18 A similar trendwas observed in older children treated with budesonidefor 3 years in the START trial; again, specic use of prnSAB was not reported. 33
It is difcult to make comparisons between the stud-ies regarding degree of symptom improvement becauseof differences in populations and study design. Presum-ably, for the patients who used ICSs through the run-inperiod, any statistically signicant between-treatmentdifferences resulted from deterioration of asthma control
TABLE 5 Suggestions for Reducing the Potential for Adverse Effectsof ICSs in Children1
Use the lowest dose of ICS that maintains asthma controlUse spacers or valved holding chambers with non–breath-activated metered-
dose inhaler to reduce local adverse effectsAdvise patients to rinse their mouths and spit after inhalationMonitor growthControl comorbid conditions (allergic rhinitis, sinusitis, obesity, gastroesophageal
reux disease)Review age-appropriate dietary intake of calcium and exercise with the child’s
parents/caregiversWhen considering an increase in ICS dose
Evaluate patient adherenceAssess inhaler techniqueReview environmental factors (allergen and irritant triggers) that may
contribute to asthma severityConsider adding an LABA or leukotriene receptor antagonist to a low or
medium dose of ICS rather than using a higher dose of ICS
TABLE 6 Summary of ICSs and Linear Growthin Children Based onthe Opinion of the ExpertPanel 1
Summary Statements Supporting Findings
The potential risks of ICSsare well balanced bytheir benets
The efcacy of ICSs is sufcient to outweighconcerns about growth (or othersystemic effects)
Studies in which growth has been carefullymonitored suggest that the growth-velocity effect of ICSs occurs in the rstseveral months of treatment and isgenerally small and nonprogressive
ICSs should be titrated to the lowest dosethat maintains good control of thechild’s asthmaa
Growth rates are highlyvariable in children
Short-term evaluations may not bepredictive of nal adult height
Poorly controlled asthma may delay growthIn general, children with asthma tend to
have longer periods of reduced growthrates before puberty (boys more thangirls)
The potential for adverse
effects of ICSs onlinear growth seemsto be dose dependent
Use of a low-to-medium dose of ICSs for
children with mild or moderatepersistent asthma may be associatedwith a possible, but not predictable,adverse effect on linear growth, which isusually lost after 1 y
High doses of ICSs have greater potentialfor growth suppression
Use of high doses of ICSs for children whohave severe persistent asthma hassignicantly less potential for an adverseeffect on linear growth than use of OCSs
a Nospecicrecommendations forclinical cutoffs aremadein theEPR3. However,my approachinpractice isto (1)reducetheICS dose ifthereisslowingof growthat the3-monthvisitandthechild’sasthmais stable and(2) stopICSs andconsider changingthe medication or the device if the child is still not growing after 6 months.
358 RACHELEFSKYby on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 8/16
TABLE 7 Effectof ICSs on Impairment and Risk in Children With Asthma Evaluatedin Double-Blind, Placebo-ControlledStudiesStudy Study Design and
TreatmentChildren Impairment Risk
Study duration 1 yBaker et al34 (1999) DBPC, 12 wk N 481, 6 mo to 8 y
(mean: 4.7 y)BIS: 0.25 mg qd/0.25 mg bid/
0.5 mg bid/1.0 mg qdFEV1 (L/min; 33% could perform): BIS:
0.07/0.08/0.17 (P .05)/0.11; Pl:0.04
BIS 0.25 mg qd (n 94);0.25 mg bid (n 99);0.50 mg bid (n 98);1.0 mg qd (n 95)
Moderate asthma (31% hadused ICSs 2 mo)
DT symptom score: BIS: 0.28/0.40 (P .05)/ 0.46
(P .01)/ 0.37(P .05);Pl: 0.19
Patients who discontinued treatmentbecause of disease exacerbation(most required OCSs): BIS: 21%(P .011)/21% (P .011)/19%(P .011)/31%; Pl: 39%
Pl (n 95) FEV1 %Pred: 79.6 NT symptom score: BIS:0.28/0.49 (P .001)/ 0.42
(P .01); Pl: 0.13
AE:
Used meds until trial start(through a 2- to 3-wk BL)
Albuterol days/14 d: BIS: 4.4/5.2/4.9/4.4 (P .01 for all);Pl: 2.4
Corticotropin-stimulated cortisol: NS
de Blic et al35 (1996) DBPC, 12 wk, BIS 1 mg bid(n 20)
N 38, 6–30 mo (mean:16.4–18.1 mo)
BIS associated with less DTwheeze (P .05) and lessNT wheeze (P .01) datanot provided
Children with 1 exacerbation: BIS:40% (P .01); Pl: 83%
Pl (n 18) Recurrent severe asthma (3exacerbations of Median of total treatment timeduring which nebulized SAB Children with no exacerbation: BIS:55% (P .05); Pl: 8%dyspnea in 12 previousmo; 1 exacerbation permonth required steroidsfor 3 mo before orpersistent symptom for15 d before entry)
was needed: BIS: 5.2%; Pl:8.8%
Median of total treatment timeduring which an OCS was needed:BIS: 0% (P .05); Pl: 14.5%
Hoekstra et al38 (1996) DBPC, 12 wk N 34, 8–14 y (mean:10.8 y)
Morning wheezing: FP: 0.14(P .006); Pl: 0.08
