Airway Management (Videos) - Mayur
147
Airway Management Airway Management Presented By: Mayur Jain
-
Upload
drjainmayur1 -
Category
Documents
-
view
102 -
download
0
description
Airway management techniques; their indications, contraindications, advantages and disadvantages.....
Transcript of Airway Management (Videos) - Mayur

Airway ManagementAirway Management
Presented By:
Mayur Jain

Introduction Introduction Difficulty in breathing is one of
the most disconcerting problems for the patient who is conscious yet unable to breath properly. One needs to be aware of the psychological aspect of the patient while management of airway obstruction.
Indications
Indications of Airway ManagementIndications of Airway Management
Maxillofacial traumaAspiration of foreign bodyVasodepressor syncopeAsthmaHeart failureHypoglycemiaOverdose reactionAnaphylaxisEpilepsy
Diagnosis
Diagnosis of Airway Diagnosis of Airway ObstructionObstruction
LOOK : Respiratory movements, gasping , suprasternal retraction
LISTEN: Breath sounds
FEEL : Expired air
DiagnosisDiagnosis of Airway Obstruction of Airway Obstruction
Abnormal sounds in airway obstruction◦Snoring - due to obstruction of upper
airway by the tongue ◦Gurgling - due to obstruction of upper
airway by liquids (blood, vomit) ◦Wheezing - due to narrowing of the
lower airways ◦Complete airway obstruction is silent.
Definition of Airway Definition of Airway managementmanagement
Definition of Airway Definition of Airway managementmanagement
“Airway management involves ensuring that the patient has a patent airway through which effective ventilation can take place.”
PurposePurpose

PurposePurposeDeprived of oxygen; brain death will
occur within minutes. To provide an artificial airway that is
as close to the patient's natural airway as possible along with a continuous source of oxygen.
Anatomy of Respiratory Anatomy of Respiratory SystemSystem
Anatomy of Respiratory Anatomy of Respiratory SystemSystemThe airways can be divided in to parts namely: The upper airway. The lower airway
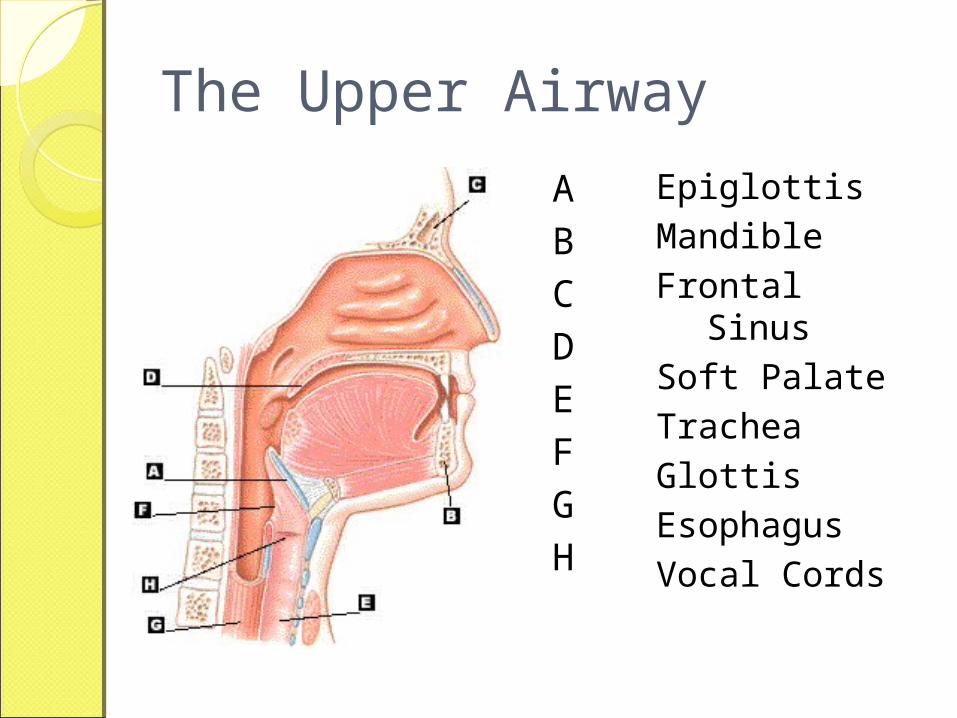
The Upper Airway
EpiglottisMandibleFrontal SinusSoft PalateTracheaGlottisEsophagusVocal Cords
ABCDEFGH
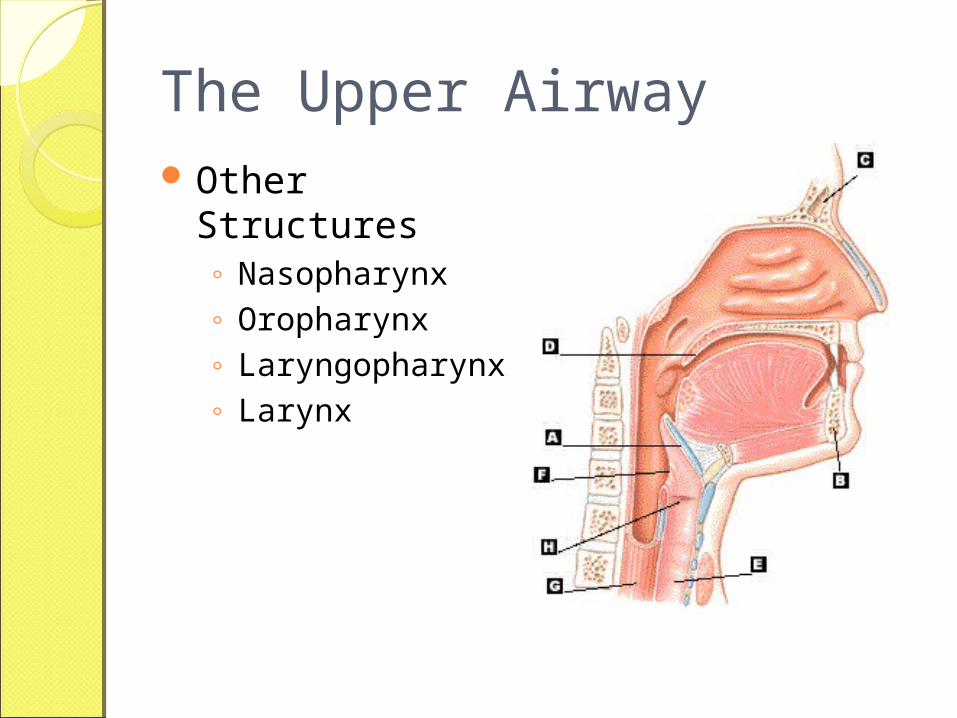
The Upper Airway Other Structures
◦ Nasopharynx◦ Oropharynx◦ Laryngopharynx◦ Larynx
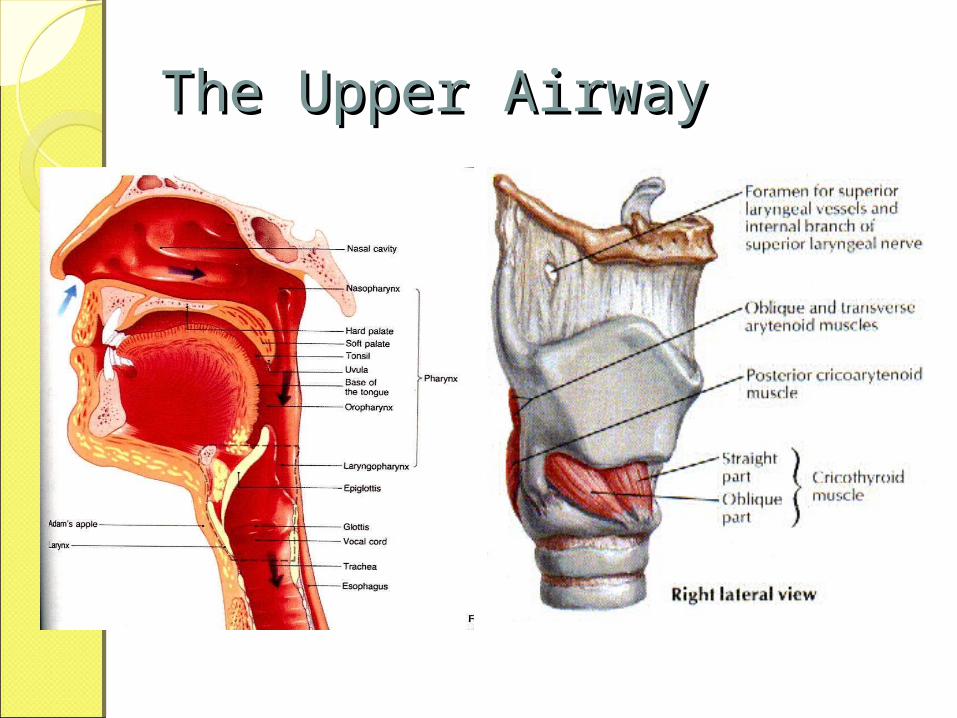
The Upper AirwayThe Upper Airway
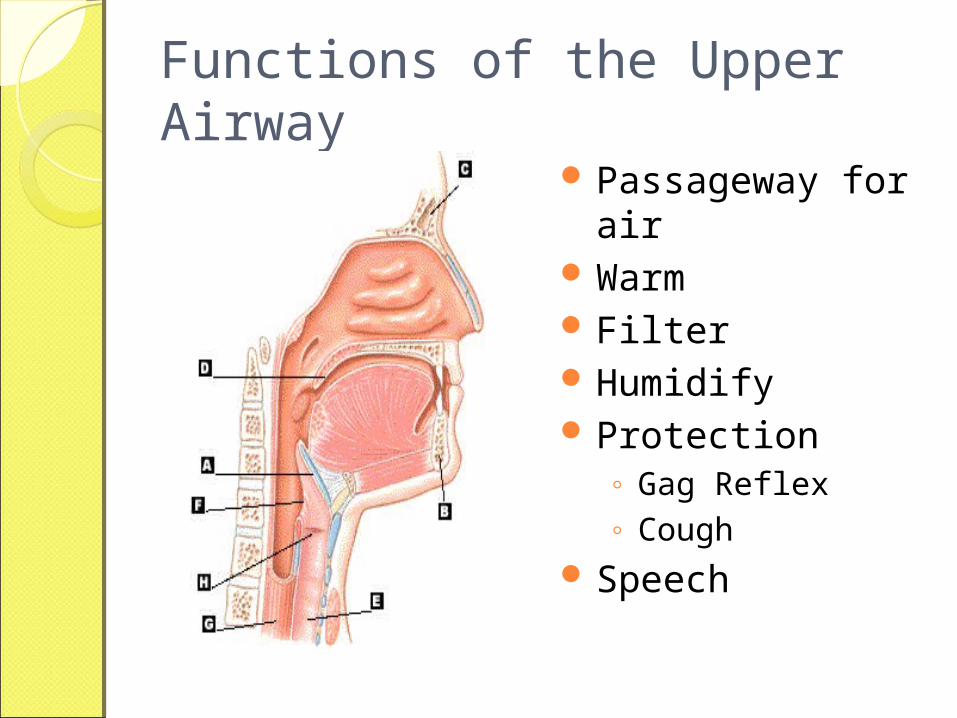
Functions of the Upper Airway
Passageway for air
Warm Filter Humidify Protection
◦ Gag Reflex◦ Cough
Speech
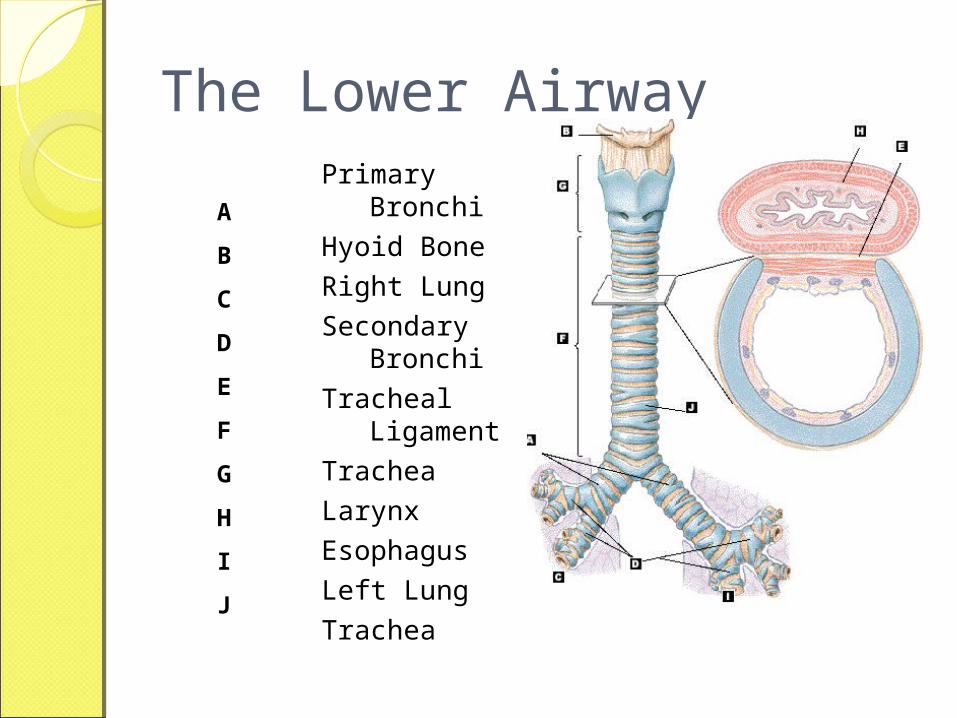
The Lower AirwayPrimary Bronchi
Hyoid Bone
Right Lung
Secondary Bronchi
Tracheal Ligament
Trachea
Larynx
Esophagus
Left Lung
Trachea
A
B
C
D
E
F
G
H
I
J
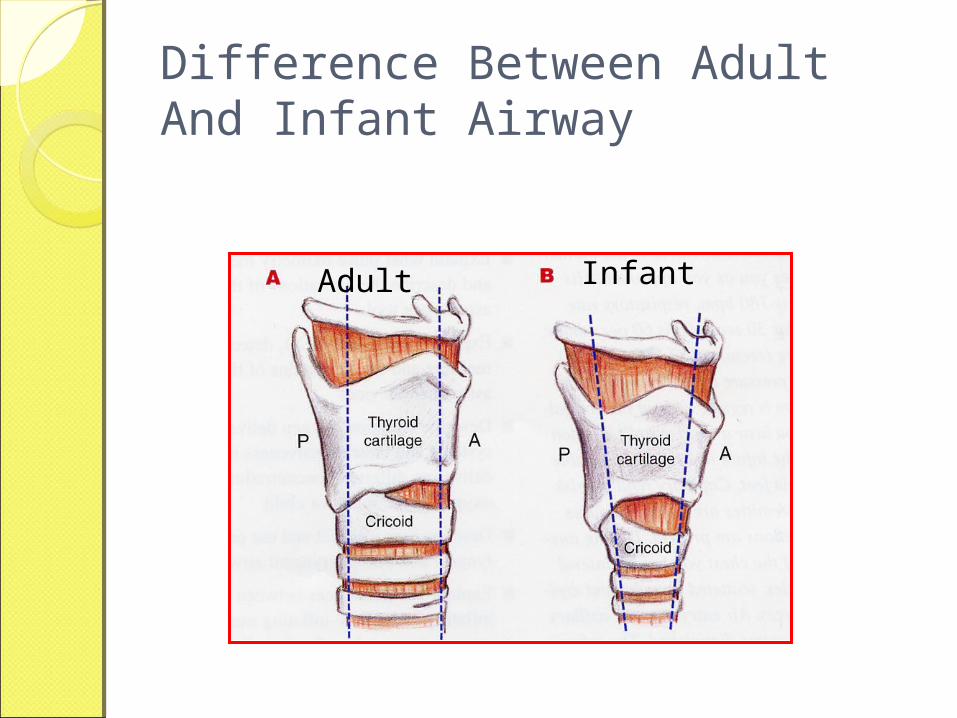
Difference Between Adult And Infant Airway
Adult Infant
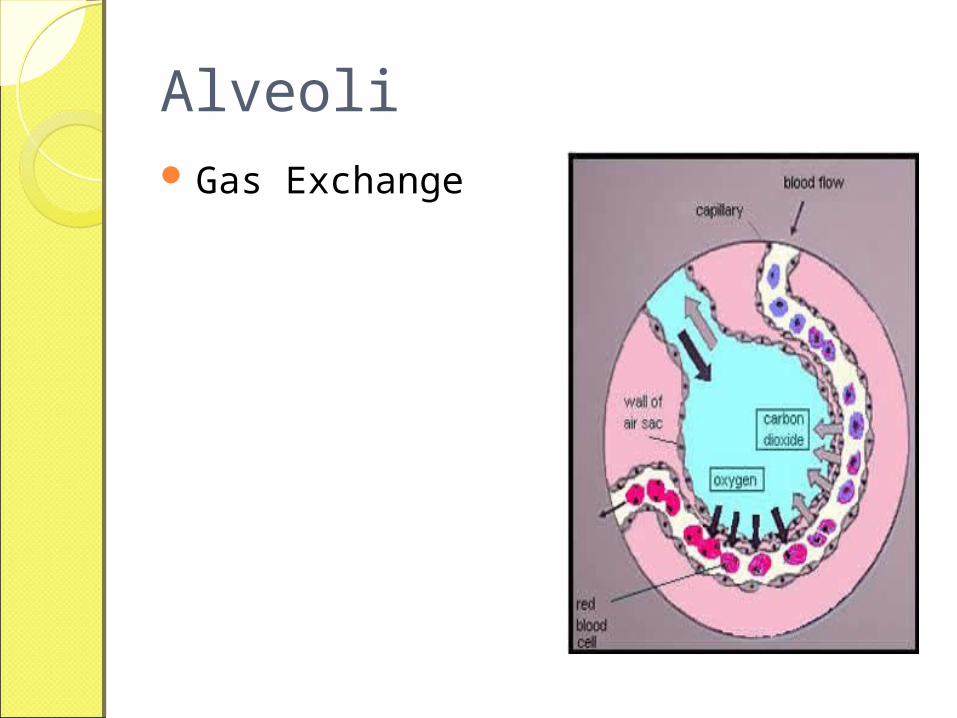
Alveoli Gas Exchange
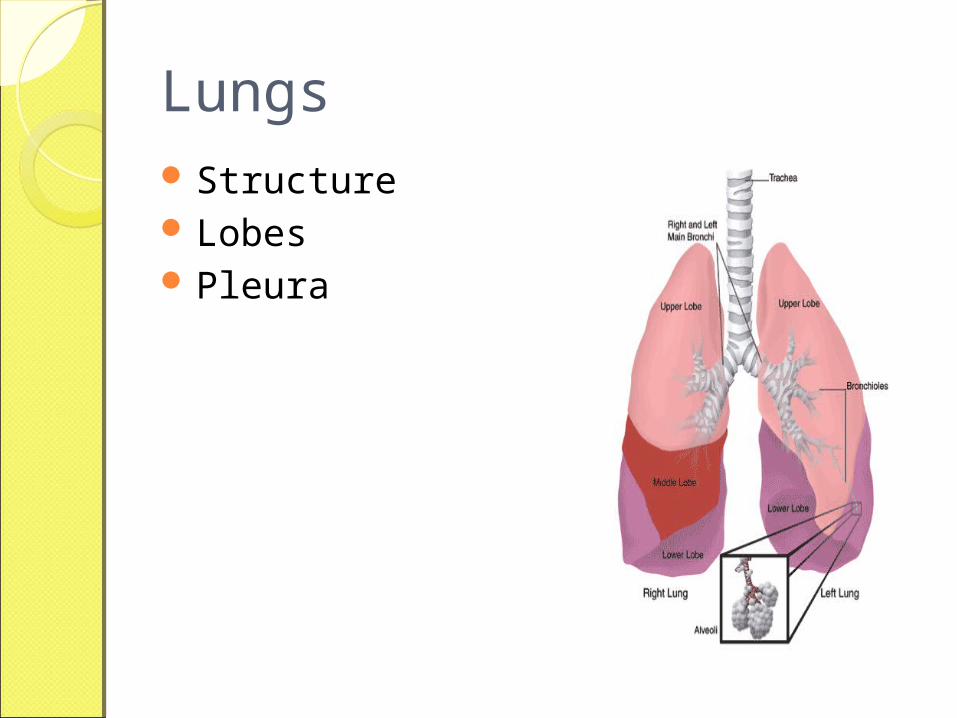
Lungs Structure Lobes Pleura
