Ncp Proper 1
5
NURSING CARE PLAN PROPER 1 Problem 1: Nursing Diagnosis: Impaired Gas Exchange related to immaturity of the lungs secondary to premature t/c hyaline membrane disease Goal: After all nursing interventions, the patient will be able to breathe normally without any devices such as oxygen therapy, incubator and being stimulated, and injecting surfactants Objective: After a week of nursing interventions, the patient will be able to manifest signs and symptoms of improvement of normal breathing continuously by a. Reduce s ufferin g of RDS, wit h reduces wor k of br eathing b. Maintain periodi c breath ing patt ern and norma l vital s igns c. Mai ntai n PaO2 an d PaCO2 leve ls wit hin norma l d. Leadin g to n ormal laborat ory or diagnos tic stu dies CUES EXPLANATION Subjective: Objectives: On incubator On oxygen therapy @ 1 lpm With D5 IMD x 7-8mgtts Afebrile Apgar score of 6-7 @1.5 min With a current weight of 1.2 kg Current VS: RR-32; CR-128; T-36.8C Temperature fluctuates easily With slight clammy pale extremities Abnormal breathing pattern with episodes of apnea Lies in an extended position Low muscle tone and activity Thin and less body fat A premature baby, or preemie, is born before the 37th week of pregnancy. Premature birth occurs in between 8 percent to 10 percent of all pregnancies in the United States. Because they are born too early, preemies weigh much less than full-term babies. They may have health problems because their organs did not have enough time to develop. Preemies need special medical care in a neonatal intensive care unit, or NICU. They stay there until their organ systems can work on their own. Respiratory distress syndrome (RDS) is a breathing disorder that affects newborns. RDS is more common in premature infants because their lungs aren't able to make enough surfactant. Surfactant is a liquid that coats the inside of the lungs. It helps keep them open so that infants can breathe in air once they're born. Without surfactant, the lungs collapse and the infant has to work hard to breathe. He or she might not be able to breathe in enough oxygen to support the body's organs.
-
Upload
noreen-pineda -
Category
Documents
-
view
242 -
download
0
Transcript of Ncp Proper 1

8/3/2019 Ncp Proper 1
http://slidepdf.com/reader/full/ncp-proper-1 1/6
NURSING CARE PLAN PROPER 1
Problem 1:
Nursing Diagnosis: Impaired Gas Exchange related to immaturity of the lungs secondary to premature t/c hyaline membrane disease
Goal: After all nursing interventions, the patient will be able to breathe normally without any devices such as oxygen therapy, incubator and being stimulated, and injecting surfactants
Objective: After a week of nursing interventions, the patient will be able to manifest signs and symptoms of improvement of normal breathing continuously by
a. Reduce suffering of RDS, with reduces work of breathing
b. Maintain periodic breathing pattern and normal vital signs
c. Maintain PaO2 and PaCO2 levels within normal
d. Leading to normal laboratory or diagnostic studies
CUES EXPLANATION
Subjective:
Objectives:
On incubator
On oxygen therapy @ 1 lpm
With D5 IMD x 7-8mgtts
Afebrile
Apgar score of 6-7 @1.5 min
With a current weight of 1.2 kg
Current VS: RR-32; CR-128; T-36.8C
Temperature fluctuates easily With slight clammy pale extremities
Abnormal breathing pattern with episodes of
apnea
Lies in an extended position
Low muscle tone and activity
Thin and less body fat
A premature baby, or preemie, is born before the 37th
week of pregnancy. Premature birth occurs in between 8
percent to 10 percent of all pregnancies in the United
States. Because they are born too early, preemies weigh
much less than full-term babies. They may have health
problems because their organs did not have enough time
to develop. Preemies need special medical care in a
neonatal intensive care unit, or NICU. They stay there
until their organ systems can work on their own.
Respiratory distress syndrome (RDS) is a breathing
disorder that affects newborns. RDS is more common in
premature infants because their lungs aren't able to make
enough surfactant. Surfactant is a liquid that coats the
inside of the lungs. It helps keep them open so that
infants can breathe in air once they're born.
