
Management of diabetic ketoacidosis - · PDF fileDefinition of Diabetic Ketoacidosis ......
33
Management of diabetic ketoacidosis: from a perspective of nephrologist 제29차 대한당뇨병학회 춘계학술대회 조 장 희 경북대학교병원 신장내과
Transcript of Management of diabetic ketoacidosis - · PDF fileDefinition of Diabetic Ketoacidosis ......
Management of diabetic ketoacidosis:
from a perspective of nephrologist
제29차 대한당뇨병학회 춘계학술대회
조 장 희 경북대학교병원 신장내과
없 음
본 발표와 관련된 이해관계
대한당뇨병학회 학술위원회
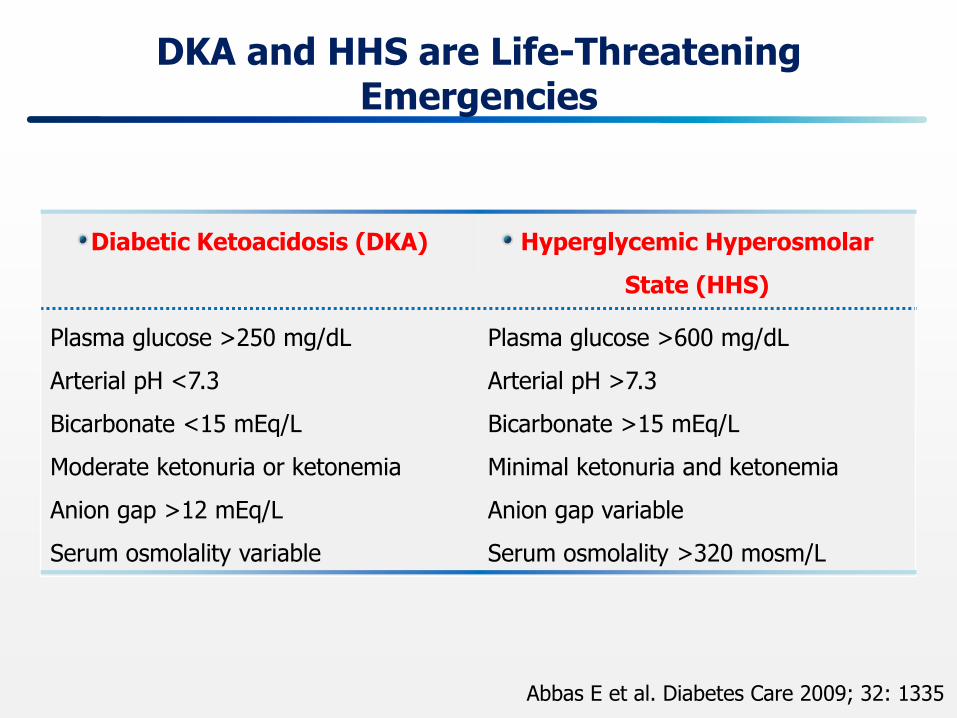
DKA and HHS are Life-Threatening Emergencies
Abbas E et al. Diabetes Care 2009; 32: 1335
Diabetic Ketoacidosis (DKA) Hyperglycemic Hyperosmolar
State (HHS)
Plasma glucose >250 mg/dL
Arterial pH <7.3
Bicarbonate <15 mEq/L
Moderate ketonuria or ketonemia
