Pituitary Tumors 2005

of 20
Transcript of Pituitary Tumors 2005
-
7/31/2019 Pituitary Tumors 2005
1/20
F O C U S I N G O N T U M O R S
Pituitary Tumors
-
7/31/2019 Pituitary Tumors 2005
2/20
A Word About ABTAFounded in 1973, the not-for-profit AmericanBrain Tumor Association has a proud historyof funding research, providing patient services,and educating people about brain tumors. Ourmission is to eliminate brain tumors throughresearch and to meet the needs of brain tumorpatients and their families.
We gratefully acknowledge John A. Jane, Jr., MD,Assistant Professor of Neurological Surgery,Department of Neurosurgery, University of VirginiaHealth Sciences Center, Charlottesville for hisassistance in writing this publication. We also thankEdward R. Laws, Jr., MD and Dawn H. Mitchell,PhD, for the original editions of this publication.
This publication was made possible throughthe generosity of Compass Bank, the InterlakeFoundation, Beverly McHugh Grant, and
June M. Thomas.
ISBN 0-944093-72-8
COPYRIGHT 2002, 2006 ABTA
REPRODUCTION WITHOUT PRIOR WRITTEN PERMISS ION IS PROHIB ITED.
-
7/31/2019 Pituitary Tumors 2005
3/20
| 1PITUITARY TUMORS
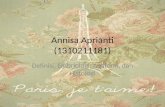
IntroductionThe pituitary gland is a bean-sized organ located
in the midline at the base of the brain just behindthe bridge of the nose in a bony pouch called thesella turcica.
The pituitary is known as the master glandbecause it helps to control the secretion of hormonesfrom a number of other glands and organs in thebody including the thyroid, the adrenals, testes,and ovaries. The pituitary gland releases hormonesinto the blood stream, where they are carried todistant glands or organs in the body. Those distantglands release other hormones which, in turn, feed
back to the brain through the bloodstream. Onceback in the brain,hormones cause the hypothalamus(a part of the brain near the pituitary) to signal thepituitary gland to secrete more hormones or slowdown hormone production, depending on theneeds of the body. A stem-like stalk connects thepituitary gland to the hypothalamus and it isthrough this stalk that the hypothalamus sendssignals to control the activity of the pituitary gland.
The medical term for pituitary tumors is pituitaryadenoma adeno means gland, oma means
tumor. Most pituitary adenomas develop in thefront two-thirds of the pituitary gland. That area iscalled the adenohypophysis, or the anterior pituitary.Pituitary tumors rarely develop in the rear one-thirdof the pituitary gland, called the neurohypophysisor the posterior pituitary. They are almost always
T H E P I T U I T A R Y G L A N D
H Y P O T H A L A M U S
S E L L A T U R C I C A
P I T U I T A R Y S T A L K
O P T I C C H I A S M
P I T U I T A R Y G L A N D
-
7/31/2019 Pituitary Tumors 2005
4/20
PITUITARY TUMORS2 |
benign and are very treatable. Some tumors can betreated effectively with medications while othersrequire surgery. Because the pituitary gland isimportant in the function of other glands in thebody, treating a pituitary tumor requires an activemulti-disciplinary health care approach, support,and follow-up.
IncidencePituitary tumors account for 715% of all primarybrain tumors,making them the third most commonprimary brain tumor in adults following menin-giomas and the gliomas. Abnormalities includingsmall tumors and benign cysts within the pituitaryare quite common. Although exact statistics arenot yet available on these tumors (registries onlyrecently began counting pituitary tumors in theirdata) it is estimated that 2025% of the general
population may have small, symptomless pituitarytumors. It appears that 10% of the general popu-lation will have an abnormality big enough to seeon magnetic resonance imaging (MRI). Thoseabnormalities most often do not cause symptomsand do not require medical or surgical therapy.
L A T E R A L V I E W O F T H E B R A I N
H Y P O T H A L A M U S
S P H E N O I DB O N E
P I T U I T A R Y G L A N D
S P H E N O I DS I N U S
T H I R D V E N T R I C L E
-
7/31/2019 Pituitary Tumors 2005
5/20
| 3PITUITARY TUMORS
Pituitary tumors can be found in every age group,but their incidence increases with age up to age 74,at which it seems to peak. Functioning (also called
secreting) tumors tend to occur in younger adults.Non-functioning (non-secreting) tumors tend tooccur in older adults. Women are diagnosed withpituitary tumors slightly more often than men.This may be due to the tumors interference withthe female menstrual cycle,which sometimes makessymptoms more obvious.
