病案討論 -Systemic Lupus Erythematosus 曾素卿 2006/09 曾素卿 2006/09.
46
病病病病 -Systemic Lupus Erythe matosus 病病病 病病病 2006/09 2006/09
-
Upload
claude-brooks -
Category
Documents
-
view
233 -
download
0
Transcript of 病案討論 -Systemic Lupus Erythematosus 曾素卿 2006/09 曾素卿 2006/09.
病案討論-Systemic Lupus Erythematosus
曾素卿 曾素卿 2006/092006/09
The case
General patient informationGeneral patient informationName:Name: 林林 ×× ××
Age:40Age:40Gender:femaleGender:femaleEducation: highEducation: high
Marital status: marriedMarital status: married
Occupation: office ladyOccupation: office ladyAdmission date:94/04/22Admission date:94/04/22Discharge date:94/04/25Discharge date:94/04/25Chart No:61591622Chart No:61591622
Chief complaintChief complaint
Progressive lower limb edema and gain of body Progressive lower limb edema and gain of body weight for about 10 daysweight for about 10 days
Present illness (Present illness (ΙΙ)) A 40-year-old woman was a case of SLE and diagnosA 40-year-old woman was a case of SLE and diagnos
ed at ed at 南門醫院 南門醫院 at age 19. She was under treatment at age 19. She was under treatment at at 東元醫院 東元醫院 and had received several cycles of pulsand had received several cycles of pulse therapy.e therapy.
She had operation history of endometriosis s/p on MShe had operation history of endometriosis s/p on MMH in 1994 and pregnancy with abortion (due to feveMH in 1994 and pregnancy with abortion (due to fever) for two times and an episode of interauterine death, r) for two times and an episode of interauterine death, followed by acute renal failure s/p hemodialysis for 3 followed by acute renal failure s/p hemodialysis for 3 months. months.
Present illness (Present illness (ⅡⅡ)) She sustained from repeated cystitis and PIP in 2001/1She sustained from repeated cystitis and PIP in 2001/1
0 and followed by HPV infected 0 and followed by HPV infected vaginitis in 2002/7. Type lupus nephritis was told fⅣvaginitis in 2002/7. Type lupus nephritis was told fⅣ
rom renal biopsy at rom renal biopsy at 台大醫院台大醫院 . Mrs.Lin appeared to our clinic in 2004/. Mrs.Lin appeared to our clinic in 2004/
2/6 with severe Raynaud’s phenomenom and digital v2/6 with severe Raynaud’s phenomenom and digital vasculitic purpura which were also present over elbowasculitic purpura which were also present over elbows, lower limbs and pretibial area.s, lower limbs and pretibial area.
Present illness (Present illness (ⅢⅢ)) She was admitted to received pulse She was admitted to received pulse therapy and cystitis with vaginitis treatment dutherapy and cystitis with vaginitis treatment du
ring 93/05/14-93/05/20. She was admitted twicring 93/05/14-93/05/20. She was admitted twice to our hospital due to finger and toe tips vasce to our hospital due to finger and toe tips vasculitis and malar rash (2004/5, 2004/7) and herbulitis and malar rash (2004/5, 2004/7) and herbal medicine induce flare.al medicine induce flare.
Present illness (Present illness (ⅣⅣ))
Due to her eager for baby, she refused treatments as pulse aDue to her eager for baby, she refused treatments as pulse and cytotoxics. However, recurrent lower limb edema with nd cytotoxics. However, recurrent lower limb edema with heavy proteinuria despite prednisolone and azathiprine. Hyheavy proteinuria despite prednisolone and azathiprine. Hydroxychloroquine was withheld due to patient’s fear of skidroxychloroquine was withheld due to patient’s fear of skin hyperpigmentation. n hyperpigmentation.
Present illness (Present illness (ⅤⅤ))
Her laboratory tests resulted in Her laboratory tests resulted in
dsDNA=31.9>42>95>626>1850>3100>322>235>61>78>dsDNA=31.9>42>95>626>1850>3100>322>235>61>78>
44.5>144>10.9>4044.5>144>10.9>40
C3/C4=25/10>26/10>38>57>50C3/C4=25/10>26/10>38>57>50
ESR=41>75>91>83>72>53>51>57>50>49ESR=41>75>91>83>72>53>51>57>50>49
alb=2.7>2.5>3.5>2.0 Uprotein=2.77>2.05>5.44>4.7g/dayalb=2.7>2.5>3.5>2.0 Uprotein=2.77>2.05>5.44>4.7g/day
Present illness (Present illness (ⅥⅥ) ) aCLIgG=7.8>17.3GPL/ml(N<1aCLIgG=7.8>17.3GPL/ml(N<10),0),
aCLIgM=3.2>9.8MPL/ml(<7) within 4 months. The antiboaCLIgM=3.2>9.8MPL/ml(<7) within 4 months. The antibodies included Sm(-) RNP(+) SSA(-) SB(-)dies included Sm(-) RNP(+) SSA(-) SB(-)
cryoglobulin(-).cryoglobulin(-).
