Rehabilitation for Patients with Cardiovascular Disease MR
MA
Slide 2
Book Reading ACSM's Resource Manual for Guidelines for
Exercises Testing and Prescription Chapter 35 Exercise Prescription
in Patients with Cardiovascular Disease Braddom Chapter 34 Cardiac
Rehabilitation DeLisa Chapter 83 Cardiac Rehabilitation
Slide 3
Background 18 ~ 65 years old healthy adults need
1.Moderate-intensity activity at least 30 minutes on 5 days per
week Or Vigorous-intensity aerobic activity at least 20 minutes on
3 days per week 2.Resistance training involving the major muscle
groups at least 2 days per week Exercise is also recommended for
the elderly or people with illness
Slide 4
Canadian Family Physician,
http://www.cfpc.ca/cfp/2002/jan/vol48-jan-cme-1.asp DeLisa Table
83-7
Slide 5
Cardiac Rehabilitation 1.Introduction of Cardiac Rehabilitation
2.Disease-Specific Effects on Physiologic Responses and Fitness
3.Scientific and Physiologic Rationale for Exercise Therapy in
Patients with Heart Disease 4.Morbidity, Mortality, and Safety of
Cardiac Rehabilitation 5.Exercise Prescription and Programming
Slide 6
Definition Cardiac rehabilitation is an interdisciplinary team
approach to patients with functional limitations secondary to heart
disease
Slide 7
Goals Restore patients to their optimal medical, physical,
psycological, social, emotional, sexual, vocational, and economic
status compatible with the severity of their heart disease
Prevention of heart disease Primary screen healthy people to
identify and treat risk factors Secondary to improve heart disease
risk factors and limit further morbidity and mortality
Slide 8
Cardiac Rehabilitation 1.Introduction of Cardiac Rehabilitation
2.Disease-Specific Effects on Physiologic Responses and Fitness
3.Scientific and Physiologic Rationale for Exercise Therapy in
Patients with Heart Disease 4.Morbidity, Mortality, and Safety of
Cardiac Rehabilitation 5.Exercise Prescription and Programming
Slide 9
Cardiovascular Response during Exercise Heart Rate Normal
Achieving HR within 2 standards deviations of an age-predicted
maximum value Decreasing HR to baseline fairly quickly during
recovery
Slide 10
Cardiovascular Response during Exercise Heart Rate Abnormal
Chronotropic Incompetence Failure to achieve 85% predicted maximum
HR (without medication effect) Predict CAD and associated with
increased risk of Mortality/Morbidity Abnormal HR recovery alking:
decrease in HR < 12 bpm / 1 minute Supine: decrease in HR <
22 bpm / 2 minutes Predict future cardiac mortality
Slide 11
Cardiovascular Response during Exercise Blood Pressure Normal
DBP: Constant or slightly decrease SBP: Increase progressively
about 8~12 mmHg/MET, with a plateau at peak exercise Abnormal In
patients with CAD, SBP during exercise may respond normally or may
disproportionately increase or inappropriately decrease
Slide 12
Cardiovascular Response during Exercise Blood Pressure Abnormal
Exertional hypertension: SBP > 250 mmHg or DBP > 115 mmHg
Exertional hypotension: Compare to resting BP, SBP decrease 10mmHg
Exertional systolic hypertension/hypotension would increase cardiac
event risk Increase DBP 10mmHg Often a marker for future
hypertension
Slide 13
Cardiovascular Response during Exercise Cardiac Output and
Oxygen uptake Normal Peak VO2: 30~45 ml/kg/min CAD patient Peak VO2
reduction 20% Due to Cardiac Output Cardiac Output = Heart Rate x
Strove volume Heart Rate Chronotropic incompetence Strove Volume
Left ventricular dysfunction With Exercise Training VO215~30%
Slide 14
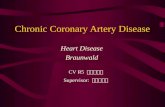
Oxygen Consumption 1 MET (Metabolic Equivalent) = Oxygen
consumption at resting = Basal metabolic rate At rest, 70kg man O2
consumption = 3.5ml oxygen/ minute/ Kg of BW Braddom Figure 34-1
Relationship between oxygen consumption and intensity of work being
performed.