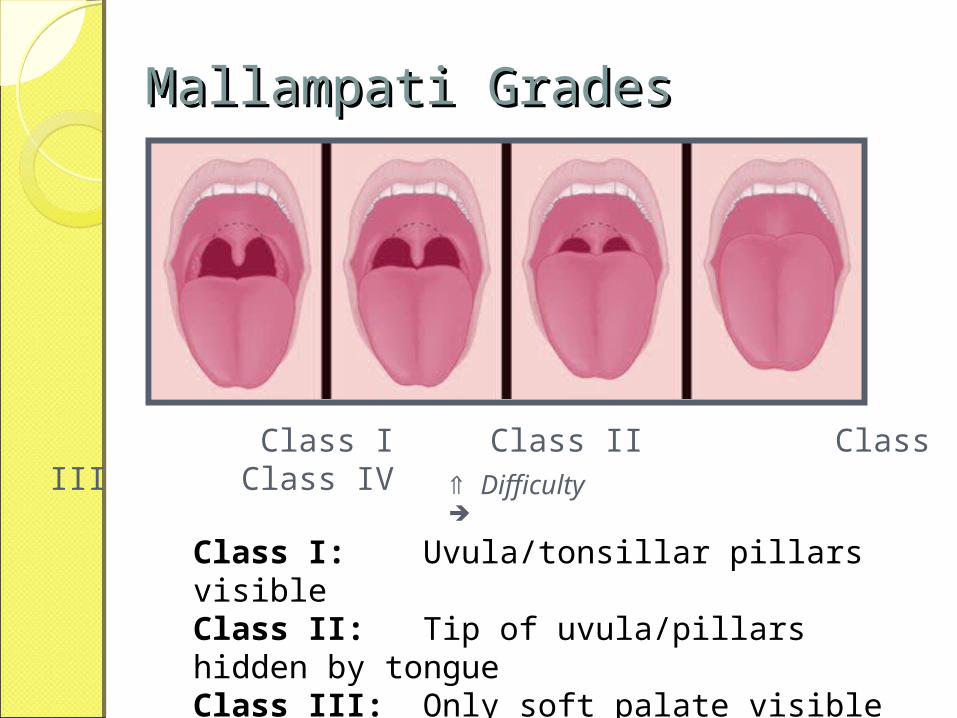
Mallampati GradesMallampati Grades
Difficulty
Class I Class II Class III Class IV
Class I: Uvula/tonsillar pillars visibleClass II: Tip of uvula/pillars hidden by tongueClass III: Only soft palate visibleClass IV: Only hard palate visible
Airway management Airway management proceduresprocedures
Airway management Airway management proceduresproceduresA. Noninvasive procedures
1. Back Blows2. Head Tilt Chin lift procedure3. Heimlich maneuver (Abdominal thrust)4. Chest thrust5. Finger sweep6. Ambu -Bag
B. Invasive procedures1. Oropharangeal airway 2. Nasopharangeal airway3. Cricothyroidectomy4. Tracheotomy5. Endotracheal tube6. Laryngeal Mask Airway
Non Invasive ProceduresNon Invasive Procedures

Back BlowsBack Blows
Back BlowsBack Blows
◦ Indications: Infants
◦ Contraindications:Not recommended for Children and
adults◦ Advantages
Ease
Back BlowsBack Blows
◦Disadvantages1.Not as effective as Heimlich
Maneuver◦Procedure
1.Hold the infant in one hand2.Head lower than trunk3.Support jaws4.Blow with heel of hands between
shoulder blades
Back Blow Video
Heads Tilt Chin lift procedure
Head Tilt Chin lift procedure
Indications :◦To open the airway
Caution with :◦Suspected Neck injury
Procedure :◦One hand on forehead to tilt head
back ◦With fingers of other hand Lift
mandible upward and outward
Heads Tilt Chin lift procedure: Video
Heimlich maneuver Heimlich maneuver
Heimlich maneuver Heimlich maneuver ◦ Indications:
To remove foreign body.◦ Advantages
Effective procedure◦ Disadvantages
Injury to intra-abdominal organs may occur
Heimlich maneuverHeimlich maneuver
◦Procedure Conscious patient :1.Position behind patient and wrap
arms around waist2.Grasp one fist with other hand and
position it slightly above umbilicus; caution- xiphoid process
3. Inward and upward thrusts until foreign body is out.
Heimlich Manuever : Conscious Patient Video
Heimlich manueverHeimlich manuever
Procedure◦Unconscious patient :
1. Patient positioned supine
2. Open airway by “head tilt technique”3. Place heel of one hand on abdomen just above the umbilicus and second hand on top of that4. Provide 6-10 thrusts.
Chest ThrustChest Thrust
Chest ThrustChest Thrust◦ Indications:
1. Infant and child upto 8 years old2. Pregnant female3. Extreme obesity
◦ Contraindications:1. Geriatric patients
◦ Advantages1. Alternative to Heimlich Maneuver
Chest ThrustChest Thrust◦ Procedure
Conscious victim :
1.Stand behind patient encircling victim’s chest
2.Place same grip on middle of sternum
3.Perform until foreign body is out
Chest ThrustChest Thrust◦ Procedure
Unconscious victim :
1.Supine position2.“Head tilt technique”3.Same hand position on lower half
of sternum4.6-10 downward thrusts
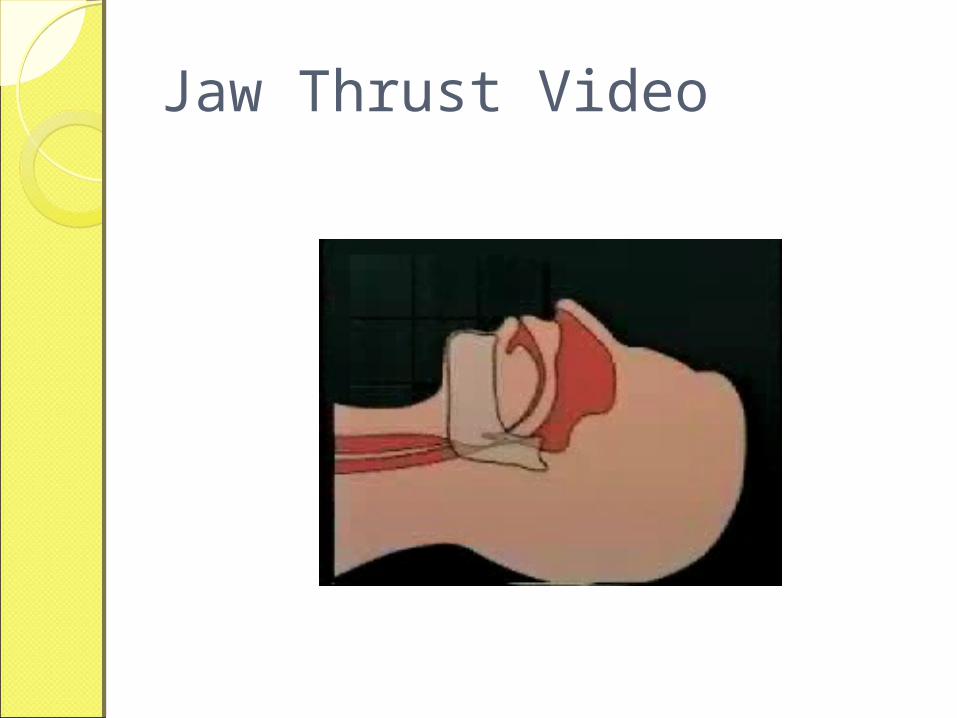
Jaw Thrust
Jaw ThrustIndication :
◦To open the airway blocked due to tongue prolapse
Procedure :◦Grasp the angles of the lower jaw,
one hand on each side, and displacing the mandible forward.