Anion gap >12 mEq/L
Serum osmolality variable
Plasma glucose >600 mg/dL
Arterial pH >7.3
Bicarbonate >15 mEq/L
Minimal ketonuria and ketonemia
Anion gap variable
Serum osmolality >320 mosm/L
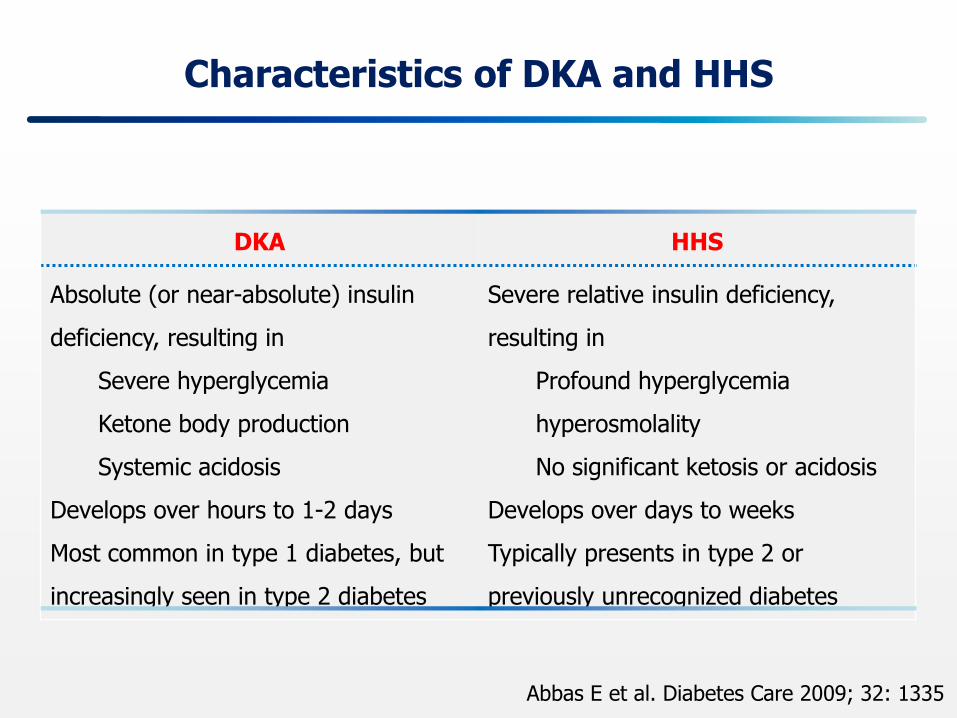
Characteristics of DKA and HHS
Abbas E et al. Diabetes Care 2009; 32: 1335
DKA HHS
Absolute (or near-absolute) insulin
deficiency, resulting in
Severe hyperglycemia
Ketone body production
Systemic acidosis
Develops over hours to 1-2 days
Most common in type 1 diabetes, but
increasingly seen in type 2 diabetes
Severe relative insulin deficiency,
resulting in
Profound hyperglycemia
hyperosmolality
No significant ketosis or acidosis
Develops over days to weeks
Typically presents in type 2 or