CausesPituitary tumors, similar to tumors locatedelsewhere in the body, develop from one single
abnormal cell that multiplies into many abnormalcells, eventually forming a tumor. Stimulationfrom the hypothalamus may also contribute totumor growth. If your doctor determines youhave a tumor, the next step is learning the typeof pituitary tumor.
Types of TumorsPituitary tumors may be classified and named by:
the hormones they secrete, if any
their size
the appearance of the tumor cells under amicroscope
H O R M O N E S
Some pituitary tumors inappropriately secreteexcessive amounts of a particular hormone. Theseare known by several names including functioningadenomas, hormonally active adenomas, andsecretory adenomas.Functioning or secretingtumors may cause the pituitary gland to ignore thesignals from the hypothalamus, allowing thepituitary gland to secrete excessive amounts ofhormones such as prolactin (PRL), growth hormone(GH), adrenocorticotropic hormone (ACTH), orthyroid-stimulating hormone (TSH). Sometimesthese tumors secrete more than one type of hormone.Other pituitary tumors do not oversecrete any active
-
7/31/2019 Pituitary Tumors 2005
6/20
PITUITARY TUMORS4 |
hormone and may even cause a slow down or astoppage in hormone production (a condition calledhypopituitarism). These tumors are commonly
called nonfunctioning adenomas(NFAs). Otherdoctors refer to these tumors as hormonallyinactive or non-secretory adenomas.
S I Z E
Pituitary tumors are also classified by their size.Tumors appearing to be less than 10 mm (about3/4) on a scan are called microadenomas. Thoselarger than 10 mm are called macroadenomas.
M I C R O S C O P I C A P P E A R A N C E
If your tumor is surgically removed, it will be sent toa pathologista doctor specially trained to look attumor cells using a microscope. The pathologist willexamine the sample of tumor tissue,and provide areport to your doctor. The pathology report
describes the hormone content, structure, and thecells that gave rise to your tumor. It takes about aweek for your doctor to receive the surgical pathologyreport. All of this information is then used todetermine your tumor type, form a treatment plan,and predict the possible future activity of the tumor.
E N D O C R I N E G L A N D S
P I T U I T A R Y
T E S T E S ( M A L E )
A D R E N A L S
T H Y R O I DP A R A T H Y R O I D S
O V A R I E S ( F E M A L E )
P A N C R E A S
-
7/31/2019 Pituitary Tumors 2005
7/20
-
7/31/2019 Pituitary Tumors 2005
8/20
PITUITARY TUMORS6 |
abdomen may be necessary to verify that thehormone imbalances are caused by the pituitarygland. An ophthalmologist - a doctor specializingin visual problems - may examine your eyes ifthe tumor affects your eyesight.
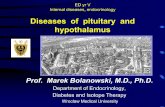
Sometimes, pituitary tumors are found incidentally.This usually means the tumor was seen on an MRIscan ordered for another, unassociated medicalreason such as a sports-related accident. Thesesymptomless tumors require careful evaluation,but may not always need immediate treatment.
M R I O F A P I T U I T A R Y A D E N O M A
MRI courtesy of Dr. Laws
T U M O R
ACTH Controls the production of 9 to 52 pg/mladrenocorticotropic cortisol a natural steroid
hormone needed to control bloodpressure, sugar and salt levels
GH Conrtos bone growth; 0 to 3 ng/mlgrowth hormone height; body proportion
in the extremities and jaw
PRL Controls milk production in Males andprolactin women, impacts sex drive non-pregnant
and sperm counts in men women:0 to 20 ng/ml
In pregnancy:10 to 300 ng/ml
TSH Controls thyroid functions 0.2 to 4.7 mcU/mlthyroid stimulating such as metabolism,hormone heart rate and appetite
Hormone Responsible forNormal BloodLevels in Adults
-
7/31/2019 Pituitary Tumors 2005
9/20
| 7PITUITARY TUMORS
Specific TumorsP R O L A C T I N O M A S , O R
P R O L A C T I N - P R O D U C I N G A D E N O M A S
Prolactinomas represent about 30-40% of allpituitary tumors, making them the most commonof these tumors. Prolactinomas are most oftenfound in women of childbearing age. In men,prolactinomas are more frequent in the fourth andfifth decade of life. About half of these tumors aremicroadenomas, which are small tumors.