Marked lower limb edema developed for the past one weeMarked lower limb edema developed for the past one week with difficulty performing daily activity.Albumin level ok with difficulty performing daily activity.Albumin level on 4/19 yielded 2.0. She is admitted for albumin supplement n 4/19 yielded 2.0. She is admitted for albumin supplement and also pulse therapy.and also pulse therapy.
Past Medical HistoryPast Medical History
Systemic lupus erythematosusSystemic lupus erythematosus
Hyperlipidemia (mixed type)Hyperlipidemia (mixed type)
Severe RaynaudSevere Raynaud’’s phenomenons phenomenon
Physical ExaminationPhysical Examination Vital sign:T:36.3 P:98 R:20 BP:120/74Vital sign:T:36.3 P:98 R:20 BP:120/74 Status:ill-lookingStatus:ill-looking Cons:clear, alertCons:clear, alert General:recent weight change(+) fatigue(+)General:recent weight change(+) fatigue(+) gain of body weight:3-4 kg/10 daysgain of body weight:3-4 kg/10 days Skin:rash(+) lumps(+) pruritus(+)Skin:rash(+) lumps(+) pruritus(+)
Extremities:bilateral legs pitting edema LExtremities:bilateral legs pitting edema L’’tt >> RR’’tt
DxDx 1.Systemic lupus erythematosus with lupus 1.Systemic lupus erythematosus with lupus nephritis class with peripheral Ⅳnephritis class with peripheral Ⅳ vasculitis with flare(hypoalbuminemia,vasculitis with flare(hypoalbuminemia, heavy proteinuria) s/p pulse therapyheavy proteinuria) s/p pulse therapy 2.Acute pharyngitis2.Acute pharyngitis 3.Hyperlipidemia(mixed type) 3.Hyperlipidemia(mixed type) 4.Severe Raynaud’s phenomenon4.Severe Raynaud’s phenomenon 5.Insomia5.Insomia

Drug profile藥物劑量藥物劑量 // 頻次頻次 // 使使用方法用方法 // 時間時間
4/224/22 4/234/23 4/244/24 4/254/25
Prednisolone(5 mg) taPrednisolone(5 mg) tab po b po
6# st6# st 4# qd4# qd
MethylprednisoloneMethylprednisolone
(500 mg) 2 vial in D5(500 mg) 2 vial in D5W 100 cc iv dripW 100 cc iv drip
qdqd qdqd
Albumin 25% 1 BT iv Albumin 25% 1 BT iv dripdrip
qdqd qdqd qdqd
Lasix(20 mg) 1 amp Lasix(20 mg) 1 amp post albumin iv post albumin iv
qdqd qdqd qdqd
Lasix (40 mg) tab po Lasix (40 mg) tab po 1#bid1#bid 1#q8h1#q8h 1#q8h1#q8h 1#qd1#qd
Lipitor(10 mg) po Lipitor(10 mg) po 1#qd pm1#qd pm