previously unrecognized diabetes

Definition of Diabetic Ketoacidosis
Adapted from Kitabchi AE, Fisher JN. Diabetes Mellitus. In: Glew RA, Peters SP, ed. Clinical Studies in Medical Biochemistry. New York, NY: Oxford University Press; 1987:105.
Hyperglycemia
Ketosis
Acidosis
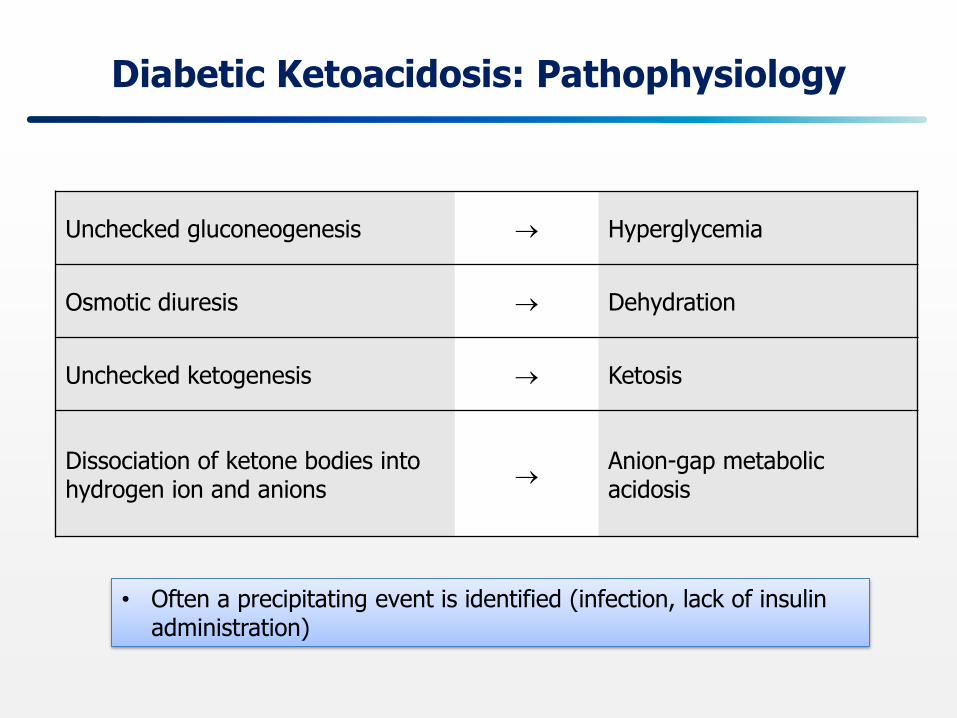
Diabetic Ketoacidosis: Pathophysiology
Unchecked gluconeogenesis Hyperglycemia
Osmotic diuresis Dehydration
Unchecked ketogenesis Ketosis
Dissociation of ketone bodies into hydrogen ion and anions
Anion-gap metabolic acidosis
• Often a precipitating event is identified (infection, lack of insulin administration)
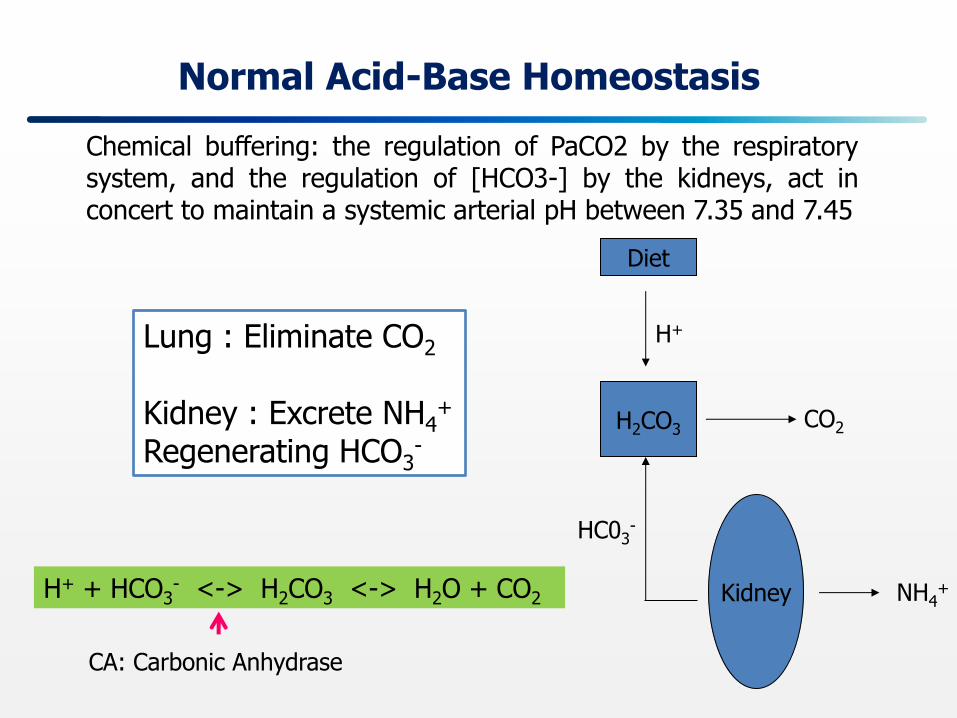
Normal Acid-Base Homeostasis