Slide 15
LevelSelf-careHouseholdRecreationalVocational Light (1-3
metabolic equivalents, METS) Sponge bathing Shaving Dressing or
undressing Preparing light meals Setting table Dusting Walking 2
mph Writing Reading Playing piano Typing Light machine work
Lifting
ACSM s TABLE 35-2. Pathophysiologic Effects of Exercise and
Exercise Training Pathophysiologic VariableAcute ExerciseChronic
Exercise Training Vascular Vascular stenosisPartial regression
(>2200 kcalwk -1 ) Coronary collaterals Endothelial dysfunction
Capillary flow Autonomic nervous symptoms Parasympathetic
Sympathetic Hemostatic Fibrinogen Factor VII Platelet aggregation
Fibrinolysis Viscosity 1400 kcal per week showed improved
cardiopulmonary fitness >1500 kcal per week demonstrated the
slowest rate of disease progression >2200 kcal per week showed
regression of CAD
Slide 25
Cardiac Rehabilitation 1.Introduction of Cardiac Rehabilitation
2.Disease-Specific Effects on Physiologic Responses and Fitness
3.Scientific and Physiologic Rationale for Exercise Therapy in
Patients with Heart Disease 4.Morbidity, Mortality, and Safety of
Cardiac Rehabilitation 5.Exercise Prescription and Programming
Slide 26
Morbidity, Mortality, and Safety of Cardiac Rehabilitation
Total cardiovascular mortality are reduced in patients following
myocardial infarction who participate in cardiac rehabilitation
exercise training The 1995 Agency for Heath Care Policy and
Research (AHCPR) Clinical Practice Guidelines for Cardiac
Rehabilitation Cardiac rehabilitation reduced all-cause mortality
by approximately 25% Taylor RS, Brown A, Ebrahim S, et al.
Exercise-based rehabilitation for patients with coronary heart
disease: systematic review and meta-analysis of randomized
controlled trials. Am J Med. 2004;116:682 692.
Slide 27
Classification of Cardiac Rehabilitation Inpatient phase
Minimize the de-conditioning time Education about risk factors and
lifestyle modification Early outpatient phase Maintenance phase
Follow-up phase Differing based on extent of supervision and
monitoring, subject independence, and time from the event Improve
exercise performance and modify cardiac risk factors
Slide 28
Cardiac Test Rest/ Exercise cardiac test should be performed
before prescription Cardiac Testing Resting EKG, CXR, 2D- echo,
Holter exam, Coronary angiography, Cardiac exercise stress test
Cardiac exercise stress test is generally safe, and adverse
outcomes are infrequent
Slide 29
Cardiac Exercise Stress Test Modality Treadmill, Bicycle, Arm
ergometers Dipyridamole, Adenosine End point Normal EST = 85%
age/gender predicted HR max Symptom-limited maximum EST Low-level
submaximal EST HR = 120 70% HR max Peak MET = 5
Slide 30
Braddom Box 34-6 Contraindications to exercise stress testing
Absolute Acute myocardial infarction (within 2 days) High-risk
unstable angina Uncontrolled cardiac arrhythmias causing symptoms
of hemodynamic compromise Symptomatic severe aortic stenosis
Uncontrolled symptomatic congestive heart failure Acute pulmonary
embolus or pulmonary infarction Acute myocarditis or pericarditis
Acute aortic dissection Relative Left main coronary artery disease
Moderate stenotic valvular heart disease Electrolyte abnormalities
A Severe arterial hypertension (> 200 mmHg systolic blood
pressure and/or 110 mmHg diastolic blood pressure) Tachyarrhythmias
or bradyarrhythmias Hypertrophic cardiomyopathy and other forms of
left ventricular outflow tract obstruction Mental or physical
impairment leading to inability to exercise adequately High-degree