Brown mixture Brown mixture
15 cc po 15 cc po qidqid qidqid qidqid qidqid
Problem listProblem list
1.SLE with lupus nephritis class with peripheraⅣ1.SLE with lupus nephritis class with peripheraⅣl vasculitisl vasculitis
2.Hypoalbuminemia2.Hypoalbuminemia
3.Hyperlipidemia(mixed type)3.Hyperlipidemia(mixed type)
Discussion SLE with lupus nephritis class with peripⅣheral vasculitis
S:S: progression lower limb edema and gain of body progression lower limb edema and gain of body weight for about 10 daysweight for about 10 days
O:O: 1.Gain of body weight:3-4 kg/10 days1.Gain of body weight:3-4 kg/10 days 2.Extremities:bilateral legs pitting edema L’t2.Extremities:bilateral legs pitting edema L’t >> R’tR’t
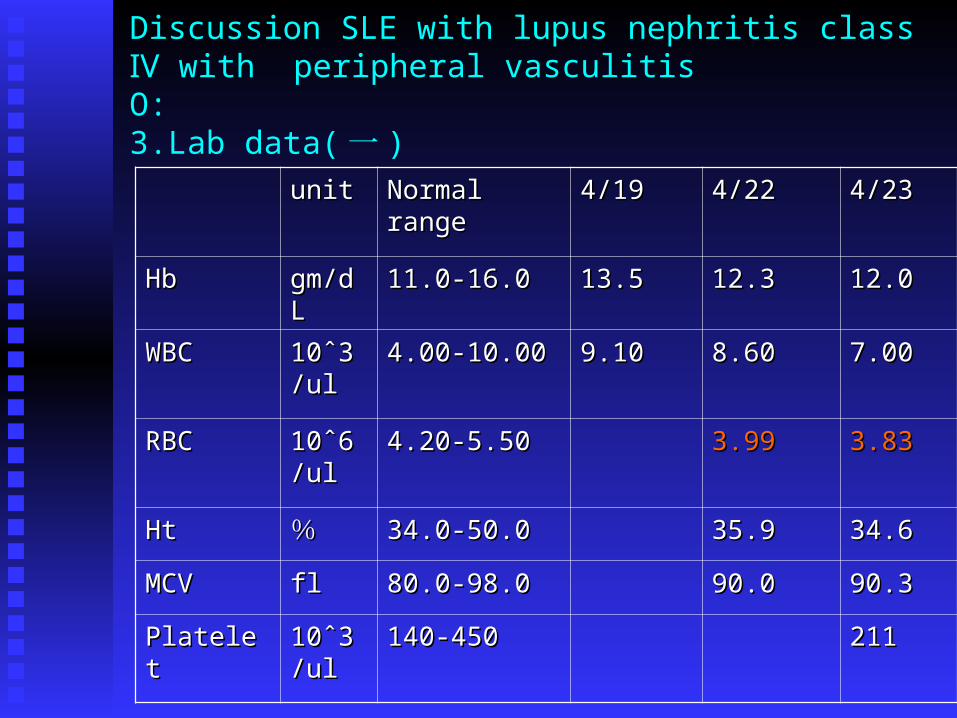
Discussion SLE with lupus nephritis class with peripheral ⅣvasculitisO:3.Lab data( 一 )
unitunit Normal Normal rangerange
4/194/19 4/224/22 4/234/23
HbHb gm/dLgm/dL 11.0-16.011.0-16.0 13.513.5 12.312.3 12.012.0
WBCWBC 10ˆ310ˆ3/ul/ul
4.00-10.004.00-10.00 9.109.10 8.608.60 7.007.00
RBCRBC 10ˆ610ˆ6/ul/ul
4.20-5.504.20-5.50 3.993.99 3.833.83
HtHt %% 34.0-50.034.0-50.0 35.935.9 34.634.6
MCVMCV flfl 80.0-98.080.0-98.0 90.090.0 90.390.3
PlatelePlatelett
10ˆ310ˆ3/ul/ul
140-450140-450 211211
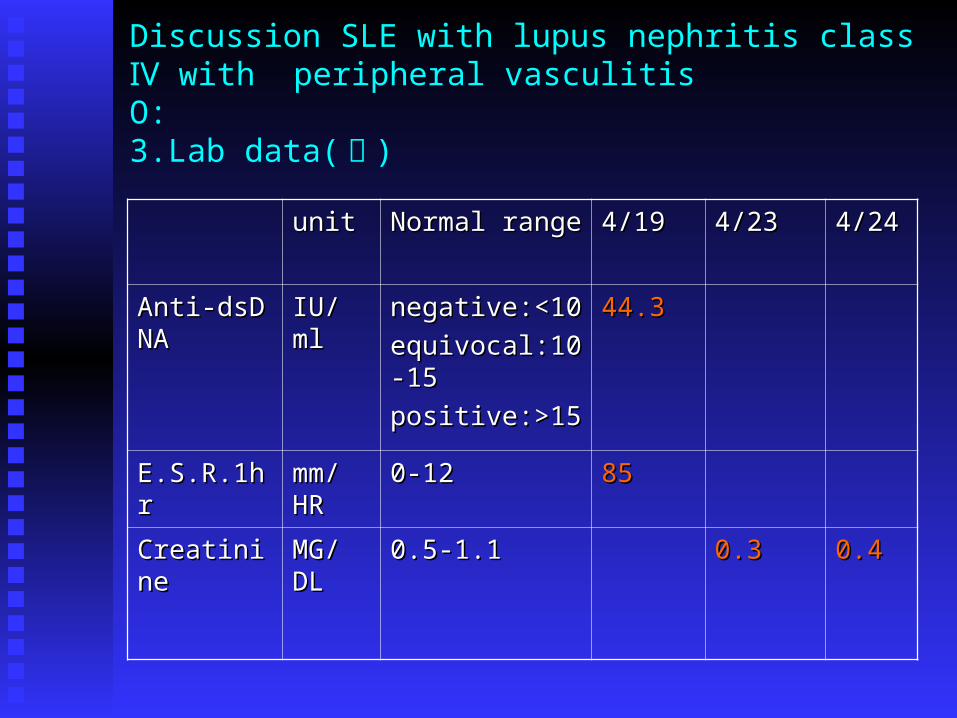
Discussion SLE with lupus nephritis class with peripheral ⅣvasculitisO:3.Lab data( 二 )
unitunit Normal Normal range range
4/194/19 4/234/23 4/244/24
Anti-dsDNAAnti-dsDNA IU/IU/mlml
negative:<1negative:<100
equivocal:1equivocal:10-150-15
positive:>1positive:>155
44.344.3
E.S.R.1hE.S.R.1hrr
mm/mm/HRHR
0-120-12 8585
CreatinineCreatinine MG/MG/DLDL
0.5-1.10.5-1.1 0.30.3 0.40.4
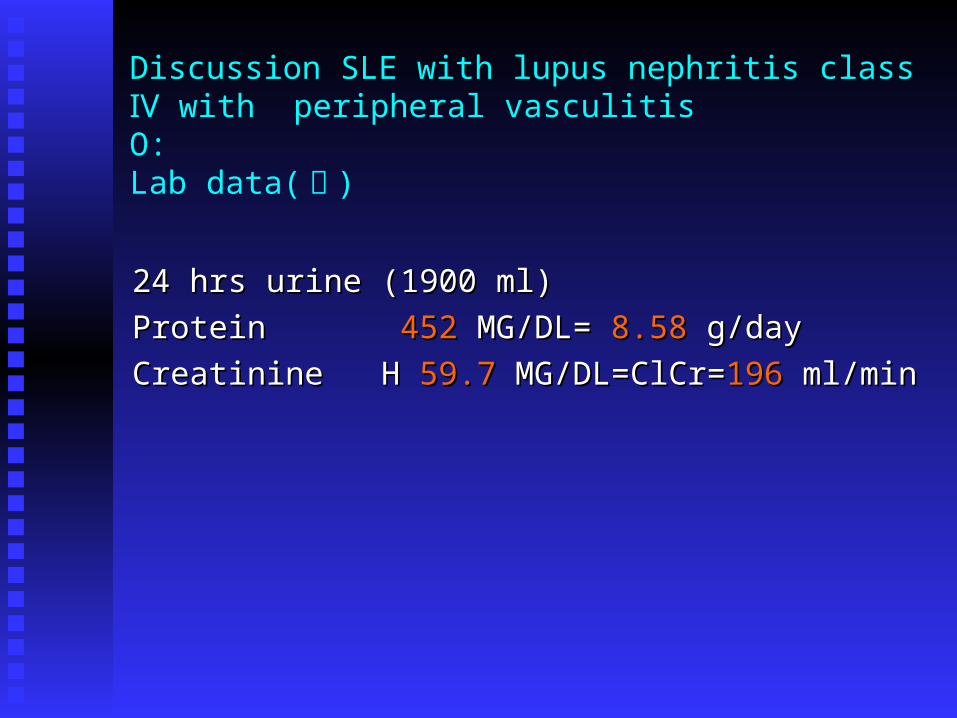
Discussion SLE with lupus nephritis class with peripheral ⅣvasculitisO: Lab data( 三 )
24 hrs urine (1900 ml)24 hrs urine (1900 ml)
Protein Protein 452452 MG/DL= MG/DL= 8.588.58 g/day g/day
Creatinine H Creatinine H 59.759.7 MG/DL=ClCr= MG/DL=ClCr=196196 ml/min ml/min
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Assessment:Assessment:
