




Languages
Pages
Legal

8/4/2019 MUSCULAT DYSTROPHY
1/28
MUSCULAR DYSTROPHY
DEFINITION
Muscular dystrophy is a group of disorders that involve progressive
muscle weakness and loss of muscle tissue.
Those classified as the muscular dystrophies all have in common a
progressive degeneration of striated muscle with no associated
abnormality of central nervous system.
CLASSIFICATION OF THE MUSCULAR DYSTROPHIES ACCORDING TO
PATTERN OF INHERITANCE.
1) X-LINKED RECESSIVE
Duchenne Muscular Dystrophy
Becker Muscular Dystrophy
Emery-Dreifuss Muscular Dystrophy
2) AUTOSOMAL RECESSIVE
Limb-Girdle Muscular Dystrophy
Congenital Muscular Dystrophy
3) AUTOSOMAL DOMINANT
Facioscapulohumeral Dystrophy
Myotonic Dystrophy
8/4/2019 MUSCULAT DYSTROPHY
2/28
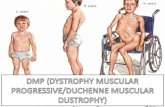
DUCHENNE MUSCULAR DYSTROPHY
Most common type and affects BOYS.
Caused by genetic problem that makes protein-DYSTROPHIN ( which
help cells keep their shape and length)
Symptom start usually by the age of 2-6 yrs old, and by the time 12 yrs
old, used a wheel chair.
Will develop scoliosis and tightness in joints
Over time, even muscles that control breathing get weaker, and patient
may need ventilator to breathe.
Lungs and heart specialist may need.
PATHOPHYSIOLOGY
The gene that codes for the protein dystrophin is mutated, so little or no
dystrophin is present in the sarcolemma.
The dystrophin gene is located on the short arm of chromosome X near
the p21 locus and codes for the large protein Dp427, which contains 3685
amino acids.
Dystrophin accounts for only approximately 0.002% of the proteins in
striated muscle, but it has obvious importance in the maintenance of themuscle's membrane integrity (Hoffman et al).
Dystrophin aggregates as a homotetramer at the costomeres in skeletal
muscles, as well as associates with actin at its N-terminus and the DAG
complex at the C-terminus, forming a stable complex that interacts with
laminin in the extracellular matrix (Hoffman et al). .
Lack of dystrophin leads to cellular instability at these links, with
progressive leakage of intracellular components; these results in the high
levels of creatine phosphokinase (CPK) noted on routine blood workup of
patients with Duchenne MD.
Without the reinforcing effects of the the dystrophin, the sarcolemma tears
easily during muscle contraction, causing muscle rupture and die.
8/4/2019 MUSCULAT DYSTROPHY
3/28
There is decrease in the muscle fibers, necrosis, infiltration of fat cells and
increase in connective tissues.
Muscles eventually reduced to fat and connective tissues.
(pseudohypertrophy).
CLINICAL FEATURES
Symptoms vary with the different types of MD.In Duchenne MD,
unless a sibling has been previously affected to warrant a high index of
suspicion, no abnormality is noted in the patient at birth, and
manifestations of the muscle weakness do not begin until the child begins
to walk. Three major time points for patients with Duchenne MD are
when they begin to walk, when they lose their ability to ambulate, and
when they die.
The child's motor milestones may be at the upper limits of
normal, or they may be slightly delayed. Some of the delays may be
caused by inherent muscle weakness, but a component may stem from
brain involvement. Although the association of intellectual impairment in
MD has long been recognized, it was initially thought to be a result of
limited educational opportunities (Prosser et al, 1969). In addition to mental deficits, another milestone delay is the
patient's age at ambulation. Children with Duchenne MD usually do not
begin to walk until about age 18 months or later. In the Dubowitz study
(1995), 74% of children with Duchenne MD manifested the disease by age
4 years. By age 5 years, awareness increases as the disease is
manifested in all affected children when they experience difficulty with
school-related activities (eg, getting to the bus, climbing stairs, reciprocal
motions during activities).
