Multiple esophagogastric granular cell tumors
5
J Gastroenterol 2003; 38:776–780 DOI 10.1007/s00535-002-1145-9 Case report Multiple esophagogastric granular cell tumors Hiroshi Maekawa 1 , Takeo Maekawa 1 , Kiyotaka Yabuki 1 , Kouichi Sato 1 , Yoshihisa Tamazaki 1 , Keizou Kudo 1 , Ryo Wada 2 , and Michio Matsumoto 2 1 Department of Surgery, Izunagaoka Hospital, Juntendo University, 1129 Nagaoka Izunagaoka-cho, Tagata-gun, Shizuoka 410-2211, Japan 2 Department of Pathology, Izunagaoka Hospital, Juntendo University, Shizuoka, Japan with multiple granular cell tumors in the esophagus and stomach. Case report A 53-year-old man was admitted to our hospital, with- out symptoms, on 9 January, 2001, after esophageal and gastric abnormalities were noted on mass-screening by upper gastrointestinal barium roentogenogram. Past history included an episode of medication for gastric ulcer when he was 40 years old. There were no abnor- malities on physical examination, laboratory findings, or routine chest X-ray films. On gastroenterography, a filling defect, 0.5 cm in size, was found in the lower esophagus. Two filling defects were found in the posterior wall of the upper stomach. A convergency of folds was also noted in the same area of the stomach. Upper gastrointestinal endoscopy demonstrated a small round yellowish nodule in the lower thoracic esophagus (Fig. 1a) and three hemispherical tumors and an ulcer scar were detected in the posterior wall of the greater curvature in the upper stomach (Fig. 1b,c). These gastric tumors were covered with mucosa and were thought to be submucosal tumors. Biopsy of the esophageal tumor and the gastric tumors was per- formed, and pathological examination of the specimens demonstrated that the esophageal tumor and the gastric tumors were all granular cell tumors. On computed tomographic scan of the chest and ab- domen, there were no liver tumors, and no swollen lymph nodes were detected. There were no remarkable abnormalities in the colon or rectum on barium enema. Based on these findings, we diagnosed multiple esophagogastric granular cell tumors, but we could not determine whether these tumors were benign or malig- nant. Informed consent was obtained from the patient for endoscopic resection and gastrectomy. Initially, Multiple granular cell tumors of the esophagus and the stomach found in a 53-year-old man are reported. One lesion was detected within the lower thoracic esophagus and seven lesions were detected in the stomach. The esophageal tumor was resected endoscopically, and gas- trectomy was performed for the multiple gastric lesions. Histologically, the tumors consisted of spindle or poly- hedral cells and the cytoplasm contained punctated eosinophilic granules with positive immunohistochemi- cal staining for S-100 protein. The tumors were mainly located in the submucosal layer. Some tumor cells were seen in the mucosae propria and the muscularis propria. The tumor cells were only slightly positive for p53- and Ki-67-immunohistochemical stainings. Based on these findings, we diagnosed the granular cell tumors as be- nign. Granular cell tumor is comparatively rare in clini- cal practice, but a few such tumors have been seen in the digestive tract. A few cases of multiple esophagogastric granular cell tumors have also been reported in the literature. Key words: granular cell tumor, esophagus, stomach Introduction Granular cell tumor is comparatively rare in clinical practice, although granular cell tumors may arise at many sites, including skin, tongue, respiratory tract, and digestive tract. 1,2 Approximately 2.7%–8.1% of granular cell tumors arise in the gastrointestinal tract, 1–4 and ap- proximately 5%–12% of the tumors show multiple oc- currences. 1–5 We describe our experience with a patient Received: April 17, 2002 / Accepted: October 25, 2002 Reprint requests to: H. Maekawa
-
Upload
hiroshi-maekawa -
Category
Documents
-
view
213 -
download
1
Transcript of Multiple esophagogastric granular cell tumors

J Gastroenterol 2003; 38:776–780DOI 10.1007/s00535-002-1145-9
Case report
Multiple esophagogastric granular cell tumors
Hiroshi Maekawa1, Takeo Maekawa
1, Kiyotaka Yabuki1, Kouichi Sato
1, Yoshihisa Tamazaki1, Keizou Kudo
1,Ryo Wada
2, and Michio Matsumoto2
1 Department of Surgery, Izunagaoka Hospital, Juntendo University, 1129 Nagaoka Izunagaoka-cho, Tagata-gun, Shizuoka 410-2211, Japan2 Department of Pathology, Izunagaoka Hospital, Juntendo University, Shizuoka, Japan
with multiple granular cell tumors in the esophagus andstomach.
