Short Bowel Syndrome Aug 20 th 2010 นพ. อธิบดี มีสิงห์ นพ....
77
Short Bowel Syndrome Aug 20 th 2010 นน.นนนนนน นน นนนนน นน.นนนนนนนนน นนนนนนนนนนนน Nutrition Topic Short Bowel Syndrome Short Bowel Syndrome Short Bowel Syndrome Short Bowel Syndrome Short Bowel Syndrome
-
Upload
phillip-payne -
Category
Documents
-
view
215 -
download
1
Transcript of Short Bowel Syndrome Aug 20 th 2010 นพ. อธิบดี มีสิงห์ นพ....

Short Bowel Syndrome
Aug 20th 2010
นพ.อธิ�บดี� มี�สิ�งห์�นพ.เอ��อพงศ์� ลิ�มีปพนาสิ�ทธิ�
Nutrition Topic
Short Bowel SyndromeShort Bowel SyndromeShort Bowel SyndromeShort Bowel SyndromeShort Bowel Syndrome

Outline
• Anatomy• Etiology• Incidence and Prevalence• Pathophysiology• Medical management• Complications• Surgical management• Pharmacologic Enhancement of Bowel adaptation• Survival And Quality of life

Oral cavity• Major glands• Salivary gland• Pancrease• Liver• Gall bladder
Alimentary canal• Esophagus• Stomach• Small intestine :Duodenum, jejunum, ileum• Large intestine : colon,caecum, rectum, anal canal
Anatomy of GI tract
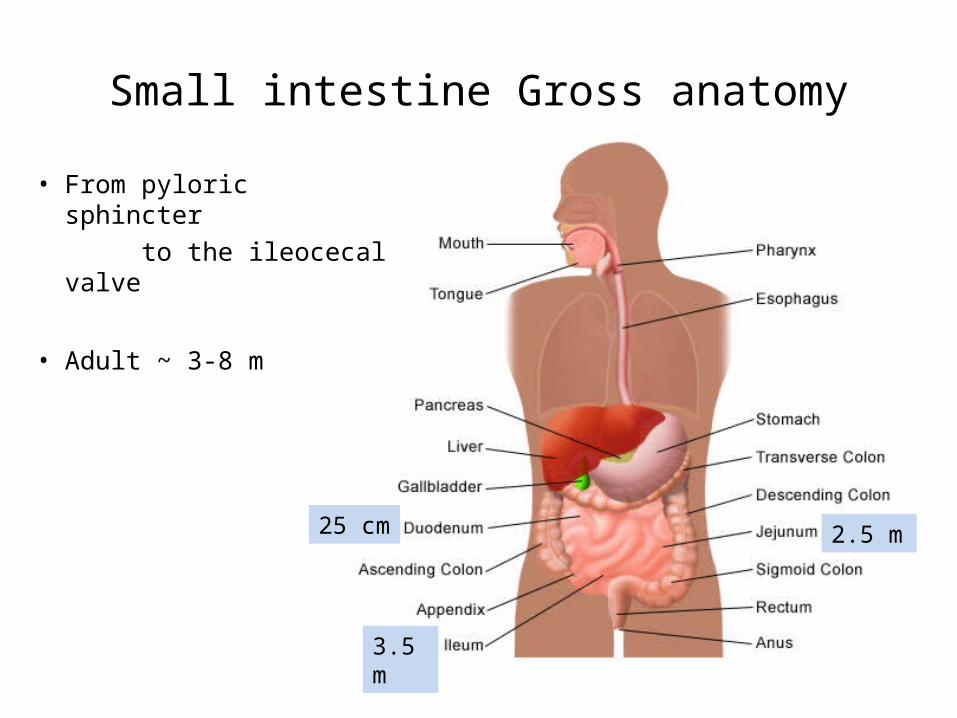
Small intestine Gross anatomy
• From pyloric sphincter
to the ileocecal valve
• Adult ~ 3-8 m
25 cm 2.5 m
3.5 m