atrioventricular block
Slide 31
Contraindications to Exercise Unstable angina Resting ST
depression > 2mm Uncontrolled arrhythmias Critical aortic
stenosis Uncompensated congestive heart failure Resting SBP >
200mmHg or DBP >110mmHg Fall in SBP > 10mmHg with exercise
Symptomatic orthostatic SBP drop 10-20 mmHg
Slide 32
Comorbidities Impacting the Safety of Exercise
DiabetesHypoglycemia AnticoagulationProgressive bruise or INR >
5.0 Visual and Cognitive Impairment Need close supervision Wound
and Skin IntegritySacral pressure sores require pressure relief
Rheumatologic, Neurologic, Orthopedic, or Balance disorders Warrant
close attention
Slide 33
Cardiac Rehabilitation 1.Introduction of Cardiac Rehabilitation
2.Disease-Specific Effects on Physiologic Responses and Fitness
3.Scientific and Physiologic Rationale for Exercise Therapy in
Patients with Heart Disease 4.Morbidity, Mortality, and Safety of
Cardiac Rehabilitation 5.Exercise Prescription and Programming
Braddom Box 34-4 Adaptations noted with aerobic training
Functional Higher peak work rate Reduced disturbance of body
function Enhanced rate of recovery after exercise Cardiovascular
and pulmonary Increased stroke volume and peak CO Increased
respiratory muscle strength, maximal voluntary ventilation Reduced
dyspnea Musculoskeletal Increased flexibility Increased muscle,
tendon, and cartilage strength Increased bone density Increased
lean muscle mass Reduced body fat percentage Biochemical Increased
aerobic enzyme concentration Endocrine Reduced stress hormone
release Psychologic Improved depression and anxiety
Slide 36
Exercise Pattern Resistance Exercise Moderate-intensity dynamic
resistance exercise (defined as 50% 60% of one repetition maximum
[1RM]) results in improved muscle strength and endurance A small
reduction of 3 and 4 mm Hg for resting systolic blood pressure and
diastolic blood pressure, respectively A commonly recommended
resistance-training program involves performing one set of eight to
10 regional exercises, performed 2 to 3 days per week Isometric
exercises are not recommended because of a potential significant
rise in systolic and diastolic blood pressure
Slide 37
Exercise Pattern Resistance Exercise Time to Start Resistance
Exercise Catheterization with or without PCI 3 weeks later Recover
from an uncomplicated MI 5 weeks later CABG surgery or valve
surgery involving a sternotomy avoid upper-limb resistance training
until sternal healing has occurred), generally 6 to 12 weeks after
surgery
IllnessIntensityComments Coronary artery disease 40/50%-85% of
HRRTo affect mortality, frequency, duration, and intensity of
training should sum to yield a weekly energy expenditure .1,500
kcalwk -1.a,b Angina or equivalent 40/50%-85% of HRR with necessary
adjustment to keep upper HRR limit to no more than 10 beats below
ischemic threshold Consider a prophylactic nitroglycerin 15 min
before anticipated exertion if symptoms limit routine ADLs or
ability to exercise. Myocardial infarction 40/50%-85% of HRRAchieve
1,500-2,000 kcal of energy expenditure through physical activity
each week.a,b PTCA with or without stent 40/50%-85% of HRRAchieve
1,500-2,000 kcal of energy expenditure through physical activity
each week.a,b ACSM s Table 35-4 Summary of Unique Exercise
Prescription Issues among Patients with Cardiovascular Disease
Slide 40
IllnessIntensityComments CABG or valve surgery 40/50%-85% of
HRR Restrict upper-body movement until sternum is healed (6-12 wk).