Without surfactant, the lungs collapse and the infant has
to work hard to breathe. He or she might not be able to
breathe in enough oxygen to support the body's organs.
8/3/2019 Ncp Proper 1
http://slidepdf.com/reader/full/ncp-proper-1 2/6
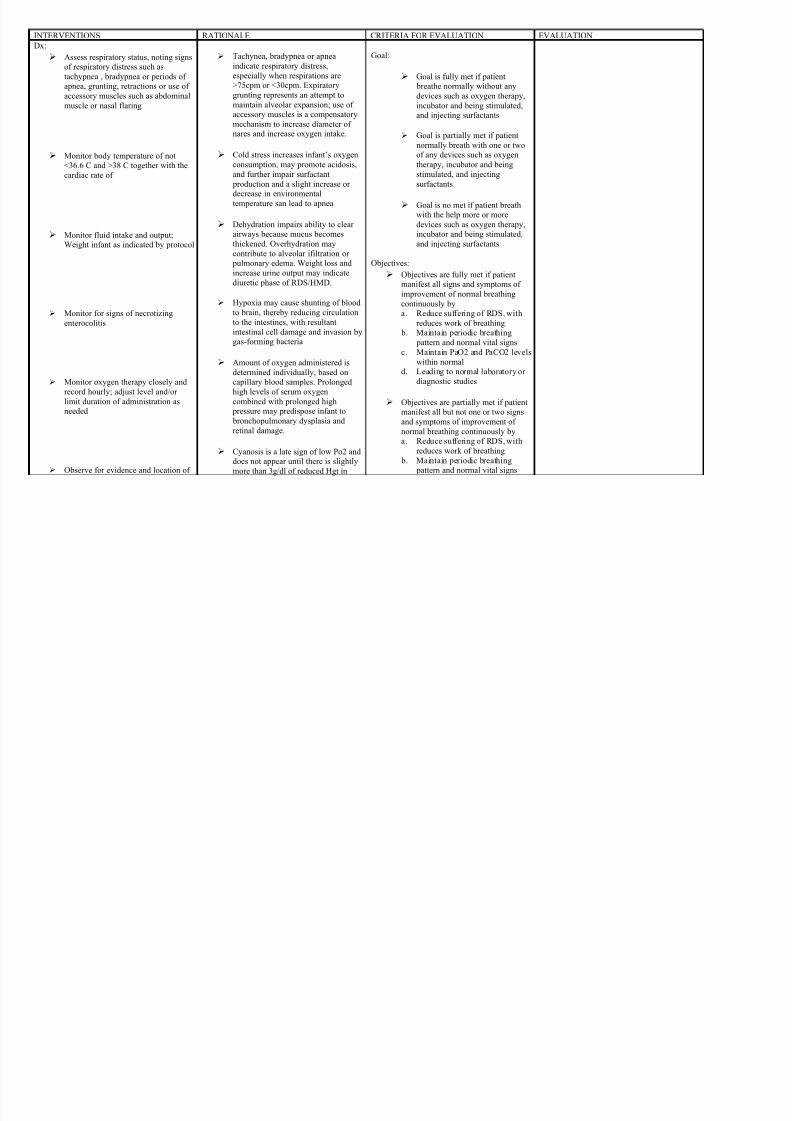
INTERVENTIONS RATIONALE CRITERIA FOR EVALUATION EVALUATION
Dx:
Assess respiratory status, noting signs
of respiratory distress such as
tachypnea , bradypnea or periods of
apnea, grunting, retractions or use of
accessory muscles such as abdominal
muscle or nasal flaring
Monitor body temperature of not
<36.6 C and >38 C together with the
cardiac rate of
Monitor fluid intake and output;
Weight infant as indicated by protocol
Monitor for signs of necrotizing
enterocolitis
Monitor oxygen therapy closely and
record hourly; adjust level and/or
limit duration of administration as
needed
Observe for evidence and location of
Tachynea, bradypnea or apnea
indicate respiratory distress,
especially when respirations are
>75cpm or <30cpm. Expiratory
grunting represents an attempt to
maintain alveolar expansion; use of
accessory muscles is a compensatory
mechanism to increase diameter of
nares and increase oxygen intake.