FEV1 averaged 9% higher with FP(P .0005) data not provided
FP 100 g bid (n 15); Pl(n 19)
Allergic asthma requiringmaintenance therapy,which was discontinued4 wk before trial
Evening wheezing: FP: 0.21(P .004); Pl: 0.10
AE:
FEV1 %Pred: 88–92 FP associated with lessalbuterol (P .05) data notprovided
Urine cortisol: 57% lower with FP(P .009) but change withingroup from BL was NS
School absences: NSKemp et al36 (1999) DBPC, 12 wk N 359, 6 mo–8 y (mean:
4.8 y)BIS: 0.25/0.5/1.0 mg FEV1 (L/min, 36% could perform): BIS:
0.01/ 0.03 (P .044)/ 0.03(P .033); Pl: 0.07
BIS 0.25 mg qd (n 91);0.5 mg qd (n 83); 1.0mg qd (n 93)
Mild persistent asthma,steroid naive
DT symptom score: BIS: 0.57/0.46/ 0.50 (P .05 for
all); Pl: 0.26
AE:
Pl (n 92) FEV1 %Pred: 81.4 NT symptom score: BIS:0.49/0.42/ 0.42 (P .05 for
all); Pl: 0.16
Corticotropin-stimulated cortisol: NS
albuterol days/14 d: BIS: 6.3/6.3/ 6.0 (P .038 for all);Pl: 4.2
LaForce et al (2000(39)
DBPC, 12 wk 52 wk OLextension
N 242, 4–11 y (mean:8.6 y)
FP 200/100 g FEV1 %Pred: FP: 6.5 (P .05)/12.2(P .05); Pl: 1.5
FP DPI 200 g qd (n84); 100 g bid (n80)
Mild-to-moderatepersistent asthma: 57%used ICSs or CROM, 43%used only SAB beforestudy
Awakenings night: FP: 0.04/0.06 (P .05); Pl: 0.04
FEV1 (L): FP: 0.13 (P .05)/0.23 (P .05); Pl: 0.04
Pl (n 78) FEV1 %Pred: 70–73 Symptom score: FP: 0.24(P .05)/ 0.28 (P .05);Pl: 0.01
AE:
2 wk BL on Pl only Albuterol puff per day: FP:0.5/ 0.7; Pl: 0
Morning plasma cortisol: NS
PEDIATRICS Volume 123, Number 1, January 2009 359by on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 9/16
TABLE 7 ContinuedStudy Study Design and
TreatmentChildren Impairment Risk
Nayak et al40 (2002) DBPC, 12 wk N 353, 5–12 y (mean:8.9–9.4 y)
BDP HFA 80/160 g FEV1 % change (absolute): BDP: 13.3/14.5 (P .01 for both); Pl: 5.7
BDP HFA 80 g/d (n120); 160 g/d (n117)
Moderate, symptomaticasthma; SAB prn onlybefore study
Days free from asthmasymptom: BDP: 3.8%/3.9%(P .05); Pl: 3.9 %
FEV1 %Pred: BDP: 9.2/10 (P .01 forboth); Pl: 3.9
Pl (n 116) FEV1 %Pred: 71.0–72.3 BDP 160g associated with AE:less daily SAB (P .05)data not provided
Morning plasma cortisol: NS
Peden et al41 (1998) DBPC, 12 wk N 437, 4–11 y FP 50/100 g FEV1 %change (absolute): FP: 15.77–17.93 (P .05 for all); Pl: 6.96
FP DPI 50 g bid (n181); 100 g bid (n170) (given byDiskhaler and Diskus)
Mild-to-moderate asthma:before study 45% usedICSs, 9% CROM, 46% SABonly
Symptom score: FP: 0.36 to0.41 (P .05 for all); Pl:0.02
FEV1 %Pred: FP: 11.25–12.74 (P .05for all); Pl: 4.72
Pl (n 86) FEV1 %Pred:72–74 Awakenings per night: FP:0.03 to 0.06 (P .05 for
all); Pl: 0.07
AE:
Treatment continued Albuterol puffs per day: FP: Morning plasma cortisol: NSduring 2-wk BL 0.75 to 1.04(P .05 for
all); Pl: 0.08
Urine cortisol: NS
Roorda et al37 (2001) DBPC, 12 wk (pooled datafrom 2 studies)
N 305, 12–47 mo (mean:28.5 mo)
Signicant improvements withFP in children who hadfrequent symptoms:
Exacerbation-free patients: FP: 75%(P .033); Pl: 64%
FP 100 g bid (n 153) Documented history of recurrent wheeze orasthma symptom;symptom on at least 7 of last 14 d of 4 wk RI (noICSs)
Days and nights with nosymptom: FP: 45 (P .005);Pl: 25
Pl (n 152) Separated into 2 groups:those with symptoms
Days with no cough: FP: 56%(P .011); Pl: 42%
3 d/wk and 75% of RI days (n 169) and
Days with no wheeze: FP: 92%(P .002); Pl: 80%
those with less-frequentsymptoms (n 127)
Days with no rescue meds: FP:80% (P .048); Pl: 71%
Shapiro et al42 (1998) DBPC, 12 wk N 178, 4–8 y (mean:6.7 y)
BIS 0.25/0.5/1.0 mg FEV1 (L/min): BIS: 0.05/0.08 (P .05)/0.07; Pl: 0.01
BIS 0.25 mg bid (n 47);0.5 mg bid (n 42);1.0 mg bid (n 45)
Moderate-to-severeasthma, maintained onICSs
DT asthma score: BIS: 0.45(P .05)/ 0.53 (P .01)/
0.55 (P .01);Pl 0.11
Patients requiring OCSs: BIS: 11%/5%/18%; Pl: 36%
Pl (n 44) FEV1 %Pred: 79.6 NT asthma score: BIS:0.36/0.37/ 0.36 (P .05 for
all); Pl: 0.08
AE:
2 wk BL on Pl only All doses of BIS wereassociated with less use of albuterol (P .032) datanot provided
Corticotropin-stimulated cortisol: NS
Shapiro et al (2001(43)
DBPC, 12 wk N 274, 6–17 y (mean:12.1 y)
Budesonide 200/400 g FEV1 %Pred: budesonide: 2.65 (P .015)/3.29 (P .005); Pl: 1.49
Budesonide 200 g qd(n 90); 400 g qd(n 93)
Moderate-to-severeasthma, maintained onICSs 16 wk
DT asthma score: budesonide:0.03/ 0.12 (P .001 for
both); Pl: 0.19Pl (n 91) FEV1 %Pred: 76.6–77.5 NT asthma score: budesonide:
0.12/ 0.11 (P .001 forboth); Pl: 0.14
Used ICSs through BL up torandomization totreatment
Albuterol puff per day:budesonide: 0.69/ 0.70(P .001 for both); Pl: 0.39
360 RACHELEFSKYby on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 10/16
in the placebo group rather than substantial increases inasthma control with the ICSs. However, no subanalyseswere performed, leaving this to speculation.