Heart failure40/50%-70% of HRR If needed, initially guide exercise
intensity at 60% of HRR and adjust duration to three bouts of 10
min each, progressing to 30-40 min. Cardiac transplant RPE
11-14Restrict upper-body resistance exercises until sternum is
healed (6-12 wk). Pacemaker, ICD, biventricul ar, RCT 10% below
activation threshold Avoid activities that stretch the arms. After
8 wk, nonballistic activities may be resumed, and ballistic
activities may be resumed after 12 wk. ACSM s Table 35-4 Summary of
Unique Exercise Prescription Issues among Patients with
Cardiovascular Disease
Slide 41
Coronary Artery Disease Intensity 40/50%-85% of HRR To affect
mortality, frequency, duration, and intensity of training should
sum to yield a weekly energy expenditure 1500 kcal/ week Total
energy expenditure is more important than duration or type of
activity
Slide 42
Braddom Box 34-1 Risk Factors for Coronary Artery Disease
Modifiable Physical inactivity Hypertension Smoking Dyslipidemia
Overweight or obesity Diabetes Metabolic syndrome Non-modifiable
Increasing age Gender: male > female Prior history: cardiac,
peripheral vascular, or cerebrovascular disease Family history:
genetics Cultural or socioeconomic
Slide 43
ACSM s Table 35-3 Summary of Effects of Cardiorespiratory
Exercise Training on Selected Cardiovascular Risk Factors Risk
FactorEffect SmokingBy itself: little or no effect Exercise should
be part of a comprehensive smoking cessation program Lipid
abnormalities CholesterolLittle or no effect LDL cholesterolLittle
or no effect HDL cholesterolMild to moderate increase
HypertensionReduces incidence (especially among white men)
SystolicReduced: average, 6 mm Hg DiastolicReduced: average, 5 mm
Hg ObesityExercise alone: mild effect Exercise should be part of a
comprehensive weight- management program
Slide 44
Angina Exercise, lifestyle behavior changes, and medical
compliance 40/50%-85% of HRR Patients with evidence of
exercise-induced ischemia (i.e., angina, ECG changes), the upper HR
for exercise training should be set 10 or more beats below the HR
or RPP Goal for patients with angina To perform routine daily
activities at a lower RPP, thus reducing the amount of angina/
fatigue they experience To increase the amount of work, home
activity, or exercise they can perform at a given RPP
Slide 45
Angina Patients need to recognize and understand their symptoms
first Patients regularly experience angina at relatively low
workloads (e.g., 2 METs) to take one sublingual nitroglycerin about
15 minutes before starting their warm-up. Exercise in a pain-free
manner and at slightly higher workloads A longer warm-up (10 min)
to minimize or avoid ischemia
Slide 46
Myocardial Infarction Start at the lower end of their training
intensity (40% 60% of HR reserve method) Three nonconsecutive days
of cardiac rehabilitation per week, with each exercise session
consisting of a 5- to 10-minute warm-up and cool- down period
Progressively increase exercise intensity and duration up to 85% of
HR reserve method and 20 to 60 minutes Encouraged to adopt an
active life style, including exercise and daily activities, so that
they expend >1500 kcal each week
Slide 47
Revascularization (Coronary Artery Bypass Graft and
Percutaneous Coronary Intervention) Signs of ischemia during
exercise are often eliminated after revascularization Patients
undergoing PCI Recommendations for exercise programming for
patients after PCI are generally the same as for other patients
with CAD Because patients undergoing PCI frequently do not
experience myocardial damage or extensive surgery, they can
sometimes begin cardiac rehabilitation, return to work, and resume
ADLs much sooner Cardiac rehabilitation can begin within 48 hours
after PCI
Slide 48
Revascularization (Coronary Artery Bypass Graft and
Percutaneous Coronary Intervention) Patients undergoing CABG
surgery Begin rehabilitation as early as 2 weeks after surgery,
with the initial focus on aerobic-type exercises All upper-body
exercise should be limited to ROM and light repetitive activities
until 4 to 8 weeks after surgery Following the initial wound
healing, patients should be able to exercise up to 85% of HR
reserve method, 3 to 4 days per week, for 20 to 60 minutes After
the sternum is healed at 6 to 12 weeks, patients can then begin a
resistance-training program similar to other patients with
cardiovascular disease
Slide 49
Valve Dysfunction/Repair/Replacement Heart valve abnormalities
Increase the work the heart due to reducing effective cardiac