Case report
A 53-year-old man was admitted to our hospital, with-out symptoms, on 9 January, 2001, after esophageal andgastric abnormalities were noted on mass-screening byupper gastrointestinal barium roentogenogram. Pasthistory included an episode of medication for gastriculcer when he was 40 years old. There were no abnor-malities on physical examination, laboratory findings, orroutine chest X-ray films.
On gastroenterography, a filling defect, 0.5cm in size,was found in the lower esophagus. Two filling defectswere found in the posterior wall of the upper stomach.A convergency of folds was also noted in the same areaof the stomach.
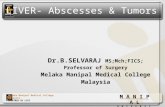
Upper gastrointestinal endoscopy demonstrated asmall round yellowish nodule in the lower thoracicesophagus (Fig. 1a) and three hemispherical tumors andan ulcer scar were detected in the posterior wall of thegreater curvature in the upper stomach (Fig. 1b,c).These gastric tumors were covered with mucosa andwere thought to be submucosal tumors. Biopsy of theesophageal tumor and the gastric tumors was per-formed, and pathological examination of the specimensdemonstrated that the esophageal tumor and the gastrictumors were all granular cell tumors.
On computed tomographic scan of the chest and ab-domen, there were no liver tumors, and no swollenlymph nodes were detected. There were no remarkableabnormalities in the colon or rectum on barium enema.Based on these findings, we diagnosed multipleesophagogastric granular cell tumors, but we could notdetermine whether these tumors were benign or malig-nant. Informed consent was obtained from the patientfor endoscopic resection and gastrectomy. Initially,
Multiple granular cell tumors of the esophagus and thestomach found in a 53-year-old man are reported. Onelesion was detected within the lower thoracic esophagusand seven lesions were detected in the stomach. Theesophageal tumor was resected endoscopically, and gas-trectomy was performed for the multiple gastric lesions.Histologically, the tumors consisted of spindle or poly-hedral cells and the cytoplasm contained punctatedeosinophilic granules with positive immunohistochemi-cal staining for S-100 protein. The tumors were mainlylocated in the submucosal layer. Some tumor cells wereseen in the mucosae propria and the muscularis propria.The tumor cells were only slightly positive for p53- andKi-67-immunohistochemical stainings. Based on thesefindings, we diagnosed the granular cell tumors as be-nign. Granular cell tumor is comparatively rare in clini-cal practice, but a few such tumors have been seen in thedigestive tract. A few cases of multiple esophagogastricgranular cell tumors have also been reported in theliterature.
Key words: granular cell tumor, esophagus, stomach
Introduction
Granular cell tumor is comparatively rare in clinicalpractice, although granular cell tumors may arise atmany sites, including skin, tongue, respiratory tract, anddigestive tract.1,2 Approximately 2.7%–8.1% of granularcell tumors arise in the gastrointestinal tract,1–4 and ap-proximately 5%–12% of the tumors show multiple oc-currences.1–5 We describe our experience with a patient
Received: April 17, 2002 / Accepted: October 25, 2002Reprint requests to: H. Maekawa

H. Maekawa et al.: Multiple esophagogastric granular cell tumors 777
endoscopic resection was attempted for the esophagealtumor. Total gastrectomy was performed because thegastric granular cell tumors had a multifocal appear-ance. Intraoperatively, there were no findings of livermetastasis or regional lymph node swelling.
Macroscopic findings of the resected specimen
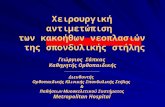
A 1.0 � 1.2-cm specimen of endoscopically resectedesophagus was examined. A yellowish hemisphericaltumor, measuring 0.3 cm in maximal diameter, wasfound. The stomach measured 22 � 17 cm, and linearulcer scars were seen in the lesser curvature of the upperstomach. A hemispherical nodular lesion 1.5cm indiameter was noted in the upper stomach. Several othernodular lesions, measuring 0.5 to 0.7cm in maximaldiameter, were detecteded surrounding the ulcer scarsin the upper stomach (Fig. 2).