Small intestine Microsopic anatomy
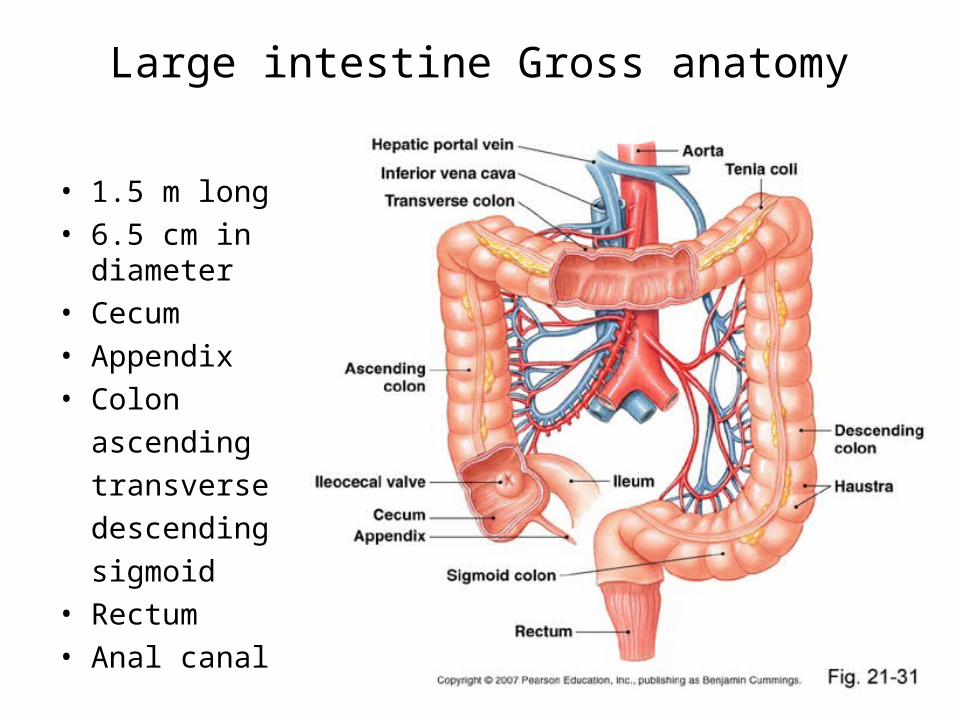
Large intestine Gross anatomy
• 1.5 m long
• 6.5 cm in diameter
• Cecum
• Appendix
• Colon
ascending
transverse
descending
sigmoid
• Rectum
• Anal canal

Large intestine Microscopic anatomy


4 basic digestive processes
• Motility
• Secretion
• Digestion
• Absorption

Motility
Pylorus → ICV 3-5 h
ICV → T.colon 8-15 h
T.Colon → sigmoid 2-3 d

Secretion


Digestion

Absorption
Site NutreintsDuodenum Calcium , magnesium ,iron , zinc
Jejunum Mono , disaccharideProteinFat-soluble vitamin A and DWater-soluble vitamin : B1,B2,B6,C,folic acid
Ileum Fat , B12 , bile salts
Colon Fluid,electrolyte



Short bowel syndrome

Back ground
• Malabsorption insufficient intestinal surface area• unable to absorb sufficient fluid, energy, or nutrients • small intestine ≤ 200 cm
Intestinal Failure
EtiologyIn Adults• Catastrophic vascular accidents
Superior mesenteric arterial embolism Superior mesenteric arterial thrombosis Superior mesenteric venous thrombosis
• Chronic intestinal pseudo-obstruction• Intestinal resection for tumor• Midgut volvulus• Multiple intestinal resections for Crohn's disease• Radiation enteritis• Refractory sprue• Scleroderma and mixed connective tissue disease • Trauma

Etiology
In Children
• Congenital villus atrophy• Extensive aganglionosis• Gastroschisis• Jejunal or ileal atresia• Necrotizing enterocolitis

