Short febril illness2016 new
112
ن م ح ر ل ه ا ل ل م ا س ب ن م ح ر ل ه ا ل ل م ا س ب م ي ح ر ل ا م ي ح ر ل اShort febrile illness Short febrile illness BY BY : : Dr, WALAA SALAH MANAA Dr, WALAA SALAH MANAA SPECIALEST OF SPECIALEST OF fever fever & PEDIATRIC & PEDIATRIC ش ل م ي ش ل س م
-
Upload
walaa-manaa -
Category
Health & Medicine
-
view
136 -
download
3
Transcript of Short febril illness2016 new

بسم الله الرحمن بسم الله الرحمن الرحيمالرحيم
Short febrile illnessShort febrile illnessBYBY: :
Dr, WALAA SALAH MANAADr, WALAA SALAH MANAA SPECIALEST OF SPECIALEST OF fever fever & PEDIATRIC & PEDIATRIC
مـستشفى حمـيات كـفر الشـيخمـستشفى حمـيات كـفر الشـيخ

قال صلى الله عليه وسلم :قال صلى الله عليه وسلم : ) إن الحمى من فيح جهنم فأبردوها ) إن الحمى من فيح جهنم فأبردوها
بالماء ( بالماء ( رواه البخاريرواه البخاري
وقوله عندما ذكرت الحمى فسبها وقوله عندما ذكرت الحمى فسبها رجل :رجل :
) ال تسبها فإنها تنقى الذنوب كما ) ال تسبها فإنها تنقى الذنوب كما تنقى النار خبث الحديد ( رواه تنقى النار خبث الحديد ( رواه
مسلممسلم

Controlled Inc. of body Controlled Inc. of body temp. above normaltemp. above normal

NormalNormal::
( N….rectal: 36.5-37.8).( N….rectal: 36.5-37.8). ( N……..oral: less 0.5).( N……..oral: less 0.5). ( AM ….....: ( AM ….....: >> 37.2). 37.2). ( PM ………….: ( PM ………….: >> 37.7).37.7).

FF = 9 × c +32.= 9 × c +32. 55 cc = 5 )F -32( . = 5 )F -32( . 99
2°F (1.1°C), 2°F (1.1°C),

IF fever is transient esp. in children & temp. decrease to normal with in 1 hr. without antipyretics or cold fomentations.
(this case is consider
afebrile)

Measuring ! temp. Measuring ! temp. is mandatory is mandatory
,,,,,,,,,,why?,,,,,,,,,,why?1-some pt. may c/p of
joint pain headache without saying fever.
2-fever may not be felt by tactile palpation..

DegreeDegree::Mild….rectal….37.8-38.4 c.Mod…rectal….38.5-39.5 c.High…rectal….39.5- 41 c.Hyperpyrexia…> 41 c.

HyperthermiaHyperthermia:: It is an elevation of body temp. dt ext.
heating : 1)heat stroke (S.S). 2)high incubator temp.
SO Hyperthermia is not a true fever. because the elevation of body temp. is against its desire.
Fever…pt. feels cold ± cold extremities.
Hyperthermia pt. feels hot + hot extremities.

HypothermiHypothermiaa
1-septic shock.2-enviromental exposure. 3-hypothyrodism.4-DM with autonomic
dysfunction.


Types:Types:1) Continuous: temp. does not reach the normal
base line, at any time in 24 hrs. & variation between
upper pole & lower pole < 1 c. 2) Remittent: temp. does not reach the normal base line, at any time in 24 hrs. & variation between
upper pole & lower pole >1 c.
3) Intermittent or hectic: at any time in 24 hrs. temp. reach the base line.
4) Relapsing: there are several days of cont. fever followed by several days of normal temp .

Continuous:Sepsis-drug.
Remittent:typhoid &brucellosis`
Intermittent or hecticAbscess.

What are the factors What are the factors which produce dynamic which produce dynamic
pattern of fever & pattern of fever & diseases?diseases?i.e.
=atypical presentation
=change in specific temp. pattern
=clinical overlap.

1-Chang in ! Environment
2-Misuse of antibiotics.
3-Vaccination.
4-Mutation of infectious agents (RVF).