Other early features include a gait abnormality, which classically
is a waddling, wide-based gait with hyperlordosis of the lumbar spine and
toe walking. The waddle is due to weakness in the gluteus maximus and
gluteus medius muscles and the patient's inability to support a single-leg
8/4/2019 MUSCULAT DYSTROPHY
4/28
stance. The child leans the body toward the other side to balance his or
her center of gravity, and the motion is repeated with each step. Hip
extensor weakness also results in a forward tilt of the pelvis, which
translates to a hyperlordosis of the spine to maintain posture. The child
then walks on his or her tiptoes because it is easier to stay vertical with an
equinus foot position than on a flat foot, although no real tendon Achillis
contracture exists at this early point.
Gradually, noticeable difficulty with step taking by the child is
observed. Frequent falls without tripping or stumbling often occur and
are described as the feet being swept away from under the child. The child
then begins having problems getting up from the sitting or supine position,
and he or she can rise to an upright stance only by manifesting the Gower
sign.
Gowers sign.
While still ambulatory, the child may have minimal deformities, including
iliopsoas or tendo Achillis tightness. Mild scoliosis may be present if the
child has an asymmetrical stance. Upper-extremity involvement rarely
occurs in the beginning, although proximal arm muscle weakness may be
evident on manual strength testing. When upper-extremity involvement
manifests in later stages of Duchenne MD, it is symmetrical and, along
with distal weakness, usually follows a rapid worsening of the child's
condition toward being wheelchair bound.
8/4/2019 MUSCULAT DYSTROPHY
5/28
The second important phase in Duchenne MD is the loss of ambulation.
This usually occurs between the ages of 7 and 13 years, with some
patients becoming wheelchair bound by age 6 years. If children with MD
are still ambulating after age 13 years, the diagnosis of Duchenne MD
should be questioned, because these patients usually have Becker MD,
the milder form of MD.
Other clinical features include:
Muscles weakness that slowly gets worse
Frequent fall.
Delayed development of muscle motor skills
Problems walking (delayed walking)
Difficulty using one or more muscle groups
Hypertrophied of calf muscles
Mental retardation (only in some types of conditions)
Hypotonia (low muscle tone)
Joint Contractures (clubfoot, claw hand or others)
Scoliosis (curves spine)
COMPLICATIONS
Complications of MD usually include early wheelchair dependence in patients
who develop minor musculoskeletal injuries (eg, ankle sprain) and those who are
immobilized. Prolonged immobilization worsens the clinical weakness caused by
MD and ultimately results in the patient's non-ambulatory status.
MEDICAL MANAGEMENT
There are no known cures for the various muscular dystrophies. The goal
of treatment is to control symptoms.
Corticosteroids- taken by mouth are sometimes prescribed to children to
keep them walking for as long as possible and to reduce muscle
degeneration.
8/4/2019 MUSCULAT DYSTROPHY
6/28
Immunosuppressant- delay damage to dying muscle cell.
Antibiotic- fight respiratory infections
Orthopedic appliances such as braces and wheelchairs can improve
mobility and self-care abilities.The orthopedic problems in children with
MD are progressive weakness with loss of ambulatory status, soft-tissue
contractures, and spinal deformities. The role of the orthopedic surgeon is
to correct the deformities and to help maintain the dystrophic child's
ambulatory status for as long as possible, usually 1 to 3.5 years (Brooke
et al, 1989; Heckmatt et al, 1985). The modalities available to obtain these
goals have been well outlined by Drennan (1990); they include functional
testing; physical therapy; use of orthoses; fracture management; soft-
tissue, bone, and spinal surgeries; use of a wheelchair when indicated;
and genetic and/or psychological testing.
Surgery on the spine or legs may help improve function.
Despite modern advances in gene therapy and molecular biology, MD remains
incurable. With proper care and attention, patients have a better quality of life
than they would otherwise, but most still die by the time they are age 30 years,
usually as a result of cardiopulmonary failure.
8/4/2019 MUSCULAT DYSTROPHY
7/28
CASE STUDY ASESSMENT
PATIENTS PROFILE
Date of assessment: 12. September. 2007
Unit: Pediatric Gym of Physiotherapy Department, Hospital Malacca.