In women, high prolactin levels may causemenstruation to stop (amenorrhea) or inappropriateproduction of breast milk (galactorrhea) may
develop. In men, prolactin-secreting tumorsmay cause a decreased sex drive and impotence.Men also tend to develop larger tumors whichmay cause headaches or vision problems.
G R O W T H H O R M O N E - P R O D U C I N GA D E N O M A S
These tumors represent about 20% of the pituitaryadenomas. Growth-hormone producing tumorsare more common in men than in women. Oftenmacroadenomas, these tumors may extend towardthe cavernous sinus, an area of the brain located
next to the pituitary. Mixed prolactin and growthhormone-secreting tumors are not uncommon.
Growth hormone-secreting tumors may causegigantism in children and adolescents. In adultswho have reached their full height, the hands, feet,and lower jaw become enlarged. This is calledacromegaly. Excessive growth hormone canaggravate other medical conditions such asdiabetes mellitus, hypertension, and heart disease.
A C T H - P R O D U C I N G A D E N O M A S
These tumors represent about 14% of the pituitaryadenomas. They are much more common inwomen than in men. ACTH (adrenocorticotropichormone) stimulates the adrenal gland to makeand secrete glucocorticoids, which are naturalsteroids. Excess glucocorticoids cause Cushing's
-
7/31/2019 Pituitary Tumors 2005
10/20
PITUITARY TUMORS8 |
disease. Some of the symptoms of Cushing'sdisease are a moon-shaped face, excess hair growthon the body, bruising, menstrual irregularities,
and high blood pressure.O T H E R H Y P E R S E C R E T I N GP I T U I T A R Y A D E N O M A S
This group represents less than 1% of pituitaryadenomas. Some of these tumors excreteincreased amounts of thyrotropin (thyroidstimulating hormone). Others may secrete folliclestimulating hormone/luteinizing hormone(which controls the ovaries and testes) or alphasubunit (a glycoprotein hormone).
N O N - S E C R E T I N G T U M O R SAlso called non-functioning tumors, theserepresent about 25% of the pituitary adenomas.Null cell adenomas, oncocytomas,silent corticotrophadenomas, and gonadotroph adenomas fall into thisgroup. These tumors grow slowly and generallycause minimal symptoms. They may be sizablebefore their presence is suspected. When theyexpand outside the sella turcica, they may presson the nearby optic nerves causing vision loss andheadache. Such tumors can also compress thepituitary gland itself so it cannot produce its normaloutput of hormones. Called hypopituitarism, thissymptom is associated with general weakness andfatigue, a pale complexion, loss of sexual functionand apathy.
P I T U I T A R Y C A R C I N O M A
Cancers, or true malignancies of the tissue of thepituitary gland, are very rare. Instead, a pituitarycarcinoma is usually defined as a tumor thatbegan in the pituitary gland then metastasized,or spread, within the brain or outside the central
nervous system. These tumors are generallymacroadenomas which are resistant to therapy,recur locally several times, then metastasize tothe spinal canal or other organs of the body.The majority of pituitary carcinomas are functionaltumors, secreting prolactin or ACTH.
-
7/31/2019 Pituitary Tumors 2005
11/20
| 9PITUITARY TUMORS
TreatmentTreatment of a pituitary tumor depends on the
hormonal activity of the tumor, the size andlocation of the tumor, as well as the age andoverall health of the person with the tumor.The goals of treatment may be to remove thetumor, to reduce or control tumor size, and/orto re-balance hormone levels.
S U R G E R Y
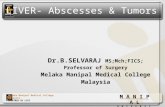
If your doctor recommends surgery, the goalwill be to remove as much tumor as possible.A transsphenoidal approach literally meaningacross the sphenoid bone is the most common.
During this surgery, extremely small instrumentsand microscopes are used to remove the tumorfrom within the nose (endonasal) or under the lipand above the teeth (sublabial). Less often, acraniotomy may be done, during which a portionof the skull bone is temporarily removed to gainaccess to the pituitary gland. Some surgeons usean endoscope, a long, thin tube-like instrument,to reach the tumor.