Causes:Causes:
Common causes:Common causes: 1-Infections:1-Infections:
Bacterial, Viral, Fungal , ParasiticBacterial, Viral, Fungal , Parasitic 2-Collagen diseases. 2-Collagen diseases. 3-Tissue injury or infarction3-Tissue injury or infarction 4- Immunization reactions4- Immunization reactions.. 5- Inflammatory disorders 5- Inflammatory disorders 6-6- Drug Fever:(DD nasocomial infection)Drug Fever:(DD nasocomial infection) Penicillin , cephalosporin's , Penicillin , cephalosporin's ,
sulphonamides , phenytoin ,antihistamines , aspirin & sulphonamides , phenytoin ,antihistamines , aspirin & theophylline intoxication and theophylline intoxication and
anti cholinergics, paracetamolanti cholinergics, paracetamol. .

Other causes:Other causes: 7- Malignancy.7- Malignancy. 8- Heat illness.8- Heat illness. 9- Allergic reactions.9- Allergic reactions. 10- Thyrotoxicosis.10- Thyrotoxicosis. 11- Hypothalamic injury.11- Hypothalamic injury. 12- Hyperactivity, seizers or vigorous12- Hyperactivity, seizers or vigorous exerciseexercise 13- Neuroleptic malignant syndrome.13- Neuroleptic malignant syndrome. 14- Malignant hyperthermia.14- Malignant hyperthermia. 15- Factitious fever [Hysterical]15- Factitious fever [Hysterical]

Factitious fever: 10% of FUO adults with health care experience. psychiatric problems. history of multiple hospitalizations. fever may be caused by injection of non sterile
material (eg, feces, milk).
* Rapid changes of body temperature without associated shivering or sweating,
* large differences between rectal and oral temperature,
* discrepancies between fever, pulse rate, or general appearance.

Non infectious fever:………………… infectious fever Non fever infections: 1-elderly & neonats. 2-severe debilitating
diseases. 3-immune deficiency pt. HIV.

Precaution in temp. Precaution in temp. Measurement to avoid Measurement to avoid Factitious feverFactitious fever::

1- rectal temp. is more accurate.2- oral…………is acceptable.3- tactile………is not acceptable.
why?(Skin may be cold in: obese- collapsed pt.---Shock--- gram –ve infection--- exposure to cold)
4- axillary & skin temp. is not accurate,
(especially in shocked pt. & in hot or cold whether)

Neither the height of the temp. nor fever curve correlates with etiology or severity of the disease.
Fever >39.5 is of greater concern & often point to infection.

Harmful effects of Harmful effects of feverfever
There are 3 circumstances in which high fever can be harmful ,specially in young children :
1)cardiac pt., hypoxia (increased oxygen
consumption and cardiac output) 2)>42 c CNS damage. 3)febrile convulsion.

Fever is not an Fever is not an enemy…….it mayenemy…….it may be be
even a friendeven a friend?..?.. 1( it activate leucocytosis and
phagocytosis.2( Inc. interferon production.3( It increases the sensitivity of the
organisms to antibiotics.4( increases the sensitivity of tumor
cells to chemotherapy. 5( proliferation and transport of
lymphocytes.

Classification Classification according to duration:according to duration:1) Short febrile illness (acute fever): < 8day.
2) Prolonged fever (sub acute form) : > 8days-- < 21days. Or >21days with out doing ! traditional
investigation.
3) FUO : > 21 days without diagnosis after doing complete clinical history & all traditional investigation.

Short febrile Short febrile illnessillness::
*Fever less than 1 w.
* 25% of urgent presentation. Our role is to diff. if it is:
a( simple benign infection.
B( serious infection . which is life threatening need urgent ttt.

Short febrile Short febrile illnessillness::
This category include:
1-most viral infection (e.g. URTI which often cured within 1 week).
2-bacterial self-limited disease like URTI.
3-specific fever like typhoid & brucellosis and other ,in its beginning time.

Short febrile illnessFocal infection Fever with out focus
simple serious

Focal infectionFocal infection=organ related=organ related
(1)CNS:
Meningitis--- encephalitis ---br. Abscess.
(2)Respiratory:
Upper: nasoph.—O.M.—sinusitis Tonsillitis—laryngitis
Lower: bronchitis—brochiolitis----Pneumonia---lung abscess empyma.

(3)G.I.T.:
stomatitis,G.E.,hepatitis,peritonitis, appendicitis,pancreatitis.
(4)U.T.I.:
pyelonephritis,,cystitis. (5)Orthop.inf.:
osteomylitis,arthritis. (6)Skin inf.:
cellulitis, abscess

Short febrile illnessFocal infection Fever with out focus
simple serious

Serious Serious infectioninfection:: =serious focal inf. should be excluded…:
1)bacterial meningitis:
Dist. consciousness\convulsion\ mening. Irritation \ inc. ICP.
2)Pneumonia: Resp. distress \ crepitation \ bronch. Breathing.