◦Thumbs opening the mouth
Jaw Thrust Video
Finger sweepFinger sweep
Finger sweepFinger sweep◦ Indications:
1.Removal of foreign body in unconscious patients
◦ Contraindications:1.Conscious patient
Finger sweepFinger sweep
◦ Procedure
1.Supine position2.Grasp tongue and anterio portion
of mandible, pull the tongue3.Use index finger to dislodge the
foreign body4.CAUTION: Don’t force the object
deep into airway
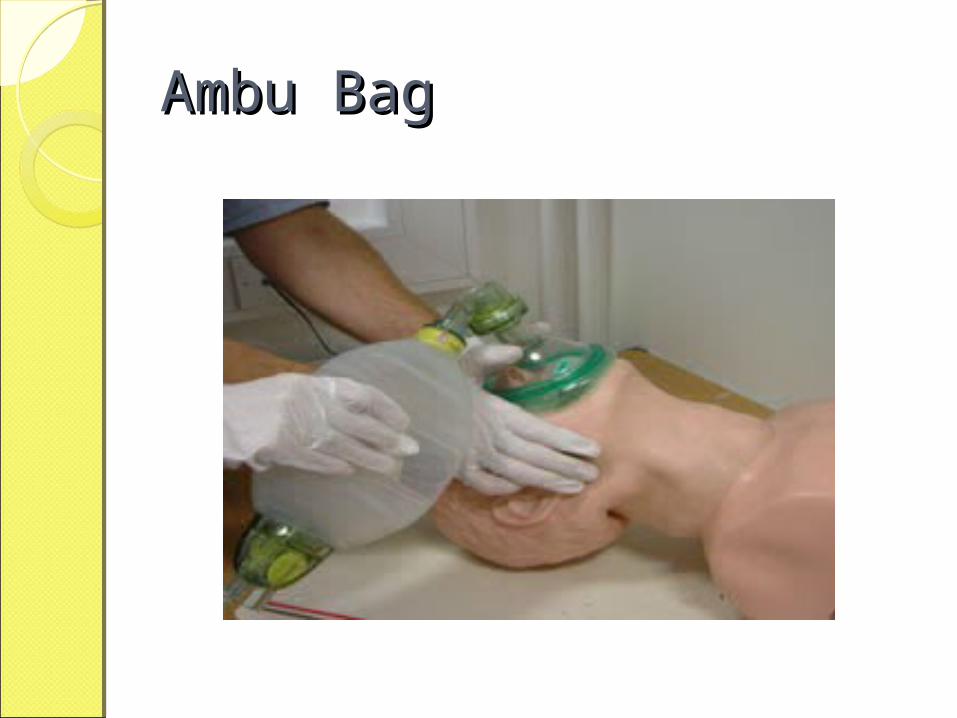
Ambu BagAmbu Bag
Ambu BagAmbu BagIndications:
◦Unconscious patients◦Supplemental oxygen Source
Advantages :◦Can be used directly with
Endotracheal tube Supplemental O2
◦Allows spontaneous ventilation
Ambu BagAmbu BagDiasdvantages:
◦Require special training◦Does not ensure adequate airway

Ambu BagAmbu Bag
Ambu BagAmbu BagTechnique:
◦Attach appropriate mask◦Ensure good seal◦Hold mask with one hand and
squeeze bag intermittently with other hand
Ambu BagAmbu Bag

Recovery Position Video
Invasive TechniquesInvasive Techniques

Invasive techniquesInvasive techniques Indications:
1.Failure of noninvasive techniques2.Obstruction due to swelling;
laryngeal edema, epiglottitis Contraindications:
1. Inadequate training2.Lack of proper equipments
Invasive TechniquesInvasive Techniques Advantages
1.Higher success rate Disadvantages:
1. Need for expertise2. Equipments3. Cost
Risks/Protective MeasuresRisks/Protective Measures
Be prepared for:◦Coughing◦Spitting◦Vomiting◦Biting
Body Substance Isolation◦Gloves◦Face masks◦Eye shields
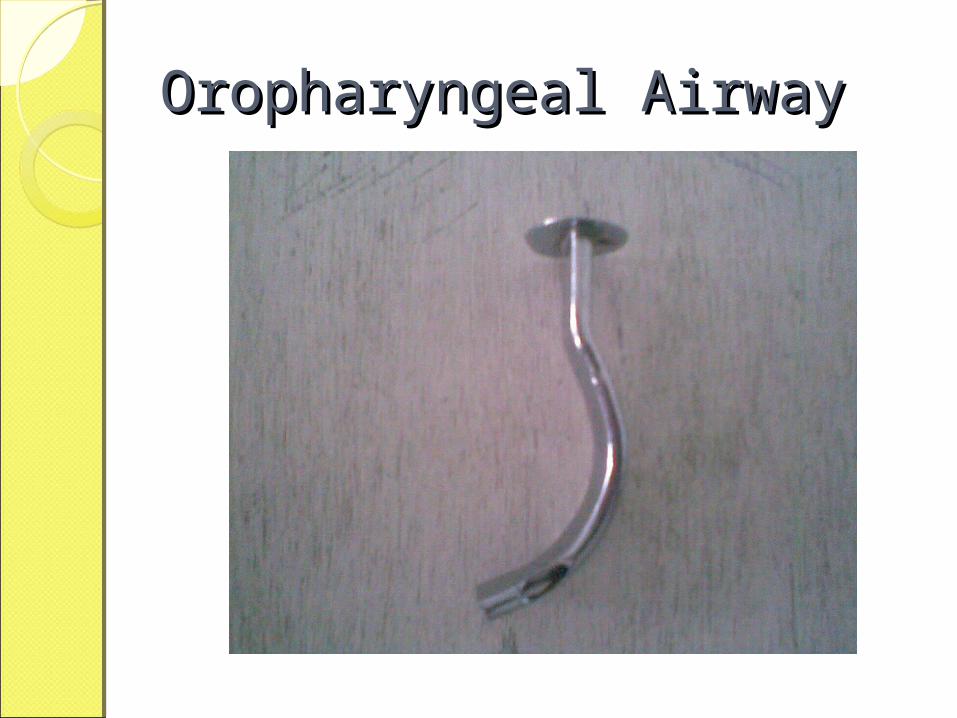
Oropharyngeal AirwayOropharyngeal Airway
Oropharyngeal AirwayOropharyngeal AirwayIndications :
◦Unconscious but spontaneously breathing patients due to tongue positions
Advantages :◦Seperates tongue from posterior
pharyngeal wallDisadvantages :
◦Activates gag reflex in conscious patients
Oropharyngeal AirwayOropharyngeal AirwaySize :
◦Adult : 100 mm◦Small adult : 80 – 90 mm
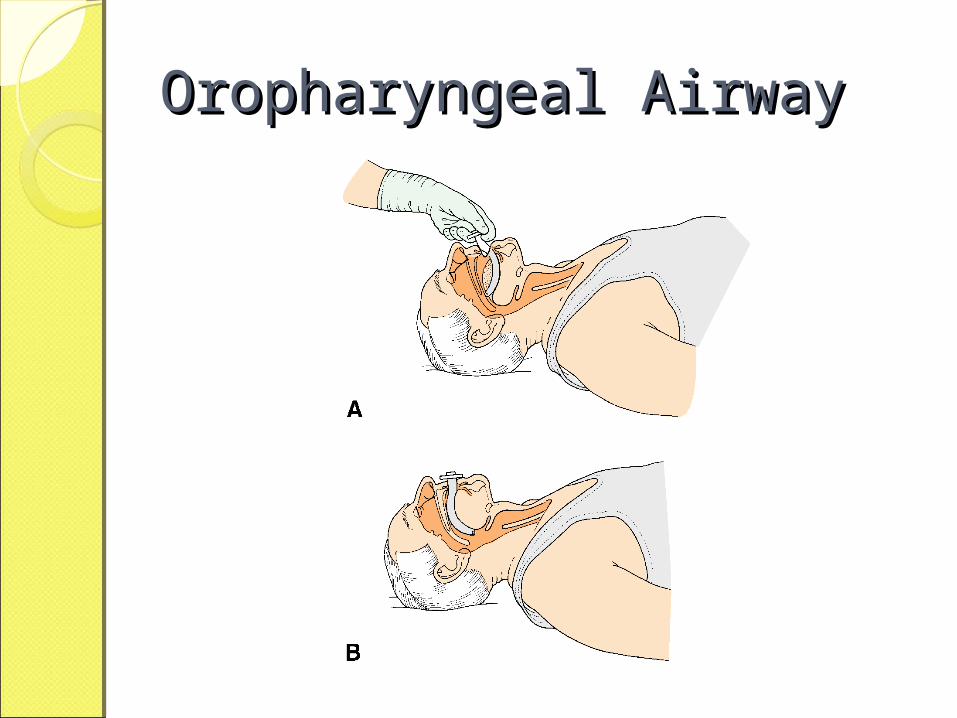
Technique :◦Position◦Use tongue blade◦Insert inverted and later rotate
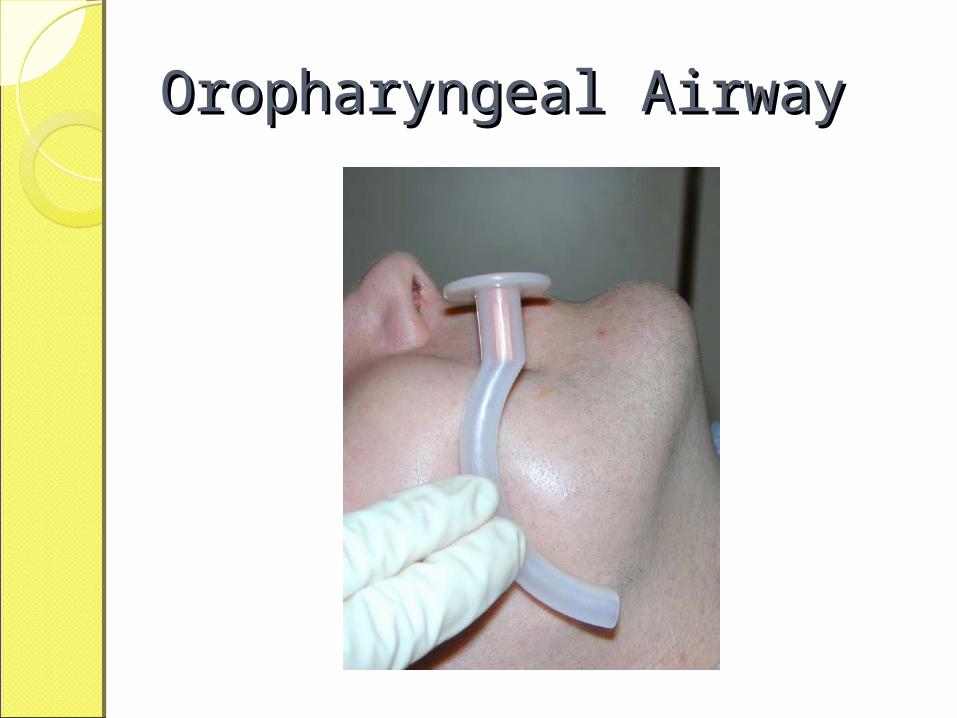
Oropharyngeal AirwayOropharyngeal Airway
Oropharyngeal AirwayOropharyngeal Airway

Oropharyngeal AirwayOropharyngeal AirwayVarious Sizes
Oropharyngeal AirwayOropharyngeal Airway
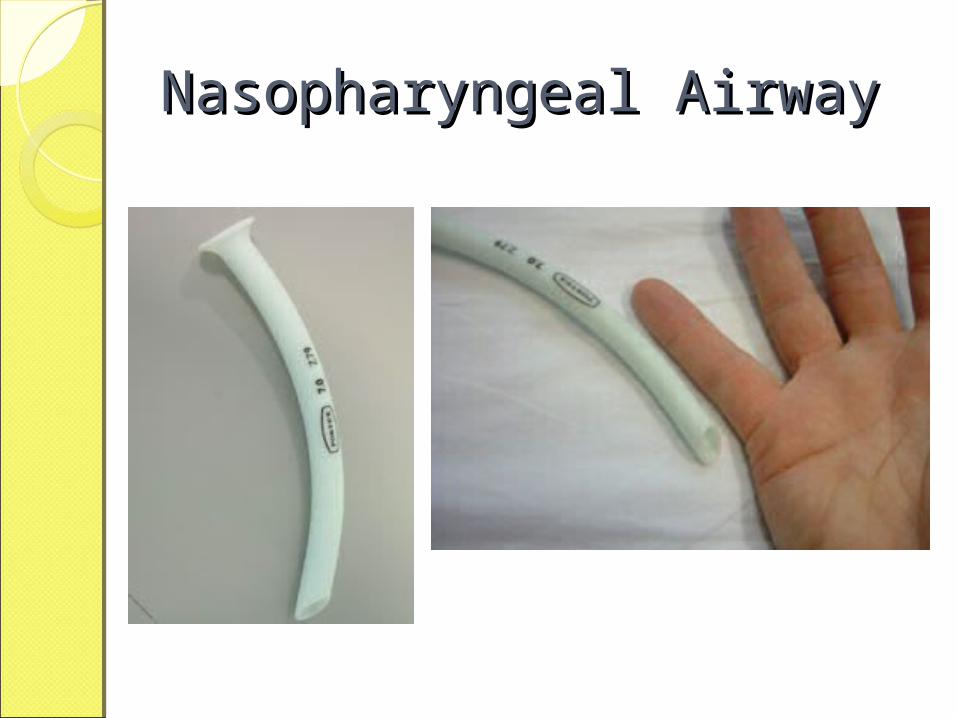
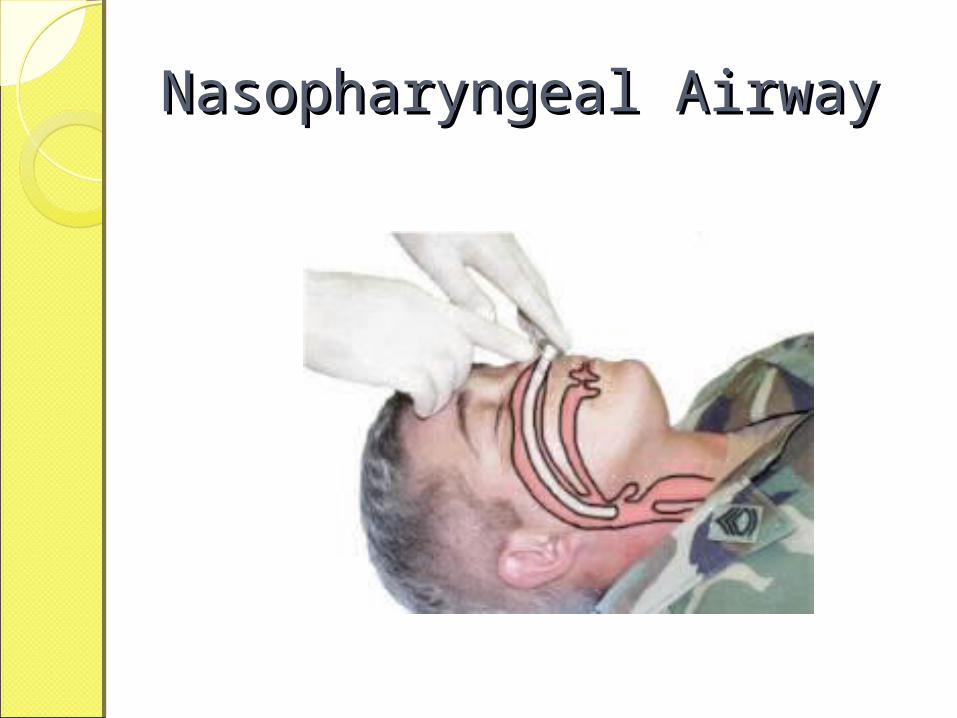
Nasopharyngeal AirwayNasopharyngeal Airway
Nasopharyngeal AirwayNasopharyngeal AirwayIndications:
◦Tongue obstruction◦Inadequate oral opening◦Oral Surgery
Advantages :◦Well tolerated even in conscious
patientSizes : (Internal Diameter)
◦Large adult :8-9 mm◦Small adult : 6-8 mm
Nasopharyngeal AirwayNasopharyngeal Airway
Nasopharyngeal AirwayNasopharyngeal Airway
Various Sizes
Nasopharyngeal AirwayNasopharyngeal AirwayPositionDetermine the size of tubesLocal AnesthesiaLubricate
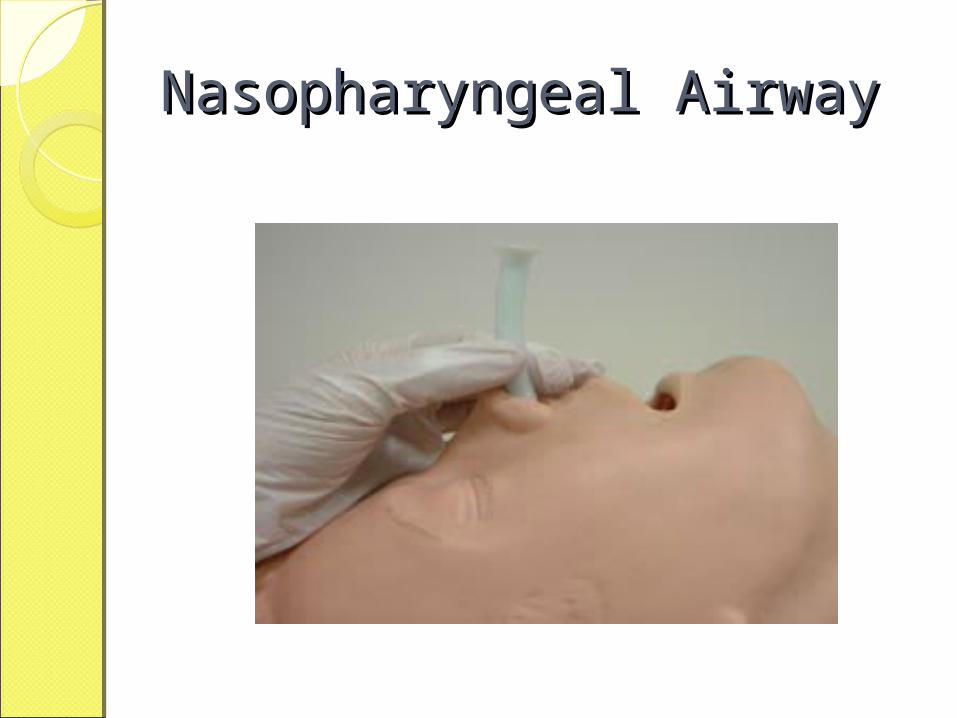
Nasopharyngeal AirwayNasopharyngeal Airway
Nasopharyngeal AirwayNasopharyngeal Airway
TracheotomyTracheotomy
TracheostomyTracheostomyDefinition :
“Formation of a fistulas hole between the skin and trachea”
TracheostomyTracheostomyClassification:
◦Emergency Tracheostomy◦Semi-emergency Tracheostomy◦Planned Tracheostomy
◦High Level : 1, 2, 3 tracheal rings ◦Low Level : 2,3,4 tracheal rings
◦Temporary : for respiratory distress◦Permanent :Laryngopharyngectomy