Name: Kid
Age: 9 yrs
Gender: Male
Race: Chinese
Hometown: Bukit Baru, Melaka
R/N: 5590
Drs Diagnosis: Duchene Muscular Dystrophy
Drs Management: Medication
Problem: Weakness of both lower limbs
8/4/2019 MUSCULAT DYSTROPHY
8/28
SUBJECTIVES ASESSMENT
1) Patients complain:
Mother complains that her child had weakness at both lower limb.
Her child easily fatigue and had difficulty to stand from sitting, to sit from
supine lying and difficulty of climbing stairs.
2) Current Hx:
Mother claimed that her child had frequently fall and unable to rise back
easily since two years ago.
Had being diagnosed as Duchene Muscular Dystrophy and being referred
to physiotherapy treatment.
3) Past Medical Hx:
-nil-
4) Pain Scale: No pain at the limbs and joints.
4) Home/ social situation:
Youngest in family of 3 siblings.
Loves to play, R.C car, badminton, cycling, and comp. games.
A vegetarian and usually take bowl of rice daily and 2-3 liters of
water/day.
At school, able to socialized but doesnt involved in any physical activity.
Using night splint while sleeping at night.
5) General Health:
-Good-
8/4/2019 MUSCULAT DYSTROPHY
9/28
6) Ix/MRI/X-Ray:
Latest on March 2007- unavailable
7) Medication:
Use alternative medicine- Chinese herbs purposely for legs and waist.
OBJECTIVES ASESSMENT
1) Observation
General:
A thin and medium size of 9 yrs Chinese boy walks into gym with
abnormal gait and hyperextended trunk.
Moody and give cooperation after being persuaded for several times.
Local:
Genu-valgus leg
Muscle wasting of both LL. Hypertrophied calf muscles.
2) Vocalization:
Speak Mandarin fluently BUT little bit Malay.
Understand Malay and English minimally.
3) Hearing:
NAD
4) Vision:
NAD
8/4/2019 MUSCULAT DYSTROPHY
10/28
5) Palpation:
TA tightness of both ankle.
No contractures of the joints.
No swelling of the joints and body.
No redness at the joints and body.
6) Range of Motion:
Joint Active
Shoulder
1) Flexion
2) Extension
3) Abduction
4) Adduction
5) Elevation via
flexion
6) Elevation via
abduction
Elbow
Flexion
Extension
Supination
Pronation
Wrist
Flexion
Extension
Ulnar dev.
Rt
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
8/4/2019 MUSCULAT DYSTROPHY
11/28
Radialdev. AFROM AFROM
Joint Active
Phalanges
Flexion
Extension
Abduction
Adduction
Thumb
opposition
Hip
Flexion
Extension
Abduction
Adduction Int.rotate
Ext.rotate
Knee
Flexion
Rt
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
AFROM
8/4/2019 MUSCULAT DYSTROPHY
12/28
Extension AFROM AFROM
Joint Active Passive
Ankle
Dorsiflexion
Plantar-flexion
Eversion
Inversion
Rt
0-5
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
Rt
0-15
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
Interpretation: Limited R.O.M of ankle dorsiflexion due to TA tightness.
8/4/2019 MUSCULAT DYSTROPHY
13/28
7) Muscle tone:
Both upper limbs: Normal
Both lower limb: Normal
8) Muscle power (Oxford Scale Classification)
Upper limb Grade
a) Shoulder
Flexors
Extensors
Abductors
Adductors
b) Elbow
Flexors
Extensors
Supinators
Pronator
3/5
3/5
3/5
3/5
3/5
3/5
3/5
3/5
c) Wrist
Flexors
Extensors
Radial deviators
Ulnar deviators
d) Fingers
Flexors
Extensors
Abductors
Adductors
3/5
3/5
3/5
3/5
3/5
3/5
3/5
3/5
Lower limb Grade
8/4/2019 MUSCULAT DYSTROPHY
14/28
a) Hip
Flexors
Extensors
Abductors
Adductors
Int. rotators
Ext. rotators
b) Knee
Flexors
Extensors
Ankle
Dorsi flexors
Plantar flexors
Inverters
Everters
3/5
3/5
3/5
3/5
3/5
3/5
3/5
3/5
3/5
3/5
3/5
3/5
Interpretation: Reduce muscle power due to myopathic disorder.9) Reflexes
Interpretation: A low normal, diminished reflex and negative Babinski sign.