3)Pyelonephritis: Chills \ dysurea)hot st. urine( \freq.\ loin
tenderness.
4)Peritonitis: Abd. tenderness \ distention. 5)Osteomyelitis&Arthritis:
Focal tenderness \ swelling \ limitation of
movement.

C/O of inc. Intra-cranial tension
Headache : esp. in older children &adult.Vomiting: repetitive-frequent-projectile.Bulging ant. Fontanelle 20% in infant < 1 yr.High pitched cry.Photophobia.



N.BN.BIn neonates )=sepsis syndrome( fever ,lethargy ,fits ,bulging ant. Fontanelle ,g.i.t.
dysfunction ,vomiting .
Children & adult )fever-neck rigidity-headache-neck pain-
irritability –change in GCS-vomiting-fits(.

Signs of meningeal Signs of meningeal irritationirritation
Late singes Neck stiffness. Back stiffness. +ve kernig’s
sing. +veBrudziniski’
neck sign. +veBrudziniski’
leg sign.
Early singe chin-chest test. Chin-knee
kissing test. Tripod singe

Rapid flexion of the head is accompanied by brisk flexion of both knee

Inability to extend the knee,when the thigh is flexed at the hip

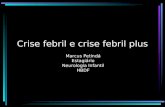
Significant left lower lobe
pneumonia and empyema in a 14-
year-old with fever

N.BN.B.)SFI(.)SFI(1)Most children can
tolerate mild to moderate Fever with no problem.
2)With high fever below 2 yr .,possibilities of serious bact. Infection is high.

3)Strept. Pharyngitis
below 2nd yr.is not common, so its diagnosis is not simply made.
)DD: purulent
tonsillitis(

4)O.M is very common in inf.&child.
-so exclusion of focal infection is not complete
without otoscop ear exam.
5)Skin inf. gluteal. & Perianal abscess.

Vomiting in SFI : is not a localizing sign: )GE.-appendix-entrica-CNS-
Renal failure) .
Diarrhea also is not a localizing sign.
(parentral)
Always remember

Grunting: ……. may occur at high
temp. )DD( : Pneumonia,,
empyema(, so it may be dt causes
other than pneumonia.

In early focal infection:
(24-48 hr) the focus is not be evident at initial exam.
Re exam.after24-
48hr reveal the focus in 40% of cases

Short febrile illnessFocal infection Fever with out focus
simple serious

Non specific feb. illness=fever with out focus
=simple fever
viremia bacteremia septicemia

Clinical diagnosis of viremiaClinical diagnosis of viremia::
Temp.: not high
G.condition: fair
ttt: antipyretic &re exam. After 24-48hr (40%may reveal a focus
after re exam.(. Investigation:no need

Clinical diagnosis of Clinical diagnosis of bacteremiabacteremia::
Temp.: high
G.codition: not fair ,sick
Investigation CBC(>15000),,CRP+ve,,
ESR .ttt :if investigation is not
available ttt with broad specterum antibiotic &
re exam. After 1-2days.


Clinical diagnosis of Clinical diagnosis of septicemiasepticemia::
Temp.: very high or even hyperpyrexia ,or….
G.condition: seriously ill ±
vomiting, pallor, rash, toxic look ,unconscious, cold extremities.

ManagementManagement of septicemiaof septicemia::urgent hospitalizationurgent hospitalization
++urgent investigationurgent investigation++immediate combinedimmediate combined
Antibiotic tttAntibiotic ttt . .

InvestigationInvestigation::
CBC >15,000 PMNL +toxic granule.ESR high. CRP +ve. Blood culture. Urine culture. CSF cytology& microbiology.

Septicemia:Septicemia:Is a serious condition with a high morbidity
& mortality so our attention should be directed to its manifestations & complication .
Because early detection early ttt good prognosis

Manifestations & Manifestations & complicationcomplication. .
1)Serious focal infection: meningitis, pneumonia ,osteomyelitis, Arthritis ,peritonitis. 2)Acute hemolytic anemia: dt dirct RBCs destruction. 3)consumptive thrombocytopenia: dt direct platelets destruction

4)DIC: dt endotoxemias, shock ,acidosis
5)Septic shock :dt hypovolemic&
Cardiogenic. 6)Acute renal failure :dt toxemia & shock 7)Toxic encephalopathy:
dist. Consciousness + inc.ICP + fits.


