Topic Review(Trauma Cholesyctitis)
18
Review 報報報: Clerk 報報報 Acute cholecystitis Tokyo Guidelines J Hepatobiliary Pancreat Surg (2007) 14:15-26, 78-82, 91-97 1
-
Upload
vincent-wang -
Category
Health & Medicine
-
view
802 -
download
0
Transcript of Topic Review(Trauma Cholesyctitis)

1
Review
報告者: Clerk 王威仁
Acute cholecystitisTokyo Guidelines
J Hepatobiliary Pancreat Surg (2007) 14:15-26, 78-82, 91-97

2
Definitions, pathophysiology, and epidemiology

3
Definition• an acute inflammatory disease of the
gallbladder

4
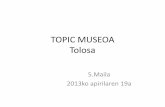
Incidence• 3%–10% of all patients with abdominal pain.
Under 50 years old (n = 6317) 50 years and over (n = 2406)Nonspecific abdominal pain
AppendicitisAcute cholecystitis
IleusAcute hepatitis
DiverticulitisCancerHernia
Vascular lesion
39.5%32.0%6.3%2.5%1.6%<0.1%<0.1%<0.1%<0.1%
Acute cholecystitisNonspecific abdominal pain
AppendicitisIleus
Acute hepatitisDiverticulitis
CancerHernia
Vascular lesion
20. 9%15.7% 15.2%12.3%7.3%5.5%4.1%3.1%2.3%
All patients with abdominal pain

5
Etiology• 90%–95% by cholecystolithiasis • 5%–10% by acalculous cholecystitis

6
Risk factors• 4/5F(fair, fat, female, fertile, forty)• Drugs(indirect)• Ascaris, AIDS
Etiological mechanism Drug/Treatment Direct chemical toxicity Hepatic artery infusion Promotion of stone formation by bile Inhibition of ACAT activity Progesterone, fibrate Increased hepatic lipoprotein receptors Estrogen Induction of acute cholecystitis in patients with cholelithiasis
Thiazides (unconfirmed)
Promotion of calcium salt precipitation in bile Ceftriaxone octreotide Altered mobility of the gallbladder Narcoid, Anticholinergic drugs Promotion of hemolysis Dapsone Immunological mechanism Antimicrobial drugs (erythromycin,
ampicillin), Immunotherapy

7
Pathophysiology• Two factors determine the progression to
acute cholecystitis 1) degree of obstruction 2) duration of the obstruction

8
Types of complications• Perforation of the gallbladder• Biliary peritonitis• Pericholecystic abscess• Biliary fistula(obstruction at the ileocecal valve)

9
Prognosis• Mortality :– acute cholecystitis : 0–10%– postoperative cholecystitis and acalculous
cholecystitis : 23%–40%• Causes of mortality :
infection myocardial infarction, cardiac failure, pulmonary infarction.
• Postoperative causes of mortality :pneumonia and sepsis malignant tumor, respiratory failure, cardiac failure

10
Recurrence rate after conservative treatment
• The recurrence rate of acute cholecystitis while waiting for cholecystectomy following conservative treatment : 2.5% to 22%
• Long-term recurrence : 10%–50% (observation for 6 months to several years)

11
Diagnostic criteria and severity assessment

12
Diagnostic criteriaA. Local signs of inflammation :
(1) Murphy’s sign, (2) RUQ mass/pain/tendernessB. Systemic signs of inflammation :
(1) Fever, (2) elevated CRP, (3) elevated WBC countC. Imaging findings:
imaging findings characteristic of acute cholecystitis(1) One item in A and one item in B are positive(2) C confirms the diagnosis
CRP level (>=3 mg/dl ) + sono findings :sensitivity of 97%, specificity of 76%positive predictive value of 95%

13
Imaging findingsSono:
① Sonographic Murphy sign ② Thickened gallbladder wall (>4 mm)③ Enlarged gallbladder (long axis diameter >8 cm, short axis diameter
>4 cm)④ Pericholecystic fluid collection
CT:⑤ Thickened gallbladder wall⑥ Pericholecystic fluid collection⑦ Enlarged gallbladder⑧ Linear high-density areas in the pericholecystic fat tissue.
MRI:⑨ Pericholecystic high signal⑩ Enlarged gallbladder⑪ Thickened gallbladder wall.

14
Severity gradingA. Mild (grade I) acute cholecystitis
① Not moderate (grade II) or severe (grade III)② Healthy patient with no organ dysfunction and only mild
inflammatory changes in the gallbladder
B. Moderate (grade II) acute cholecystitis① Elevated WBC count (>18 000/mm3) ② Palpable tender mass in the RUQ③ Duration of complaints >72 hrs④ Marked local inflammation
C. Severe (grade III) acute cholecystitis① Dysfunction of Cardiovascular, Neurological, Respiratory,
Renal, Hepatic or Hematological

15
Surgical treatment

16
Q1. When is the optimal time?earlier is preferable
Q2. Laparoscopic cholecystectomy or open cholecystectomy?Laparoscopic cholecystectomy is preferable
Q3. Optimal surgical treatment according to grade of severityMild: early laparoscopic cholecystectomy Moderate: early cholecystectomy. However, if severe local inflammation, early gallbladder drainage (percutaneous or surgical) is indicated.Severe: urgent management of organ dysfunction and management of severe local inflammation by gallbladder drainage and/or cholecystectomy. Delayed elective cholecystectomy should be performed later.

17
Q4. What are the complications of LC?Bile duct injury and injury of other organs
Q5. When is the optimal time for conversion fromlaparoscopic to open cholecystectomy?When they experience diffi culty in performing LC
Q6. When is the optimal time for cholecystectomyfollowing PTGBD?Early cholecystectomy during the initial hospital stay is preferable
Q7. When is the optimal time for LC after endoscopic stone extraction in patients with cholecysto-choledocholithiasis?Early cholecystectomy following endoscopic stone extraction during the same hospital stay is preferable

18
Thanks for your attention!