1.This patient is belong to WHO grade IV, 1.This patient is belong to WHO grade IV, [diffuse proliferative lupus nephritis (DPL[diffuse proliferative lupus nephritis (DPLN) affecting >50% of glomeruli] aggressive N) affecting >50% of glomeruli] aggressive immunosuppression is recommended.immunosuppression is recommended.
If untreated, develop end-stage renal disease If untreated, develop end-stage renal disease (ESRD) within 2 years.(ESRD) within 2 years.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Assessment:Assessment: 2.This 2.This patients with dangerous proliferative forms of glomerpatients with dangerous proliferative forms of glomer
ular damage and proteinuria (>500 mg per 24 h) therefore, ular damage and proteinuria (>500 mg per 24 h) therefore, aggressive immunosuppression is indicated (usually systeaggressive immunosuppression is indicated (usually systemic glucocorticoids plus a cytotoxic drug) but proteinuria imic glucocorticoids plus a cytotoxic drug) but proteinuria is less likely to improve on lupus nephritis immunosuppresss less likely to improve on lupus nephritis immunosuppressive therapies. Lupus nephritis tends to be an ongoing diseaive therapies. Lupus nephritis tends to be an ongoing disease, with flares requiring re-treatment over many years. se, with flares requiring re-treatment over many years.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Assessment:Assessment:
3.Treat with monthly intravenous 3.Treat with monthly intravenous cyclophosphamide,500 to 1000 mg/m2 body cyclophosphamide,500 to 1000 mg/m2 body surface area for 6 months,along with high-dose surface area for 6 months,along with high-dose corticosteroids (usually initially pulse corticosteroids (usually initially pulse methylprednisolone,1000 mg/d for 3 methylprednisolone,1000 mg/d for 3 days,followed by prednisone,40 to 60 mg/d,for the days,followed by prednisone,40 to 60 mg/d,for the first month), may be benefit for this patient.first month), may be benefit for this patient.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Assessment:Assessment:
4. Due to her eager for baby, this patient 4. Due to her eager for baby, this patient
refused treatments.refused treatments.