ConclusioConclusionn

Short febrile illnessFocal infection Fever with out focus
simple serious

Non specific feb. illness=fever e out focus
=simple fever
viremia bacteremia septicemia

Fever Fever presentationpresentation

Fever with Fever with headacheheadache::
1. Menengitis,encephalitis, menengism……… (occipital).
2. Influenza, common cold.
3. Typhoid …(frontal+dullach).
4. RVF.5. malaria.

Fever with chills or Fever with chills or rigorrigor::
Chill : sensation of coldness. Rigor: tonic contraction of
muscles + shacking of whole
body. + stucking of the teeth .
*** Chill : may accompany marked rise of temp. in any fever.

RigorsRigors: : 1-malaria 2-influenza 3-UTI. 4-pyaemia & septicaemia. 5- pus under tension (subphrenic abscess,,,,liver abscess,,,, cholangitis,,,,Puerperal sepsis). 6-after IV fluid containing pyrogens. 7-after taking antipyretics.dt sudden drop of temp.

Fever with painsFever with pains::1-Eye pain mostly viral in origin.2-Backpain meningitis ,encephalitis ,
RVF, brucellosis3-Chest pain bronchitis , pneumonia,
pleurisy.4-abdominal pain typhoid ,
peritonitis, hepatitis.

Fever with Fever with epistaxisepistaxis
1-Acute typhoid fever.
2-Acute Rh. Fever.3-Acute leukemia.4-haemorrahgic
fevers.

Fever with Fever with pallorpallor::
1- Acute Rh. Fever.
2-malaria.3-Haemolytic
anaemia.4-Malignancies.

Fever with herpes Fever with herpes labialislabialis::
1-Common cold & influenza.
2-Malaria.3-Meningo coccal
meningitis.4-Pneumonia.
exclude typhoid and brucella

Fever with Fever with jaundicejaundice::
1-Viral hepatitis.2-Paratyphoid B fever.3-I.M.N.4-Liver abscess.5-Falciparum malaria.6-Haemolytic crises.7-Septic cholangitis.8-Acute leukemia.9-Yellow fever.

Fever with Fever with convulsion:convulsion:
1-febrile convulsion.2-C.N.S.infection.3-fever associated
with other causes of seizures:
* epilepsy . * cerebral stroke . * cerebral tumor. *cerebral trauma . * drug or alcohol
withdrawal.

Fever with coma:Fever with coma:1-CNS infection encephalitis meningoencephalitis (viral, bact., rechetsial, fungal,
parasitic.)2-cerebro-vascular stroke (pontine hge. , subarachnoid hge., cerebral hge.)3-infection associated with CNS trauma , brain tumor , toxic coma : * external toxins (poison
ingestion) * internal toxins .eg. diabetic
coma, uremia , hepatic coma ,,,,,,,)

Do not diagnose hysterical coma in Do not diagnose hysterical coma in febrile pt.febrile pt.
Do not lose the hope or the Do not lose the hope or the prognosis in prolonged coma. prognosis in prolonged coma.


Fever with rash:Fever with rash:May indicate a serious bacterial
infection in 20% of cases )e.g.menengococcal menengitis,HIb,,,,,,,,,(
80% of cases are caused by viral infection.

Fever with Fever with rashrash::1-very )varecilla( chicken pox &
menigitis.2-Sick scarlet fever & erysipelas.3-People small pox.4-Must measles.5-Take typhus.6-Entire enterica.7-good glandular fever.8-Rest relapsing fever.


Dangerous sings in Dangerous sings in fever with rashfever with rash::
1-if associated with 1-if associated with sever sever constitutional constitutional S&S.S&S.
2-if hemorrhagic.2-if hemorrhagic.3-if is extensive.3-if is extensive.4- if associated with 4- if associated with
shock or coma.shock or coma.

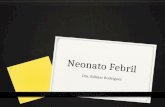
Infant with necrotizing fasciitis, a complication of varicella


fever Hosp. fever Hosp. casescases
(1)(1)



18 yr. old female pt. presented by fever,arthralgia.ESR..40-75……ASOT400
With history of recurrent tonsillitis My diagnosis was Rh. Fever& I start
LAP.……………………………………………………)true….false(.

((22))

13yr old male presented by fever ,vomiting ,abd.pain since 2 days Widal test was done 1/160 my diagnosis was typhoid fever & start ttt by ciprofloxacin………………………………… …………………………(true….false)..

Widal testWidal test::
)O(raising.7-10 day.
)H(------carrier..

Case definition:Case definition:Suspected case : fever , headache , abd. Discomfort, +at least 3 of the following: 1-toxic look 2-bronchitic chest. 3- typantic abdomen 4-palpable recessive spleen )disappear after cure(

Probable caseProbable case ::
suspected case+ +ve Widal test by
tube agglutination>160 after 1 week of fever.