TracheotomyTracheotomy◦ Indications:
1. Long term airway maintenance2. Glottic edema3. Laryngeal nerve palsy4. Head injury5. Tetanus6. Coma7. Chest injury8. Laryngeal infections
TracheotomyTracheotomyContraindications:
◦ Cervical Spine fracture◦ Tracheomalecia◦ Carcinoma of trachea
Advantages◦ Bypass upper airway obstruction◦ Reduces the dead space◦ Attachment to vetilator is possible
TracheotomyTracheotomy
◦Equipments :
1.Blade2.Tracheal dilator3.Cats paw retractor4.Tracheostomy tube
TracheotomyTracheotomy Technique :
◦Patient position◦Hyperextension of neck◦Locate the cricoid cartilage◦Vertical incision of 2-3 cm◦Retract skin using Cat paw retractor◦Incise the trachea and dilate it using
tracheal dilator◦Apply 2% lignocain gauze ( Reflex)◦Insert the tracheotomy tubes
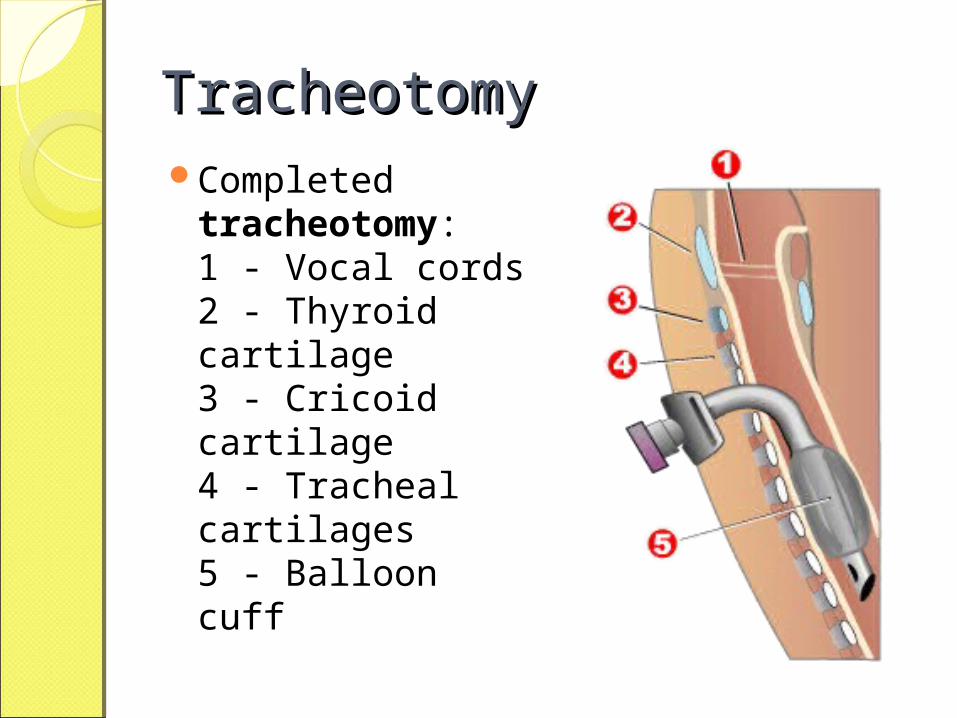
TracheotomyTracheotomyCompleted
tracheotomy:1 - Vocal cords2 - Thyroid cartilage3 - Cricoid cartilage4 - Tracheal cartilages5 - Balloon cuff
TracheotomyTracheotomy◦ Possible Complications
1. Perforation of esophagus2. Hemorrhage3. Pnemothorax4. Tracheal stenosis5. Loss of speech6. Chances of infection
Percutaneous TracheotomyProcedure
◦skin incision along relaxed skin tension lines
◦Insert of 14-gauge needle◦Tracheal dilatation◦Insert tracheostomy tube◦Connect ventilator tubing
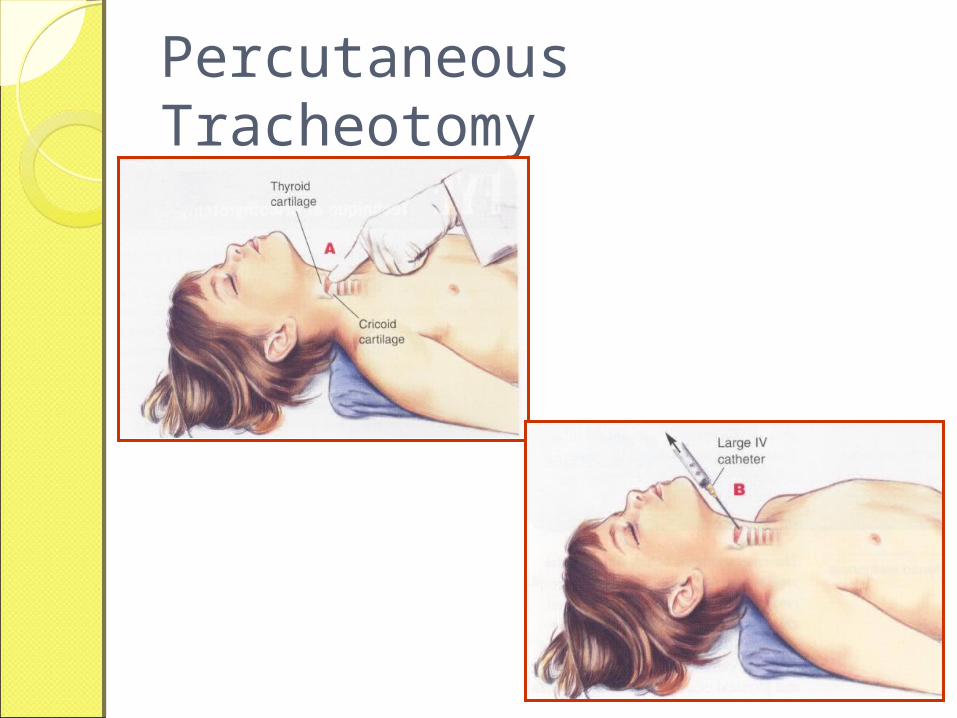
Percutaneous Tracheotomy
CricothyrotomyCricothyrotomy
CricothyrotomyCricothyrotomy
Indications◦ Absolute need for definitive airway, AND
unable to perform ETI due to structural or anatomic reasons, AND
risk of not securing airway is > than surgical airway risk
OR◦ Absolute need for definitive airway AND
unable to clear an upper airway obstruction, AND
multiple unsuccessful attempts at ETT, AND other methods of ventilation do not allow for
effective ventilation, respiration
CricothyrotomyCricothyrotomyContraindications (relative)
No real demonstrated indication Risks > Benefits Age < 8 years (some say 10, some say
12) Evidence of fractured larynx or cricoid
cartilage Evidence of tracheal transection
Advantages: Less complications Less bleeding Heals within a few days
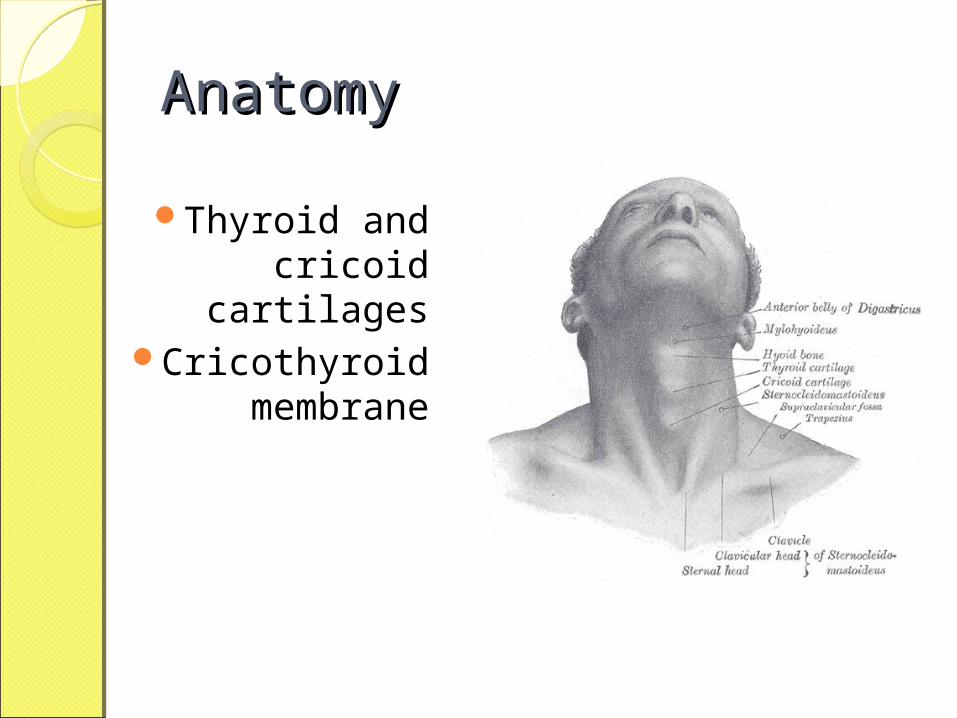
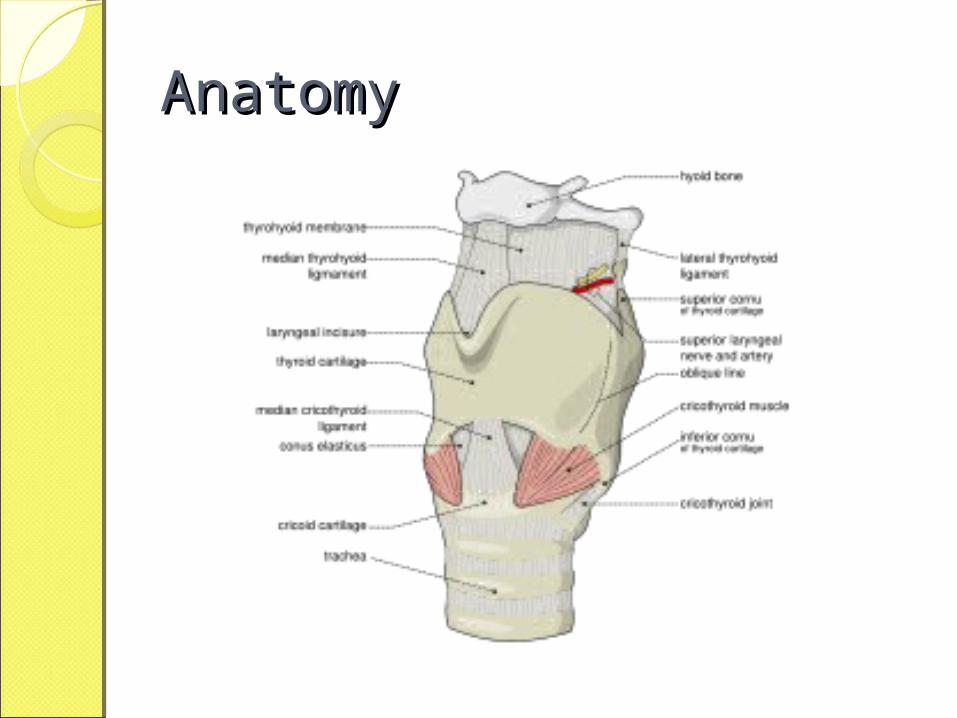
AnatomyAnatomy
Thyroid and cricoid cartilages
Cricothyroid membrane
AnatomyAnatomy
CricothyrotomyCricothyrotomy Equipments :
1. Scalpel No. 11 Blade2. Or 13 gauge half inch long needle
Cricothyrotomy VideoCricothyrotomy Video
CricothyrotomyCricothyrotomy Technique:
1. Supine position2. Hyperextension of neck3. Locate cricothyroid membrane4. Vertical skin incision5. Retract with thumb and index finger6. Horizontal incision as close to cricoid
cartilage as possible7. Rotate the blade at 90 degrees8. If available, insert tubes
Cricothyrotomy VideoCricothyrotomy Video
Endotracheal intubationEndotracheal intubation
Endotracheal IntubationEndotracheal Intubation
Introduction ◦Tube into trachea to provide
ventilations using ventilator
Endotracheal IntubationEndotracheal IntubationDefinition :
◦ Endotracheal intubation is the placement of a tube into the trachea (windpipe) in order to maintain an open airway in patients who are unconscious or unable to breathe on their own. Oxygen, anesthetics, or other gaseous medications can be delivered through the tube.