Chemical buffering: the regulation of PaCO2 by the respiratory system, and the regulation of [HCO3-] by the kidneys, act in concert to maintain a systemic arterial pH between 7.35 and 7.45
Lung : Eliminate CO2
Kidney : Excrete NH4
+
Regenerating HCO3-
Diet
H2CO3
Kidney
CO2
NH4+
H+
HC03-
H+ + HCO3- <-> H2CO3 <-> H2O + CO2
CA: Carbonic Anhydrase
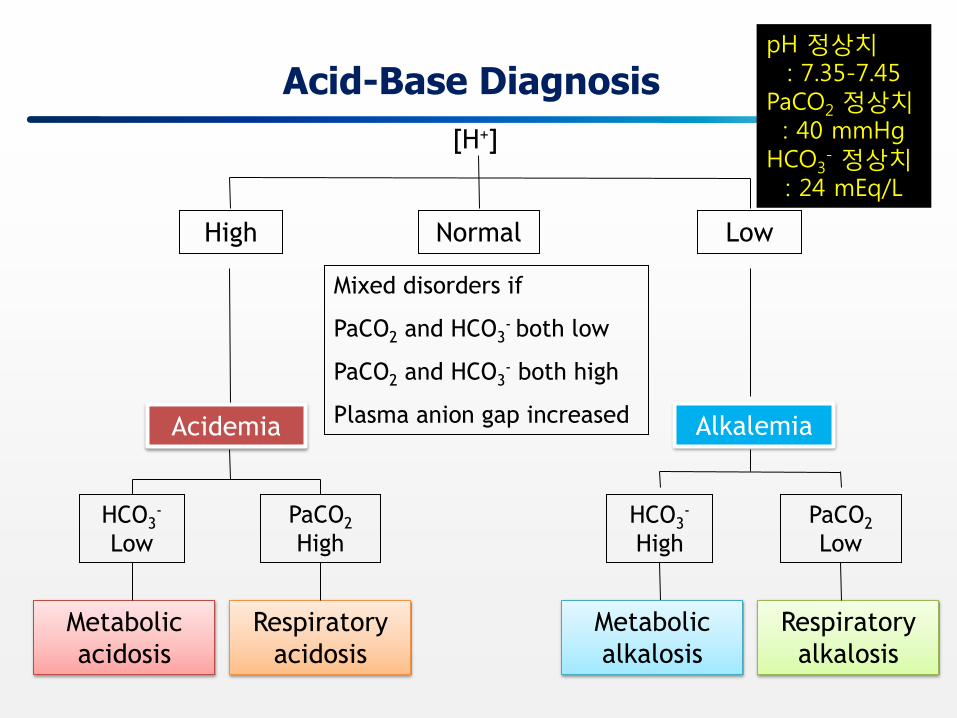
Acid-Base Diagnosis
[H+]
High Normal Low
Mixed disorders if
PaCO2 and HCO3- both low
PaCO2 and HCO3- both high
Plasma anion gap increased Acidemia Alkalemia
HCO3-
Low
HCO3-
High
PaCO2
Low
Metabolic
alkalosis
Respiratory
alkalosis
Respiratory
acidosis
Metabolic
acidosis
PaCO2
High
pH 정상치 : 7.35-7.45
PaCO2 정상치 : 40 mmHg
HCO3- 정상치
: 24 mEq/L
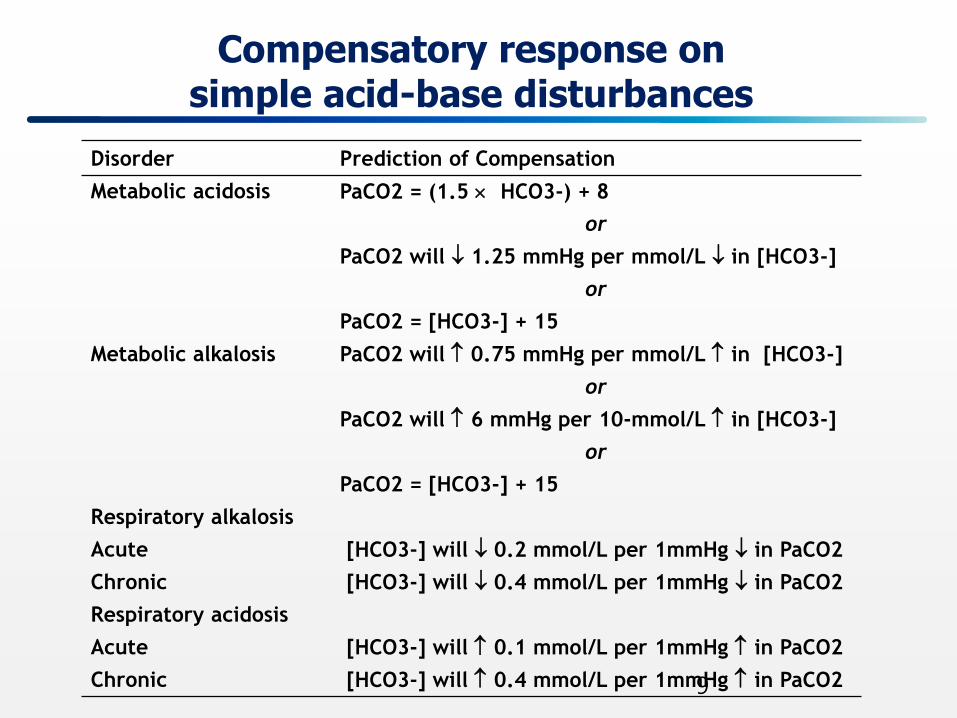