Transsphenoidal approach: To the left is a profile viewin the midline. The nasal speculum (only half seen) is
placed inside the nose up to the level of the sphenoidsinus and points toward the tumor. The bone in frontof the sphenoid sinus must be removed as well as thebone overlying the tumor. To the right are two com-mon incisions made within the nose. The incisionscannot be seen and no incision is made on the face.
Diagram courtesy of Dr. Jane.
Sphenoidsinus
2001UVA Nsgy
-
7/31/2019 Pituitary Tumors 2005
12/20
PITUITARY TUMORS10 |
Your neurosurgeon will speak with you about thesurgery planned for your tumor, the risks andbenefits of the procedure, and your follow-up
care. We offer a free publication, titled Surgery,which explains in detail the different surgical toolsavailable, how procedures are planned, andquestions to ask your physician about the procedurerecommended for you. If you would like a copy,please call us at 800-886-2282.
R A D I A T I O N T H E R A P Y O R R A D I O S U R G E R Y
Radiation therapy is often used as a second, oradjuvant, treatment for pituitary tumors. It may begiven in addition to surgery and/or drug therapy.Radiation therapy may be used to treat tumors that
have re-grown, or it may be used for aggressivetumors. The goal of radiation therapy for pituitarytumors is to reduce or control tumor size; however,it may take several months or longer before theeffects of this treatment cause a change in yourhormone levels or your MRI scan.There are severaldifferent types of radiation therapy; your doctorwill decide which is best for your tumor.Conventional external beam radiation is stan-dard radiation given 5 days a week for 5 or 6weeks. Stereotactic radiosurgery is focusedradiation therapy.
The Gamma Knife, LINAC (modified linearaccelerators), CyberKnife, and proton beamradiation are all forms of stereotactic radiosurgery.Conformal photon radiation, also known asintensity-modulated radiation therapy, shapesradiation beams to the contours of the tumor.Intracavitary and interstitial radiation place theradioactive source directly into the tumor duringsurgery. If your doctor thinks your tumor wouldbe best treated with radiation, he/she can speakwith you about the type of therapy suggested andthe effects of that particular treatment.
-
7/31/2019 Pituitary Tumors 2005
13/20
| 11PITUITARY TUMORS
D R U G T H E R A P Y
There are several drugs used to treat pituitarytumors. The drug chosen will depend on the
hormone functions of the tumor.
Dopamine agonists, such as bromocriptine(Parlodel),pergolide (Permax), or cabergoline(Dostinex), are used to control the production ofprolactin.The drugs reduce tumor size by reducingthe amount of prolactin made by the pituitarygland. Most people with prolactin-secreting tumorsrequire long term therapy to control the size of theirtumor; generally, if the medication is stopped prolactinlevels begin to increase. In a small percent of peoplewith very small tumors, treatment may be stopped
after a year or so to see if the tumor re-grows.Those with very high prolactin levels may find thatdrug therapy decreases their hormone levels butdoes not relieve all of their symptoms. In thesesituations, the drug successfully lowers the prolactinlevel but the level may still be higher than normal,thus causing symptoms.
Somatostatin analogues such as octreotide(Sandostatin or Sandostatin LAR), are used toboth reduce growth hormone levels and relievethe associated symptoms. These drugs may also
be used to control the production of thyroidstimulating hormone in thyrotrophic tumors.Dopamine agonists, such as those listed above, aregiven to treat growth-hormone secreting tumorsbut their effect is primarily relief of symptomsrather than reduction of hormone levels. Newdrugs are being tested in research studies calledclinical trials; information about those trials can befound through your endocrinologist.
Ketoconazole (Nizoral) is used to treat ACTHsecreting tumors that produce Cushings disease.
This drug lowers cortisol (natural steroid)production, but generally does not reduce thesize of the tumor.
-
7/31/2019 Pituitary Tumors 2005
14/20
PITUITARY TUMORS12 |
FollowupOnce you begin treatment, your doctors will
determine a schedule for follow-up MRI scansand endocrine testing. These are used to monitorthe effectiveness of therapy and watch for possibletumor re-growth.