Risk DomainEight of the ten 12-week studies reported pulmonaryfunction test results. 34,36,38–43 In all cases, children treatedwith ICSs had small but signicant increases in FEV 1
compared with placebo-treated children regardless ofICS use before random assignment.
Two of the long-term studies included children who wereable to perform spirometry: CAMP and START. In both stud-ies, ICS use was associated with slight improvements in FEV 1
in therst year that gradually decreasedthroughout thetreat-ment period so that no signicant between-treatment differ-ences were evident at trial end. 29,32,33
TABLE 7 ContinuedStudy Study Design and
TreatmentChildren Impairment Risk
Study duration 1 yCAMP29 (2000)
(budesonide andDBPC, 4–6 y N 519, 5–12 y (mean:
8.9 y)Symptom score: budesonide:
0.44 (P .005); Pl: 0.37FEV1 : NS
matching placeboarms)
Budesonide 200 g bid(n 311)
Mild-to-moderate asthma(symptoms or SAB 2/wk)
Episode-free d/mo:budesonide: 11.3 (P .01);Pl: 9.3
No./100 child-years:
Pl (n 208) FEV1 %Pred: 93.4–94.2 NT awakenings/mo: NS Prednisone course: budesonide: 70(P .001); Pl: 122
38% used ICSs in 6 mobefore study; stopped all
Albuterol puffs per week:budesonide: 7.4 (P
Urgent care visits: budesonide: 12(P .001); Pl: 22
asthma meds except prnSAB 28 d before
.001); Pl: 5.3 Hospital izations: budesonide: 2.5(P .04); Pl: 4.4
randomization AE:Increase in height: budesonide: 22.7
cm (P .005); Pl: 23.8 cmChen et al33 (2006);
Pauwels et al32
(2003); Weiss et al44
(2006) START in
early asthma(pediatric arms)
DBPC, 3 y followed by 2 yOL
N 1974, 5–10 y (mean:8.4 y);N 1221, 11–17 y
Subanalysis of 5–10 y:Symptom-free d/y:
budesonide: 964 (P .001);Pl: 948
FEV1 %Pred (at 1 y/at 3 y): 5–10 y:budesonide: 4.35/3.77; Pl: 2.12/2.48; 11–17 y: budesonide: 4.44/3.97; Pl: 2.91/3.54
Usual care budesonide200 g qd (n 1000,5–10 y), budesonide400 g qd (n 640,11–17 y), Pl (n 974,5–10 y; 581, 11–17 y)
Mild, persistent asthma for3 mo and 2 y beforeentry
FEV1 %Pred: 85%–85.5%(for 5–10 y)
No ICSs 30 d
Patients requiring intervention:with other ICSs: budesonide:13.6% (P .01); Pl: 24.8%;with OCSs: budesonide:1.1%; Pl: 2.5%; with SAB:budesonide: 60.9%; Pl:65.9%
Subanalysis of 5–10 y:
Hospitalizations: budesonide: 34; Pl:53
ED visits: budesonide: 18; Pl: 29Hazard ratio for risk of an SARE: 0.60
(P .012); risk reduction 40%AE:Difference in growth rate per year vs
Pl: budesonide 200 g (5–10 y):0.43 cm (P .0001);
budesonide 400 g (11–17 y):0.40 cm (P .003)
Guilbert et al18 (2006) DBPC, 2 y followed by 1 ywithout treatment
N 285, 2–3 y (mean: 3 y) Episode-free days: FP: 93.2%;Pl: 88.4% (P .006)
No./100 child-years:
Prevention of EarlyAsthma in Kids(PEAK)
FP 88 g bid (n 143) At high risk for asthma( API); 66%–67% hadED visit for asthmaexacerbation and 10%were hospitalized inprevious year
Bronchodilator use: FP: 14.4d/y; Pl: 18.0 d/y
Exacerbations requiring OCSs: FP:57.4 (P .001); Pl: 89.4
Pl (n 142) 4 mo ICSs; no ICSs inmonths before
Supplemental use of FP: FP: 8.3d/y (P .001); Pl: 17.6 d/y
Hospitalizations: FP: 1.05; Pl: 1.76
treatment (RI) Montelukast use: FP: 11.4 d/y AE:(P .001); Pl: 24.2 d/y Increase in height over 2 y: FP: 12.6
cm (P .001); Pl: 13.7 cm
FEV1 is prebronchodilator; all outcomes are reported as “change from BL” unless otherwise indicated; signicance is versus placebo unless otherwise indicated. BL indicates baseline; CROM,cromolyn sodium; DBPC, double-blind, placebo-controlled; DT, daytime; HFA, hydrouoroalkane; MDI, metered-dose inhaler; NEB, nebulized; NS, not signicant; NT, nighttime; OL, open label; placebo; RI, run in; %Pred, percent predicted; API, Asthma Predictive Index.