Cold stress increases infant’s oxygen
consumption, may promote acidosis,
and further impair surfactant
production and a slight increase or
decrease in environmental
temperature san lead to apnea
Dehydration impairs ability to clear
airways because mucus becomes
thickened. Overhydration may
contribute to alveolar ifiltration or
pulmonary edema. Weight loss and
increase urine output may indicatediuretic phase of RDS/HMD.
Hypoxia may cause shunting of blood
to brain, thereby reducing circulation
to the intestines, with resultant
intestinal cell damage and invasion by
gas-forming bacteria
Amount of oxygen administered is
determined individually, based on
capillary blood samples. Prolonged
high levels of serum oxygen
combined with prolonged high
pressure may predispose infant to bronchopulmonary dysplasia and
retinal damage.
Cyanosis is a late sign of low Po2 and
does not appear until there is slightly
more than 3g/dl of reduced Hgt in
Goal:
Goal is fully met if patient
breathe normally without any
devices such as oxygen therapy,
incubator and being stimulated,
and injecting surfactants
Goal is partially met if patientnormally breath with one or two
of any devices such as oxygen
therapy, incubator and being
stimulated, and injecting
surfactants
Goal is no met if patient breath
with the help more or more
devices such as oxygen therapy,
incubator and being stimulated,
and injecting surfactants
Objectives:
Objectives are fully met if patientmanifest all signs and symptoms of
improvement of normal breathing
continuously by
a. Reduce suffering of RDS, with
reduces work of breathing
b. Maintain periodic breathing
pattern and normal vital signs
c. Maintain PaO2 and PaCO2 levels
within normal
d. Leading to normal laboratory or
diagnostic studies
Objectives are partially met if patient
manifest all but not one or two signsand symptoms of improvement of
normal breathing continuously by
a. Reduce suffering of RDS, with
reduces work of breathing
b. Maintain periodic breathing