INCIDENCE AND PREVALENCE
• based on multinational European data
:~ 2-4 cases/ 1 million persons per year
• ~ 50 -70 % of patients can be weaned from this therapy

PATHOPHYSIOLOGY
The degree of malabsorption
1. length of the remnant intestine
2. site-specific transport processes and endocrine cells
3. the adequacy of adaptive processes in the residual intestine

PATHOPHYSIOLOGY 3 common type of small intestine resecton & anastomosis

LOSS OF ABSORPTIVE SURFACE AREA
• Nutrient Malabsorption
Most macronutrients (carbohydrate, fat, and nitrogen) are absorbed in the proximal 100 to 150 cm of intestine
loss of part of the jejunum initially compromises nutrient absorption more than does loss of an ileal segment of similar length

LOSS OF ABSORPTIVE SURFACE AREA
• Nutrient Malabsorption
the ileum is able to compensate for jejunal loss
the jejunum is unable to compensate for ileal absorption of bile salts and vitamin B12


- inadequate mixing with biliary and pancreatic secretions
- insufficient enzymatic digestion
- nutrient maldigestion
LOSS OF ABSORPTIVE SURFACE AREA
Patients with a proximal jejunostomy
rapid gastric emptying of liquids and rapid intestinal transit
compromise the gastric phase of digestion

nutrient-enterocyte contact time
LOSS OF ABSORPTIVE SURFACE AREA
Rapid intestinal transit
segmental absorption

• Patients with a high jejunostomy are net secretors of salt and fluid
• patients excrete more fluid than ingest
• fluid management may be challenging
LOSS OF ABSORPTIVE SURFACE AREA

• Jejunum ≤ 100 cm + no colon require long-term PN
• Preservation of even some colon at surgery is highly beneficial for nutrient absorption
• malabsorbed CHO are fermented by bacterial enzymes in the colon to SCFAs absorbed and used by colonocytes
• intracolonic digestive process can generate up to 1000 kcal
LOSS OF ABSORPTIVE SURFACE AREA

LOSS OF ABSORPTIVE SURFACE AREA

Water and Electrolyte Malabsorption
fecal losses of electrolytes, water, minerals, and trace elements
At least 100 cm of intact jejunum is required to maintain positive water and electrolyte balance, similar to the length of jejunum required for nutrient absorption.
LOSS OF ABSORPTIVE SURFACE AREA

LOSS OF ABSORPTIVE SURFACE AREA
COMPONENT AMOUNT LOST
Sodium 90-100 mEq/L
Potassium 10-20 mEq/L
Calcium 772 (591-950) mg/day
Magnesium 328 (263-419) mg/day
Iron 11 (7-15) mg/day
Zinc 12 (10-14) mg/day
Copper 1.5 (0.5-2.3) mg/day
Daily Stomal or Fecal Losses of Electrolytes, Minerals, and Trace Elements in Severe Short Bowel Syndrome

Water and Electrolyte Malabsorption
• The tight junctions of the jejunum are relatively leaky compared with the tight junctions of the ileum and colon
• High NaCl concentration ≥ 90 mmol/L is required in the glucose-saline solution to achieve net sodium and water absorption
LOSS OF ABSORPTIVE SURFACE AREA

Water and Electrolyte Malabsorption
• Water transport into the enterocyte is directly proportional to Na+ transport
• Absorptive and secretory processes occur simultaneously
• A mixture of 90 to 120 mmol/L NaCl and 50 mmol/L glucose is recommended
LOSS OF ABSORPTIVE SURFACE AREA

• Electrolyte and water absorption continue in the colon
• 100 to 150 mL of water is lost in the stool / day
• The colon has a large reserve absorptive
capacity for electrolytes and water ~ 3 to 4 L of isotonic salt solution / day
LOSS OF ABSORPTIVE SURFACE AREA

Water and Electrolyte Malabsorption
• Preservation of even part of the colon can reduce fecal electrolyte and water losses significantly in patients with SBS
LOSS OF ABSORPTIVE SURFACE AREA