Confirmed case:Confirmed case: any suspected case with + ve blood
culture. Or : significant rise in the tube
agglutination..N.B. bright spleen is one of the abdominal U/S
findings if the bright spleen is reversible after cure.

Chlormaphenichol is not prescribed except WBCS>3.000
Quinolones are contra indicated: 1-child<18 yrs 2-pregnancy & lactation. 3-elderly> 65yr 4-psycho-neurological diseases. 5- joint disease.
Always remember

(3)(3)

Degree of Degree of tetanustetanus::
Mild: trismus ,distance between upper & lower
incisors >2cm.
Moderate: trismus + mild fits+ D.I <2cm.
Severe : trismus +frequent fits +)D.I(<1cm




((44))



Management of Management of febrile patientfebrile patient

11--antipyreticsantipyretics::1-paracetamol,,,,,10-15mg/kg/dose_4-6
hr.2-acetylsalicylic acid ,,,,,,,,,,,,,,,,,,,, Ryes syndrome.3-Ibuprofen,,,,,,,,,,,,,,,,,,10-15mg/kg/
dose.4-diclophenac Na.,,,,,,,,, 0.5
mg/kg/dose.

Indication of antipyretics in SFI:Indication of antipyretics in SFI:
1-Very high fever to comfort the pt..
2-To avoid 2nd ry harmful effect of hyper metabolic state ) elderly , cardiac , chest disease(.
3-To avoid febrile convulsions in child
with +ve history of febrile convulsions

22--External External coolingcooling::1-By tepid sponges with tap water….YES.
2-Cold or iced water sponges ……….NO. )as it induces shivering & inc. heat production( 3-Alcohol sponges……………………….NO, )as it causes peripheral V.C. & dec. heat loss( 4- Running tap water over limbs……..V.good ) inc. heat loss by conduction(.

33--Internal Internal coolingcooling::
Used in pt. with hyper pyrexia not responding to antipyretics & tepid sponges .
E.g: 1-cold I.V.. fluids. 2-iced saline gastric
irrigation. 3-iced saline enema. 4-iced saline bladder
irrigation.

44--good hydrationgood hydration::Excess fluid intake.
) in patient receiving I.V. fluids , the
requirement is increased 10% for each degree rise of body temp.(

55--ttt the ttt the causecause

Indication of Indication of empirical antibioticsempirical antibiotics
1.1. Fever. > 105.6 FFever. > 105.6 F2.2. Immunosuppression: Immunosuppression:
)Neutropenia,asplenia,cirrhosis,()Neutropenia,asplenia,cirrhosis,(3.3. Elderly.Elderly.4.4. Unstable vital singe.Unstable vital singe.5.5. Presence of prothetic Presence of prothetic
device&foreign body.device&foreign body.6.6. Recent bite.Recent bite.7.7. Recent travel.Recent travel.

What are the feverish What are the feverish patient requirepatient require? ?
1-Plenty of fluids1-Plenty of fluids either oral or parentral to maintains either oral or parentral to maintains water and electrolyte balance.water and electrolyte balance.
2-Highly nutritious2-Highly nutritious , , easily digestible diet to face the easily digestible diet to face the increased demands of energy increased demands of energy
production and cover the needs of immuneproduction and cover the needs of immune system.system.
3-Rest,3-Rest, physical and mentalphysical and mental . .
4-Keeping the temp4-Keeping the temp.. below the lethal level.below the lethal level.
5-Quick diagnosis & proper therapy5-Quick diagnosis & proper therapy..
6-Re-assurance&6-Re-assurance& information about his illness.information about his illness.

Admission to hospital is Admission to hospital is mandatory for:mandatory for:
1-cases of suspected epidemiological importance e.g. 1-cases of suspected epidemiological importance e.g. cholera , diphtheria , SARS , (Avian,swine) Flu , RVF,,,cholera , diphtheria , SARS , (Avian,swine) Flu , RVF,,,
2-SFI with toxemia or serious focal lesion.2-SFI with toxemia or serious focal lesion.
3-All cases of prolonged fever >8days.3-All cases of prolonged fever >8days. esp. if the home care is defective.esp. if the home care is defective.
4-All cases pf FUO.4-All cases pf FUO.
5-All cases of fever in immuno-compromised pt.5-All cases of fever in immuno-compromised pt.
6-Any fever with careless family esp., in infants & 6-Any fever with careless family esp., in infants & children.children.

Thank
You