Fig. 1. a Upper gastrointestinal endoscopic findings of theesophagus. A small round yellowish nodule was noted inthe lower thoracic esophagus. b Upper gastrointestinalendoscopic findings of the stomach. Three hemisphericalnodules covered with normal mucosa and an ulcer scar, wereseen on the posterior wall of the greater curvature of theupper stomach was seen. c Upper gastrointestinal endo-scopic findings of the stomach. A hemispherical nodule wasnoted just below the cardia. The surface mucosa of thetumor showed erosive change. Hiatal hernia was also noted
�
a
b
c
Fig. 2. Resected specimen: stomach. The stomach measured22 � 17 cm. Linear ulcer scars were seen on the lesser curva-ture of the upper stomach. A hemispherical nodular lesion1.5 cm in diameter was noted in the upper stomach; severalother nodular lesions, measuring 0.5 to 0.7 cm in maximaldiameter, were seen in the same area. Each of the sevenlesions is indicated with an arrowhead

778 H. Maekawa et al.: Multiple esophagogastric granular cell tumors
Histopathological findings
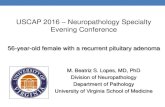
In the resected specimen of the esophageal tumor andgastric tumors, polyhedral cells aggregated and theircytoplasm had punctated eosinophilic granules (Fig.3a). These tumor cells were periodic acid-Schiff (PAS)-positive and remained positive after diastase digestion.These tumor cells were mainly located in the submu-cosal layer. However, some parts of the tumor arisingfrom the submucosal layer were noted in the mucosaepropria and the muscularis propria. Most tumor cellsshowed positive immunohistochemical staining forS-100 protein (Fig. 3b). These findings suggested thatthese tumors were granular cell tumors. Only focal
pleomorphisms were seen, but malignant features suchas necrosis, spindling of the tumor cells, vesicular nucleiwith large nucleoli, and increased mitotic rate were notdetected. These tumor cells were partially positive forp53 and Ki-67 immunohistochemical stainings (Fig.4a,b). On the immunohistochemical stainings, the p53positivity rate was 7% and the Ki-67 value was lessthan 10%. No lymph node metastases were detectedhistologically.
The patient’s postoperative clinical course was un-eventful and he was discharged on the fifteenth post-operative day. He has remained asymptomatic after 14months of follow up.
a b
Fig. 3. a Histological findings of the resected specimen with H&E staining. The polyhedral cells showed aggregation and thecytoplasm contained punctated eosinophilic granules. b Histological findings of the resected specimen with immunohistochemicalstaining for S-100 protein. The tumor cells showed positive immunohistochemical staining for S-100 protein
a b
Fig. 4. a Histological findings of the resected specimen with p53 immunohistochemical staining. Some of the tumor cells werepositive for p53 immunohistochemical staining. b Histological findings of the resected specimen with Ki-67 immunohistochemicalstaining. Some of the tumor cells were positive for Ki-67 immunohistochemical staining

H. Maekawa et al.: Multiple esophagogastric granular cell tumors 779
Discussion
Granular cell tumor is a comparatively rare lesion inclinical practice. If was first reported by Abrikossoff asmyoblastoma in 1926.6 Although the tumor cells weremorphologically similar to myoblast cells, immunohis-tochemical techniques employing antisera to S-100 pro-tein proved that this tumor originated from Schwanncells.7,8 Although the tumors most often arise in skin orsubcutaneous tissue, 2.7%–8.1% of granular cell tumorsoccurred in the digestive tract1–4 and 5%–12% of granu-lar cell tumors were multiple.1–3,5 One-third of digestive-tract granular cell tumors arose in the esophagus and10% arose in the stomach.3–5 There are some reports ofpatients in whom several granular cell tumors arosefrom the esophagus,3,4,9–11 the stomach,12–15 or both theesophagus and stomach.12,16,17 Histologically, the tumorswere usually located in the submucosal layer, but some-times the tumor cells were seen in the proper musclelayer or mucosal layer, though the cells were histologi-cally benign.5,12,13,18,19