LOSS OF SITE-SPECIFIC TRANSPORT PROCESSES
• Nutrient absorption potentially takes place at any level of the small intestine
• the proximal-to-distal gradient in functional activity of microvillus enzymes and transporters

intact duodenum + a variable length of jejunum
or
proximal jejunostomy
LOSS OF SITE-SPECIFIC TRANSPORT PROCESSES
iron, phosphorus, or water-soluble vitamin deficiency

• The active absorption of vitamin B12 and bile acids are taken up by specific transport proteins in ileal enterocytes
• The degree of malabsorption depends on the length of resected ileum
• Vitamin B12 malabsorption usually is demonstrable when ≥ 60 cm of ileum has been resected
LOSS OF SITE-SPECIFIC TRANSPORT PROCESSES
• Resection ≤ 100 cm of ileum moderate bile acid malabsorption and bile acid loss to the colon or in stomal effluents
• loss of bile acids to the colon induces electrolyte and water secretion and can exacerbate diarrhea
LOSS OF SITE-SPECIFIC TRANSPORT PROCESSES

exceeds hepatic synthesis
ileal resections ≥ 100 cm
severe bile acid malabsorption
bile acid loss
bile acid pool size
LOSS OF SITE-SPECIFIC TRANSPORT PROCESSES
insufficient micellar solubilization of lipolytic products
steatorrhea

• extensive ileal resection fat malabsorption develops fat-soluble vitamin deficiency
• essential fatty acid (linoleic acid) deficiency is rare
• the fatty acids are hydroxylated by colonic bacteria
• hydroxylated fatty acids stimulate colonic electrolyte and water secretion
LOSS OF SITE-SPECIFIC TRANSPORT PROCESSES

LOSS OF SITE-SPECIFIC ENDOCRINE CELLS AND GASTROINTESTINAL HORMONES
proximal gastrointestinal tract endocrine cells
Gastrin, cholecystokinin (CCK), secretin, gastric inhibitory polypeptide and motilin
regulate secretory processes and motility

• hormones are synthesized usually is intact in patients with SBS
• ~ 50% of patients with extensive intestinal resections hypergastrinemia and gastric acid secretion temporarily develop in the early postoperative phase resolves spontaneously
LOSS OF SITE-SPECIFIC ENDOCRINE CELLS AND GASTROINTESTINAL HORMONES

• GLP-1 & GLP-2, neurotensin, and PYY are produced in the ileum and proximal colon
• released by intraluminal fat and carbohydrates, cause a delay in gastric emptying, and slow intestinal transit
• Patients with SBS and preserved colon have
GLP-1 & GLP-2 concentrations and demonstrate normal gastric emptying
LOSS OF SITE-SPECIFIC ENDOCRINE CELLS AND GASTROINTESTINAL HORMONES

LOSS OF THE ILEOCECAL VALVE
• The primary functions of the ileocecal valve are to separate ileal and colonic contents
• minimizing bacterial colonization of the small intestine, and to regulate emptying of ileal contents into the colon
• consequence of which intestinal transit time
and bacterial overgrowth is risked if the ileum is anastomosed to the colon
• nutrient and cobalamin malabsorption

INTESTINAL ADAPTATION TO RESECTION
• adaptive changes are more pronounced in the ileum than in the jejunum
• After jejunectomy and duodenoileal anastomosis, the ileum attains the morphologic characteristics of the jejunum, with taller villi and deeper crypts
• an increase in ileal diameter and length

INTESTINAL ADAPTATION TO RESECTION
• jejunoileal bypass operation (20 cm of jejunum anastomosed to 25 cm of ileum) showed an increase in the length and diameter of the jejunum and ileum after 18 months of observation
• In humans, these adaptive changes can take 1 to 2 years to develop fully
• Adaptive changes depend on the presence of food and biliary and pancreatic secretions

• induce these adaptive processes, patients with SBS are encouraged to start oral intake as early as possible in the postoperative phase
• SBS whose colon is in continuity demonstrate qualitative and quantitative changes in colonic flora result in
capacity to metabolize carbohydrate and in an
fecal bacterial mass
INTESTINAL ADAPTATION TO RESECTION