Tendons Grade
1) Biceps 1+
2) Triceps 1+
3) Knee jerk 1+
4) Tendon Achilles 1+
5) Babinski -ve
8/4/2019 MUSCULAT DYSTROPHY
15/28
10. Posture
Lumbar lordosis with shoulder and upper trunk thrust backward, with
lateral sway back of the trunk.
11) Gait
Type: high stepping/ waddling gait
a) Stance phase:
Increase in anterior pelvic tilt
Reduce in hip extension
b) Swing phase:
Increase in hip flexion characterized by high stepping gait/waddling gait.
Lack of dorsiflexion
12) Functional Ability
Test for functional ability based on ability to walk.
Grade Functional ability
1 Walks and climbs stairs without assistance
2 Walks and climbs stairs with aid of a railing
3 Walks and climbs stairs slowly with the aid of a railing (over
25 sec for eight standard steps)
4 Walks unassisted rise from chair but cannot climb stairs.
8/4/2019 MUSCULAT DYSTROPHY
16/28
5 Walks unassisted but cannot rise from chair and stairs.
6 Walks only with assistance or walks independently with long
leg braces.
7 Walks in long leg braces but requires assistance for balance.
8 Stands in long leg braces but unable to walk even with
assistance.
9 Is in wheelchair. Elbow flexors more than antigravity.
10 Is in wheelchair. Elbow flexors less than antigravity.
Also has difficulty to stand from squatting (Gowers sign)
Interpretation: Grade 4
13. Balance Testing
Position Static Dynamic
a) Sitting Good Good
b) Standing Fair Fair
c) Walk standing Fair Fair
Interpretation: Reduce stability in standing and walk standing due to muscle
weakness.
8/4/2019 MUSCULAT DYSTROPHY
17/28
PROBLEM LISTING
1. Reduce muscle strength of both lower limbs.
2. Lordotic posture while walking and standing.
3. Tightness of Tendon Archilles.
4. Difficulty of climb stairs and stand from squatting.
5. Waddling gait.
PHYSIOTHERAPIST IMPRESSION
4. Reduce muscle strength of both lower limbs due to myopathic disorder.
5. Lordotic posture while walking and standing due to relative postural
alignment of the upper body.
6. Tightness of Tendon Archilles due to weakness of ankle dorsiflexors.
4. Difficulty of climb stairs and stand from squatting due to weakness of
extensor muscles, particularly gluteus maximus.
5. Waddling gait due to weakness of quadriceps, hip extensors and ankle
dorsiflexors.
AIM OF TREATMENT
Short term goal:
1. To reduce muscle tightness.
2. To prevent deformity and soft tissue contracture.
3. To prevent immobility and inactivity, both mental and physical.
Long term goal:
1. To ensure the child practice a healthy life- style.
2. To prevent secondary complication.
PLAN OF TREATMENT
1. Breathing exercise
2. Stretching exercise
8/4/2019 MUSCULAT DYSTROPHY
18/28
3. Mobilizing exercise
4. Home exercise program (HEP) and patient education.
METHOD OF TREATMENT
1) Breathing exercise
Position: sitting/standing
Method: Deep breathing exercise with 6
repetition 3x/day.
2. Stretching exercise
Active stretching:
Child standing with pelvis forwards, arms on the wall, heels remain on the
ground with knee fully extended, hold for 10sec.
Modified push-up done over a wedge or double-pillow with 10 rep, 10 sec
hold.
Passive stretching:
Stretching of calf muscles while pt in supine,10rep, 10 sec hold.
Stretching of iliotibial band, pt in prone and knee is flexed and hip fully
extended. Pressure given to the pelvis to minimize the lumbar spine
movement. Repeat for 10 times, with 10 sec hold.