Endotracheal Intubation
Indications: ◦ Treatment of symptomatic hypercapnia.◦ Treatment of symptomatic hypoxemia.◦ Airway protection against aspiration.◦ Pulmonary toilet◦ Present or impending respiratory failure◦ Apnea◦ Unable to protect own airway
Contraindications: ◦ Awake patient.◦ Airway can be managed less invasively
Endotracheal IntubationEndotracheal Intubation
Advantages◦Secures airway◦Route for a few medications ◦Optimizes ventilation, oxygenation◦Allows suctioning of lower airway
Hazards:◦Esophageal intubation◦Damage to vocal cords◦Damage to teeth (Laryngoscope)◦Endobroncheal intubation
Endotracheal IntubationEndotracheal Intubation Equipment:
1. Endotracheal tube
Adult female= 7- 8 mm
Adult Male = 8 – 9 mm
child = diameter of little finger
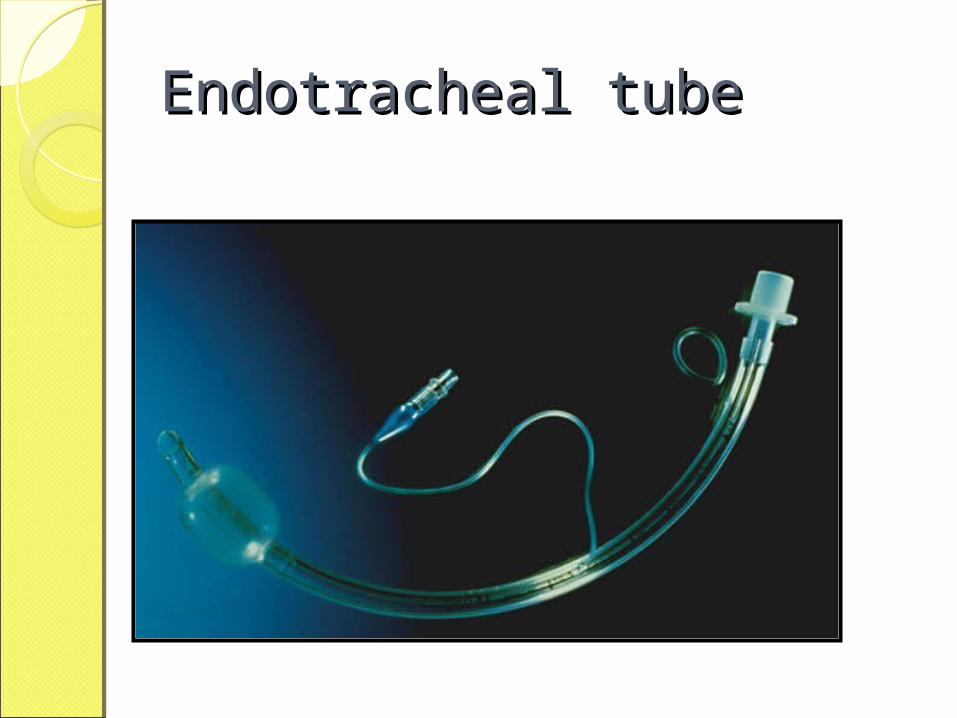
Endotracheal tubeEndotracheal tube
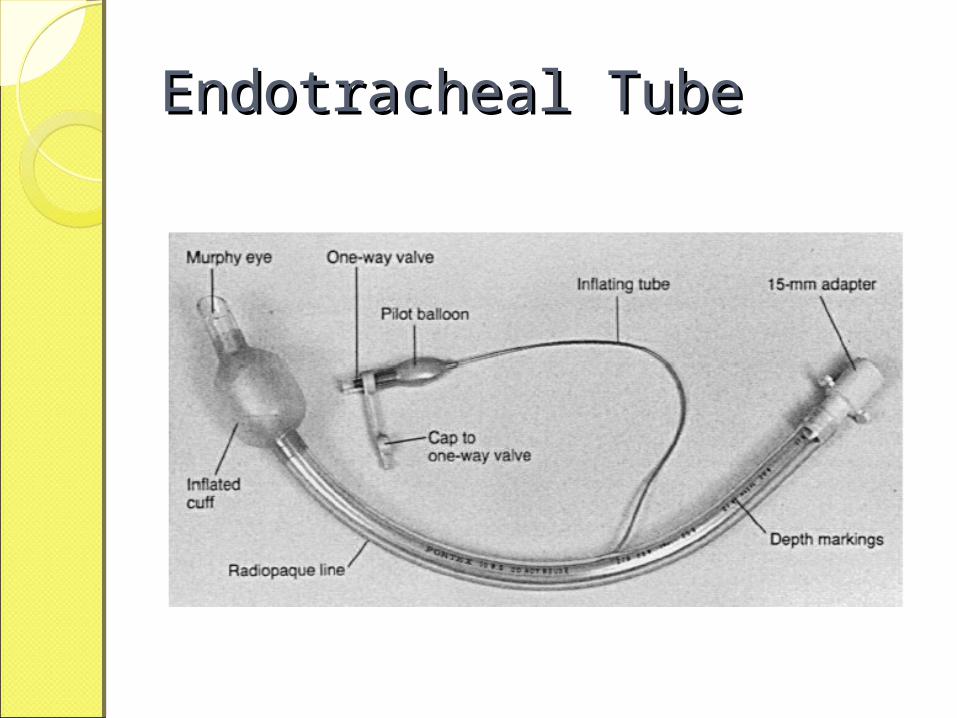
Endotracheal TubeEndotracheal Tube
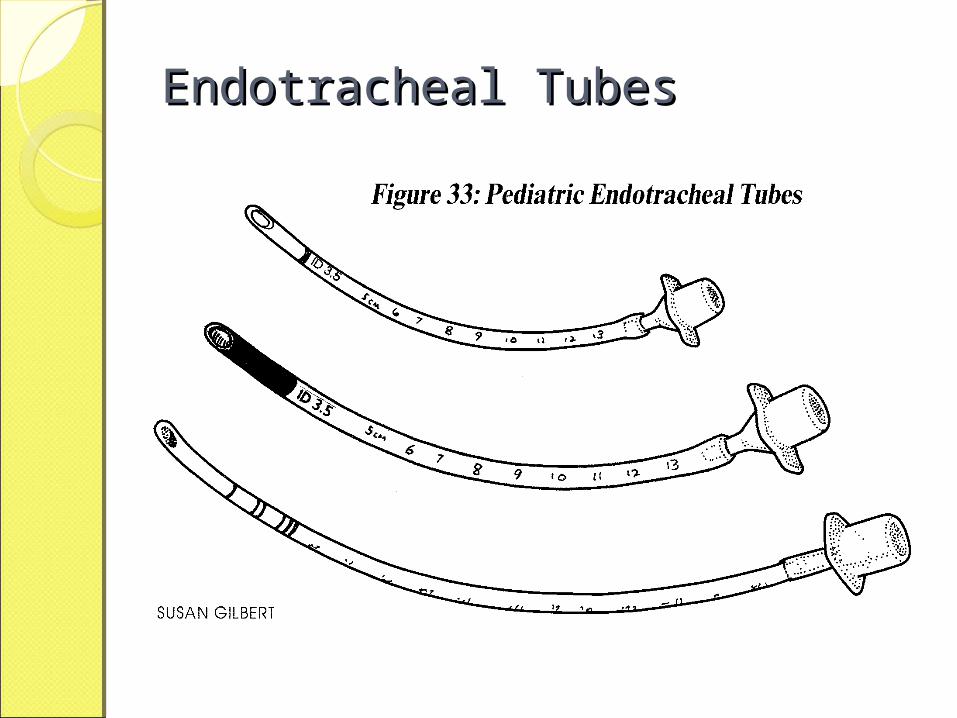
Endotracheal TubesEndotracheal Tubes
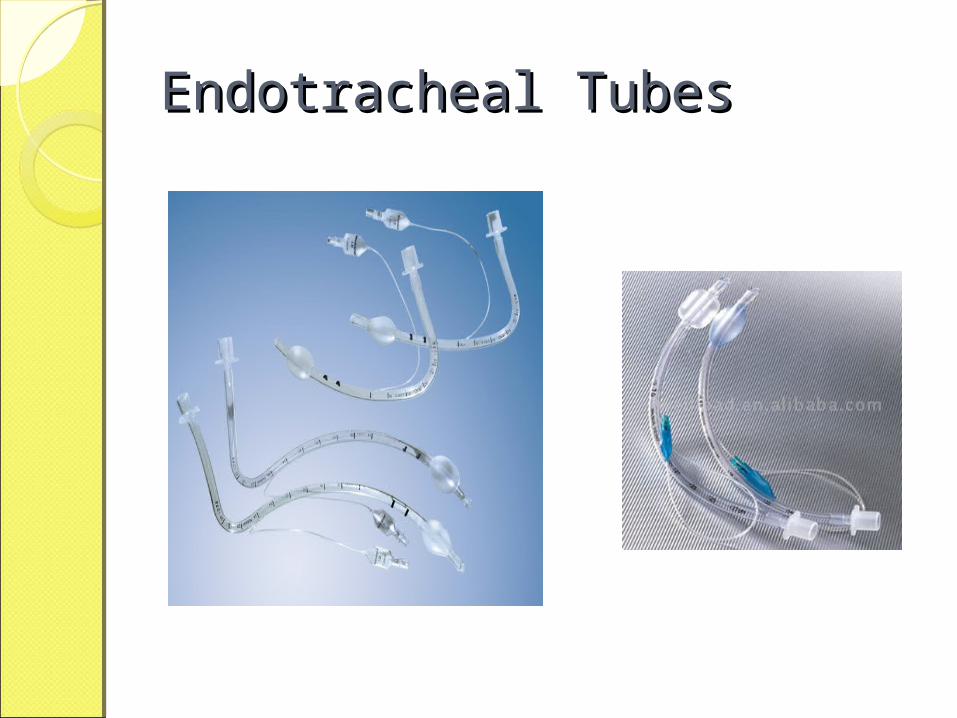
Endotracheal TubesEndotracheal Tubes
Endotracheal IntubationEndotracheal Intubation Equipments1. Laryngoscope blade
1. Stright1. Adult : size 3 to 42. Child : Size 2-33. Baby : size 1- 2
2. Curved1. Adult : size 3 to 42. Child : Size 2-33. Baby : size 1- 2

Laryngoscope
Straight Laryngoscope
Curved Laryngoscope
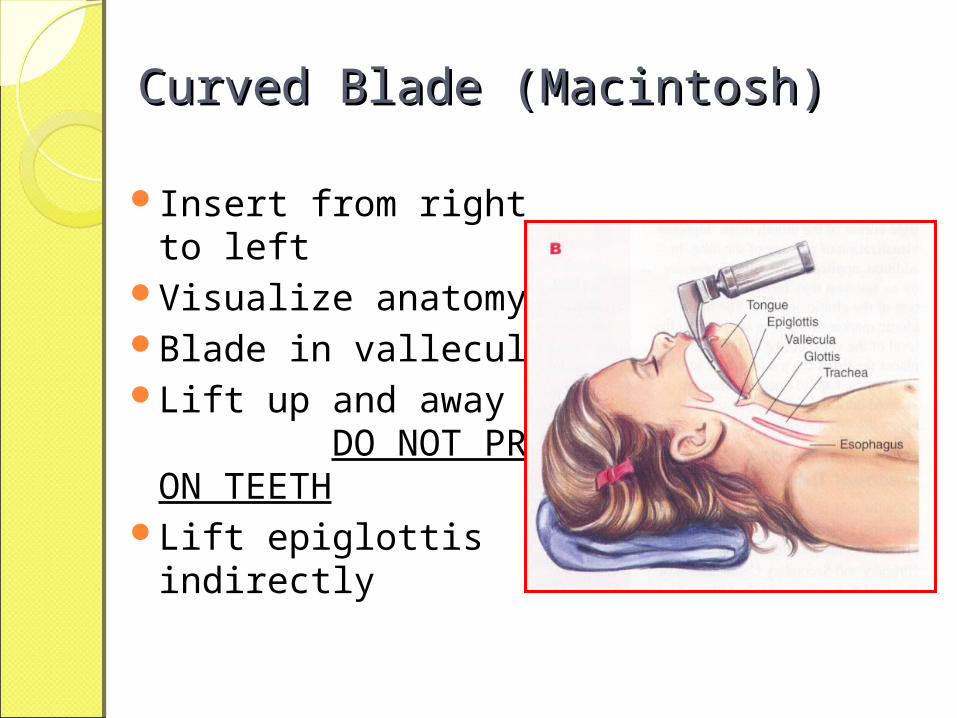
Curved Blade (Macintosh)Curved Blade (Macintosh)
Insert from right to left
Visualize anatomy Blade in valleculaLift up and away
DO NOT PRY ON TEETH
Lift epiglottis indirectly

Straight Blade (Miller)Straight Blade (Miller)
Insert from right to left
Visualize anatomyBlade past vallecula
and over epiglottisLift up and away
DO NOT PRY ON TEETH
Lift epiglottis directly
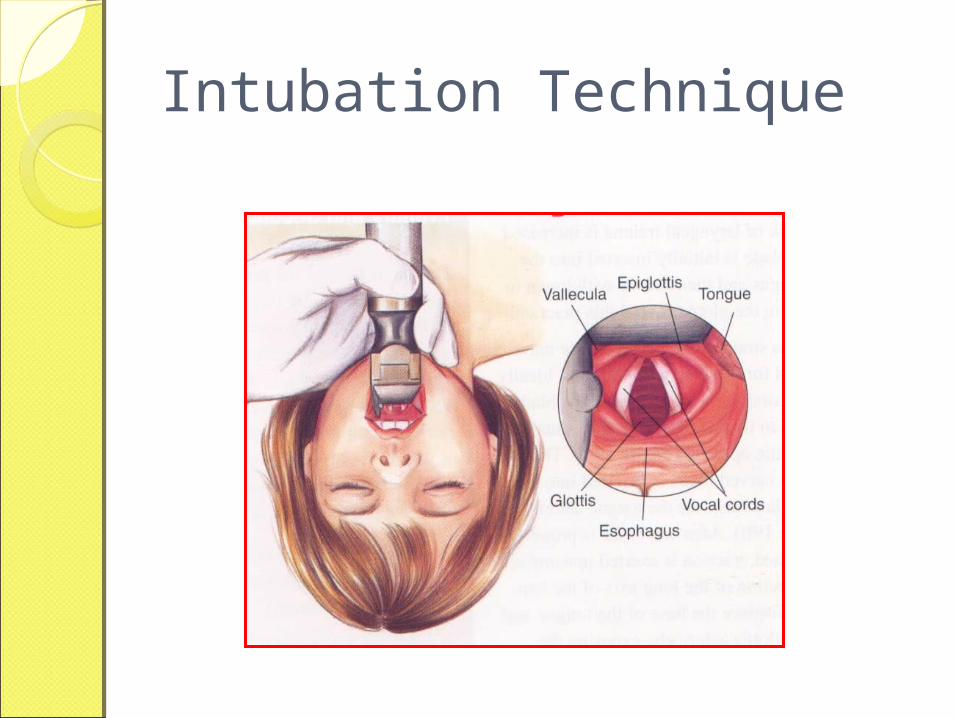
Intubation Technique
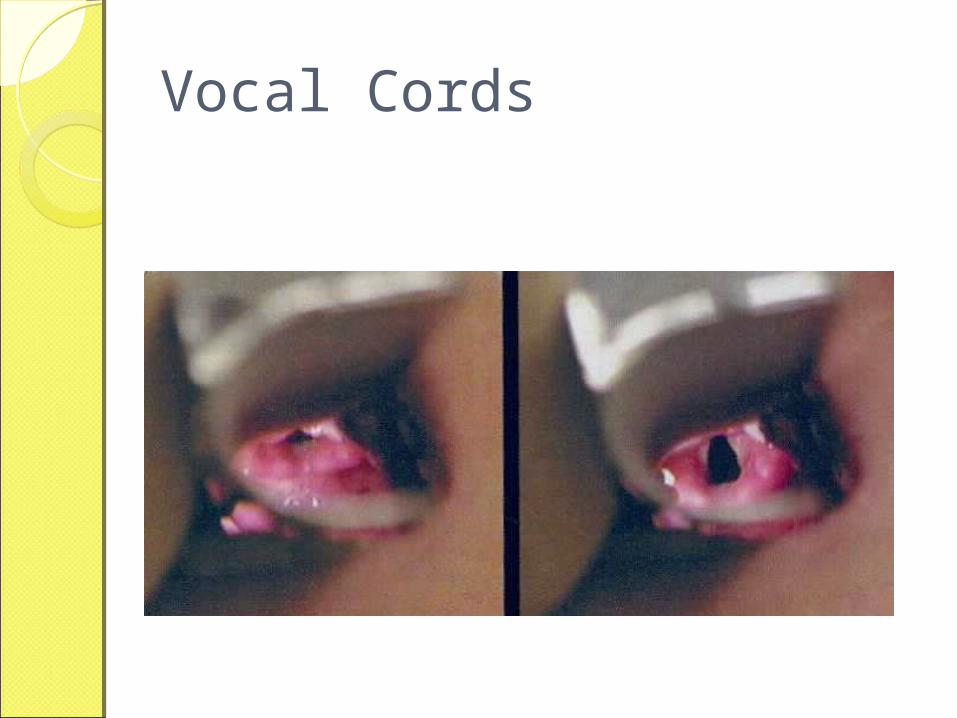
Vocal Cords
LaryngoscopyLaryngoscopy
Endotracheal IntubationEndotracheal IntubationProcedure: Assess
◦ airway – note landmarks, swelling, deformities.