PEDIATRICS Volume 123, Number 1, January 2009 361by on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 11/16
Five studies assessed exacerbations or worsening ofasthma requiring a short course of OCSs. 18,29,35,40,42 Chil-dren treated with ICSs required signicantly fewer
courses of OCSs regardless of whether they were 5 or5 years old. 18,29,35 Although signicance was not noted,
2 studies reported more OCSs for “worsening asthma” in
TABLE 8 Effectof ICSs on Impairment and Risk in Children With Asthma Evaluatedin Controlled Comparator TrialsStudy Study Design and Treatment Children Impairment Risk
Study duration 1 yOstrom et al45 (2005) DBDD, 12 wk N 342, 6–12 y (mean: 9.1–
9.6 y)DT asthma score: FP: 0.81;
montelukast: 0.75FEV1 (change): FP: 10.62% (P .002);
montelukast: 4.60%Montelukast 5 mg qd (n 170) SAB use only before study NT asthma score: FP:0.4 (P
.001); montelukast: 0.19% patients with 10% improvement
in FEV1:FP DPI 50 g bid (n 172) FEV1 %Pred: 75.4–76.4 Albuterol puffs per day: FP:
1.43 (P .018);montelukast: 1.23
BL FEV1 %Pred 75%: FP: 35 (P .031); montelukast: 18
NT albuterol use: FP: 0.39 (P .001); montelukast: 0.21
BL FEV1 %Pred 65–75: FP: 65 (P .007); montelukast: 42
Symptom-free days: FP: 37.7%;montelukast: 31.3%
Patients who withdrew because of asthma exacerbation: FP: 5.2%;
Rescue free days: FP: 45.1% (P .002); montelukast: 35%
montelukast: 8.2%
Sorkness et al31 (2007) DBDD, 48 wk N 285, 6–14 y (mean: 9.6–10.3 y)
Pl vs montelukast: FEV1 %Pred: FP: 6.32 (P .001); FP/salmeterol: 3.62 (P .01);montelukast: 0.58
Pediatric AsthmaController Trial(PACT)
FP 100 g bid (n 96) Mild-to-moderate asthma; nocontroller medications 2wk before randomization
Asthma-control days: FP: 64.2%(P .004); FP/salmeterol:59.6%; montelukast: 52.5%
Time to rst prednisone burstfavored FP vs montelukast (P .002)
FP/salmeterol 100/50 g AMsalmeterol 50 g PM(n 94) FEV1 %Pred: 96.8–97.8 Episode-free days: FP: 26.4%(P .04);FP/salmeterol:26.8% AE:
Montelukast 5 mgPM(n 95) (P .032); montelukast:17.8%
Increase in height: NS
Szeer et al46 (2005);Zeiger et al47
DMCO, 16 wk (2–8 wktreatment periods)
N 144, 6–17 y Asthma-control d/wk: FP: 5 (P .001); montelukast: 4.3
FEV1 % change (absolute): FP: 6.8(P .001); montelukast: 1.9
(2006) FP 100 g bid Mild-to-moderate asthma, prnSAB only before study
Albuterol puffs per week: FP: 3.1(P .031); montelukast: 4.4
No. of patients with exacerbationsrequiring OCSs (treatment
Montelukast 5–10 mg qdPM FEV1 %Pred: 88–99 failures): FP: 2; montelukast: 10(P .019)
Study duration 1 yCAMP29 (2000) DBPC, 4–6 y N 1041, 5–12 y (mean: 8.9 y) Symptom score: budesonide:
0.44 (P .005); NED: 0.38;Pl: 0.37
FEV1: NS
Budesonide 200 g bid (n311)
Mild-to-moderate asthma:symptoms or used SAB
2 /wk
Episode-free d/mo: budesonide:11.3 (P .01); NED: 9.3; Pl: 9.3
No./100 person-years:
NED 8 mg bid (n 312) FEV1 %Pred: 93.4–94.2 Night awakenings per month: NS Prednisone course: budesonide: 70(P .001); NED: 102 (P .01); Pl:122
Matching Pl for budesonide/NED (n 208/210)
38% used ICSs in 6 mobefore study; stopped meds
Albuterol puffs per week:budesonide: 7.4 (P .001);
Urgent care visits: budesonide: 12(P .001); NED: 16 (P .02); Pl:22
except prn SAB 28 dbefore randomization
NED: 6.7; Pl: 5.3 Hospitalizations: budesonide: 2.5(P .04); NED: 4.3; Pl: 4.4
AE:Increase in height: budesonide: 22.7
cm (P .005); NED: 23.7; Pl: 23.8cm
Garcia et al30 (2005)Montelukast Study
DBDD, 12 mo N 994, 6–14 y (median: 9 y) Rescue-free days: FP: 25.2%;montelukast: 22.4%
FEV1
%Pred: FP: 2.7 (P .004);montelukast: 0.6
of Asthma in Montelukast 5 mg qd (n 495) Mild, persistent asthma Days with SAB use: FP:25.4% FEV1 (L): FP: 0.30; montelukast: 0.27Children (MOSAIC) FP DPI 100g bid (n 499) FEV1 %Pred: 86.8 (P .003); montelukast:
22.7%Patients using OCSs: FP: 10.5% (P
.001); montelukast: 17.8%Asthma controller meds AE:
stopped during 4-wk RI Growth rate (cm/y): FP: 5.81 (P .018); montelukast: 6.18
FEV1 isprebronchodilator;all outcomesare reportedas “changefrom BL” unless otherwiseindicated;signicance isversus placebo unless otherwiseindicated.BL indicatesbaseline;CO, cross-over;DBPC, double-blind, placebo-controlled; DD, double dummy; DM, double masked; DT, daytime; MDI,metereddose inhaler;NS, not signicant; NT, nighttime; Pl, placebo; RI, runin; %Pred, percentpredicted.