Therefore consider other drugs like Therefore consider other drugs like
azathioprine or mycophenolate.azathioprine or mycophenolate.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Assessment:Assessment:
5.5. Azathioprine (a purine antagonist) added to glucocorticoi Azathioprine (a purine antagonist) added to glucocorticoids probably reduces the number of SLE flares and the maids probably reduces the number of SLE flares and the maintenance glucocorticoid requirement; however, this approantenance glucocorticoid requirement; however, this approach requires several months to be effective, and cyclophospch requires several months to be effective, and cyclophosphamide is effective in a higher proportion of patients. Dailhamide is effective in a higher proportion of patients. Daily oral azathioprine may have fewer adverse effects than day oral azathioprine may have fewer adverse effects than daily oral cyclophosphamide; ily oral cyclophosphamide;
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Assessment:Assessment:
6.A recent prospective study in Chinese patients wit6.A recent prospective study in Chinese patients with lupus nephritis comparing daily oral mycophenoh lupus nephritis comparing daily oral mycophenolate plus prednisolone for 12 months to daily oral late plus prednisolone for 12 months to daily oral cyclophosphamide plus prednisolone for 6 months cyclophosphamide plus prednisolone for 6 months followed by oral daily azathioprine plus prednisolfollowed by oral daily azathioprine plus prednisolone showed good improvement in 80% of patients one showed good improvement in 80% of patients in both groups at 1 year of follow-up and fewer adin both groups at 1 year of follow-up and fewer adverse effects with mycophenolate. verse effects with mycophenolate.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Assessment:Assessment:
77.Pregnancy and lupus:.Pregnancy and lupus:
this patient should avoid becoming pregnant this patient should avoid becoming pregnant
before disease stable.before disease stable.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Plan:Plan:
1.Recommended drug treatment:1.Recommended drug treatment:
pulse therapy :systemic glucocorticoids(0.5~2mg/kg per dpulse therapy :systemic glucocorticoids(0.5~2mg/kg per day orally or 1000 mg of methylprednisolone sodium succinay orally or 1000 mg of methylprednisolone sodium succinate intravenously daily) for 3 days. ate intravenously daily) for 3 days.
maintenance therapy: combine corticosteroids(5~10 mg/damaintenance therapy: combine corticosteroids(5~10 mg/day)and immunosuppressive drugs[azathioprine (1~2 mg/kg/y)and immunosuppressive drugs[azathioprine (1~2 mg/kg/d) or mycophenolate(500~1500 mg/d)].d) or mycophenolate(500~1500 mg/d)].
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Plan:Plan:
2.Goal:2.Goal:
There is no cure for SLE, and complete sustained There is no cure for SLE, and complete sustained remissions are rare. Therefore, the physician should plan to remissions are rare. Therefore, the physician should plan to control acute, severe flares then develop maintenance control acute, severe flares then develop maintenance strategies that suppress symptoms to an acceptable level strategies that suppress symptoms to an acceptable level and prevent organ damage. and prevent organ damage.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Plan:Plan: 3.Monitoring parameters:3.Monitoring parameters: It is useful to follow tests that indicate the status of organ iIt is useful to follow tests that indicate the status of organ i
nvolvement known to be present during SLE flares. These nvolvement known to be present during SLE flares. These might include hemoglobin levels, platelet counts, urinalysimight include hemoglobin levels, platelet counts, urinalysis, and serum levels of creatinine or albumin. There is great s, and serum levels of creatinine or albumin. There is great interest in identification of additional markers of disease acinterest in identification of additional markers of disease activity. Candidates include levels of anti-dsDNA antibodies, tivity. Candidates include levels of anti-dsDNA antibodies, several components of complement (C'3 is most widely avseveral components of complement (C'3 is most widely available), activated complement products, soluble interleukiailable), activated complement products, soluble interleukin (IL)n (IL)22, and urinary monocyte chemotactic protein 1. , and urinary monocyte chemotactic protein 1.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Plan:Plan: 4.Patient education4.Patient education · Stress the importance of compliance with drug regimen · Stress the importance of compliance with drug regimen and follow-up visits.and follow-up visits. · When starting treatment with prednisone, inform · When starting treatment with prednisone, inform patients about weight control, low-fat diet, and patients about weight control, low-fat diet, and exercise.exercise. · Advise patients about proper use and side effect · Advise patients about proper use and side effect profiles of other medications used in treating profiles of other medications used in treating SLESLE.. · Counsel the patient about the importance of developing · Counsel the patient about the importance of developing a social support system that will provide feedback a social support system that will provide feedback about lupus self-management behaviors, problem solving,about lupus self-management behaviors, problem solving, and alternate solution planning.and alternate solution planning.
Discussion SLE with lupus nephritis class with peripheral Ⅳvasculitis
Plan:Plan:
5.5.Institute measures to prevent steroid-induced osteoporosiInstitute measures to prevent steroid-induced osteoporosis. s.
.Vitamin D and calcium supplementation .Vitamin D and calcium supplementation . Weight-bearing exercise. Weight-bearing exercise .Bisphosphonates or HRT; unless otherwise .Bisphosphonates or HRT; unless otherwise contraindicated, alendronate and HRT can both be used.contraindicated, alendronate and HRT can both be used.