◦ Remove dentures. – Assess tongue size, dental obstruction, visibility of oropharynx,
◦ degree of neck mobility. - Maintain cervical spine stability as necessary.
Open airway: suction or manually extract foreign material. – Chin lift, jaw thrust.
Heimlich maneuver as needed.

Endotracheal IntubationEndotracheal IntubationPosition patient into “sniffing
position” if possible; restrain as necessary.
Standing at the supine patient’s head, gentle insert laryngoscope blade with left hand.
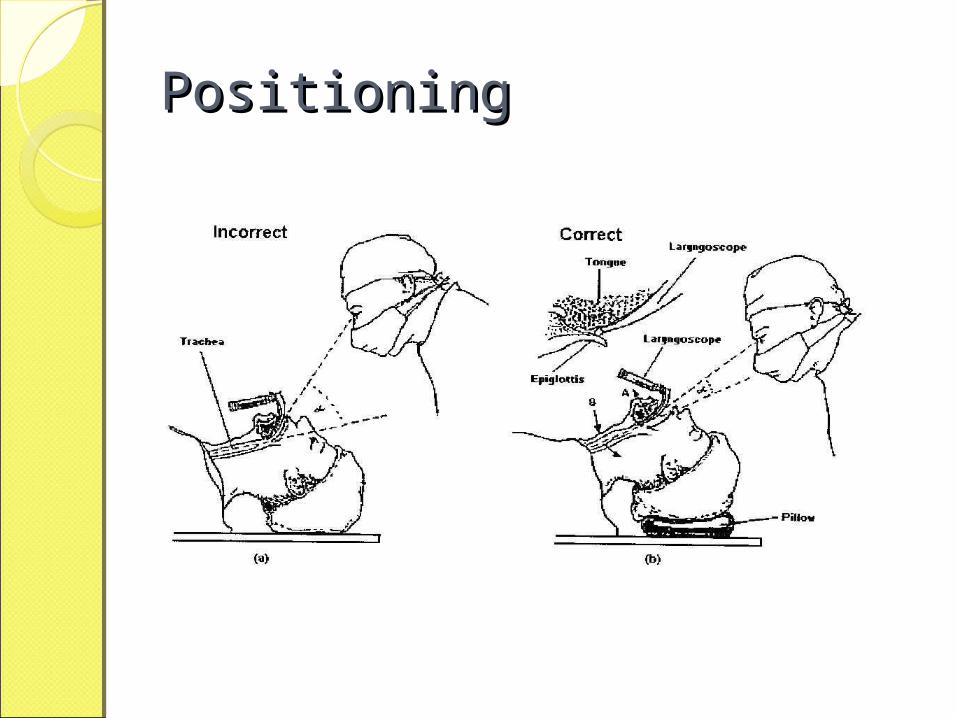
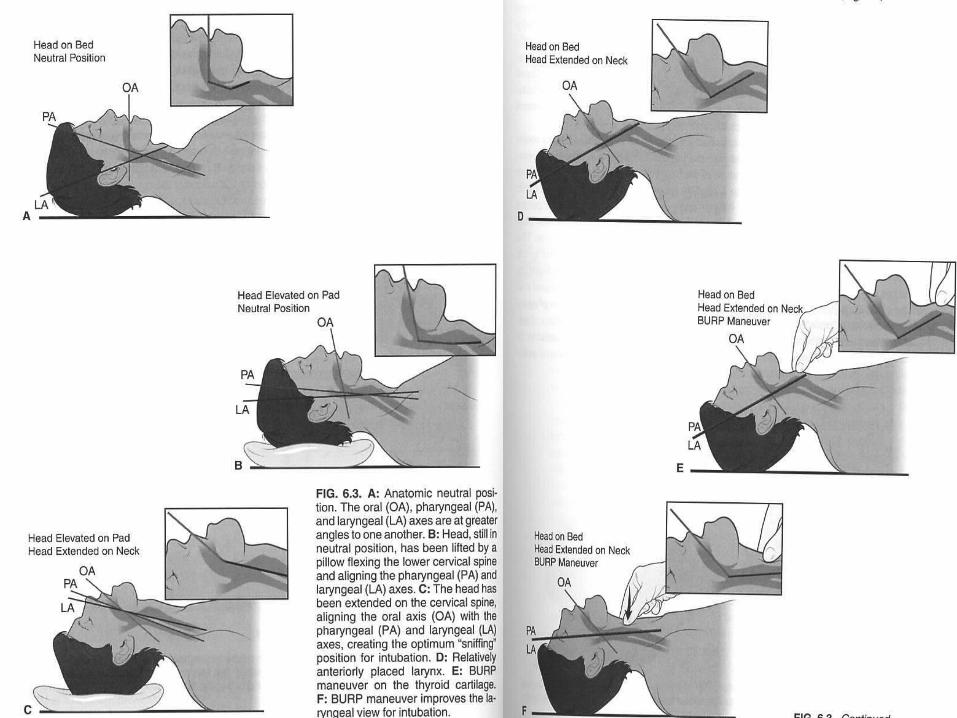
PositioningPositioning
PositioningPositioning
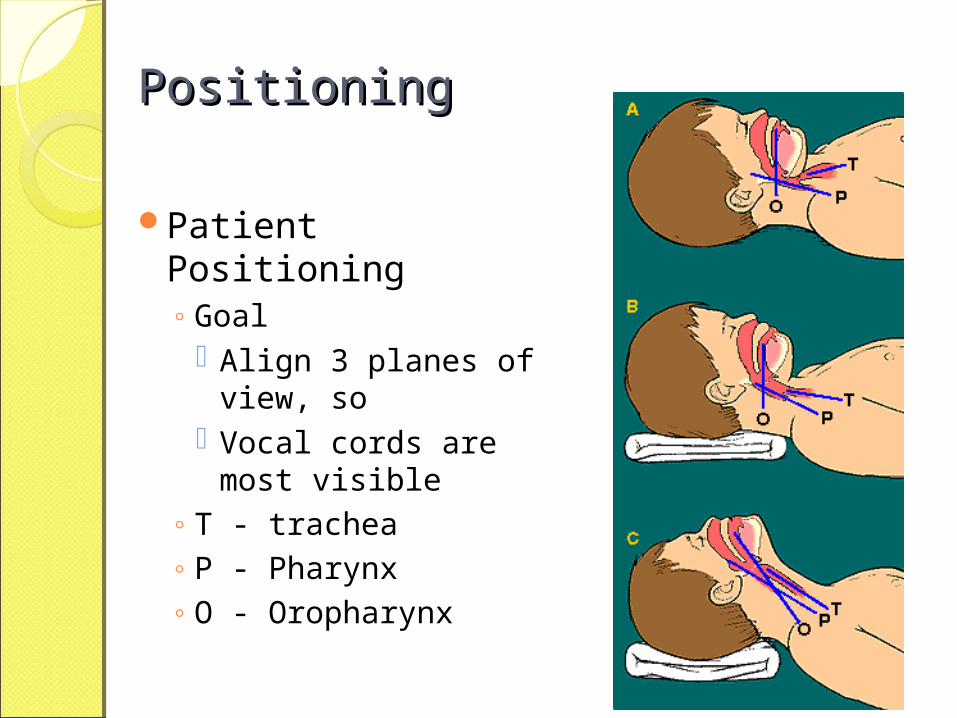
Patient Positioning◦ Goal
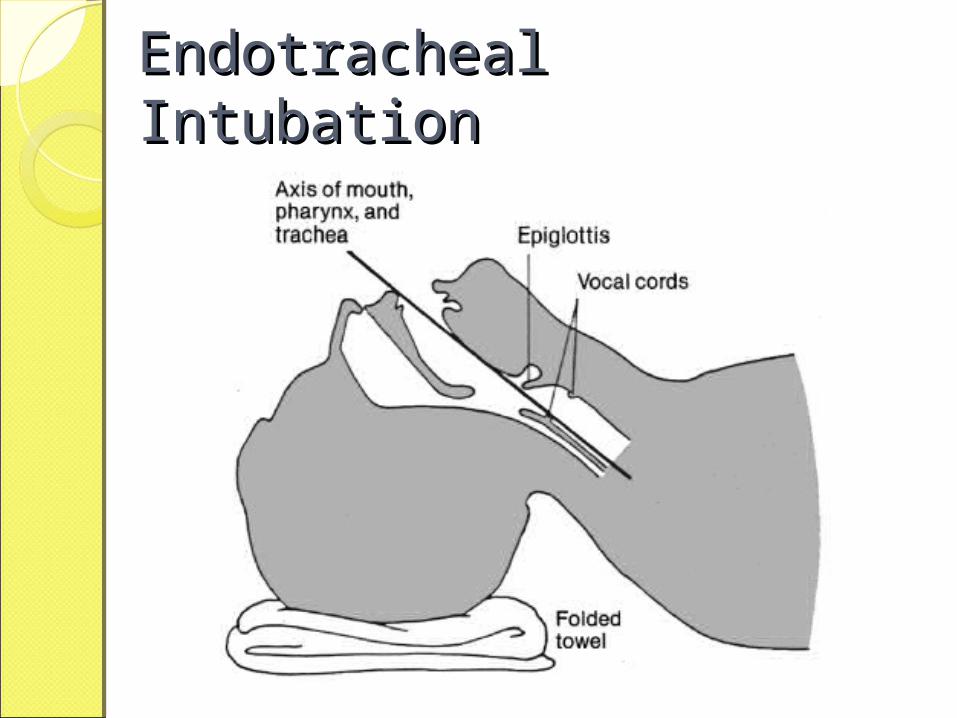
Align 3 planes of view, so
Vocal cords are most visible
◦ T - trachea◦ P - Pharynx◦ O - Oropharynx
Endotracheal IntubationEndotracheal Intubation
Endotracheal Endotracheal IntubationIntubationVisualize glottic opening/vocal
cords.Insert the tubes
Endotracheal Endotracheal IntubationIntubation
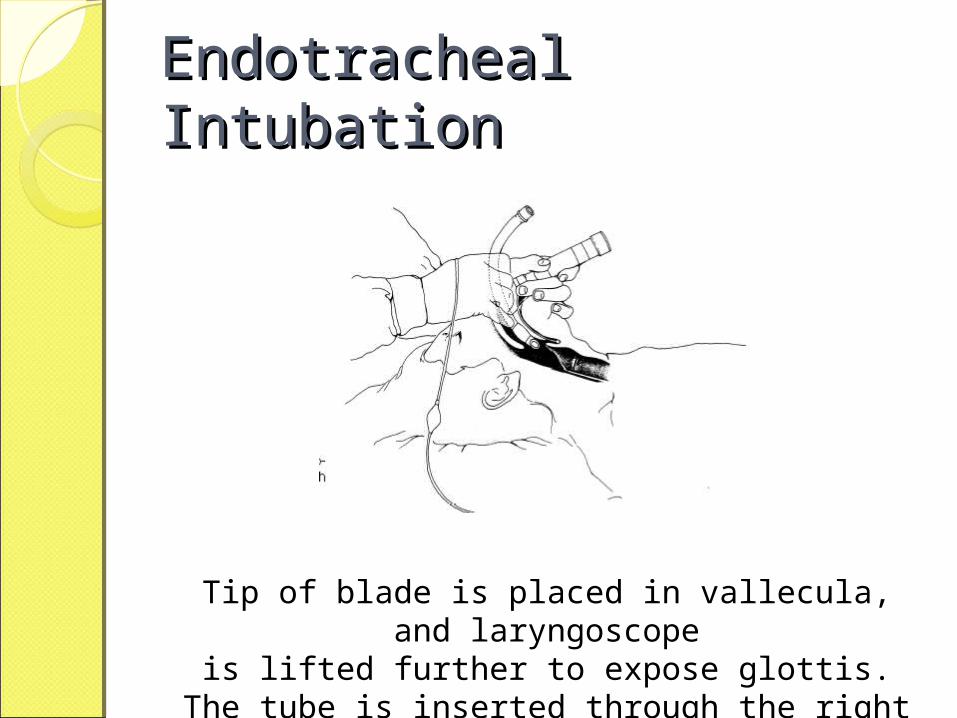
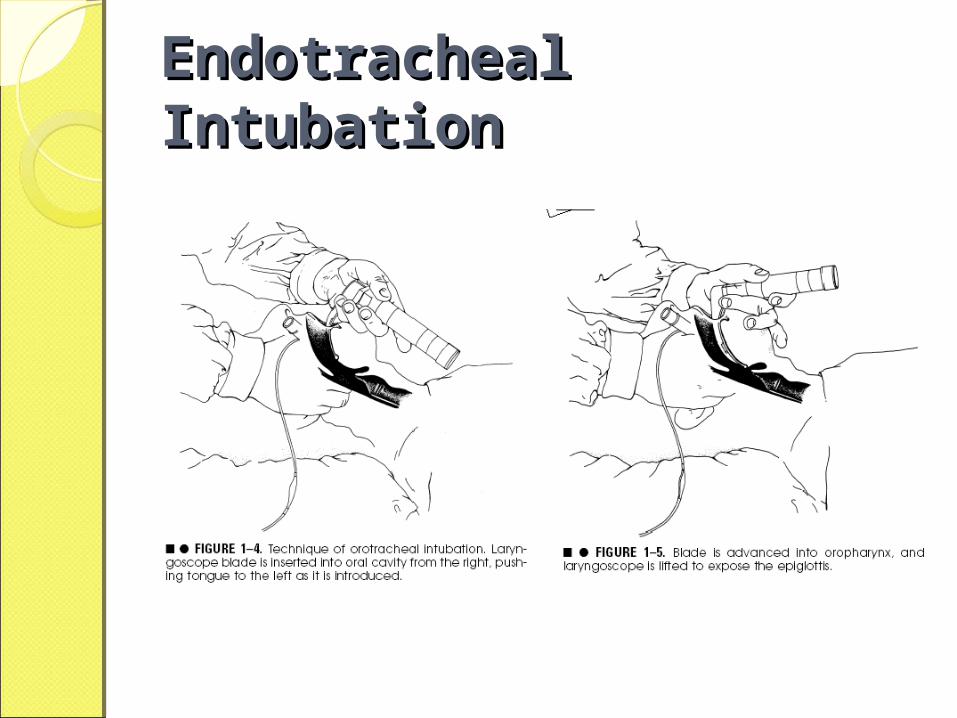
Endotracheal IntubationEndotracheal Intubation
Tip of blade is placed in vallecula, and laryngoscopeis lifted further to expose glottis. The tube is inserted
through the right side of the mouth.