362 RACHELEFSKYby on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 12/16
school-aged children treated with placebo or usual carecompared with budesonide. 33,42 More infants and pre-schoolers ( 48 months old) were “exacerbation-free”with FP treatment compared with placebo treatment(P .033). 37
Nayak et al 40 (2002) noted a trend toward later onsetof “time to rst exacerbation” with hydrouoroalkane-BDP, but statistical signicance was not reached. Theaddition of qd budesonide to usual care was associatedwith a signicant increase in the time to rst severeasthma-related event (SARE) in children between 5 and10 years of age in the START trial. 33 The risk of an SAREdecreased by 40% with the addition of budesonide tousual care (hazard ratio: 0.60; P .012). 33
Children treated with budesonide had signicantlyfewer hospitalizations and urgent care visits than pla-cebo-treated children during the 4 to 6 years of theCAMP. 29 Fewer hospitalizations were also reported dur-ing 2 years of FP, although statistical signicance was notachieved. 18 In the START trial, adding budesonide tousual care was associated with a 50% reduction in hos-
pitalizations and a 34% decrease in emergency visitsover 3 years; statistical signicance was approached butnot achieved. 33,44 Additional comparisons are difcultbecause of differences between studies in both designand study population.
All ICSs used in these studies were well tolerated, andthere were no serious AEs related to any of the studymedications. Seven studies evaluated hypothalamic-pi-tuitary-adrenal axis function. 34,36,38–41,43 No ICS-specicchanges were observed except for a small decrease inurinary cortisol reported in some children treated withFP who had previously used ICSs. 38
No changes in growth with ICSs were reported in two
12-week studies.34,35
However, small decreases in growthwith ICSs were reported in the 3 long-term studies. 18,29,32
Compared with usual care alone, children treated withbudesonide showed a reduction in growth of 0.43 cm/year ( P .001) in the START trial regardless of dosing at400 or 200 g/day. 32 In the CAMP, the mean increase inheight was also lower (by 1.1 cm) with budesonide. 29
The long-term study of FP showed a small but signicantdifference in height percentiles after 2 years (FP: 51.5%;placebo: 56.4% [ P .001]). 18 Where assessed, thesechanges in growth rates were predominant during therst year of treatment, and all groups had similar rates ofgrowth at the end of the treatment periods. 18,29
“Catch-up growth” was not evaluated. No other sys-temic effects were observed in these studies.
Controlled Comparisons With Nonsteroid AntiinammatoryMedicationsFive placebo-controlled studies comparing an ICS to anonsteroid antiinammatory medication are describedin Table 8. 29–31,45–47 These studies included 2806 children:1222 were exposed to ICSs (budesonide, 200 g bid [ n311]; FP, 50–100 g bid [ n 908]), and 1216 receivedcomparator nonsteroid medications (NED, 8 mg bid [ n312]; montelukast, 5–10 mg qd [ n 904]). The CAMPincluded matching placebos for budesonide and NED(n 418). 29 In addition, 1 of the trials comparing FP and
montelukast included a third group of children whowere treated with the combination of FP and salmeterol,100 g/50 g in the morning and salmeterol alone, 50
g, in the evening. 31
Each trial was unique, which makes comparisons dif-cult. Treatment duration ranged from 12 weeks to 6years. The inhaled medications were given twice daily;montelukast (tablet or sprinkles) was given once perday, usually in the evening. All children were only usingan SAB at random assignment.
Overall, treatment with ICSs improved measuresof impairment and risk to a greater extent than thenonsteroid antiinammatory medications.
Impairment DomainImpairment was evaluated by symptom scores, episode-free days (or asthma-control days), and rescue-medica-tion use. Compared with montelukast, FP-treated pa-tients had more asthma-control days, episode-free days,and rescue-free days. 30,31,45,46 Ostrom et al 45 (2005) alsoreported signicant reductions in nighttime asthmasymptoms ( P .001) and rescue albuterol use ( P .018)with FP compared with montelukast.
In the CAMP, both NED and budesonide improvedasthma symptoms, episode-free days, and albuterol usecompared with placebo treatment. 29 Differences be-tween the active treatments did not reach statistical sig-nicance, but the clinical improvements were consis-tently greater with budesonide; only budesonideattained statistical signicance compared with placebo. 29
Risk DomainThe 5 studies included FEV 1 , and signicant increaseswith the ICSs versus the nonsteroid antiinammatorymedication were evident in all except the CAMP. 29–31,45–47
Improvements in asthma exacerbations favored FPover montelukast when measured as the time to rstprednisone burst ( P .002) 31 or worsening of asthmarequiring a short course of OCSs ( P .019; P .001). 30,46
Compared with placebo, both budesonide and NED sig-nicantly reduced the number of prednisone courses per100 person-years and the number of asthma-related ur-gent care visits. 29 The decreases were greater with budes-onide, but the differences were not statistically signi-cant. Only budesonide signicantly decreased thenumber of asthma-related hospitalizations. 29
All treatments in the comparator studies were welltolerated, with no signicant between-treatment differ-ences for AEs and no serious AEs related to any of thestudy drugs. Small reductions in growth rates were ob-served with ICSs versus the comparator medications inthe 2 long-term studies. 29–31 No other systemic effectswere observed.
