







Languages
Pages
Legal


FAQIH RUHYANUDIN

TERMASUK:TERMASUK:1. SUHU TUBUH2. NADI3. PERNAFASAN4. TEKANAN DARAH5. (NYERI : sering
disebut tanda-tanda vital yang ke-5)
Status fisiologis fungsi tubuh seseorang dapat direfleksikan oleh indikator TTV perubahan TTV indikasikan perub. kesehatan

Vital signVital sign NormalNormal vital vital
signs signs berubah berubah dipengaruhi oleh dipengaruhi oleh : umur,: umur, sex, sex, berat badanberat badan, , AktivitasAktivitas, , dan dan kondisi kondisi (sehat/sakit)(sehat/sakit)

Pengukuran TTV Sesuai permintaan, untuk melengkapi data
dasar pengkajian Sesuai permintaan dokter Sekali sehari klien stabil Setiap 4 jam 1 /> TTV abnormal Setiap 5 – 15mnt klien tidak stabil atau
resiko perubahan fisiologi secara cepat post op
Ketika kondisi klien tampakberubah
Setiap menit atau lebih sering, bila ada perubahan signifikan dari hasil pengukuran sebelumnya
Ketika klien merasa tidak seperti biasa Sebelum,selama dan setelah transfusi Sebelum pemberian obat efek
perubahan TTV

SUHU TUBUH SUHU TUBUH MENUNJUKKAN
KEHANGATANTUBUH MANUSIA Panas tubuh Diproduksi :
exercise dan metabolisme makanan
Hilang : melalui kulit, paru, dan produk sisa melalui proses radiasi, konduksi,konveksi, evaporasi

Suhu tubuh mencerminkan keseimbangan antara produksi panas dan kehilangan panas, dan diukur dalam unit panas yang disebut derajat.
Ada 2 macam suhu tubuh:1. Suhu inti jaringan dalam tubuh: rongga
abdomen dan rongga pelvic Relatif konstan
2. Suhu permukaan suhu kulit, SC, dan lemak SC naik dan turun merespon thd lingkungan

FAKTOR-FAKTOR YANG MEMPENGARUHI PRODUKSI PANAS1. BMR : jumlah energi yang digunakan
ubuh untuk melakukan aktivitas utama seperti bernafas
2. AKTIVITAS OTOT: termasuk menggigil, meingkatkan metabolisme rate
3. TYROXINE OUTPUT: meningkatnya output tyroxine akan meningkatkan metabolisme sel seluruh tubuh

4. Stimulasi/respon Epineprin, norephinephrine, simpatis. Hormon ini dengan seketika meningkatkan metbolisme sel dibeberapa jaringan tubuh
5. Fever, meningkatkan jumlah metabolisme tubuh
MEKANISME KEHILANGAN PANASRadiasi adalah pemindahan panas dari
permukaan objek tertentu ke permukaan onjek yang lain tanpa adanya kontak antara kedua objek, yang paling sering adalah dengan sinar inframerah. (atau penyebaran panas dengan gelombang elektromagnetik)
Konduksi adalah perpindahan panas ke objek lain melalui kontak langsung
Evaporasi (penguapan) adalah perubahan dari cairan menjadi uap. Seperti cairan tubuh dalam bentuk keringat menguap dari kulit
Konveksi adalah penyebaran panas oleh karena pergerakan udara dengan kepadatan yang tidak sama. orang yang menggunakan kipas angin
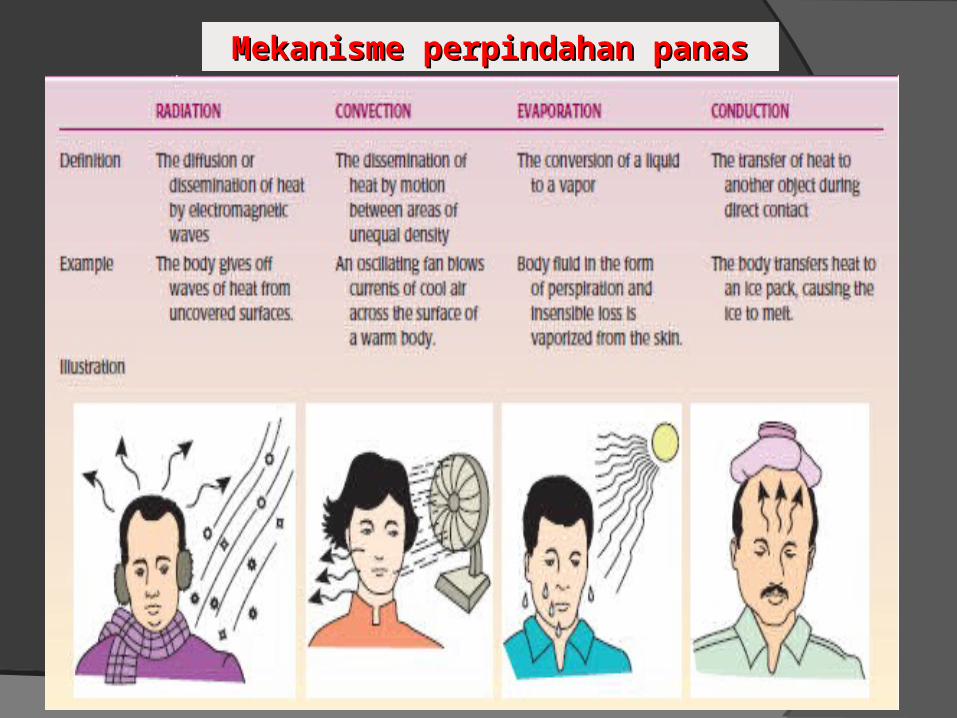
Mekanisme perpindahan panasMekanisme perpindahan panas
FAKTOR YANG MEMPENGARUHI SUHU TUBUHCircadian Rhythms perubahan fisiologis, seperti
perubahan suhu dan TTV yang lain secara fluktuatif : pagi hari lebih rendah dibandingkan sore hari, suhu tubuh berfluktuasi 0,28o – 1,1oC selama periode 24jam
Usia suhu tuuh bayi dan anak-anak berubah lebih cepat dalam merespon perubahan panas dan dingin