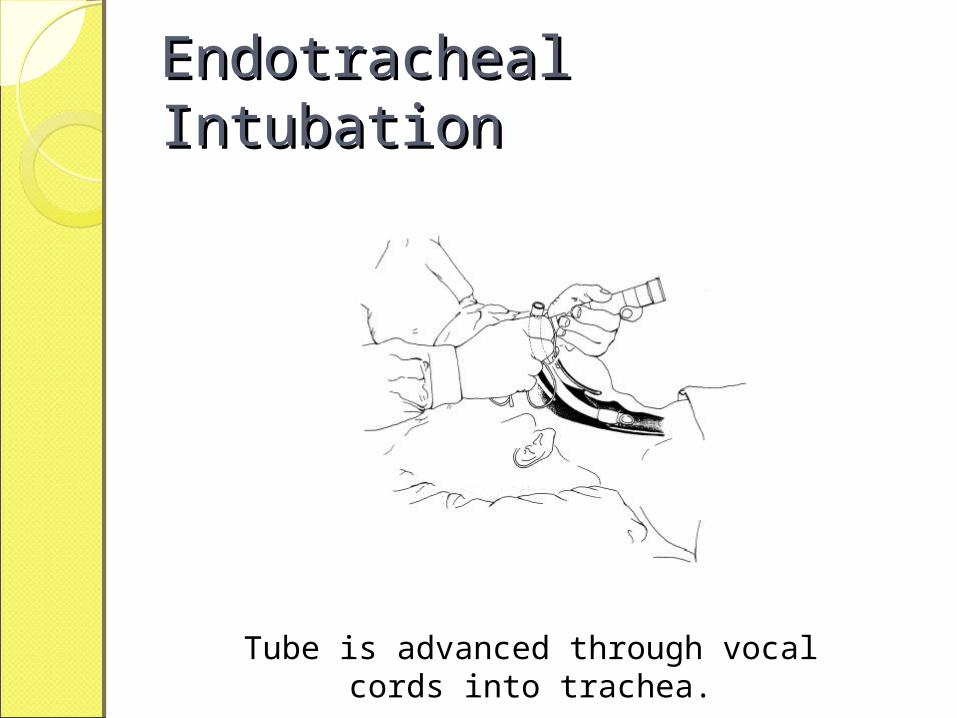
Endotracheal IntubationEndotracheal Intubation
Tube is advanced through vocal cords into trachea.
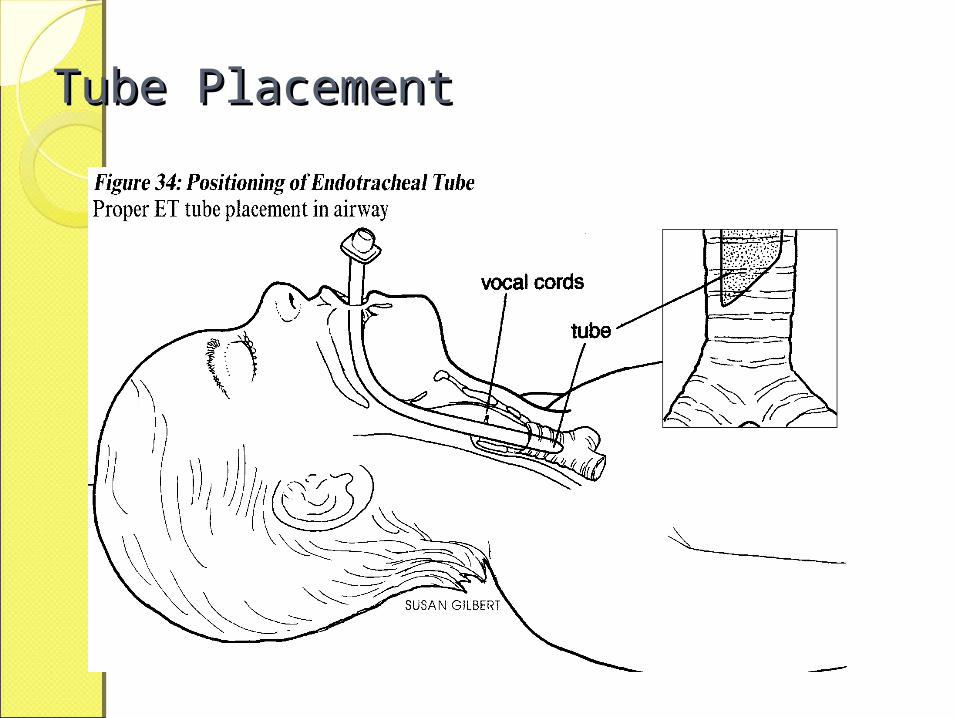
Tube PlacementTube Placement
Endotracheal Endotracheal IntubationIntubationInflate ETT cuff with 5 – 10 cc air
via syringe. Ventilate with bag and oxygen.
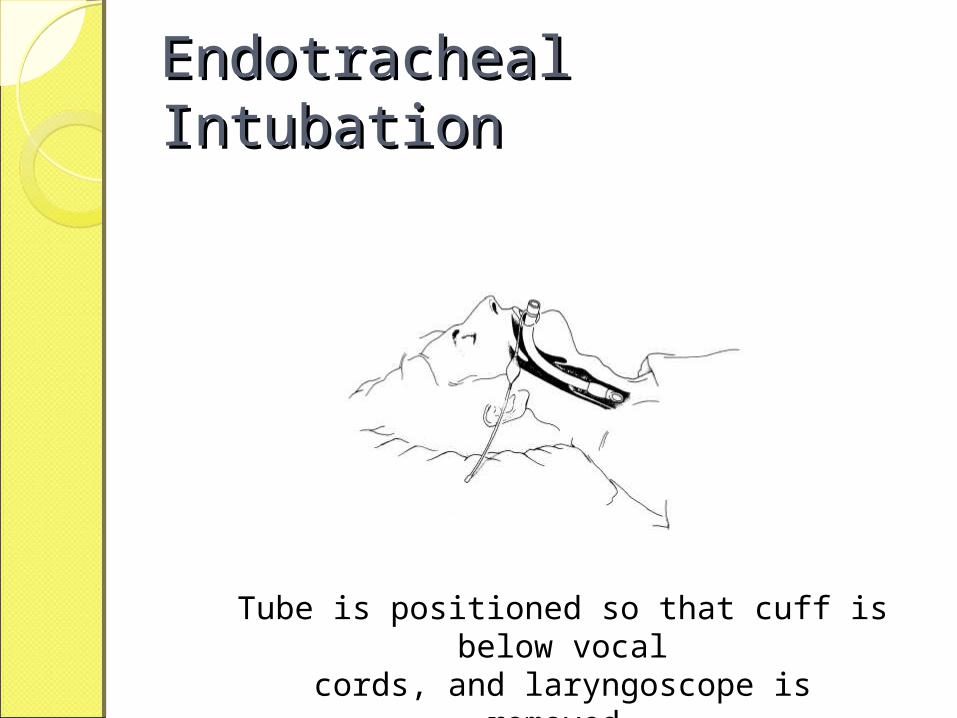
Endotracheal IntubationEndotracheal Intubation
Tube is positioned so that cuff is below vocalcords, and laryngoscope is removed.
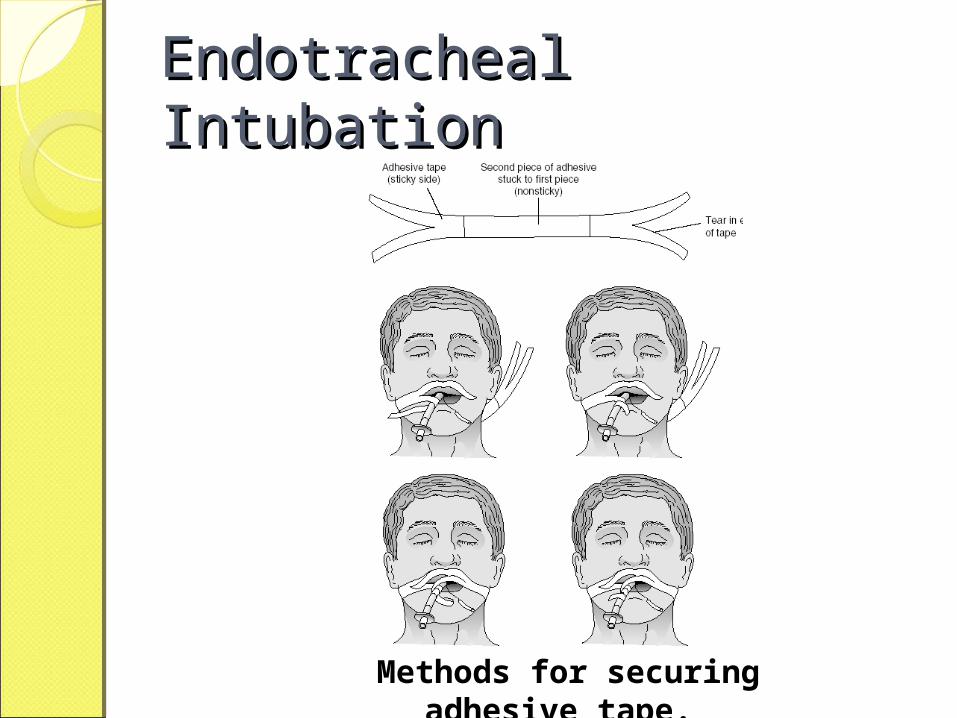
Endotracheal IntubationEndotracheal Intubation
Methods for securing adhesive tape.

Endotracheal IntubationEndotracheal IntubationConfirm tube placement
◦ chest auscultation, ◦ CO2 monitor ◦ chest x-ray.
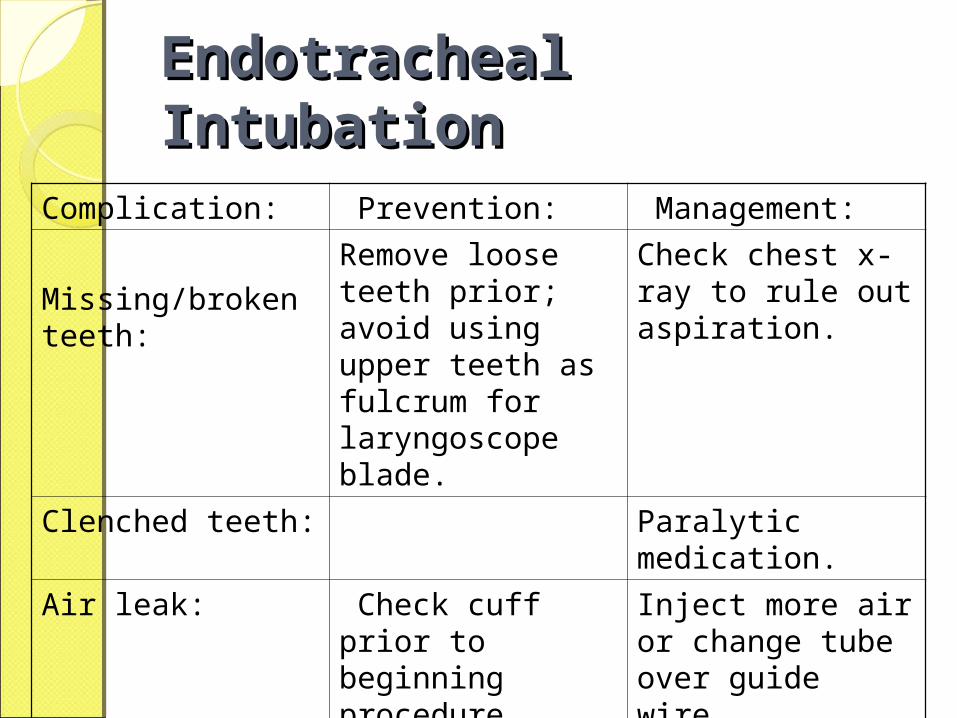
Endotracheal Endotracheal IntubationIntubation
Complication: Prevention: Management:
Missing/broken teeth:
Remove loose teeth prior; avoid using upper teeth as fulcrum for laryngoscope blade.
Check chest x-ray to rule out aspiration.
Clenched teeth: Paralytic medication.
Air leak: Check cuff prior to beginning procedure.
Inject more air or change tube over guide wire.