SUMMARYChildren with asthma remain a signicant challenge,particularly as the relationship between early treatmentof asthma symptoms and the development of adult dis-ease is not yet clearly delineated. ICSs are recommendedas the primary controller medication for children (as
PEDIATRICS Volume 123, Number 1, January 2009 363by on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 13/16
well as adults) with asthma. The efcacy and safety ofICSs to treat children has been well documented, al-though the data are more limited than for adults. 1 Whenused at indicated doses, ICSs are safe. However, efcacywith dose plateaus; thus, when a child is symptomatic, itmay be better to add another medication rather thanincrease the dose of ICSs beyond medium. 1 Discussion ofwhat to add is beyond the scope of this article. Theevidence reviewed in the EPR3 suggests that the addi-tion of a long-acting bronchodilator (LABA) providesgreater asthma control than increasing the dose of ICSsor adding a leukotriene modier. 1 However, adjunctivetherapy for children between 5 and 11 years of age hasnot been well studied, and data are lacking for youngerchildren. 1 The reader is directed to the EPR3, 1 and otherresources for parents of children with asthma may behelpful. 48
The National Asthma Education and Prevention Pro-gram guidelines continue to serve as a basis for treat-ment recommendations; the latest report describes anew paradigm targeting asthma control through the do-
mains of impairment and risk. 1 This systematic reviewstrengthens previous evidence (reported in the EPR2and clinical practice guidelines) supporting the safe andeffective use of ICSs to treat children with asthma. Inaddition, the data provide new evidence linking ICS usein children with asthma to improved asthma control asnow dened by the EPR3 according to the domains ofrisk and impairment. Data from placebo-controlled stud-ies conrm that treatment with ICSs improves bothdomains in children (0–17 years old). 18,29–43,45–47
1. Compared with placebo, ICS treatment was associ-ated with reductions in the impairment domain re-ported as symptoms scores, specic symptom epi-sodes, episode-free days (or asthma-control days),rescue-free days, and/or rescue-medication use.
2. Compared with placebo, ICS treatment was associ-ated with reductions in the risk domain evident asincreased FEV 1 (in children able to perform spirom-etry), fewer courses of OCSs, decreased exacerbationrates, and/or less use of urgent care services.
3. The reductions in the impairment and risk domainsobserved with ICSs were generally greater than re-ductions observed with nonsteroid antiinammatorycomparator medications.
4. ICSs were well tolerated in all studies.
5. Small reductions in growth rates compared with pla-cebo and/or comparator nonsteroid antiinammatorymedications were evident in several long-term ( 1-year) studies. 18,29–32 These changes decreased withtime, and the clinical signicance is unclear. Otherdata suggest that asthmatic children treated with ICSsattain their full adult height despite initial reductionsin growth rates. 29,49
More in-depth comparisons are difcult to make becauseof differences in study protocols.
Additional studies that use appropriate indicators forimpairment and risk are warranted. For impairment,
rescue-medication use, daytime and nighttime symptomscores, and asthma/episode-free days are recommendedas indicators. For risk, FEV 1 should be reported for chil-dren who can perform spirometry; exacerbations thatrequire OCSs and urgent care usage are also suggested asindicators. Attention should be given to standardizingvariables that can be used to compare outcomes betweentrials.
The majority of pediatric data are for children 12years; only 5 of the 18 studies included adolescents(13–18 years old). 30,31,38,43,46 Data for this population arelost when assessing childhood asthma, either groupedwith adults (eg, studies in patients 12 years old) or notincluded (eg, studies of school-aged children 12 yearsold). More studies are needed to evaluate whether diag-nosing asthma and starting therapy early affects thecourse of the disease in adolescence. More information isalso needed to assess how treatment can better meet theneeds of the adolescent patient.
The evidence presented in this systematic retrievaland review of the literature is not ranked, because this is
the work of a single author and not a committee. How-ever, the studies chosen were separated according todesign: double-blind, placebo-controlled studies andrandomized, controlled, comparison trials. No nonran-domized trials or observational studies were included.Thus, all of the data collected in this review would fallinto category A and B evidence according to the deni-tions in the EPR3. 1
Asthma is a complex and heterogeneous disease.Many factors affect impairment and risk and inuencechoice of therapy. Not addressed in this article but ofsignicant impact are adherence with treatment, envi-ronmental control, comorbid conditions, differences in
delivery devices, and penetration of medication into thesmall airways. The reader is directed to the EPR3 foradditional information. 1
In summary, the available data indicate that ICSsimprove asthma control in children by reducing bothimpairment and risk associated with the disease andsupport current recommendations for treatment.
ACKNOWLEDGMENTS
This work was funded partially by an unrestricted edu-cational grant from Teva Pharmaceuticals.
The expert research and technical support of JudithFarrar, PhD, is greatly appreciated; this publication
would not have been possible without her editorial as-sistance.
REFERENCES1. National Asthma Education and Prevention Program. Expert