Compensatory response on simple acid-base disturbances
Disorder Prediction of Compensation
Metabolic acidosis PaCO2 = (1.5 HCO3-) + 8
or
PaCO2 will 1.25 mmHg per mmol/L in [HCO3-]
or
PaCO2 = [HCO3-] + 15
Metabolic alkalosis PaCO2 will 0.75 mmHg per mmol/L in [HCO3-]
or
PaCO2 will 6 mmHg per 10-mmol/L in [HCO3-]
or
PaCO2 = [HCO3-] + 15
Respiratory alkalosis
Acute [HCO3-] will 0.2 mmol/L per 1mmHg in PaCO2
Chronic [HCO3-] will 0.4 mmol/L per 1mmHg in PaCO2
Respiratory acidosis
Acute [HCO3-] will 0.1 mmol/L per 1mmHg in PaCO2
Chronic [HCO3-] will 0.4 mmol/L per 1mmHg in PaCO2 9
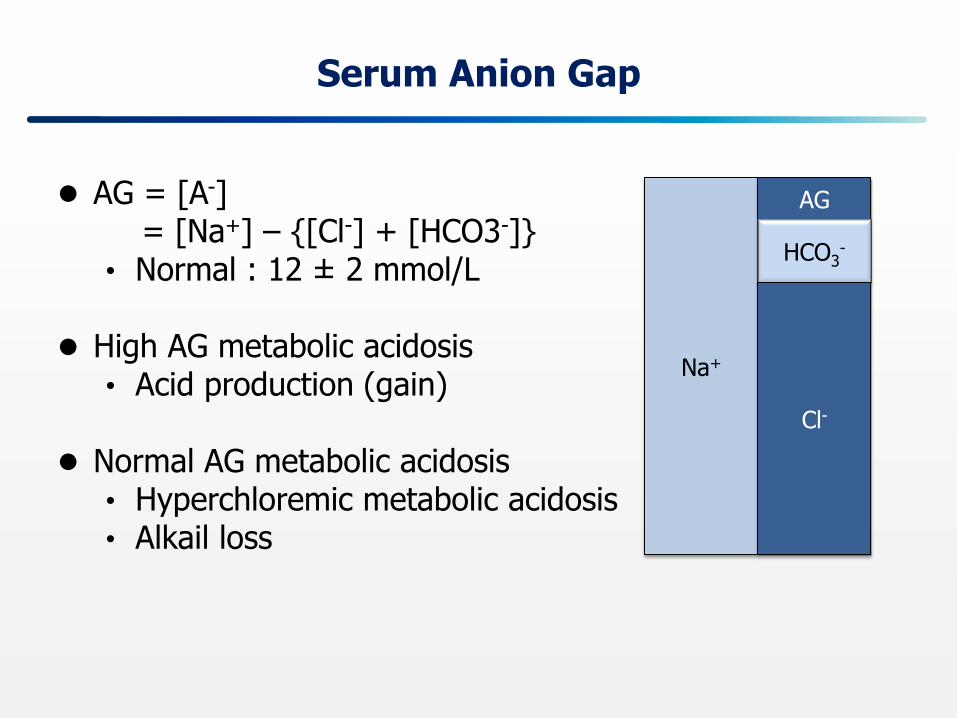
Serum Anion Gap
AG = [A-] = [Na+] – {[Cl-] + [HCO3-]}
• Normal : 12 ± 2 mmol/L High AG metabolic acidosis
• Acid production (gain)