Hormonal perempuan cenderung lebih fluktuatif dibandingkan dengan laki-laki, karena perubahan hormon
Stress respon tubuh terhadap stress fisik dan emosi akan meningkatkan produksi epineprin dan nor epineprin sehingga mengakibatkan peningkatan metabolisme rate peningkatan suhu tubuh
SUHU TUBUH NORMAL Suhu Permukaan : 36,8o – 37,4o C (96,6o – 99,3o
F) Suhu inti : 36,4o – 38o C (97,5o – 100,4o F)
Suhu diukur dengan termometer.
Termometer yang paling dikenal Celsius (C), Reaumur (rankine) (R), Fahrenheit (F), Kelvin (K), dengan perbandingan antara satu dan lainnya mengikuti:
C:R:(F-32) = 5:4:9
Contoh: oC=5/9(F-32) dan F=9/4R+32

PENGATURAN SUHU PENGATURAN SUHU Suhu manusia dikendalikan
oleh HIPOTHALAMUS
Anterior hilangnya panas
Vasodilatasi dan bengkak
Posterior produksi dan menyimpan panas
1. Menyesuaikan dengan sirkulasi darah
2. Piloerectile (mengatur konstriksi atau dilatasi pori-pori kulit)
3. Respon menggigil

Hipotalamus meningatkan produksi panas dengan cara meningkatkan metabolisme melalui sekresi hormon thyroid, yaitu epinephrin dan norepinephrin medulla adrenalis
Dalam keadaan normal, hipotalamus menjaga suhu inti “set point”(suhu tubuh optimal) sebesar 1˚C oleh perubahan suhu permukaan tubuh dan darah
Suhu > 41°C, dan < 34°C indikasi kerusakan di pusat pengaturan hipotalamus

Pengaturan Suhu Tubuh Pengaturan Suhu Tubuh oleh HIPOTALAMUSoleh HIPOTALAMUS

PENGUKURAN SUHUPENGUKURAN SUHU
1. ORAL
Termometer diletakkan di dibawah lidah sublingual artery
- biasanya hasil pengukuran 0,5 – 0,8 °C dibawah suhu inti
KONTRA INDIKASI PENGUKURAN SUHU DI ORAL:1. Klien tidak kooperatif
2. Bayi atau toodler
3. Tidak sadar
4. Dalam keadaan menggigil
5. orang yang biasa bernafas dengan mulut
6. Pembedahan pada mulut
7. Pasien tidak bisa menutup mulut

Untuk menjamin keakuratan hasil pengukuran perlu dikaji:Pengukuran dilakukan 30 menit setelah klien :
1. Mengunyah permen/permen karet
2. Merokok
3. Makan dan minum panas atau dingin

2. Rektal2. Rektal
Berbeda 0,1°C dengan suhu inti
KontraindikasiKontraindikasi Diare Pembedahan rektal Clotting disorders Hemorrhoids

3. Aksila 3. Aksila
Hasil pengukuran 0,6°C lebih rendah dibandingkan suhu oral
Paling sering dilakukan mudah, nyaman
Contraindication of axillary temperatureContraindication of axillary temperature Pasien kurus Inflamasi Lokal daerah aksila Tidak sadar, shock Konstriksi pembuluh darah perifer

TEMPAT PENGUKURAN
CELCIUS
Oral 37°
Rektal (setara) 37,5°
Aksila (setara) 36,4 °
Ekuivalen Pengukuran suhuEkuivalen Pengukuran suhu

4. Telinga (Aural)4. Telinga (Aural) Riset menunjukkan suhu ditelinga pada
membran timpani paling mendekati suhu inti tubuh
Kesimpulan ini diddasarkan pada 2 fakta anatomi:1. Membran tympani hanya berjarak 3,8 cm dari
hipotalamus
2. Darah pada arteri karotis internadan eksterna, adalah pembuluh darah yang menyuplai hipotalamus dan membran tympani

Tympanic Thermometer

PENINGKATAN SUHU PENINGKATAN SUHU TUBUHTUBUH1. Pyrexia : istilah yang digunakan untuk
menggambarkan suhu tubuhlebih tinggi dari set point normal
2. Fever (demam) : suhu tubuh > 37,4°C, tanda dan gejala:
- Kulit kemerahan- Gelisah, - irratibilitas (lekas marah)- Tidak nafsu makan- Pandangan menurun dan sensitif terhadap cahaya
Banyak KeringatSakit kepalaNadi dan RR meningkatDisorientasi dan bingung (jika suhu terlalu
tinggi)Kejang pada infantdan anak-anak
3. Hiperthermi : suhu tubuh > 40,6°Csangat beriko terjadi kerusakan otak bahkan kematian kerusakan pusat pernafasan

TAHAPAN DEMAM (FEVER)1. Prodromal phase : gejala tidakspesifik
sebelumpeningkatan suhu
2. Onset or invasion phase (fase serangan)
peningkatan suhu tubuh, menggigil
3. Stationary phase : demam menetap
4. Resolution phase : suhu kembali normal

Nursing Interventions for Client's with fever:• Monitor vital signs• Assess skin color and temperature• Monitor WBC, HCT, and other laboratory reports for
indications of infection or dehydration• Remove excess blanket when the client feels warm,
but provide extra warmth when the client feels chilled.
• Measure intake and output• Provide adequate nutrition and fluid• Reduce physical activity to limit heat production.

Administer antipyretic Provide oral hygiene to keep the mucous
membrane moist. Provide a tepid sponge bath to increase heat loss
through conduction. Provide dry clothing and bed linens.
Hypothermia; is a core body temperature below the lower limit of normal. The three physiologic mechanisms of hypothermia are:
Excessive heat loss Inadequate heat production to counteract heat
loss Impaired hypothalamic thermoregulation

The clinical signs of hypothermia:Decreased body temperature, pulse, and
respirationSevere shiveringFeelings of cold and chillsPale, cool skinHypotensionDecreased urinary outputLack of muscle coordinationDisorientationDrowsiness progressing to comaFrostbite(nose, fingers, toes)
Nursing Interventions for Client's with Nursing Interventions for Client's with HypothermiaHypothermia1. Provide a warm environment
2. Provide dry clothing
3. Apply warm blanket
4. Keep limbs close to body
5. Cover the client's scalp with a cap
6. Supply warm oral or intravenous fluids
7. Apply warming pads

DIAGNOSA KEPERAWATAN DIAGNOSA KEPERAWATAN BERHUBUNGAN DENGAN SUHU BERHUBUNGAN DENGAN SUHU TUBUHTUBUH
1. Resiko Trauma
2. Hyperthermia
3. Hypothermia
4. Resiko ketidakseimbangan suhu tubuh
5. Ineffektif termoregulasi

PROSEDUR PEMERIKSAAN SUHU1. Pastikan frekuensi dan cara pemeriksaan
suhu sesuai dengan permintaan dokter atau rencana keperawatan (nursing care plan)
2. Identifikasi pasien3. Jelaskan prosedur pemeriksaan kepada
pasien4. Pastikan termometer dalam keadaan siap
pakai5. Cuci tangan dan gunakan sarung tangan bila
ada indikasi6. Pilih letak pemasangan termometer

7. Ikuti tahap-tahap pengukuran sesuai pedoman secara berurutan menyesuaikan dengan jenis termometer
8. Cuci tangan
9. catat hasil pengukuran

PEMERIKSAAN NADIPEMERIKSAAN NADI
Nadi Nadi adalah sensasi denyutan seperti gelombang yang dapat dirasakan/ dipalpasi di arteri perifer, terjadi karena gerakan atau aliran darah ketika konstraksi jantung

Nadi adalah gelombang darah yang dibuat oleh kontraksi ventrikel kiri jantung
Pada orang dewasa kontraksi jantung 60 – 100 x/mnt saat istirahat
Cardiac output; adalah volume darah yang dipompakan kedalam arteri oleh jantung dan = SVxHR
Nadi Perifer; nadi yang berada jauh dari jantung, ex: kaki, radialis, leher
Nadi apical; nadi central, lokasinya di apex jantung

KECEPATAN NADI (PULSE RATE) Pulse Rate (jumlah denyutan perifer
yang dirasakan selama 1 menit) dihitung dengan menekan arteri perifer dengan menggunakan ujung jari
Tachycardia: nadi >100 -150 x/mnt jantung overwork oksigenasi sel tidak adequat
Palpitasi Palpitasi : perasaan berdebar-debar, sering menyertai tachycardi
Denyut Nadi sangat fluktuatif dan meningkat dengan :1.exercise, 2.illness, 3.injury, and 4.emotions. wanita cenderung dibandingkan laki-laki. Athlets, mis. Pelari, bisa jadi heart rates-nya 40 x/mnt dan tidak masalah.

Bradycardia : denyut nadi < 60 x/mnt kejadian lebih sedikit dibandingkan tachycardia

FACTOR YANG FACTOR YANG MEMPENGARUHI NADIMEMPENGARUHI NADI
1. Usia; peningkatan usia, nadi berangsur-angsur menurun
2. Jenis Kelamin; pria sedikit lebih rendah daripada wanita (P=60-65 x/mnt ketika istirahat, W=7-8 x/mnt lebih cepat)
3. Circadian rhythm; rata-rata menurun pada pagi hari dan meningkat pada siamg dan sore hari

4. Bentuk tubuh; tinggi, langsing biasanya denyut jantung lebih pelan dan nadi lebih sedikit dibandingkan orang gemuk
5. Aktivitas dan exercise; nadi akan meningkat dengan aktivitas dan exercise dan menurun dengan istirahat
6. Stress dan emosi; rangsangan syaraf simpatis dan emosi seperti cemas, takut, gembira meningkatkan denyut jantung dan nadi.
Nyeri, adalah stressor yang dapat memacu nadi lebih cepat

7. Suhu Tubuh; setiap peningkatan 1°F nadi meningkat 10x/mnt, peningkatan 1°C nadi meningkat 15x/mnt. Sebaliknya bila terjadi penurunan suhu tubuh maka nadi akan menurun
8. Volume darah; kehilanngan darah yang berlebihan akan menyebabkan peningkatan nadi
9. obat-obatan; beberapa obat dapat menurunkan atau meningkatkan kontraksi jantung. Golongan digitalisdan sedatifmenurunkan HR, Caffeine, nicotine,cocaine, hormon tyroid, adrenalin meningkatkan HR

Penghitungan Nadi Penghitungan Nadi NormalNormal
USIA RENTANG NORMAL
RATA-RATA
BBL 120 – 160 140
1 – 12 BL 80 – 140 120
1 – 2 TH 80 – 130 110
3 – 6 TH 75 – 120 100
7 – 12 TH 75 – 110 95
REMAJA 60 – 100 80
DEWASA 60 – 100 80

IRAMA NADI
1. REGULER; pola dan jarak waktu denyutan pada tiap denyutan teraba sama/teratur NORMAL
2. IRREGULER (arrhythmia/dysrhythmia); pola dan jarak waktu denyutan pada tiap denyutan teraba tidak sama/tidak teratur

ISI DENYUTANISI DENYUTANAdalah kualitas denyutan yang teraba yang
berhubungan dengan julah darah yang dipompakan oleh jantung ketika berkontraksi
Kualitas definisi Deskripsi0 Tidak ada nadi Tidak teraba, meskipun ditekan dengan
kuat
1+ Nadi sangat lemah (thready Pulse)
Pulsasi susah dirasakan, dengan tekanan ringan tidak teraba
2+ Nadi lemah Denyutan Lebih kuat dibanding Thready
3+ Normal Dapt teraba dengan mudah,dengan palpasi ringan denyutan tidak teraba
4+ Denyutan kuat dan teraba dengan palpasi sedang

PENGUKURAN NADIPENGUKURAN NADI1. Temporal; passes over the
temporal bone of the head. The site is superior and lateral to the eye.
2. Carotid; at the side of the neck between the trachea and the sternocleiodomastoid muscle.
3. Apical; at the apex of the hearty. About 8cm to the left of the sternum and at the fourth and sixth intercostals space.
4. Brachial; at the inner aspect of the biceps muscle of the arm

5. Radial; on the thumb side of the inner aspect of the wrist
6. Femoral; alongside the inguinal ligaments
7. Popliteal; behind the knee
8. Posterior tibial; on the medial surface of the ankle
9. Pedal “dorsalis pedis”; over the bones of the feet



Adalah jumlah frekuensi pernafan seseorang selama satu menit
Frekuensi pernafasan dihitung setiap satu gerakan inhalasi dan ekshalasi

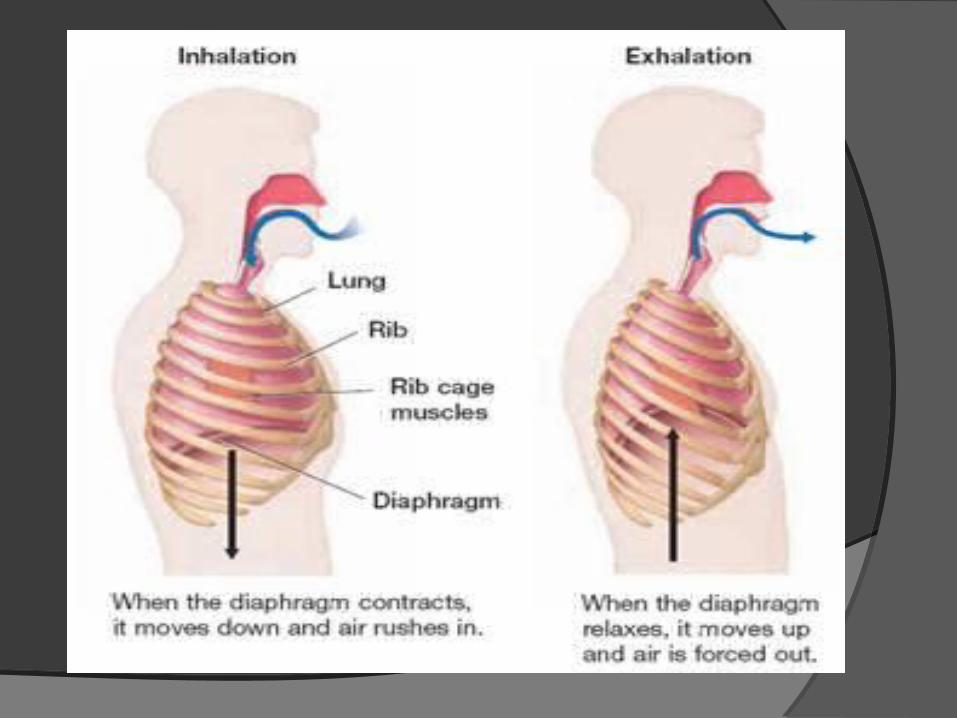
Mechanics and regulation of breathing
During inhalation, the diaphragm contracts the ribs move upward and outward, and the sternum moves outward, thus enlarging the thorax and permitting the lungs to expand.
During exhalation. The diaphragm relaxes, the ribs move downward and inward, and the sternum moves inward, thus decreasing the size of the thorax as the lungs are compressed.

Respiration is controlled by (a) respiratory centers in the medulla oblongata and the pons of the brain and (b) by chemo receptors located centrally in the medulla and peripherally in the carotid and aortic bodies.
External respiration; the interchange of oxygen and carbon dioxide between the alveoli of the lungs and the pulmonary blood. Internal respiration; the interchange of these same gases between the circulating blood and the cells of the body tissues.

The respiratory rate is normally described in breaths per minute, normal in depth and rate called eupnea. Bradypnea; abnormally slow respirations. Tachypnea; abnormally fast respirations. Apnea; the absence of breathing.

Abnormal Respiratory Rate
Respiration rates over 25 or under 12 breaths per minute (when at rest) may be considered abnormal
under 12 breathsunder 12 breaths
over 25 breathsover 25 breaths
Respiratory Rate
Normal respiration rates at rest range from 15 to 20 breaths per minute. In the cardio-pulmonary illness, it can be a very reliable marker of disease activity.
1515
2020

Factors affecting Respirations
Factors increase the rate:○Exercise○ Increase metabolism○Stress○ Increased environmental temperature○Lowered oxygen concentration
Factors decrease respiration rate: Decreased environmental temperature Certain medications such as narcotics Increased intra cranial pressure

Respiration depth; is generally described as normal, deep, or shallow. Deep respirations; large volume of air is inhaled and exhaled, inflated most of the lungs.
Shallow breathing involve the exchange of a small volume of air and often the minimal use of a lung tissue
Hyperventilation; refers to very deep, rapid respiration.
Hypoventilation; refers to very shallow respirations

Respiratory rhythm refers to the regularity of the expirations and the inspirations .An respiratory rhythm can be described as regular or irregular.
- Cheyne-stokes breathing, from very deep to very shallow breathing and temporary apnea.

Breath sounds
- Stridor, harsh sound heard during inspiration with laryngeal obstruction
- Stertor, snoring respiration usually due to a partial obstruction of the upper airway.
- Wheeze, continuous, high pitched musical sound occurring on expiration when air moves through narrowed or partially obstructed air way.
Secretions and coughing
- Hemoptysis, the presence of blood in the sputum
- Productive cough, a cough accompanied by expectorated secretions
- Nonproductive cough, a dry, harsh cough without secretions



Preparation for measurement Patient should
abstain from eating, drinking, smoking and taking drugs that affect the blood pressure one hour before measurement.

Remember the following for accuracy of your readings Instruct your patients
to avoid coffee, smoking or any other unprescribed drug with sympathomimetic activity on the day of the measurement

Preparation for measurement
Because a full bladder affects the blood pressure it should have been emptied.

Preparation for measurement Painful procedures
and exercise should not have occurred within one hour.
Patient should have been sitting quietly for about 5 minutes.

Preparation for measurement BP take in quiet room
and comfortable temperature, must record room temperature and time of day.

Position of the Patient Sitting position Arm and back are
supported. Feet should be
resting firmly on the floor
Feet not dangling.
Position of the arm
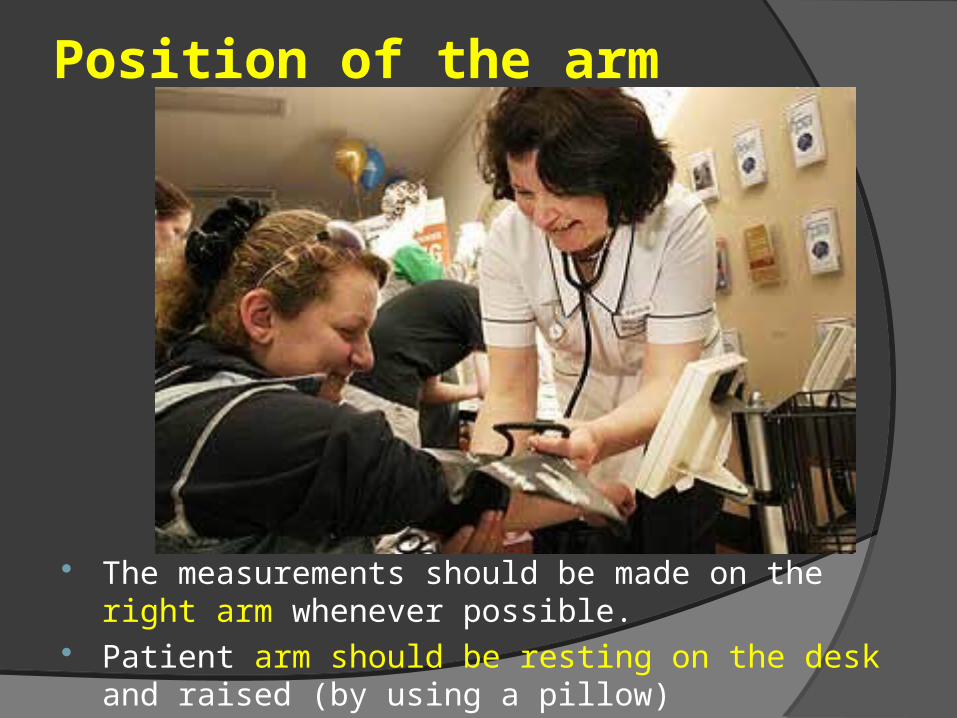
The measurements should be made on the right arm whenever possible.
Patient arm should be resting on the desk and raised (by using a pillow)
Position of the arm
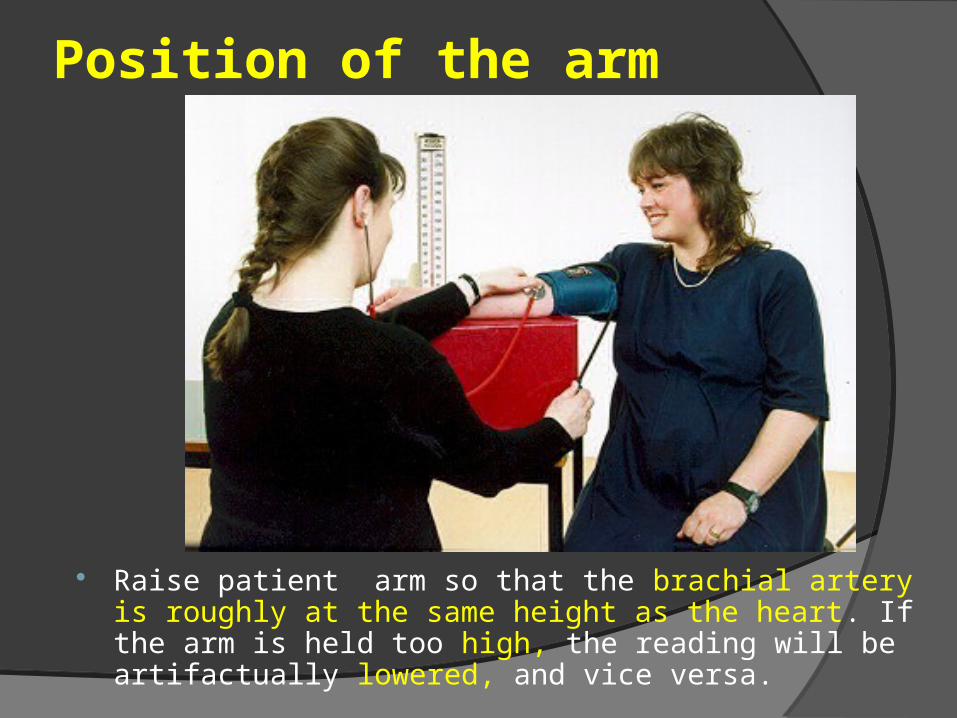
Raise patient arm so that the brachial artery is roughly at the same height as the heart. If the arm is held too high, the reading will be artifactually lowered, and vice versa.

Position of the arm
Palm is facing up. The arm should remain somewhat bent and
completely relaxed


In order to measure the Blood Pressure (equipment) Pediatric Cuff size
Minimum Cuff Width: 2/3 length of upper arm
Minimum Cuff length: Bladder nearly encircles arm

In order to measure the Blood Pressure (equipment)
Adult Cuff size Cuff Width: 40% of
limb's circumference Cuff Length: Bladder at
80% of limb's circumference
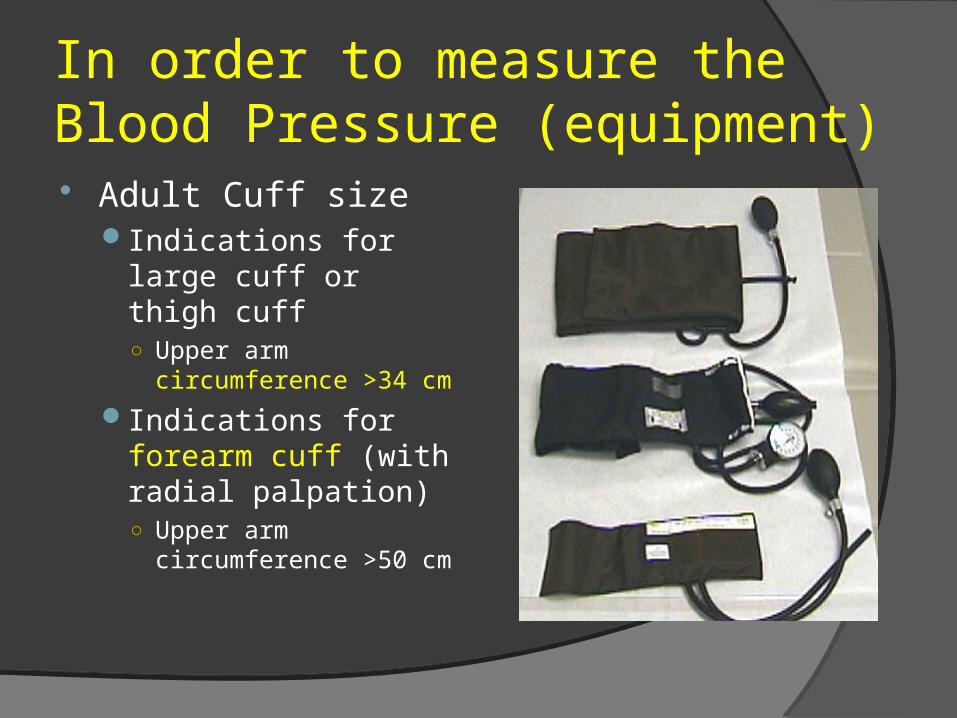
In order to measure the Blood Pressure (equipment) Adult Cuff size
Indications for large cuff or thigh cuff ○ Upper arm
circumference >34 cm
Indications for forearm cuff (with radial palpation) ○ Upper arm
circumference >50 cm

Blood Pressure If it is too small, the
readings will be artificially elevated. The opposite occurs if the cuff is too large. Clinics should have at least 2 cuff sizes available, normal and large.


In order to measure the Blood Pressure (Cuff Position) Patient's arm
slightly flexed at elbow
Push the sleeve up, wrap the cuff around the bare arm
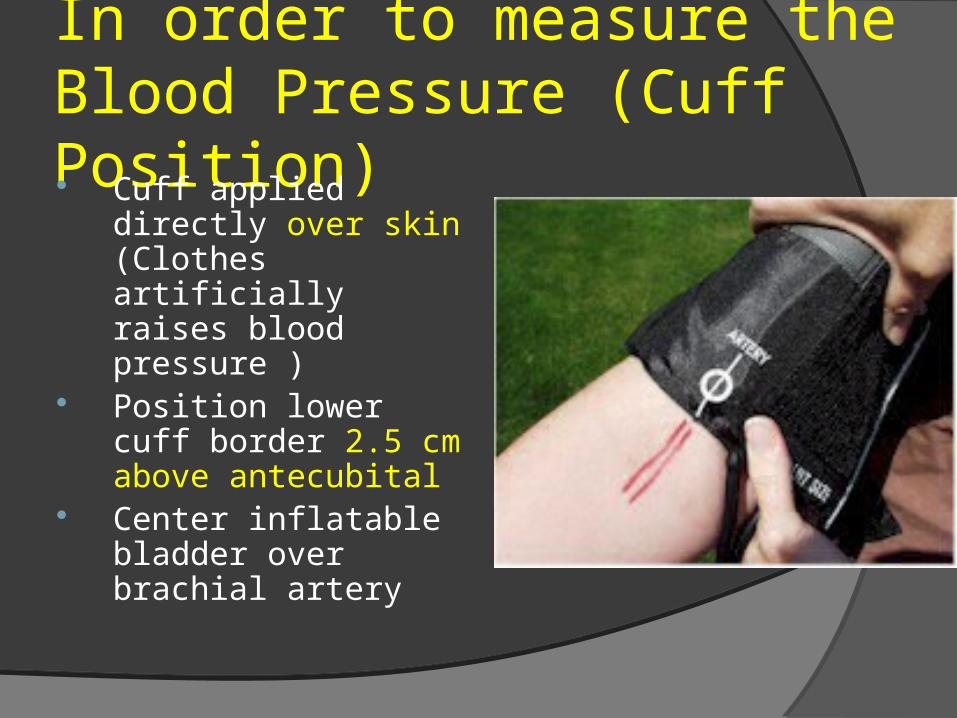
In order to measure the Blood Pressure (Cuff Position) Cuff applied directly
over skin (Clothes artificially raises blood pressure )
Position lower cuff border 2.5 cm above antecubital
Center inflatable bladder over brachial artery

Measurement of the pulse rate
The manometer scale should be at eye level, and the column vertical. The patient should not be able to see the column of the manometer

In order to measure the BP
Feel for a pulse from the artery coursing through the inside of the elbow (antecubital fossa).

In order to measure the BP Wrap the cuff around
the patient's upper arm
Close the thumb-screw.
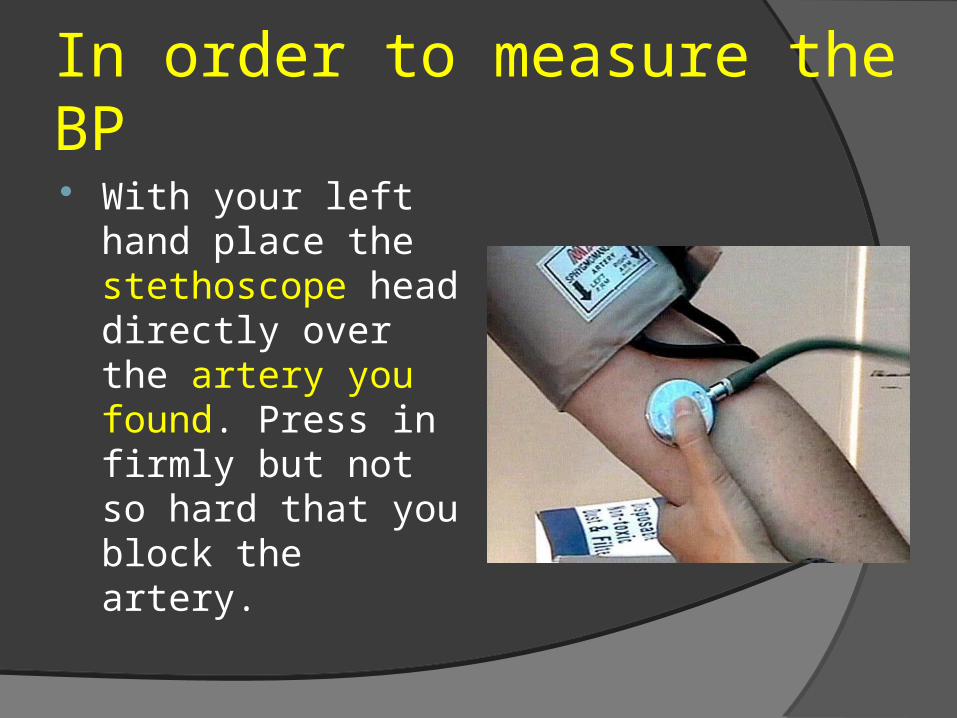
In order to measure the BP With your left hand
place the stethoscope head directly over the artery you found. Press in firmly but not so hard that you block the artery.

Technique of BP measurement Use your right hand
to pump the squeeze bulb several times and Inflate the cuff until you can no longer feel the pulse to level above suspected SBP

Technique of BP measurement
If you immediately hear sound, pump up an additional 20 mmHg and repeat

Technique of BP measurement
Deflate cuff slowly at a rate of 2-3 mmHg per second until you can again detect a radial pulse

Technique of BP measurement Listen for auditory
vibrations from artery "bump, bump, bump" (Korotkoff)

In order to measure the BP Systolic blood
pressure is the pressure at which you can first hear the pulse.

In order to measure the BP
Diastolic blood pressure is the last pressure at which you can still hear the pulse

In order to measure the BP Avoid moving your
hands or the head of the stethescope while you are taking readings as this may produce noise that can obscure the Sounds of Koratkoff.

Technique of BP measurement BP must take
in both arms and one lower extremity.

In order to measure the BP The two arm
readings should be within 10-15 mm Hg. Differences greater then 10-15 imply differential blood flow.

In order to measure the BP If you wish to repeat
the BP measurement you should allow the cuff to completely deflate, permit any venous congestion in the arm to resolve and then repeat a minute or so later.
Remember the following for accuracy of your readings If the BP is
surprisingly high or low, repeat the measurement towards the end of your exam (Repeated blood pressure measurement can be uncomfortable).

In order to measure the BP
You can verify the SBP by palpation. Place the index and middle fingers of your right hand over the radial artery.


In order to measure the BP Diastolic blood
pressure allow free flow of blood without turbulence and thus no audible sound. These are known as the Sounds of Koratkoff.

Blood pressure The minimal SBP
required to maintain perfusion varies with the individual. Interpretation of low values must take into account the clinical situation.

Blood pressure for adult Physician will want to
see multiple blood pressure measurements over several days or weeks before making a diagnosis of hypertension and initiating treatment.

What Abnormal Results Mean
Pre-high blood pressure: systolic pressure consistently 120 to 139, or diastolic 80 to 89
Stage 1 high blood pressure: systolic pressure consistently 140 to 159, or diastolic 90 to 99

What Abnormal Results Mean Stage 2 high blood
pressure: systolic pressure consistently 160 or over, or diastolic 100 or over

What Abnormal Results Mean Hypotension (blood
pressure below normal): may be indicated by a systolic pressure lower than 90, or a pressure 25 mmHg lower than usual
Hypertension
High blood pressure greater than 139-89..

Blood pressure (mm Hg) Normal blood
pressure 100/60 and 139/89.
Prehypertension 120,139-80,89…

Blood pressure may be affected by many different conditions Cardiovascular
disorders Neurological
conditions Kidney and urological
disorders

Blood pressure may be affected by many different conditions Pre eclampsia in
pregnant women Psychological factors
such as stress, anger, or fear
EclampsiaEclampsia

Blood pressure may be affected by many different conditions
Various medications "White coat hypertension" may occur if the
medical visit itself produces extreme anxiety


Remember the following for accuracy of your readings Orthostatic (postural)
measurements of pulse and blood pressure are part of the assessment for hypovolemia.

Remember the following for accuracy of your readings First measuring BP
when the patient is supine and then repeating them after they have stood for 2 minutes, which allows for equilibration.
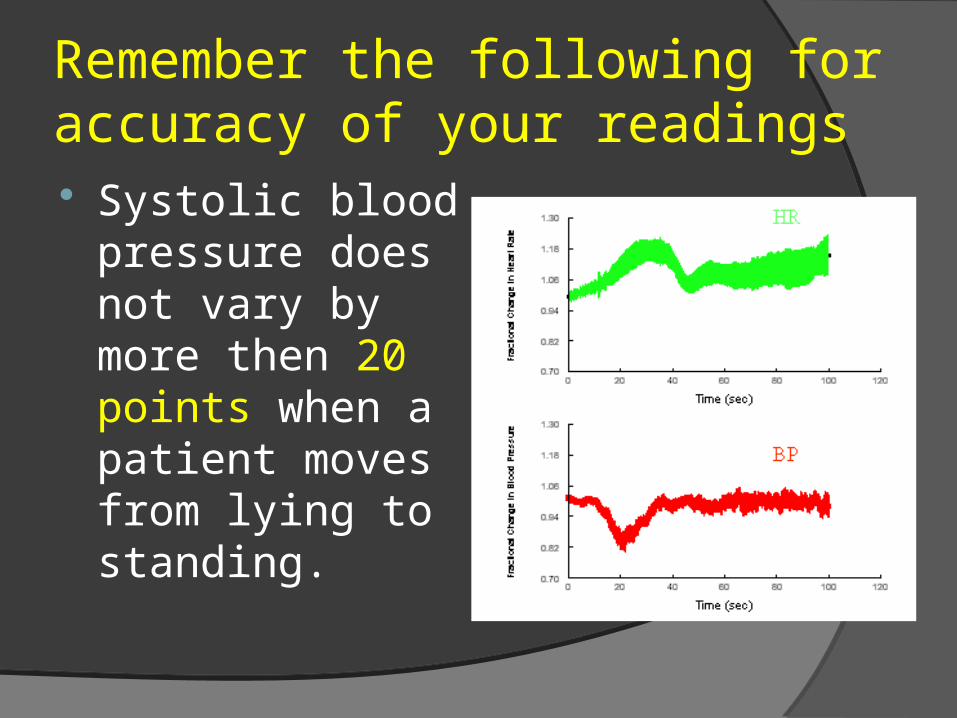
Remember the following for accuracy of your readings Systolic blood
pressure does not vary by more then 20 points when a patient moves from lying to standing.

Remember the following for accuracy of your readings Orthostatic
measurements may also be used to determine if postural dizziness (diabethic autonomic nervous system dysfunction) is the result of a fall in blood pressure.

Vital signs

Oxygen Saturation Over the past
decade, Oxygen Saturation measurement of gas exchange and red blood cell oxygen carrying capacity has become available in all hospitals and many clinics.

Oxygen Saturation Oxygen Saturation
provide important information about cardio-pulmonary dysfunction and is considered by many to be a fifth vital sign.

Oxygen Saturation For those suffering
from either acute or chronic cardio-pulmonary disorders, Oxygen Saturation can help quantify the degree of impairment.
Top Related