Panel Report 3: Guidelines for the Diagnosis and Management of Asthma . Bethesda, MD: National Institutes of Health; 2007.Available at: www.nhlbi.nih.gov/guidelines/asthma. AccessedOctober 30, 2007
2. Centers for Disease Control and Prevention, National Centerfor Health Statistics. Summary health statistics for U.S.children: National Health Interview Survey, 2005. Available at:www.cdc.gov/nchs/data/series/sr 10/sr10 231.pdf. AccessedOctober 25, 2007
364 RACHELEFSKYby on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 14/16
3. Centers for Disease Control and Prevention, National Centerfor Health Statistics. Asthma prevalence, health care use andmortality: United States, 2003– 05. Available at: www.cdc.gov/nchs/products/pubs/pubd/hestats/ashtma03-05/asthma03-05.htm. Accessed October 25, 2007
4. Djukanovic R, Wilson JW, Britten KM, et al. Effect of aninhaled corticosteroid on airway inammation and symptomsin asthma. Am Rev Respir Dis. 1992;145(3):669–674
5. Leung TF, Wong GWK, Ko FWS, et al. Analysis of growthfactors and inammatory cytokines in exhaled breath conden-sate from asthmatic children. Int Arch Allergy Immunol. 2005;137(1):66–72
6. Jarjour NN, Wilson SJ, Koenig Sm, et al. Control of airwayinammation maintained at a lower steroid dose with 100/50microg of uticasone propionate/salmeterol. J Allergy Clin Im-munol. 2006;118(1):44–52
7. Hauber H, Taha R, Bergeron C, Migounov V, Hamid Q, Oliv-enstein R. Effects of hydrouoroalkane and dry powder-formulated corticosteroids on sputum inammatory markers inasthmatic patients. Can Respir J. 2006;13(2):73–78
8. Bousquet J, Ben Joseph R, Messonnier M, Alemao E, GouldAL. A meta-analysis of the dose-response relationship of in-haled corticosteroids in adolescents and adults with mild to
moderate persistent asthma. Clin Ther. 2002;24(1):1–209. Holt S, Suder A, Weatherall M, Cheng S, Shirtcliffe P, Beasley
R. Dose-response relation of inhaled uticasone propionate inadolescents and adults with asthma: meta-analysis. BMJ. 2001;323(7307):253–256
10. Szeer SJ, Martin RJ, King TS, et al. Signicant variability inresponse to inhaled corticosteroids for persistent asthma. J Allergy Clin Immunol. 2002;109(3):410–418
11. Masoli M, Weatherall M, Holt S, Beasley R. Systematic reviewof the dose-response relation of inhaled uticasone propionate.Arch Dis Child. 2004;89(10):902–907
12. Aalbers R, Backer V, Kava TT, et al. Adjustable maintenancedosing with budesonide/formoterol compared with xed-dosesalmeterol/uticasone in moderate to severe asthma. Curr Med Res Opin. 2004;20(2):225–240
13. Boushey HA, Sorkness CA, King TS, et al. Daily versus as-needed corticosteroids for mild persistent asthma. N Engl J Med.2005;352(15):1519–1528
14. Foresi A, Morelli MC, Catena E. Low-dose budesonide with theaddition of an increased dose during exacerbations is effectivein long-term asthma control. On behalf of the Italian StudyGroup. Chest. 2000;117(2):440–446
15. Harrison TW, Oborne J, Newton S, Tatterseld AE. Doublingthe dose of inhaled corticosteroid to prevent asthmaexacerbations: randomised controlled trial. Lancet. 2004;363(9405):271–275
16. Green RH, Brightling CE, McKenna S, et al. Asthma exacerba-tions and sputum eosinophil counts: a randomized controlledtrial. Lancet. 2002;360(9347):1715–1721
17. Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR.Use of exhaled nitric oxide measurements to guide treatmentin chronic asthma. N Engl J Med. 2005;352(21):2163–2173
18. Guilbert TW, Morgan WJ, Zeiger RS, et al. Long-term inhaledcorticosteroids in preschool children at high risk for asthma.N Engl J Med. 2006;354(19):1985–1997
19. Taussig LM, Wright AL, Holberg CJ, Halonen M, Morgan WJ,Martinez FD. Tucson children’s respiratory study: 1980 topresent. J Allergy Clin Immunol. 2003;111(4):661–675
20. Castro-Rodríguez JA, Holberg CJ, Wright AL, Martinez FD. Aclinical index to dene risk of asthma in young children withrecurrent wheezing. Am J Respir Crit Care Med. 2000;162(4 pt1):1403–1406
21. Guilbert TW, Morgan WJ, Zeiger RS, et al. Atopic characteris-tics of children with recurrent wheezing at high risk for the
development of childhood asthma. J Allergy Clin Immunol.2004;114(6):1282–1287
22. Bacharier LB, Phillips BR, Bloomberg GR, et al. Severe inter-mittent wheezing in preschool children: a distinct phenotype. J Allergy Clin Immunol. 2007;119(3):604–610
23. Fabbri L, Burge PS, Croonenborgh L, et al. Comparison ofuticasone propionate with beclomethasone dipropionate inmoderate to severe asthma treated for one year. InternationalStudy Group. Thorax. 1993;48(8):817–823
24. Kamada AK, Szeer SJ, Martin RJ, et al. Issues in the use ofinhaled glucocorticoids. The Asthma Clinical Research Net-work. Am J Respir Crit Care Med. 1996;153(6 pt 1):1739–1748
25. Gustafsson P, Tsanakas J, Gold M, Primhak R, Radford M,Gillies E. Comparison of the efcacy and safety of inhaleduticasone propionate 200 micrograms/day with inhaled be-clomethasone dipropionate 400 micrograms/day in mild andmoderate asthma. Arch Dis Child. 1993;69(2):206–211
26. van Essen-Zandvliet EE, Hughes MD, Waalkens HJ, Duiver-man EJ, Pocock SJ, Kerrebijn KF. Effects of 22 months oftreatment with inhaled corticosteroids and/or beta2-agonistson lung function, airway responsiveness, and symptoms inchildren with asthma. The Dutch Chronic Non-specic LungDisease Study Group. Am Rev Respir Dis. 1992;146(3):547–554
27. Agertoft L, Pedersen S. Short-term knemometry and urinecortisol excretion in children treated with uticasone propi-onate and budesonide: a dose response study. Eur Respir J.1997;10(7):1507–1512
28. Turktas I, Ozkaya O, Ilknur B, Bideci A, Cinaz P. Safety ofinhaled corticosteroid therapy in young children with asthma.Ann Allergy Asthma Immunol. 2001;86(6):649–654
29. Childhood Asthma Management Program Research Group.Long-term effects of budesonide or nedocromil in childrenwith asthma. N Engl J Med. 2000;343(15):1054–1063