Discussion Hypoalbuminemia
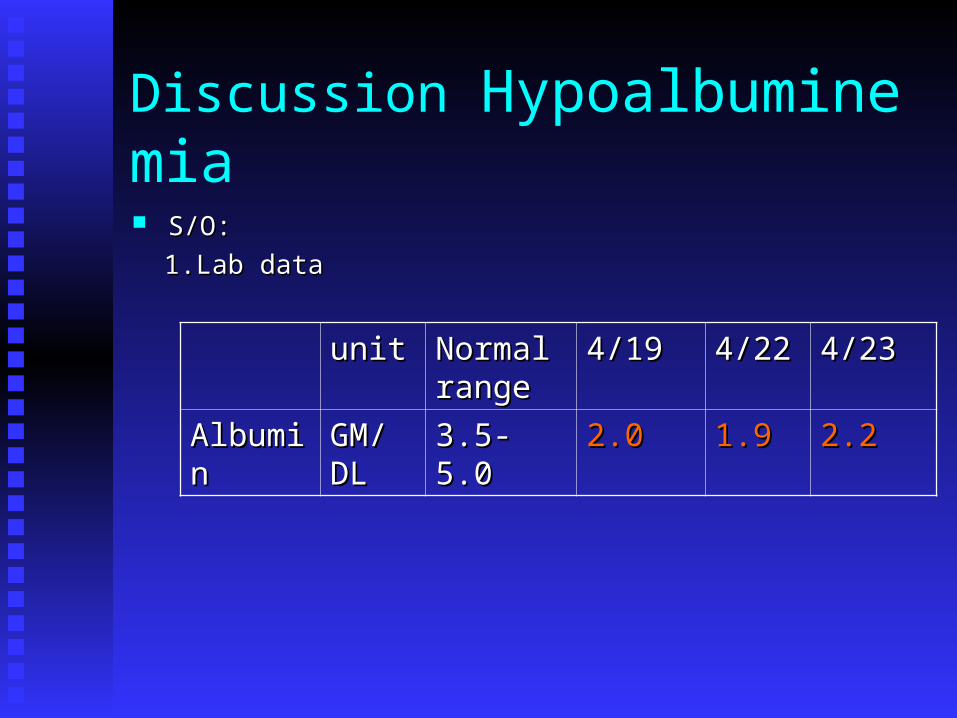
S/O:S/O:
1.Lab data1.Lab data
unitunit Normal Normal rangerange
4/194/19 4/224/22 4/234/23
AlbumiAlbuminn
GM/GM/DLDL
3.5-3.5-5.05.0
2.02.0 1.91.9 2.22.2
Discussion Hypoalbuminemia
Assessment:Assessment:
1.Hypoalbuminemia,a characteristic feature of the 1.Hypoalbuminemia,a characteristic feature of the nephrotic syndrome, results from augmentation of nephrotic syndrome, results from augmentation of both urinary albumin lossess and the catabolic rate both urinary albumin lossess and the catabolic rate of albumin.of albumin.
2.This is a temporary measure, since the infused alb2.This is a temporary measure, since the infused albumin only transiently increase serum albumin and umin only transiently increase serum albumin and is promptly excreted in the urine.is promptly excreted in the urine.
Discussion Hypoalbuminemia
Plan:Plan:
1.Recommended drug treatment:1.Recommended drug treatment:
25% albumin 1BT iv drip, then25% albumin 1BT iv drip, then
furosemide(40mg) 1 amp for 3 days.furosemide(40mg) 1 amp for 3 days.
Discussion Hypoalbuminemia
Plan:Plan:
2.Goal:2.Goal:
treatment of the underlying disorder and an treatment of the underlying disorder and an adequate protein diet combined with adequate protein diet combined with intervention aimed at reducing protein intervention aimed at reducing protein excretion may be beneficial.excretion may be beneficial.
Discussion Hypoalbuminemia
Plan:Plan:
3.Monitoring parameters:3.Monitoring parameters:
periodic measurement of serum albumin periodic measurement of serum albumin levels.levels.
4.Diet:4.Diet:
an adequate protein diet.an adequate protein diet.