pattern and normal vital signs
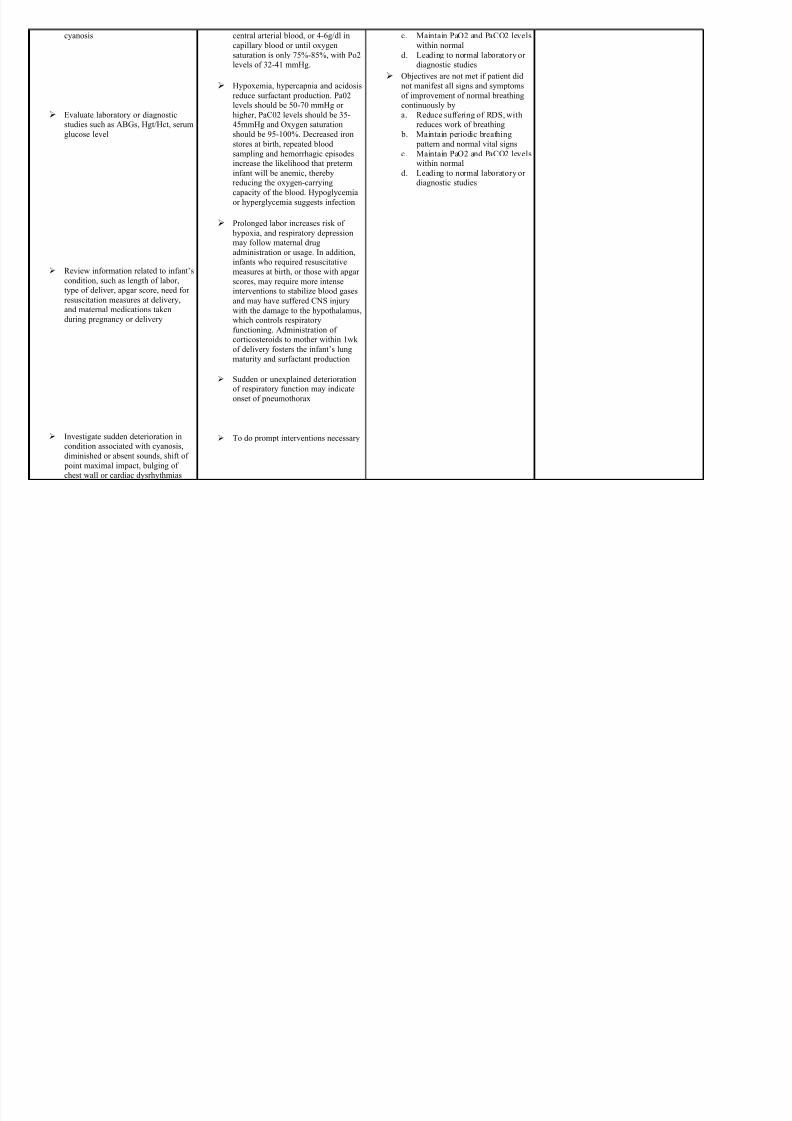
8/3/2019 Ncp Proper 1
http://slidepdf.com/reader/full/ncp-proper-1 3/6
cyanosis
Evaluate laboratory or diagnostic
studies such as ABGs, Hgt/Hct, serum
glucose level
Review information related to infant’s
condition, such as length of labor,
type of deliver, apgar score, need for
resuscitation measures at delivery,
and maternal medications taken
during pregnancy or delivery
Investigate sudden deterioration in
condition associated with cyanosis,
diminished or absent sounds, shift of
point maximal impact, bulging of
chest wall or cardiac dysrhythmias
central arterial blood, or 4-6g/dl in
capillary blood or until oxygen
saturation is only 75%-85%, with Po2
levels of 32-41 mmHg.
Hypoxemia, hypercapnia and acidosis
reduce surfactant production. Pa02
levels should be 50-70 mmHg or
higher, PaC02 levels should be 35-
45mmHg and Oxygen saturation
should be 95-100%. Decreased ironstores at birth, repeated blood
sampling and hemorrhagic episodes
increase the likelihood that preterm
infant will be anemic, thereby
reducing the oxygen-carrying
capacity of the blood. Hypoglycemia
or hyperglycemia suggests infection
Prolonged labor increases risk of
hypoxia, and respiratory depression
may follow maternal drug
administration or usage. In addition,
infants who required resuscitative
measures at birth, or those with apgar
scores, may require more intense
interventions to stabilize blood gases
and may have suffered CNS injury
with the damage to the hypothalamus,
which controls respiratory
functioning. Administration of
corticosteroids to mother within 1wk
of delivery fosters the infant’s lung
maturity and surfactant production
Sudden or unexplained deterioration
of respiratory function may indicate
onset of pneumothorax
To do prompt interventions necessary
c. Maintain PaO2 and PaCO2 levels
within normal
d. Leading to normal laboratory or
diagnostic studies
Objectives are not met if patient did