Malignant granular cell tumor is seldom encounteredclinically, and approximately 1.5%–2.7% of granularcell tumors were malignant.1,4,9 Malignant granular celltumors were classified into two types. One was the his-tologically and clinically malignant type, and the otherwas the histologically benign but clinically malignanttype.20,21 David and Jakate19 suggested that the featuresassociated with malignancy included local recurrence,rapid growth to a size greater than 4 cm, tumor necrosis,increased cellularity, cytologic atypia, and mitotic activ-ity of greater than two mitoses per high-power field. Todate, however, there have been few reports concerningthe criteria for malignant granular cell tumor with his-tology and immunohistochemical stainings for p53 orKi-67. Fanburg-Smith et al.22 reported pathologic andimmunohistochemical features including staining forp53 and Ki-67, in granular cell tumors arising in softtissue. Malignant pathologic features included necrosis,spindling of the tumor cells, vesicular nuclei with largenucleoi, increased mitotic rate (�2 mitoses/10 high-power fields at 200 � magnification), a high nuclear-to-cytoplasmic (N/C) ratio, and pleomorphism. However,if the tumor only demonstrated focal pleomorphism, itwas classified as benign. On immunohistochemicalstainings, they noted that a positivity rate of more than50% for p53 and a Ki-67 index of more than 10% weresignificantly correlated with malignancy. Benign granu-lar cell tumors were exclusively negative for proliferat-ing cell nuclear antigen (PCNA), bcl-2, p53, and Ki-67.22
Other reports have accepted these criteria22 in diagnos-ing whether granular cell tumors were benign or malig-nant.23,24 In our patient, immunohistochemical stainingsfor p53 and Ki-67 showed that the p53 positivity ratewas 7% and the Ki-67 value was less than 10%. Further-
more, there was a report of histologically benign granu-lar cell tumor showing a p53 positivity rate of 35% to42%.25 In our patient, only focal pleomorphism was de-tected histologically, and positivity for p53 and Ki-67was low. Based on these findings, our case was notconsidered to be a malignant granular cell tumor.
Asymptomatic granular cell tumors without malig-nant findings do not need to be treated. Endoscopicfollow-up and observation is indicated.16 In contrast,treatment for symptomatic and malignant granular celltumor is wide local excision with subsequent surgery forrecurrent disease, as necessary.16 Neither radiotherapynor chemotherapy has been shown to offer any advan-tage in the management of malignant granular celltumor.26 However, sufficient follow-up for granular celltumors is necessary, even when they are histologicallydiagnosed as benign after resection.27 Klima andPeters27 reported a case in which there was no mitoticactivity or other nuclear atypia present in the originalresected specimen, but malignant features such asnuclear atypia were demonstrated in the recurrenttumor. Further, 70% of malignant granular cell tumorsdemonstrated lymph-node metastasis and 50% of suchtumors showed lung metastasis during the clinicalcourse.26–28
In our patient, we performed gastrectomy for mul-tiple gastric granular cell tumors, because we could notdetermine whether these tumors were benign or malig-nant preoperatively. The results of p53 and Ki-67 immu-nohistochemical staining were slightly positive. Thesefindings suggest that the esophageal and gastric granu-lar cell tumors were not malignant.
References
1. Strong EW, McDivitt RW, Brasfield RD. Granular cellmyoblastoma. Cancer 1970;25:415–22.
2. Lack EE, Worsham GF, Callihan MD, Crawford BE,Klappenbach S, Rowden G, et al. Granular cell tumor: a clinico-pathologic study of 110 patients. J Surg Oncol 1980;13:301–16.
3. Rubesin S, Herlinger H, Sigal H. Granular cell tumors of theesophagus. Gastrointest Radiol 1985;10:11–5.
4. Ohmori T, Arita N, Uraga N, Tabei R, Tani M, Okamura H.Malignant granular cell tumor of the esophagus. A case reportwith light and electron microscopic, histochemical, and immuno-histochemical study. Acta Pathol Jpn 1987;37:775–83.
5. Johnston MJ, Helwig EB. Granular cell tumors of the gastrointes-tinal tract and perianal region. A study of 74 cases. Dig Dis Sci1981;26:807–16.
6. Abrikossoff A. Uber Myome, ausgehend von der quergestreifenwirkulichen musculature. Virchows Arch Pathl Anat Physiol1926;260:214–33.
7. Stefansson K, Wollmann RL. S-100 protein in granular cell tu-mors (granular cell myoblastomas). Cancer 1982;49:1834–8.