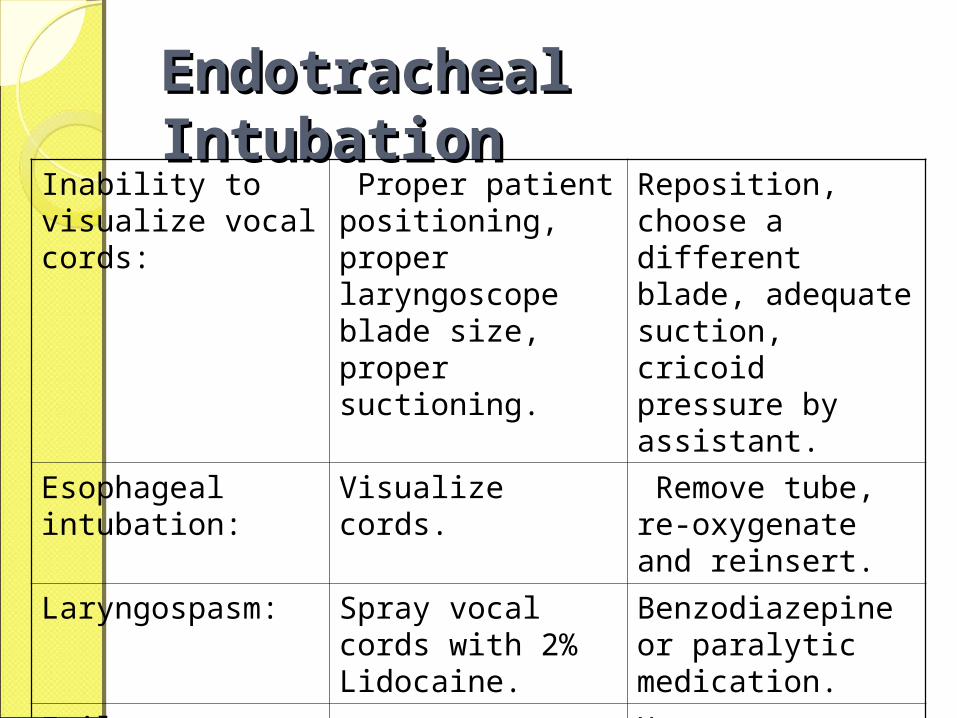
Endotracheal Endotracheal IntubationIntubation
Inability to visualize vocal cords:
Proper patient positioning, proper laryngoscope blade size, proper suctioning.
Reposition, choose a different blade, adequate suction, cricoid pressure by assistant.
Esophageal intubation:
Visualize cords. Remove tube, re-oxygenate and reinsert.
Laryngospasm: Spray vocal cords with 2% Lidocaine.
Benzodiazepine or paralytic medication.
Failure to intubate:
Have alternative plan prepared: cricothyrotomy.
Laryngeal Mask Airway
Laryngeal Mask AirwayIndications:
◦General Anesthesia◦Emergency◦In patients trapped in sitting position◦Unsuccessful intubation
Disadvantages :◦Does not protect lung from
aspiration
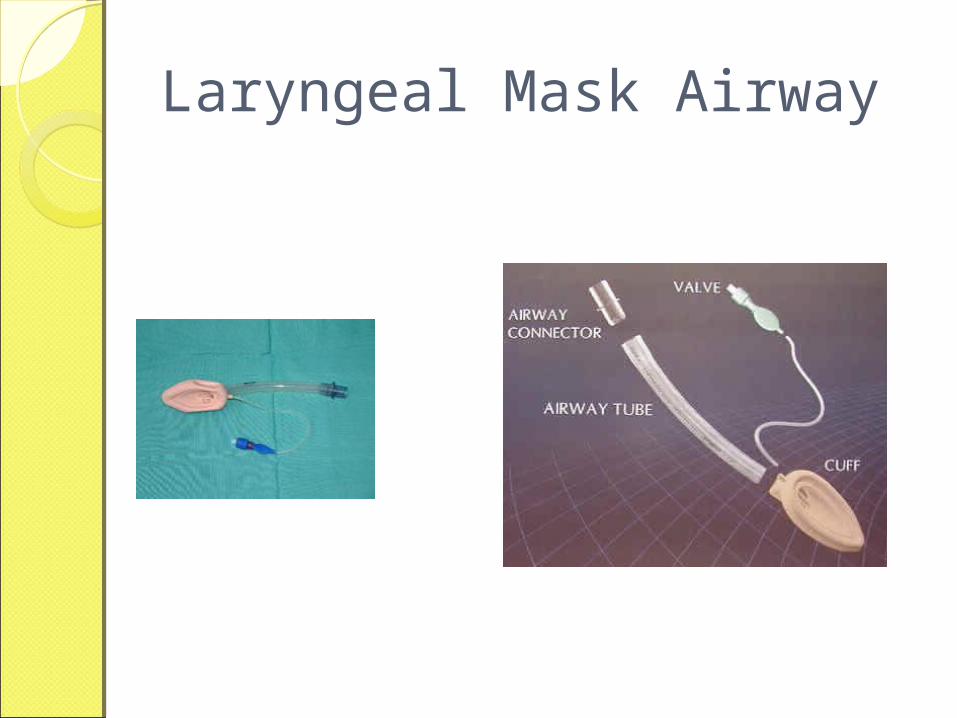
Laryngeal Mask Airway

Laryngeal Mask Airway
Laryngeal Mask AirwayProcedure:
◦ Identify correct size◦ Lubricate◦ Anesthetize◦ Extend neck◦ Insert, follow the curvatures of oropharynx
and rest over pyriform fossa◦ Inflate cuff◦ Check position using sthethoscope◦ Attach to ventilator apparatus
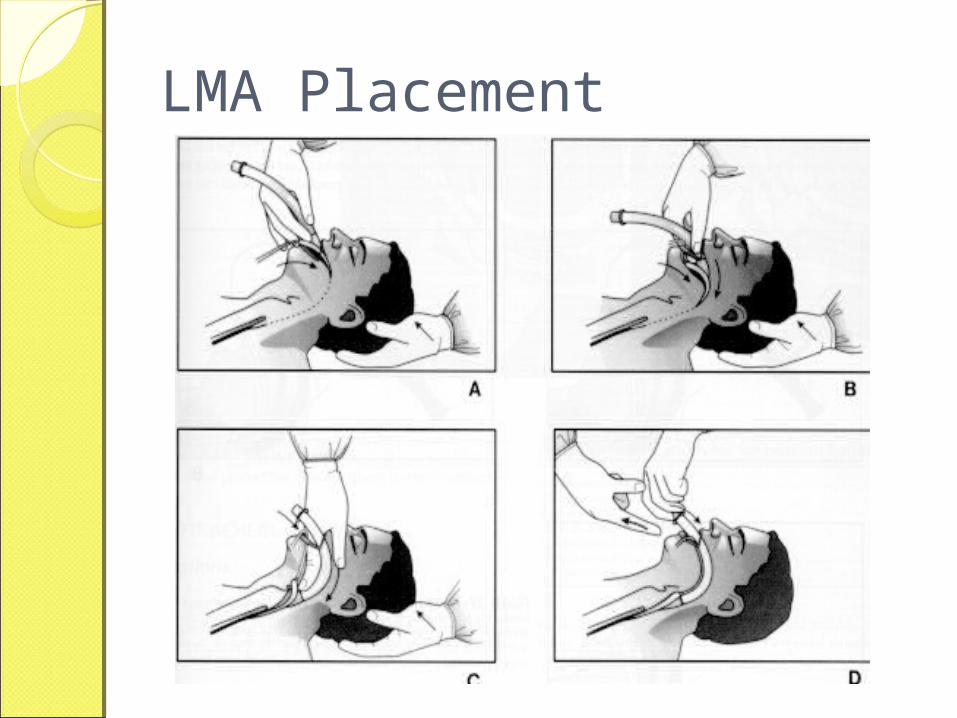
LMA Placement
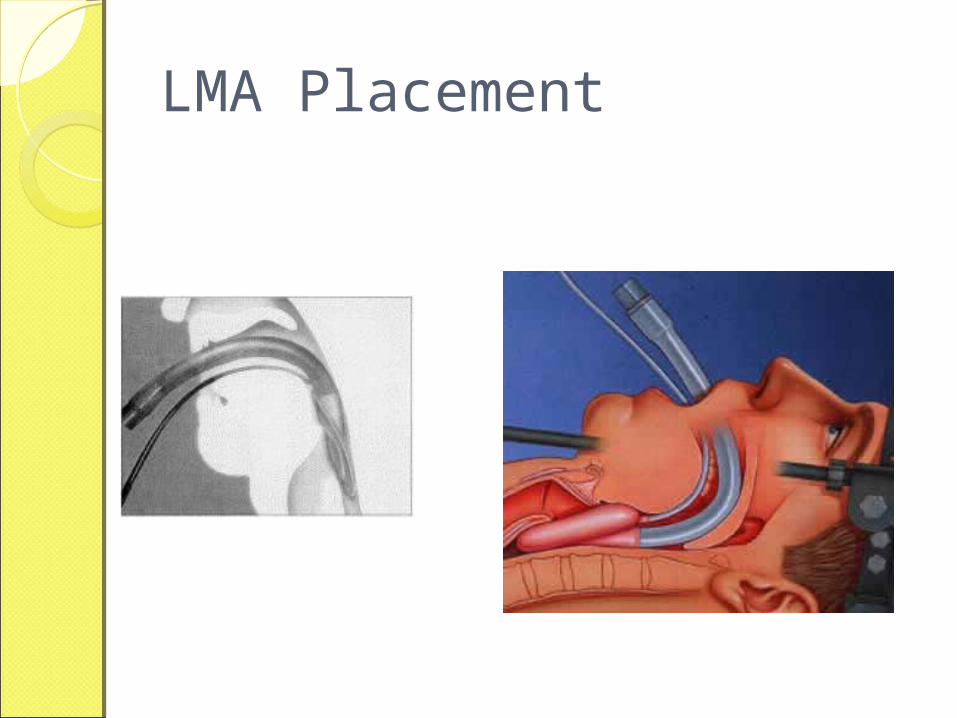
LMA Placement
PharmacologyPharmacology
Pharmacologic Assisted IntubationPharmacologic Assisted Intubation
Sedation◦ Reduce anxiety◦ Induce amnesia◦ Depress gag reflex, spontaneous
breathing◦ Used for
induction anxious, agitated patient
◦ Contraindications hypersensitivity hypotension
Pharmacologic Assisted IntubationPharmacologic Assisted Intubation
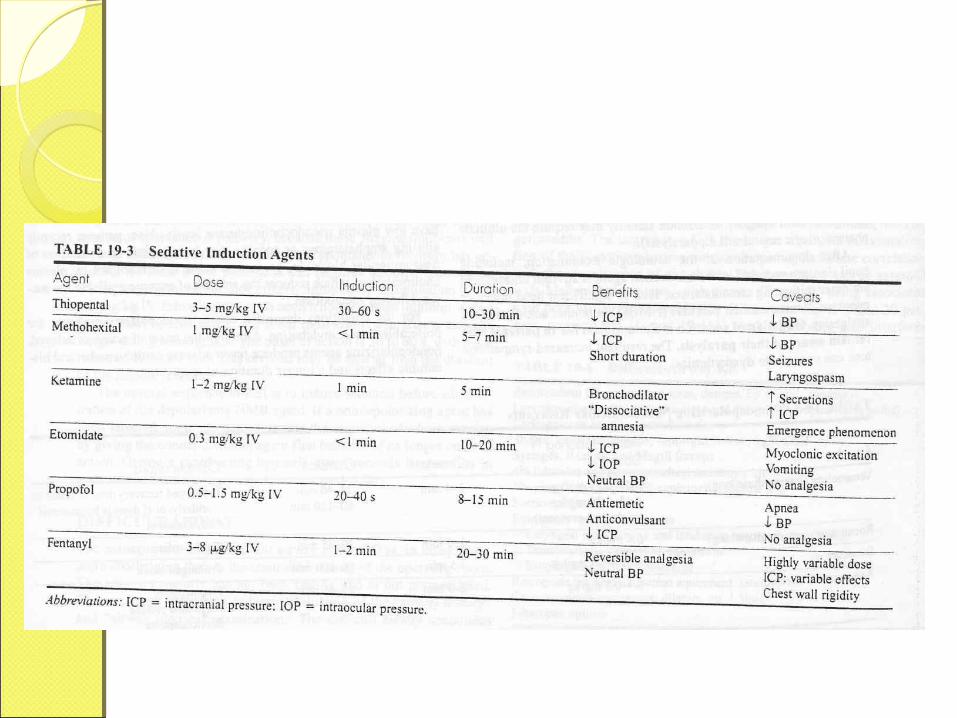
Common Medications for Sedation◦Benzodiazepines (diazepam,
midazolam)◦Narcotics (fentanyl) ◦Anesthesia Induction Agents
Etomidate Ketamine Propofol (Diprivan®)
Pharmacologic Assisted IntubationPharmacologic Assisted Intubation
Indications When intubation required in patient
who: is awake, has gag reflex, or is agitated, combative
Contraindications Most are specific to medication Inability to ventilate once paralysis
induced
Pharmacologic Assisted IntubationPharmacologic Assisted Intubation
Advantages◦ Enables provider to intubate patients who
otherwise would be difficult, impossible to intubate
◦ Minimizes patient resistance to intubation◦ Reduces risk of laryngospasm
Disadvantages/Potential Complications◦ Does not provide sedation, amnesia◦ Provider unable to intubate, ventilate after
NMB◦ Aspiration during procedure◦ Difficult to detect motor seizure activity◦ Side effects, adverse effects of specific
drugs
Pharmacologic Assisted IntubationPharmacologic Assisted Intubation
Mechanism of Action◦ Acts at neuromuscular junction where
ACh normally allows nerve impulse transmission
◦ Binds to nicotinic receptor sites on skeletal muscle
◦ Blocks further action by ACh at receptor sites
◦ These drugs brings about the neuromuscular blockade
Pharmacologic Assisted IntubationPharmacologic Assisted Intubation
Common Used NMB Agents◦Depolarizing NMB agents
succinylcholine (Anectine®) : 2.0 mg/kg result within 60 sec.
◦Non-depolarizing NMB agents vecuronium (Norcuron®) : 0.08-0.12
mg/kg rocuronium (Zemuron®) : 1 mg/kg IV pancuronium (Pavulon®) : 0.15 to 0.2
mg/kg IV
Pharmacologic Assisted IntubationPharmacologic Assisted Intubation
◦Summarized Procedure Prepare all equipment, medications while
ventilating patient Hyperventilate Administer induction/sedation agents
and pretreatment meds (e.g. lidocaine or atropine)
Administer NMB agent Intubate as usual Continue NMB and sedation/analgesia
prn
ConclusionConclusionThe airway management
techniques may be very rarely required in the “Dental Practice”, but when required these techniques differentiate between the Life And Death of the patient.
Thus it is imperative for every dental surgeon to have atleast the basic knowledge of airway management techniques.
Questions ???Questions ???
ReferencesReferencesTextbook of Medical Emergencies, Malame
d.Clinician’s Manual of Oral and Maxillofacial
Surgery, Kwon and LaskinPerforming endotracheal intubation, Cindy
GoodrichTracheostomy and its variants, Dr.Praveen
Kumar www.wikipedia.comwww.medicinenet.orgwww.anesthesiology.orgwww.emtb.comwww.clarus-medical.comwww.fotosearch.com
Thank You!Thank You!