not manifest all signs and symptoms
of improvement of normal breathing
continuously by
a. Reduce suffering of RDS, with
reduces work of breathing
b. Maintain periodic breathing pattern and normal vital signs
c. Maintain PaO2 and PaCO2 levels
within normal
d. Leading to normal laboratory or
diagnostic studies
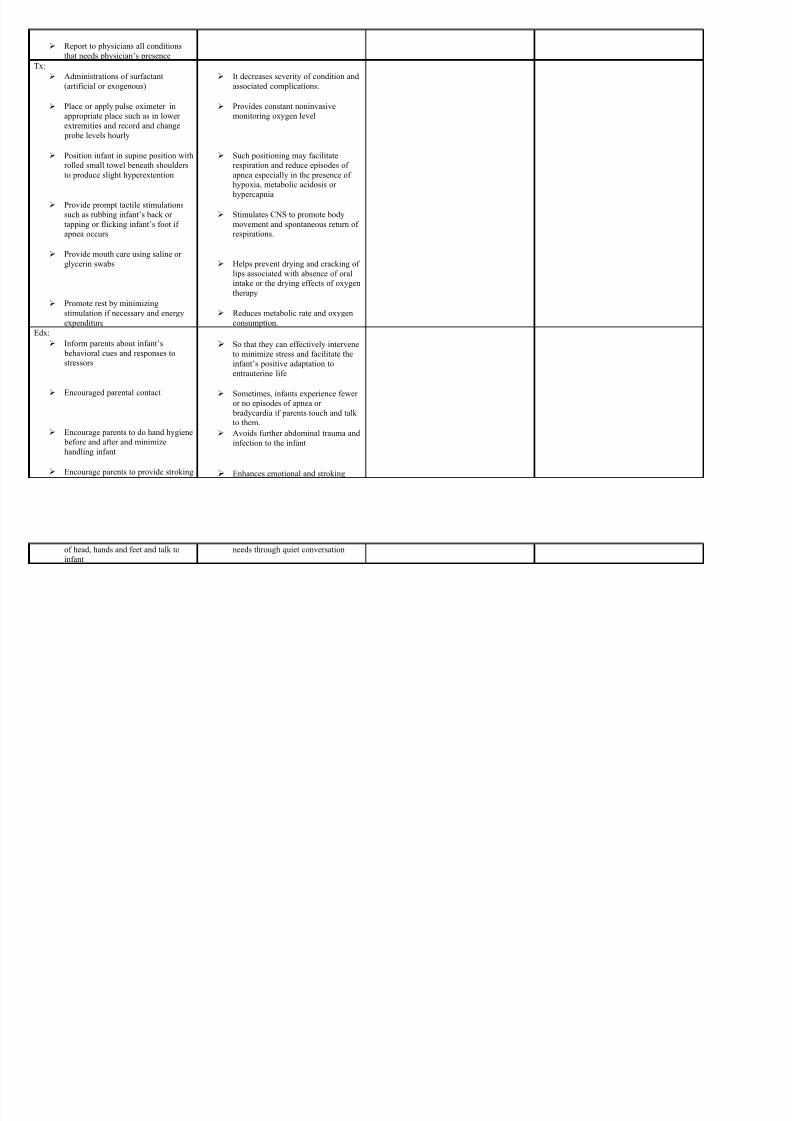
8/3/2019 Ncp Proper 1
http://slidepdf.com/reader/full/ncp-proper-1 4/6
Report to physicians all conditions
that needs physician’s presence
Tx:
Administrations of surfactant
(artificial or exogenous)
Place or apply pulse oximeter in
appropriate place such as in lower
extremities and record and change
probe levels hourly
Position infant in supine position with
rolled small towel beneath shoulders
to produce slight hyperextention
Provide prompt tactile stimulations
such as rubbing infant’s back or
tapping or flicking infant’s foot if
apnea occurs
Provide mouth care using saline or
glycerin swabs
Promote rest by minimizing
stimulation if necessary and energy
expenditure
It decreases severity of condition and
associated complications.
Provides constant noninvasive
monitoring oxygen level
Such positioning may facilitate
respiration and reduce episodes of
apnea especially in the presence of
hypoxia, metabolic acidosis or
hypercapnia
Stimulates CNS to promote body
movement and spontaneous return of
respirations.
Helps prevent drying and cracking of
lips associated with absence of oralintake or the drying effects of oxygen
therapy
Reduces metabolic rate and oxygen
consumption.
Edx:
Inform parents about infant’s
behavioral cues and responses to
stressors
Encouraged parental contact
Encourage parents to do hand hygiene
before and after and minimize
handling infant
Encourage parents to provide stroking
So that they can effectively intervene
to minimize stress and facilitate the
infant’s positive adaptation to
entrauterine life
Sometimes, infants experience fewer
or no episodes of apnea or
bradycardia if parents touch and talk to them.