Stretching of hamstring, pt in supine. Knee extended, hip flexed to 60.
Repeat for 10 times, with 10 sec hold.
3) Mobilizing exercise
Throwing and kicking gym ball for 15 minutes.
Pulley exercise for 15minutes.
Cyling on stationary bicycle for 15 minutes.
8/4/2019 MUSCULAT DYSTROPHY
19/28
4) Home exercise program
Breathing exercise with 6 rep/3x/day.
Encouraged the child to play a wind instrument, play games such as
blowing a ping pong ball around obstacles to obtain good expansion of the
lungs.
Stretching exercise done actively of passively at home to prevent soft
tissue contracture
5) Carer Education
Advice mother to make sure her child do the exercise as taught at
home regularly.
Encourage the child not to give up while doing the exercises.
REASESSMENT ON 14. SEPT. 07
S:
Mother claimed that her child do slight exercise at home.
Complain of fatigue.
O:
Pt gives good response
Walk with waddling gait, lumbar lordosis with shoulder and upper
trunk thrust backward, with lateral sway back of the trunk.
1) R.O.M:
8/4/2019 MUSCULAT DYSTROPHY
20/28
Both UL, hip, and knee: AFROM
Interpretation: limited R.O.M of ankle d/f due to TA tightness.
2) Muscle tone:
Both UL: Normal
Both LL: Normal
3) Muscle power ( Oxford Scale Classificaton) Both UL: 3/5
Both LL: 3/5
4)Posture
Lumbar lordosis with shoulder and upper trunk thrust backward, with
lateral sway back of the trunk.
6) Gait
Type: high stepping/ waddling gait
a) Stance phase:
Increase in anterior pelvic tilt
Reduce in hip extension
Joint Active Passive
Ankle
Dorsiflexion
Plantar-flexion
Eversion
Inversion
Rt
0-5
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
Rt
0-15
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
8/4/2019 MUSCULAT DYSTROPHY
21/28
b) Swing phase:
Increase in hip flexion characterized by high stepping gait/waddling gait.
Lack of dorsiflexion
7) Functional Ability
Test for functional ability based on ability to walk
Grade Functional ability
1 Walks and climbs stairs without assistance
2 Walks and climbs stairs with aid of a railing
3 Walks and climbs stairs slowly with the aid of a railing (over
25 sec for eight standard steps)
4 Walks unassisted rise from chair but cannot climb stairs.
5 Walks unassisted but cannot rise from chair and stairs.
6 Walks only with assistance or walks independently with long
leg braces.
7 Walks in long leg braces but requires assistance for balance.
8 Stands in long leg braces but unable to walk even with
assistance.
9 Is in wheelchair. Elbow flexors more than antigravity.
10 Is in wheelchair. Elbow flexors less than antigravity.
Interpretation: Grade 4
Still has difficulty to stand from squatting (Gowers sign)
8/4/2019 MUSCULAT DYSTROPHY
22/28
9) Reflexes
Interpretation: A low normal, diminished reflex and negative Babinski sign.
A:
Reducemuscle power
and poor
mobility might
due to
muscular
disorder.
P:
1) Breathing exercise
Position: sitting/standing
Method: Deep breathing exercise with 6 repetition.
Tendons Grade
1) Biceps 1+
2) Triceps 1+
3) Knee jerk 1+
4) Tendon Achilles 1+
5) Babinski -ve
8/4/2019 MUSCULAT DYSTROPHY
23/28
2) Passive stretching:
a) Stretching ofcalf muscles while pt in supine,10rep, 10 sec hold.
b) Stretching ofiliotibial band, pt in prone and knee is flexed and hip fully
extended. Pressure given to the pelvis to minimize the lumbar spine movement.
Repeat for 10 times, with 10 sec hold.
c) Stretching ofhamstring, pt in supine. Knee extended, hip flexed to 60.
Repeat for 10 times, with 10 sec hold.
2) Mobilizing exercise
Throwing and kicking gym ball for 15 minutes.
Pulley exercise for 15minutes.
3) Home exercise program
Breathing exercise with 6 rep/3x/day.