Many people with functioning pituitary tumorsare followed by an endocrinologist - a physicianspecially trained in the treatment of disorders ofthe hormone-producing glands. Hormone imbal-ances can be caused by the tumor itself, or mayresult from the treatment necessary to control thetumor. The endocrinologist will monitor your
hormone blood levels, outline a treatment plan,and make drug adjustments when needed. Theendocrinologist becomes an active member ofyour healthcare team, working closely with yourneurosurgeon and your primary care physician.
Although pituitary tumors are almost alwaysbenign, they can recur, and therefore periodicfollowup MRI scans are necessary. Your doctorwill tell you how often those scans should be done.If you do not know when your next MRI shouldbe scheduled, call your doctors office to ask.
-
7/31/2019 Pituitary Tumors 2005
15/20
| 13PITUITARY TUMORS
A Next StepSupport groups and pen-pal programs allow
you to share experiences with others who haveexperienced a pituitary tumor. Internet resources,such as online chat rooms and e-mail groups, canbe of benefit to those who do not have access to alocal support group. Social workers can help youfind these support networks. Nurses will provideyou with information about how to monitor yourhealth, especially when your treatment planinvolves hormone therapies. Dieticians, workingalong with your endocrinologist, can design ahealthy eating plan to ensure your body receivesbalanced nutrients. We can help you locate these
resources in your area.
Our web sitewww.abta.orgoffers extensivebrain tumor information, treatment and researchupdates, and patient/family stories. The thread thatruns through each of our services and programs ishope. Become involved join us in some way, tomake sure there is a cure, and ultimately, a wayto prevent brain tumors.
We hope that the information in this pamphlethelps you communicate better with the people who
are caring for you. Our purpose is not to provideanswers; rather, we encourage you to ask questions.
-
7/31/2019 Pituitary Tumors 2005
16/20
PITUITARY TUMORS14 |
Questions I Want to Ask
-
7/31/2019 Pituitary Tumors 2005
17/20
| 15PITUITARY TUMORS
Questions I Want to Ask
-
7/31/2019 Pituitary Tumors 2005
18/20
PITUITARY TUMORS16 |
Questions I Want to Ask
-
7/31/2019 Pituitary Tumors 2005
19/20
Publications & Services
B U I L D I N G K N O W L E D G E
Dictionary for Brain Tumor PatientsLiving with a Brain TumorA Primer of Brain Tumors
F O C U S I N G O N T U M O R S
EpendymomaGlioblastoma Multiforme and Anaplastic AstrocytomaMedulloblastomaMeningiomaMetastatic Brain TumorsOligodendroglioma and OligoastrocytomaPituitary Tumors
F O C U S I N G O N T R E A T M E N T
ChemotherapyConventional Radiation TherapyStereotactic RadiosurgerySteroidsSurgeryPhysician Resource List: Physicians Offering Clinical Trials for
Brain Tumors
F O R & A B O U T C H I L D R E N
Alexs Journey: The Story of a Child with a Brain Tumor (Video or DVD)Education Packet (Parent or Teacher)When Your Child Returns to School
S U P P O R T R E S O U R C E S
BibliographyCare OptionsEmergency Alert Wallet CardsEmployment InformationEnd-of-Life CareFinancial Aid ResourcesHealth Insurance ResourcesHousing During Treatment ResourcesNet-Working LinksNeuropsychology ResourcesScholarship & Educational Financial Aid ResourcesSocial Security Disability ResourcesSpanish-Language ResourcesTransportation Assistance Resources
Wig and Head Covering ResourcesWish Fulfillment Resources
N E W S L E T T E R
ABTA Brain Tumor E-NewsMessageline Newsletter
F O C U S I N G O N S U P P O R T
Listing of Brain Tumor Support GroupsListing of Bereavement (Grief) Support GroupsOrganizing and Facilitating Support GroupsPen Pal ProgramsConnections (program for patients and family members)Bridges (program for those who have lost someone to a brain tumor)Resources for Online SupportTLC (Tips for Living and Coping) e-bulletin
Single copies of our publications are available free of charge.
River Road, Suite Des Plaines, Illinois
.. TEL [email protected] EMAIL.. FAX www.abta.org WEB
-
7/31/2019 Pituitary Tumors 2005
20/20
Sharing knowledge. Sharing hope.
River Road, Suite Des Plaines, Illinois
.. TEL [email protected] EMAIL.. FAX www.abta.org WEB