Avoids further abdominal trauma and
infection to the infant
Enhances emotional and stroking
8/3/2019 Ncp Proper 1
http://slidepdf.com/reader/full/ncp-proper-1 5/6
of head, hands and feet and talk to
infant
needs through quiet conversation

8/3/2019 Ncp Proper 1
http://slidepdf.com/reader/full/ncp-proper-1 6/6
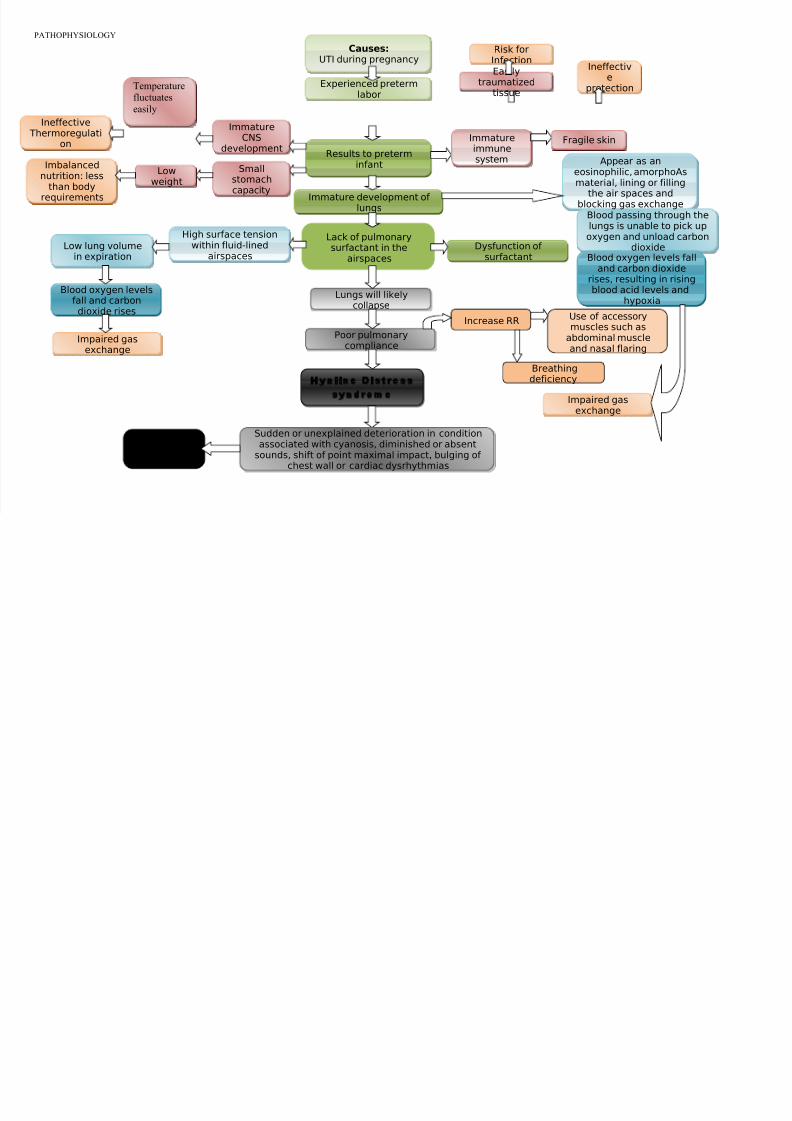
PATHOPHYSIOLOGY
Experienced pretermlabor
Results to preterminfant
Immature development of lungs
Lack of pulmonarysurfactant in the
airspaces
Dysfunction of surfactant
Appear as aneosinophilic, amorphoAsmaterial, lining or filling
the air spaces andblocking gas exchange
Causes:
UTI during pregnancy
Lungs will likelycollapse
Increase RRUse of accessorymuscles such as
abdominal muscleand nasal flaring
Impaired gasexchange
Poor pulmonarycompliance
Breathingdeficiency
High surface tensionwithin fluid-lined
airspacesLow lung volume
in expiration
Blood passing through thelungs is unable to pick upoxygen and unload carbon
dioxideBlood oxygen levels fall
and carbon dioxide
rises, resulting in risingblood acid levels and
hypoxiaBlood oxygen levels
fall and carbondioxide rises
Impaired gas
exchange
Hyaline Distress
syndrome
Immature
CNSdevelopment
Ineffective Thermoregulati
on
Smallstomachcapacity
Imbalancednutrition: less
than bodyrequirements
Immatureimmunesystem
Easilytraumatized
tissue
Risk forInfection
Fragile skin
Ineffective
protection
DEATH
Sudden or unexplained deterioration in conditionassociated with cyanosis, diminished or absent
sounds, shift of point maximal impact, bulging of chest wall or cardiac dysrhythmias
Temperaturefluctuates
easily
Lowweight