8. Mazur MT, Shultz JJ, Myers JL. Granular cell tumor. Immuno-histochemical analysis of 21 benign tumors and one malignanttumor. Arch Pathol Lab Med 1990;114:692–6.

780 H. Maekawa et al.: Multiple esophagogastric granular cell tumors
9. Patel RM, Desota-LaPaix F, Sika JV, Mallaiah LR, Purow E.Granular cell tumor of the esophagus. Report of two casesand review of the literature. Am J Gastroenterol 1981;76:519–23.
10. Subramanyam K, Shannon CR, Patterson M, Davis M, GourleyWK. Granular cell myoblastoma of the esophagus. J ClinGastroenterol 1984;6:113–8.
11. Goldblum JR, Rice TW, Zuccaro G. Granular cell tumors of theesophagus: a clinical and pathologic study of 13 cases. Ann ThoracSurg 1996;62:860–5.
12. Schwartz DT, Gaetz HP. Multiple granular cell myoblastomas ofthe stomach. Am J Clin Pathol 1965;44:453–7.
13. Krouse TB, Mobini JM. Multifocal granular cell myoblastoma.Report of a case involving trachea, stomach, and anterior abdomi-nal wall. Arch Pathol 1973;96:95–9.
14. Chen KT. Multifocal benign granular cell tumor of the stomach.J Clin Gastroenterol 1981;3(Suppl 1):65–7.
15. Seo IS, Azzarelli B, Warner TF, Goheen MP, Senteney GE. Mul-tiple visceral and cutaneous granular cell tumors. Ultrastructualand immunocytochemical evidence of Schwann cell origin. Can-cer 1984;54:2104–10.
16. Fried KS, Arden JL, Gouge TH, Balthazar EJ. Multifocal granu-lar cell tumors of the gastrointestinal tract. Am J Gastroenterol1984;10:751–5.
17. Blandamura S, Altavilla G, Castoro C, Antonini C, Piazza A.Combined granular cell tumour of the oesophagus and stomach: acase report and review of the literature. Ital J Gastroenterol1993;25:259–64.
18. Abdelwahab IF, Klein MJ. Granular cell tumor of the stomach:a case report and review of the literature. Am J Gastroenterol1983;78:71–6.
19. David O, Jakate S. Multifocal granular cell tumor of the esopha-gus and proximal stomach with infiltrative pattern. A case reportand review of the literature. Arch Pathol Lab Med 1999;123:967–73.
20. Dzubow LM, Kramer EM. Treatment of a large, ulcerating,granular-cell tumor by microscopically controlled excision.J Dermatol Surg 1985;11:392–5.
21. Gamboa LG. Malignant granular-cell myoblastoma. Arch Pathol1955;60:663–8.
22. Fanburg-Smith JC, Meis-Kindblom JM, Fante R, Kindblom L-G.Malignant granular cell tumor of soft tissue. Diagnostic criteriaand clinicopathologic correlation. Am J Surg Pathol 1998;22:779–94.
23. Kasashima S, Oda Y, Nozaki J, Shirasaki M, Nakanishi I. A caseof atypical granular cell tumor of the neurohypophysis. Pathol Int2000;50:568–73.
24. Cruz-Mojarrietta J, Navarro S, Gomez-Cabrera E, Perez-Pena L,Soriano P, Peydro-Oyala A, Llombart-Bosch A. Malignantgranular cell tumor of soft tissue. A study of two new cases. Int JSurg Pathol 2001;9:255–9.
25. Lassaletta L, Alonso S, Ballestin C, Martinez-Tello FJ,Alvarez-Vicent JJ. Immunoreactivity in granular cell tumours ofthe larynx. Auris Nasus Larynx 1999;26:305–10.
26. Wyatt MG, O’Donoghue DS, Clarke TJ, Teasdale C. Malignantgranular cell tumour of the oesophagus. Eur J Surg Oncol1991;17:388–91.
27. Klima M, Peters J. Malignant granular cell tumor. Arch PatholLab Med 1987;111:1070–3.
28. Jardines L, Cheung L, LiVolsi V, Hendrickson S, Brooks JJ.Malignant granular cell tumors: report of a case and review of theliterature. Surgery 1994;116:49–54.