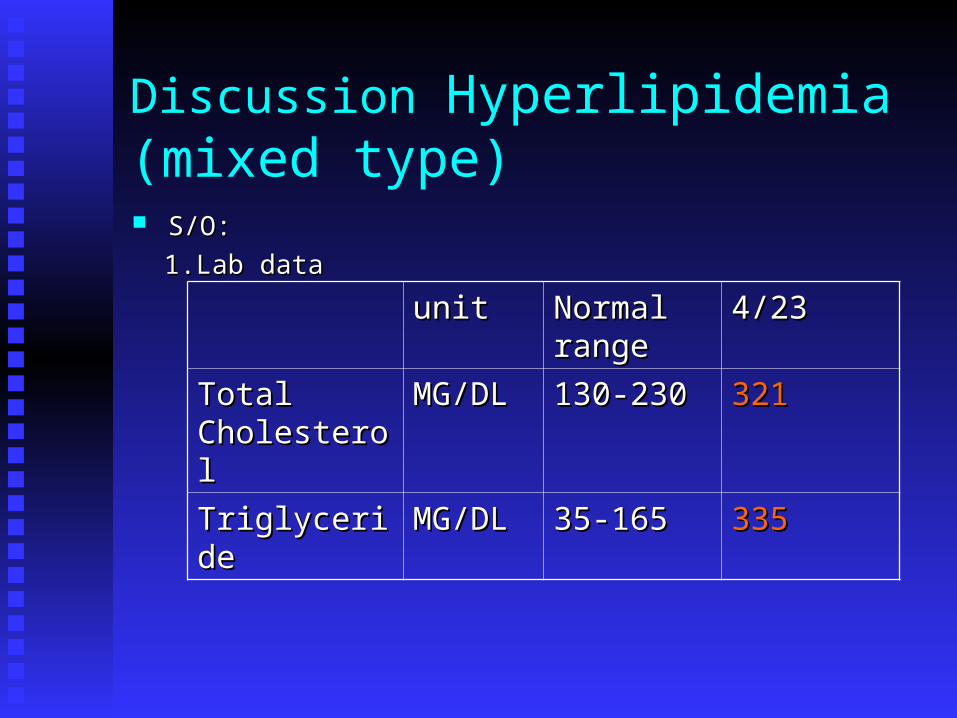
Discussion Hyperlipidemia(mixed type) S/O:S/O:
1.Lab data1.Lab data
unitunit Normal Normal rangerange
4/234/23
Total Total CholesteroCholesteroll
MG/DLMG/DL 130-230130-230 321321
TriglyceriTriglyceridede
MG/DLMG/DL 35-16535-165 335335
Discussion Hyperlipidemia(mixed type) Assessmrent:Assessmrent:
1.Lipid abnormalities including TC and TG have been descr1.Lipid abnormalities including TC and TG have been described in this patients.ibed in this patients.
2.This patients are at an increased risk for atherosclerotic ca2.This patients are at an increased risk for atherosclerotic cardiovascular disease. Since the lipid abnormalities seen in rdiovascular disease. Since the lipid abnormalities seen in nephrotic syndrome are associated with accelerated atherosnephrotic syndrome are associated with accelerated atherosclerosis. clerosis.
Discussion Hyperlipidemia(mixed type) Plan:Plan:
1.Recommended drug treatment:1.Recommended drug treatment:
Atorvastatin 10 mg qd am(without regard tAtorvastatin 10 mg qd am(without regard to time of day and with food if desired)o time of day and with food if desired)
2.Acquire other lipoprotein level eg. LDL, 2.Acquire other lipoprotein level eg. LDL, HDL.HDL.
Discussion Hyperlipidemia(mixed type) Plan:Plan:
2.Goal:2.Goal:
a. a. Reduce the risk of atherosclerosis in patient with SLE.Reduce the risk of atherosclerosis in patient with SLE.
b. NCEP( National Cholesterol Education Program)-b. NCEP( National Cholesterol Education Program)-ATPATP suggested TC level<200 mg/dl and TG<150 mg/dl.Ⅲ suggested TC level<200 mg/dl and TG<150 mg/dl.Ⅲ
Discussion Hyperlipidemia(mixed type) Plan:Plan: 3.Monitoring parameters:3.Monitoring parameters: Lipid levels after 2-4 wks; LFTs, CPK.Lipid levels after 2-4 wks; LFTs, CPK. It is recommended that liver function tests(LIt is recommended that liver function tests(L
FTs) be performed prior to and at 12 wks foFTs) be performed prior to and at 12 wks following both the initiation of therapy and elllowing both the initiation of therapy and elevation in dose, and periodically (eg. semiaevation in dose, and periodically (eg. semiannually) thereafter.nnually) thereafter.
Discussion Hyperlipidemia(mixed type) Plan:Plan:
4.Patient education:4.Patient education:
Dietary therapy and lifestyle modifications should Dietary therapy and lifestyle modifications should be tried for 3 months.be tried for 3 months.
Nondrug and drug therapy should be initiated simuNondrug and drug therapy should be initiated simultaneously. Increasing physical activity will aid in ltaneously. Increasing physical activity will aid in the treatment of hyperlipidemia and improve cardithe treatment of hyperlipidemia and improve cardiovascular health.ovascular health.
謝謝聆聽謝謝聆聽 ,, 敬請指教敬請指教 !!!!
1.WHO has classified lupus nephritis as six grades, the patient belong to g1.WHO has classified lupus nephritis as six grades, the patient belong to grade ?rade ?
(d) a.(d) a. (no histologic changes) b. (proliferative changes confined to the Ⅰ Ⅱ(no histologic changes) b. (proliferative changes confined to the Ⅰ Ⅱmesangium) c. (proliferative changes in tufts of 10 to 50% of glomerⅢmesangium) c. (proliferative changes in tufts of 10 to 50% of glomerⅢuli) d (diffuse proliferative affecting>50% of glomeruli)Ⅳuli) d (diffuse proliferative affecting>50% of glomeruli)Ⅳ
2.Which drug 2.Which drug has become the standard drug used for controlling life-has become the standard drug used for controlling life-(a) threatening active lupus nephritis, particularly in patients whose renal (a) threatening active lupus nephritis, particularly in patients whose renal
biopsies show WHO grades III, IV, and V proliferative or membranopbiopsies show WHO grades III, IV, and V proliferative or membranoproliferative forms of nephritis?roliferative forms of nephritis?