output Myocardial hypertrophy Mild diastolic dysfunction or a
decrease in ventricular distensibility Exercise will not improve or
change the function of the valves, but it will help to improve the
efficiency of oxygen extraction by the skeletal muscles and improve
the work capacity of the individual
Slide 50
Valve Dysfunction/Repair/Replacement The majority of valve
abnormalities can be corrected with surgical procedures. Patients
follow the same guidelines as CABG patients following surgery
Patients on warfarin for mechanical valves or atrial fibrillation
should avoid contact sports
Slide 51
Heart Failure Exercise intolerance Peak exercise capacity
reduced 30% to 40% in patients with heart failure Several
mechanisms to explain the exercise intolerance A reduction in peak
cardiac output (~40%) Chronotropic incompetence Reduced stroke
volume The ability to increase blood flow to the more metabolically
active skeletal muscles during exercise is attenuated Abnormalities
in the skeletal muscle, such as a reduction in myosin heavy chain I
isoforms, reduced activity of the enzymes associated aerobic
metabolism, and a reduction in fiber size
Slide 52
Heart Failure Moderate exercise is generally safe and results
in improvements in many aspects Exercise training increases
ejection fraction and decreases LV end-diastolic volume Patients
with decompensated heart failure should not be involved in an
exercise program More opportunity for rest, then progressively
increase to 30 minutes or more. The upper end of exercise intensity
at 60% of HR reserve method, based on patient's condition ECG
monitoring or not
Slide 53
Cardiac Transplant Cardiac transplant recipients continue to
experience exercise intolerance after transplantation This exercise
intolerance is believed to be primarily attributable to the absence
of efferent sympathetic innervation of the myocardium, affecting
heart rate and contractility responses, residual skeletal muscle
abnormalities developed before transplantation because of heart
failure, and decreased skeletal muscle strength
Slide 54
Cardiac Transplant After transplantation, many differences
Elevated resting HR (often >90 bpm) Elevated systolic and
diastolic BPs at rest Attenuated increase in HR during submaximal
work Lower peak HR and peak stroke volume Greater increase in
plasma norepinephrine during exercise Delayed slowing of HR in
recovery Elevated systolic and diastolic BPs at rest, partly
attributable to increased plasma norepinephrine and the
immunosuppressive medications (i.e., cyclosporine and prednisone)
Delayed HR in recovery is thought to be attributable to increased
levels of plasma norepinephrine, exerting its positive chronotropic
effect in the absence of vagal efferent innervation
Slide 55
Cardiac Transplant In the first year after surgery, it is best
to simply disregard all HR-based methods because of the abnormal HR
control in these patients Cardiac transplant patients undergo
exercise training Exercise capacity increases by about 15% to 40%
Resting HR is unchanged or decreases slightly Peak HR increases
Little change in peak stroke volume or cardiac dimensions Quality
of life is favorably altered A progressive resistance training
program started 6 to 12 weeks after transplant surgery and
performed twice per week
Slide 56
DeLisa Table 83-2 Borg Scales for Rating Perceived Exertion
15-Grade scale10-Grade Scale 6No exertion at all0Nothing 7Extremely
light 8 0.5Very, very light (just noticeable) 9Very light 10 1Very
light 11Light 12 2Light (weak) 13Somewhat hard 14 3Moderate 15Hard
(heavy)4 16 5Heavy (strong) 17Very hard6 18 7Very heavy 19Extremely
hard8 20Maximal exertion9 10Very, very heavy (maximal)
Slide 57
Pacemakers, Implantable Cardiac Defibrillators, and Arrhythmias
In general, the exercise training prescription is unaltered for
patients with these devices. Exercise intensity in patients with an
ICD should be set at least 10 beats below the programmed firing
threshold Avoid activities that stretch the arms. After 8 wk,
nonballistic activities may be resumed, and ballistic activities
may be resumed after 12 wk.
Slide 58
Summary The inclusion of exercise in the treatment of these
patients is beneficial because of its favorable effects on risk
factors, symptoms, functional capacity, physiology, and quality of
life. All patients with cardiovascular disease should be encouraged
to participate in exercise because of its real or likely positive
impact on mortality and morbidity.