• the result of an increase in crypt cell production rate
• food and secretions in the intestinal lumen growth factors
• VEGF, CCK, gastrin, insulin, neurotensin, GLP-2, and
L-glutamine have been shown to stimulate intestinal growth in experimental animals
• the mediators regulating enterocyte proliferation eventually can lead to development of pharmacologic interventions
INTESTINAL ADAPTATION TO RESECTION

Short Bowel Syndrome
•Complications•Medical Management•Surgical Management•Pharmacologic enhancement of bowel adaptation•Survival & Quality of life

Complications
• Gallstone– Interruption of enterohepatic circulation
decrease hepatic bile acid secretion
bile becomes supersaturated with cholesterol
– No effective prevention

• Liver disease– In long term TPN : >50% have severe liver disease
after 5 yrs– Cholestasis, steatosis, steatohepatitis, fibrosis– Pathogenesis
• Lack of enteral feeding • Increased hepatic fat deposition • Malabsorption of Choline
– Young children greater than adult– Prevention
• avoid dextrose overfeeding(>40 kcal/kg/d) and excessive fat emulsion infusion(>1 g/kg/day)
• ursodeoxycholic acid reduce bile stasis

• Calcium oxalate kidney stone– Unabsorbed long-chain fatty acid compete
oxalate for Ca free oxalate are absorbed in colon excrete by kidney hyperoxaluria, calcium oxalate stone formation
– Rx : restrict oxalate-containing food products, oral calcium citrate

• D-lactic acidosis– Only in pt with preserved colon– Precipitate by oral intake of refined CHO
Malabsorbed CHO is metabolized by colonic bacteria SCFA lactate lower intracolonic pH promote growth of acid-resistant gr +ve anaerobes produce D-lactate Met acidosis

– S&S : nystagmus, ophthalmoplegia, ataxia, confusion, inappropriate behavior
– Lab : Met acidosis, normal lactate level, blood D-lactate level > 3 mmol/L
– Rx : sodium bicarbonate, stopping oral intake, substitution with complex carbohydrate

Medical Management
• Goals
• Initial management
• Limited ileal resection
• Extensive small intestine resection and partial colectomy
• Home parenteral nutrition

Goals
• Maintenance and/or improvement of nutritional status
• Improvement of residual bowel function (adaptation)
• Reduction of diarrhea
• Improvement in quality of life.

Initial management
• Immediate post-op– Keep fasting– Support with TPN
– H2-blocker or PPI suppress gastric hypersecretion
– Monitor BW, volume status, stomal/fecal loss of water, Na, K, Mg, Hemodynamic stability

• Late post-op– Once Hemodynamic stable, ileus resolved
Enteral tube feeding followed by Oral feeding
– Extensive resection keep fasting 5-10 days

Limited ileal resection
• Less than 100 cm resection• Can resume intake of solid food at late
post-op phase• May develop
– Secretory diarrhea (bile acid diarrhea) Rx : cholestyramine 4 g with meals
– Steatorrhea (fat malabsorption) Rx : low fat(40 g), high carbohydrate diet, and MCT can be added as fat calorie source

AGENT DOSAGE
Loperamide 4-6 mg four times daily
Diphenoxylate-atropine 2.5-5 mg four times daily
Codeine phosphate 15-30 mg two to four times daily
Tincture of opium 0.6 mL (2.5 mg) two to four times daily
Omeprazole 40 mg twice daily
Octreotide 50-100 µg SC twice daily
Clonidine 0.3 mg transcutaneous patch once weekly
Ranitidine 300 mg twice daily
Therapeutic Agents Used to Decrease Intestinal Transit and Diarrheal Volume
The antidiarrheal agents loperamide, diphenoxylate-atropine, and codeine are given 1 h before meals & hs Dosages may be increased over those recommended, because of incomplete absorption in patients with SBS