Active and passive stretching exercise with 10 rep/3x/day.
Mobilizing exercise, walking at the park for 15 minutes.
4) Patient education Advice patient to do the exercise as taught regularly and encourage
the child to continue the exercises at home.
REASESSMENT ON 18.SEPT. 07
S:
Mother claimed that her child willing to do some exercises at home.
Complain of fatigue after doing the exercise.
O:
Pt gives good response.
8/4/2019 MUSCULAT DYSTROPHY
24/28
Still walk with waddling gait, lumbar lordosis with shoulder and
upper trunk thrust backward, with lateral sway back of the trunk.
1) R.O.M:
Both UL, hip, and knee: AFROM
Interpretation: limited R.O.M of ankle d/f due to TA tightness.
2) Muscle tone:
Both UL: Normal Both LL: Normal
3) Muscle power (Oxford Scale Classificaton)
Both UL: 3/5
Both LL: 3/5
4) Posture
Lumbar lordosis with shoulder and upper trunk thrust backward, with
lateral sway back of the trunk.
6) Gait
Joint Active Passive
Ankle
Dorsiflexion
Plantar-flexion
Eversion
Inversion
Rt
0-7
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
Rt
0-15
AFROM
AFROM
AFROM
Lt
AFROM
AFROM
AFROM
AFROM
8/4/2019 MUSCULAT DYSTROPHY
25/28
Type: high stepping/ waddling gait.
a) Stance phase:
Increase in anterior pelvic tilt.
Reduce in hip extension.
b) Swing phase:
Increase in hip flexion characterized by high stepping gait/waddling gait.
Lack of dorsiflexion
7) Functional Ability
Test for functional ability based on ability to walk
Grade Functional ability
1 Walks and climbs stairs without assistance
2 Walks and climbs stairs with aid of a railing
3 Walks and climbs stairs slowly with the aid of a railing (over
25 sec for eight standard steps)
4 Walks unassisted rise from chair but cannot climb stairs.
5 Walks unassisted but cannot rise from chair and stairs.
6 Walks only with assistance or walks independently with long
leg braces.
7 Walks in long leg braces but requires assistance for balance.
8 Stands in long leg braces but unable to walk even with
assistance.
9 Is in wheelchair. Elbow flexors more than antigravity.
10 Is in wheelchair. Elbow flexors less than antigravity.
8/4/2019 MUSCULAT DYSTROPHY
26/28
Interpretation: Grade 4
Still has difficulty to stand from squatting (Gowers sign)
9) Reflexes
Interpretation: A low normal, diminished reflex and negative Babinski sign due to
myopathic
disorder.
A:
Reduce muscle power and poor mobility might due to muscular disorder.
Able to do the active stretching exercise better.
P:
1) Breathing exercise with thoracic expansion
Position: Standing
Method: Deep breathing exercise with elevation of both arm, 6 repetition.
Tendons Grade
1) Biceps 1+
2) Triceps 1+
3) Knee jerk 1+
4) Tendon Achilles 1+
5) Babinski -ve
8/4/2019 MUSCULAT DYSTROPHY
27/28
2) Passive stretching:
a) Stretching ofcalf muscles while pt in supine,10rep, 10 sec hold.
b) Stretching ofiliotibial band, pt in prone and knee is flexed and hip fully
extended. Pressure given to the pelvis to minimize the lumbar spine movement.
Repeat for 10 times, with 10 sec hold.
c) Stretching ofhamstring, pt in supine. Knee extended, hip flexed to 60.
Repeat for 10 times, with 10 sec hold.
2) Mobilizing exercise
Throwing and kicking gym ball for 15 minutes.
Pulley exercise for 15minutes.
3) Home exercise program
Breathing exercise with 6 rep/3x/day.
Active and passive stretching exercise with 10 rep/3x/day.
Mobilizing exercise, walking at the park for 15 minutes.
4) Patient education
Advice patient to do the exercise as taught regularly and encourage
the child to continue the exercises at home.
LITERATURE REVIEW
8/4/2019 MUSCULAT DYSTROPHY
28/28
Top Related