a.cyclophosphamide b.azathioprne c.mycophenolatea.cyclophosphamide b.azathioprne c.mycophenolate3.Which one is side effect of cyclophosphamide?3.Which one is side effect of cyclophosphamide?(e) a. high rate of irreversible ovarian or testicular failure b. nausea c. mal(e) a. high rate of irreversible ovarian or testicular failure b. nausea c. mal
aise d. alopecia e.aise d. alopecia e. 以上皆是以上皆是4.Wnen flare, anti-ds DNA and serum C4.Wnen flare, anti-ds DNA and serum C33 will be? will be?(c) a. high anti-ds DNA , high C(c) a. high anti-ds DNA , high C33 b. low anti-ds DNA , low C b. low anti-ds DNA , low C33 c.high anti- c.high anti-
ds DNA , low Cds DNA , low C3 3 d. high anti-ds DNA , high Cd. high anti-ds DNA , high C33..5.5. 使用使用 statinsstatins 藥物時藥物時 ,, 要監測何值要監測何值 ??(d) a. lipid level b. liver function tests c. CPK d.(d) a. lipid level b. liver function tests c. CPK d. 以上皆是以上皆是
Document at least four of the following American College of Rheumatology classification criteria
Positive ANAPositive ANA Malar rashMalar rash Discoid lupusDiscoid lupus PhotosensitivityPhotosensitivity Oral ulcersOral ulcers Arthritis Arthritis SerositisSerositis Renal disorderRenal disorder Neurologic disorderNeurologic disorder Hematologic disorderHematologic disorder Immunologic disorderImmunologic disorder

1.If the benefits from use in pregnant women may be accept1.If the benefits from use in pregnant women may be acceptable despite the risk (e.g., if the drug is needed in a life-thrable despite the risk (e.g., if the drug is needed in a life-threatening situation or for a serious disease for which safer deatening situation or for a serious disease for which safer drugs cannot be used or are ineffective). rugs cannot be used or are ineffective).
2.Maternal SLE should be controlled with prednisone/predni2.Maternal SLE should be controlled with prednisone/prednisolone at thesolone at the lowest effective doses for the shortest time required. lowest effective doses for the shortest time required.
懷孕分級懷孕分級azathioprineazathioprine DD
mycophenolatemycophenolate CC
prednisoloneprednisolone CC
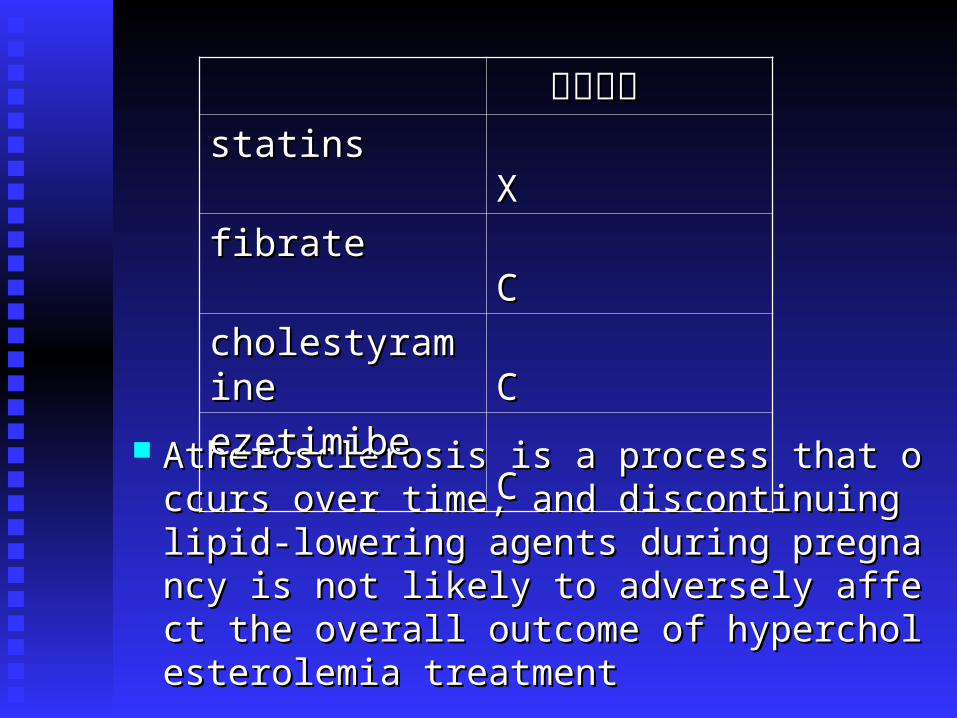
Atherosclerosis is a process that occurs over Atherosclerosis is a process that occurs over time, and discontinuing lipid-lowering agentime, and discontinuing lipid-lowering agents during pregnancy is not likely to adverselts during pregnancy is not likely to adversely affect the overall outcome of hypercholesty affect the overall outcome of hypercholesterolemia treatment erolemia treatment
懷孕分級懷孕分級statinsstatins XX
fibratefibrate CC
cholestyraminecholestyramine CC
ezetimibeezetimibe CC