– Vit B12 malabsorption assessed with Schilling test Rx : Vit B12 1 mg IM monthly lifelong
– Malabsorption of Fat-soluble vitamin, Ca, Mg Supplement before overt signs of deficiency develop

Extensive small intestine resection and partial colectomy
• Fluid & E’lyte mangement– Gastric hypersecretion H2-blocker(iv) or
PPI(iv,po)– Rapid intestinal transit cause malabsorption &
diarrhea Anti-motility e.g. Loperamide 4 to 16 mg/day, octreotide 50-100 mg tid
– ORS Promote Na & water absorption, improve hydration & reduce TPN requirement

• ORS(WHO)– Dissolving 2.5 g of table salt + 1.5 g of KCl +
2.5 g of NaHCO3+ 1.5 g of table sugar (sucrose) in 1 L of water
– Solution provides a Na conc. ~ 90 mmol/L (salt may be added to increase the osmolarity as tolerated, to 100 to 120 mmol/L )

• Dietary management– Hyperphagia diet
• 2-3 times of BMR• up to 60 kcal/kg/day orally or tube feeding• Protein requirements 1.5–2 g/kg/day
– Encourage to eat small portions throughout the day rather than meal times

– In pt whose colon spared • High complex CHO diet (starch, nonstarch-
polysaccharide, soluble fiber)
colonic bacteria will ferment into SCFA (75 mmol/10g of unabsorbed CHO) energy
• MCT(C8-C10, 8.3 kcal/g) : absorbed in colon, supplement with MCT lead to increased energy absorption

– Fat maldigestion from bile acid malabsorption• Synthetic conjugated bile acid (cholylsarcosine)• Cholestyramine
– Low fat diet : limited data
– Vit B12 , Fat-soluble vitamin deficiency (except Vit K), Zinc, Selenium deficiency

COLON PRESENT COLON ABSENT
Carbohydrate
Complex carbohydrates/starches Variable types
30-35 kcal/kg/day 30-35 kcal/kg/day
Soluble fiber
Fat
MCT/LCT LCT
20%-30% of caloric intake 20%-30% of caloric intake
Protein
Intact protein Intact protein
1.0-1.5 g/kg/day 1.0-1.5 g/kg/day
Macronutrient Requirements in Patients with Short Bowel Syndrome

MICRONUTRIENT REQUIREMENT
Vitamin A 10,000-50,000 units daily
Vitamin B121000 uq subcutaneously monthly for patients with terminal ileal
resection or disease
Vitamin C 200 mg daily
Vitamin D 50,000 units 1,25(OH2)-D3 twice weekly to twice daily
Vitamin E 30 International Units daily
Vitamin K 10 mg weekly
Calcium 1000-1500 mg daily
Magnesium See text
Iron As needed
Selenium 60-150 ug dailly
Zinc 220-440 mg daily (sulfate or gluconate form)
Bicarbonate As needed

Home parenteral nutrition
• For pt who requires long term TPN– Inadequate EN– Problem with water or e’lyte
• Compress TPN infusion over 10-12 hr period, typically overnight
• Infused into central line e.g. SVC or IVC• Instruct pt about catheter care and
dressing change, TPN & catheter related complication

Surgical Management
• Intestinal lengthening procedures– Reanastomosis of residual small bowel to residual
colon– Tapering enteroplasty– Construction of intestinal valve
• Intestinal transplantation– Indication
• TPN dependent with complicated by progressive liver diseases
• Significant fluid losses and dehydration despite appropriate medical management

Pharmacologic enhancement of bowel adaptation
• L-glutamine failed to show any benefical effect on absorption
• GLP-2 increase in several absorptive parameters, BW, mucosal growth
• Growth hormone reduced TPN requirement, FDA approve

Survival & Quality of life
• Limited small bowel resection excellent prognosis
• Remnant bowel length < 100 cm predictive for lifelong TPN dependence
• Poor survivial– High jejunostomy– Small bowel length < 50 cm– Mesenteric infarction as a cause for intestinal
resection

Thank You