30. Garcia Garcia ML, Wahn U, Gilles L, Swern A, Tozzi CA, PolosP. Montelukast, compared with uticasone, for control ofasthma among 6- to 14-year-old patients with mild asthma:the MOSAIC study [published correction appears in Pediatrics .2005;116(4):1058]. Pediatrics. 2005;116(2):360–370
31. Sorkness CA, Lemanske RF, Mauger DT, et al. Long-termcomparison of 3 controller regimens for mild-moderate persis-tent childhood asthma: the Pediatric Asthma Controller Trial. J Allergy Clin Immunol. 2007;119(1):64–72
32. Pauwels RA, Pedersen S, Busse WW, et al. Early interventionwith budesonide in mild persistent asthma: a randomised,double-blind trial. Lancet. 2003;361(9363):1071–1076
33. Chen YZ, Busse WW, Pedersen S, Tan W, Lamm CJ, O’ByrnePM. Early intervention of recent onset mild persistent asthmain children aged under 11 yrs: the Steroid Treatment as RegularTherapy in Early Asthma (START) trial. Pediatr Allergy Immunol.2006;17(suppl 17):7–13
34. Baker JW, Mellon M, Wald J, Welch M, Cruz-Rivera M, Wal-ton-Bowen K. A multiple-dosing, placebo-controlled study of
budesonide inhalation suspension given once or twice daily fortreatment of persistent asthma in young children and infants.Pediatrics. 1999;103(2):414–421
35. de Blic J, Tillie-Leblond I, Tonnei AB, Jaubert F, ScheinmannP, Gosset P. Efcacy of nebulized budesonide in treatment ofsevere infantile asthma: a double-blind study. J Allergy ClinImmunol. 1996;98(1):14–20
36. Kemp JP, Skoner DP, Szeer SJ, Walton-Bowen K, Cruz-Rivera M, Smith JA. Once-daily budesonide inhalation suspen-sion for the treatment of persistent asthma in infants andyoung children. Ann Allergy Asthma Immunol. 1999;83(3):231–239
37. Roorda RJ, Mezei G, Bisgaard H, Maden C. Response of pre-school children with asthma symptoms to uticasone propi-onate. J Allergy Clin Immunol. 2001;108(4):540–546
PEDIATRICS Volume 123, Number 1, January 2009 365by on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 15/16
38. Hoekstra MO, Grol M, Bauman K, et al. Fluticasone propionatein children with moderate asthma. Am J Respir Crit Care Med.1996;154(4 pt 1):1039–1044
39. LaForce CF, Pearlman DS, Ruff ME, et al. Efcacy and safety ofdry powder uticasone propionate in children with persistentasthma. Ann Allergy Asthma Immunol. 2000;85(5):407–415
40. Nayak A, Lanier R, Weinstein S, Stanpone P, Welch M. Efcacyand safety of beclomethasone dipropionate extrane aerosol inchildhood asthma: a 12-week, randomized, double-blind pla-cebo-controlled study. Chest. 2002;122(6):1956–1965
41. Peden DB, Berger WE, Noonan MJ, et al. Inhaled uticasonepropionate delivered by means of two different multidose pow-der inhalers is effective and safe in a large pediatric populationwith persistent asthma. J Allergy Clin Immunol. 1998;102(1):32–38
42. Shapiro G, Mendelson L, Kraemer MJ, Cruz-Rivera M, Wal-ton-Bowen K, Smith JA. Efcacy and safety of budesonideinhalation suspension (Pulmicort Respules in young childrenwith inhaled steroid-dependent persistent asthma. J AllergyClin Immunol. 1998;102(5):789–796
43. Shapiro GG, Mendelson LM, Pearlman DS. Once-daily budes-onide inhalation powder (Pulmicort Turbuhaler) maintainspulmonary function and symptoms of asthmatic children pre-
viously receiving inhaled corticosteroids. Ann Allergy AsthmaImmunol. 2001;86(6):633–640
44. Weiss K, Buxton M, Andersson FL, Lamm CJ, Liljas B, SullivanSD. Cost-effectiveness of early intervention with once-dailybudesonide in children with mild persistent asthma: resultsfrom the START study. Pediatr Allergy Immunol. 2006;17(suppl17):21–27
45. Ostrom NK, Decotis BA, Lincourt WR, et al. Comparativeefcacy and safety of low-dose uticasone propionate andmontelukast in children with persistent asthma. J Pediatr.2005;147(2):213–220
46. Szeer SJ, Phillips BR, Martinez FD, et al. Characterization ofwithin-subject responses to uticasone and montelukast inchildhood asthma. J Allergy Clin Immunol. 2005;115(2):233–242
47. Zeiger RS, Szeer SJ, Phillips BR, et al. Response proles touticasone and montelukast in mild-to-moderate persistentchildhood asthma. J Allergy Clin Immunol. 2006;117(1):45–52
48. Rachelefsky G. Free Your Child From Asthma . New York, NY:McGraw-Hill; 2006
49. Agertoft L, Pedersen S. Effect of long-term treatment withinhaled budesonide on adult height in children with asthma.N Engl J Med. 2000;343(15):1064–1069
FRAUD CHARGES CAST DOUBT ON CLAIMS OF DNA DAMAGE FROM CELL PHONEFIELDS
“The only 2 peer-reviewed scientic papers showing that electromagneticelds (EMFs) from cell phones can cause DNA breakage are at the center ofa misconduct controversy at the Medical University of Vienna (MUV). Criticshad argued that the data looked too good to be real, and in May a universityinvestigation agreed, concluding that data in both studies had been fabricatedand that the papers should be retracted.”
Science . August29, 2008Noted by JFL, MD
366 RACHELEFSKYby on March 14, 2010www.pediatrics.orgDownloaded from

8/7/2019 asma y corticoesteroides
http://slidepdf.com/reader/full/asma-y-corticoesteroides 16/16
DOI: 10.1542/peds.2007-32732009;123;353-366Pediatrics
Gary Rachelefskyand Risk
Inhaled Corticosteroids and Asthma Control in Children: Assessing Impairment
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/123/1/353including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/123/1/353#BIBLat:This article cites 45 articles, 16 of which you can access for free
Rs)3Peer Reviews (PPost-Publication
http://www.pediatrics.org/cgi/eletters/123/1/353R has been posted to this article:3One P
Subspecialty Collections
http://www.pediatrics.org/cgi/collection/asthma Asthma
following collection(s):This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at:Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be fou nd online: