Treatment of CML Transplant or Imatinib? Mark B Juckett MD Section of Hematology/BMT University of...
49
Treatment of CML Transplant or Imatinib? Mark B Juckett MD Section of Hematology/BMT University of Wisconsin
-
Upload
ezra-daniels -
Category
Documents
-
view
219 -
download
6
Transcript of Treatment of CML Transplant or Imatinib? Mark B Juckett MD Section of Hematology/BMT University of...

Treatment of CMLTransplant or Imatinib?
Mark B Juckett MDSection of Hematology/BMT
University of Wisconsin

CML - Age specific incidence
BMT Candidates

Clinical Course: Phases of CML
Chronic phase
Median 5–6 yearsstabilization
Accelerated phase
Median duration6–9 months
Blast crisis
Median survival3–6 months
Advanced phases

Cytogenetic Response and Survival With IFN-
Guilhot F et al. N Engl J Med. 1997;337:223-229.
Major response
Pro
po
rtio
n S
urv
ivin
g
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0.0 12 24 36 48 60
Minor or no response
P < .001
Months After Treatment
CCR – 70% OS at 10 yrs

Cytogenetic Abnormality of CML:The Philadelphia Chromosome
•Discovered in 1960 by Nowell and Hungerford•First consistent genetic “lesion” in human cancer

Mechanism of Action of Imatinib Mesylate
Goldman JM, Melo JV. N Engl J Med. 344:1084-1086.

Imatinib for Chronic Phase CMLCytogeneic and Hematologic Responses
All Patients Patients intolerantto interferon
CytogeneticResponse Complete 41% 47% Partial 19% 19%
HematologicResponse
95% 93%
NEJM 346:645, 2002
•Median time on treatment was 17.5 months

Accelerated Disease Study: ResponsesTalpaz, et al, 2002
400mg dose 600 mg dose
Cytogenetic Response
Complete 11% 19% Partial 5% 5%
Complete Hematologic Response
27% 37%
Blood 99: 1928, 2002

Blast Crisis Study: Responses
Sawyers et al Blood 99:3530
Kantarjian et al Blood 99:3547
Cytogenetic Response
N = 260 N = 75
Complete 7% 7% Partial 9% 4%
Any Hematologic Response ( 4 wks)
31% 46%
•Median time to major cytogenetic response was 3 months•Most patients treated with 600mg

Gleevec vs. Interferon for new CML
International Randomized Study (IRIS) 1,106 patients, 177 center, 16 countries
• Gleevec 400 mg/day vs
• INF 5 MIU/M2/day with Ara-C 20mg/M2/day 10 days per month
Median follow-up 19 months Analysis from July 2002
O’Brien S.G. N Engl J Med. 348:994.

Design
IFN- +
Ara-C
Imatinib
Crossover for:• Lack of response• Loss of response• Intolerance of treatment
Crossover
RANDOMIZEO’Brien S.G. N Engl J Med. 348:994.

Primary Endpoints
Time to Progression, defined by:
• Death from any cause
• Accelerated phase or blast crisis
• Loss of complete hematologic response (CHR)
• Loss of major cytogenetic response (MCR : 35% Ph positive)
• Increasing WBC in patients without a CHR
O’Brien S.G. N Engl J Med. 348:994.

Inclusion Criteria
Age 18 to 70
Ph positive CML
• (other cytogenetic abnl OK)
Within 6 months of diagnosis
Chronic phase of disease
No prior therapy except hydroxyurea & anagrelide
O’Brien S.G. N Engl J Med. 348:994.

Patient Status
Imatinib IFN + Ara-C
Randomized 553 553
Continued initial treatment
474 (86%) 60 (11%)
Discontinued initial treatment
68 (12%) 175 (32%)
Crossed Over 11 (2%) 318 (58%)
O’Brien S.G. N Engl J Med. 348:994.

Complete Hematologic Responses
96%
67%
p<0.001
ImatinibIFN+Ara-C
% re
spon
ding
0
10
20
30
40
50
60
70
80
90
100
Months since randomization0 3 6 9 12 15 18 21
O’Brien S.G. N Engl J Med. 348:994.

Response Imatinib
N=553
IFN+Ara-C
N=553
Major ( 35 Ph+) 85% 22%
Complete (0% Ph+) 74% 9%
Partial (1-35% Ph+) 11% 13%
Best Cytogenetic Response
p<0.001O’Brien S.G. N Engl J Med. 348:994.

Major Cytogenetic Responses
84%
30%
ImatinibIFN+Ara-C
% re
spon
ding
0
10
20
30
40
50
60
70
80
90
100
Months since randomization0 3 6 9 12 15 18 21
p<0.001
22%
85%
O'Brien, S. G. et al. N Engl J Med 2003;348:994-1004

Patients Without Progression
Estimated rate at 12 monthsImatinib 97.2% (p<0.001)IFN+Ara-C 80.3%
ImatinibIFN+Ara-C
= Censored observations
% w
ithou
t pro
gres
sion
0
10
20
30
40
50
60
70
80
90
100
Months since randomization0 3 6 9 12 15 18 21

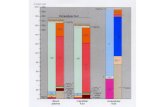
Summary of 18 Month Data
92
74
97 95
3.38.5
76
15
0
20
40
60
80
100
FFP OS AP/BC CCR
Imatinib
INF/ARAC
<0.001
<0.001
O’Brien S.G. N Engl J Med. 348:994.

Quality of Life
Hahn, E.A. et al. JCO 2003;21:2138-46
Imatinib vs. INF/ARAC

Does higher dose improve outcome?
Phase II study of 400mg twice daily 114 patients within 12 mo of Dx
• Compared to historical controls Median follow-up 15 months Results
• CHR 98%• CCR 90% (52% by 3 months)• Sokal high risk – 76% vs. 95%• Complete PCR response 28% (18 mo)
– Compared to 7% historically
Kantarjian H. Blood. 103:2873, 2004.

Results After High Dose Imatinib
Complete Cytogenetic response Complete Molecular Response
Kantarjian H. Blood. 103:2873, 2004.

Summary of Imatinib for CML
Well tolerated treatment compared to INF/ARAC• Improved QOL
Decreased progression, improved CCR rates• 18 mo rate of AP/BC 3.3%• 18 mo rate of CCR 76%
Limited activity in AP/BC Higher dose may improve cytogenetic and
molecular responses

Transplantation for CML
Curative Treatment for most patients High rate of morbidity and mortality Problems of:
• Toxicity of preparative regimen• Graft-vs-Host disease• Relapse
Regimens differ in toxicity• Cy/TBI• tBU/CY• “Mini” transplants

SURVIVAL AFTER ALLOGENEIC TRANSPLANTS FOR CML IN CHRONIC PHASE 1994-1999
PR
OB
AB
ILIT
Y,
%
100
0
20
40
60
80
0
YEARS
1 2 3 4 6
SUM02_3.ppt
P = 0.0001
HLA-identical sibling, 1y (N = 2,876)
HLA-identical sibling, 1y (N = 1,391)
Unrelated, 1y (N = 613)
Unrelated, 1y (N = 936)
5

100-DAY MORTALITY AFTER HLA-IDENTICAL SIBLING TRANSPLANTS 1999-2000
SUM02_39.ppt
MO
RT
AL
ITY
, %
100
0
20
40
60
80
464
3591,267
90
67
952
AML ALL CML MDS AplasticAnemia
ImmuneDeficiency
Numbers on bars = numbers of patients evaluable
CR1CR2+Other
386
173
212433
437258
CPAPBP

100-DAY MORTALITY AFTER UNRELATED DONOR TRANSPLANTS 1999-2000
SUM02_40.ppt
MO
RT
AL
ITY
, %
100
0
20
40
60
80
301
348
55883
53
189
AML ALL CML MDS AplasticAnemia
ImmuneDeficiency
Numbers on bars = numbers of patients evaluable
CR1CR2+Other
204
152
157 113241
258
CPAPBP

Oral BU/CY vs. CY/TBI
Clift RA. Blood. 94:3960, 1999.

BMT With tBU/cy and Matched Sibling
Radich JP. Blood. 102:31, 2003.

Radich JP. Blood. 102:31, 2003.
BMT With tBU/cy and Matched Sibling

Non-myeloablative transplant for Chronic Myeloid Leukemia
Disease Free Survival Chronic GVHD
Or, Blood 101:441, 2003
N = 24

Choosing BMT vs. Imatinib
Assumption• Imatinib is a preferred initial treatment IF long
term outcome is unchanged.– Less early risk– Good QOL– Cost ??
Consider transplantation for those who are not responding appropriately (who are those?)

Choosing BMT vs. Imatinib
Recommend BMT to some patients:
• Those who are likely to do well with transplant
• Those who are likely to do badly with Imatinib

Who will do badly with Imatinib?
Majority of patients will enter complete cytogenetic remission
Some will:• Fail to enter CCR• Progress to AP/BC• Become resistant to imatinib
Conventional cytogenetics is insensitive to predicting these events
Risk scores are helpful (Sokal, etc.) but not validated on Imatinib patients

Molecular Monitoring
Real-Time Quantitative PCR seems best Compares amplification of BCR-ABL transcript to
control gene – usually BCR or ABL Baseline transcript quantity varies between labs Log change in transcript seems to be consistent
between labs. Does not identify other clonal abnormalities May detect disease down to 0.01 – 0.001%

Reduction of BCR-ABL Transcript On Treatment
All patientsOn IRIS study

Reduction of BCR-ABL Transcript After CCR
Hughes, T. P. et al. N Engl J Med 2003;349:1423-1432
PatientsIn CCROnly

Imatinib Is Superior in Reducing Transcript Level
Estimated log-reduction of BCR-ABL transcripts after 12 months of first-line therapy by treatment arm.

Hughes, T. P. et al. N Engl J Med 2003;349:1423-1432
PFS After 12 Months of Imatinib

Correlation between Cytogenetics and qRT-PCR
Branford, S. et al. Leukemia 17:2401, 2003

Probability of Achieving 3-log Reduction
Branford, S. et al. Leukemia 17:2401, 2003

Patient Responses to Imatinib
Branford, S. et al. Leukemia 17:2401, 2003

P-loop Mutations Predict Short Survival
Branford, S. et al. Blood 102, 276, 2003

Clonal Evolution Predicts Short Survival
Cortes, J.E. et al. Blood 101:3794, 2003

Who will do well with Imatinib?
Patients who:• Enter a CCR• Have large reduction in BCR-ABL transcript
(3-log ?)• Have an early response
Patients who do not:• Have point mutations within the P-loop• Additional clonal abnormalities
Still no long-term survival information

Who will do well with BMT?
Sokal and Hasford scores not helpful in predicting success after BMT
CML-CP Risk Score (only chronic phase)• Donor type (Matched Sib vs. MUD)• Age (<30, 30-40, >40)• Donor-recipient gender (FM, other)• Interval (<1 yr vs. 1 yr)• Performance Status (KPS > 80%)
Late stage disease• Always poor risk

CML-CP Risk Score
Donor type
Matched Sib 0
Matched Unrelated 2
Age
<30 0
30 – 40 1
>40 2
Donor recipient gender
Female Male 1
Other 0
Interval from Diagnosis
< 1 year 0
> 1 year 1
Performance Status
KPS > 85 0
other 1
Passweg, J.R. et al. BJH 125:613, 2004

Survival after BMT for CML by CML-CP score
Passweg, J.R. et al. BJH 125:613, 2004

Deciding between BMT and Imatinib
Patient issues:• Psychosocial (chronic vs. cured disease)• Perception of immediate vs. future risk• Tolerance of medical care (a lot vs. a little)
Doctor issues:• Tolerance/efficacy of imatinib• Availability of BMT• Comorbid diseases
Future issues:• Combinations (endless possibilities)• Novel Transplant approaches