Normal AG metabolic acidosis • Hyperchloremic metabolic acidosis • Alkail loss
Na+
AG
HCO3-
Cl-
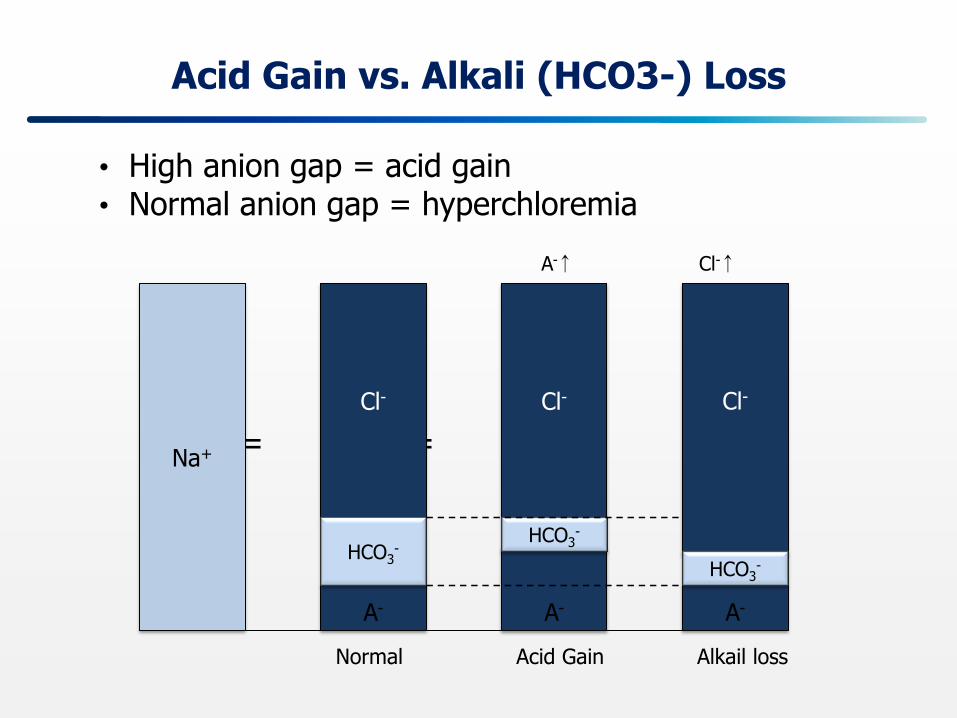
Acid Gain vs. Alkali (HCO3-) Loss
• High anion gap = acid gain • Normal anion gap = hyperchloremia
= = =
Na+
Cl- Cl- Cl-
A-
A-
HCO3-
HCO3-
A-
HCO3-
Normal Acid Gain Alkail loss
A-↑ Cl-↑
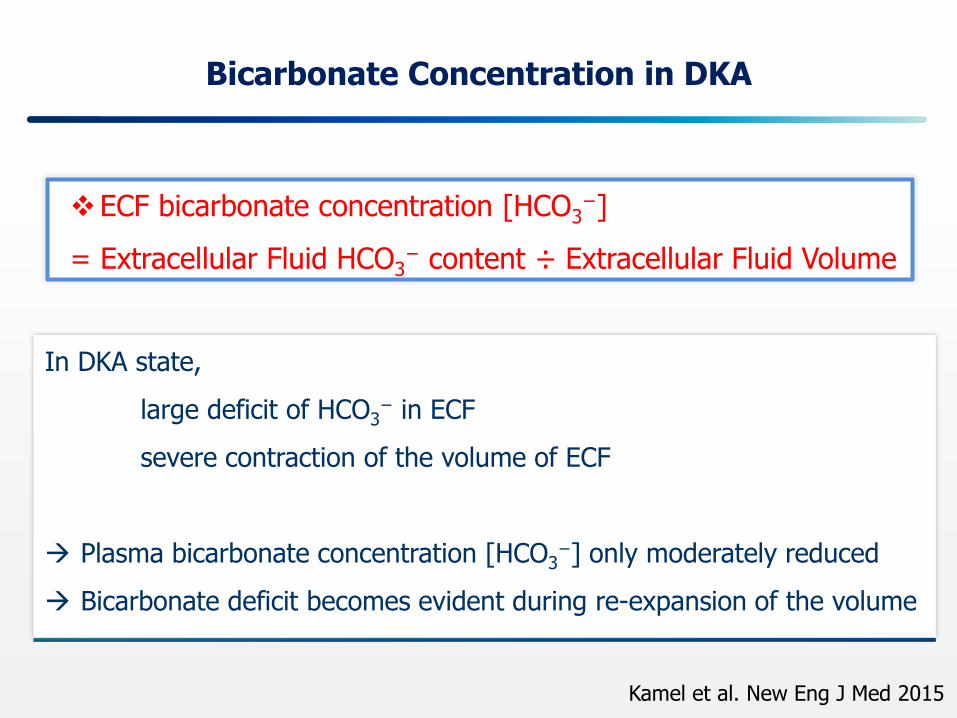
Bicarbonate Concentration in DKA
Kamel et al. New Eng J Med 2015
In DKA state,
large deficit of HCO3− in ECF
severe contraction of the volume of ECF
Plasma bicarbonate concentration [HCO3−] only moderately reduced
Bicarbonate deficit becomes evident during re-expansion of the volume
ECF bicarbonate concentration [HCO3−]
= Extracellular Fluid HCO3− content ÷ Extracellular Fluid Volume
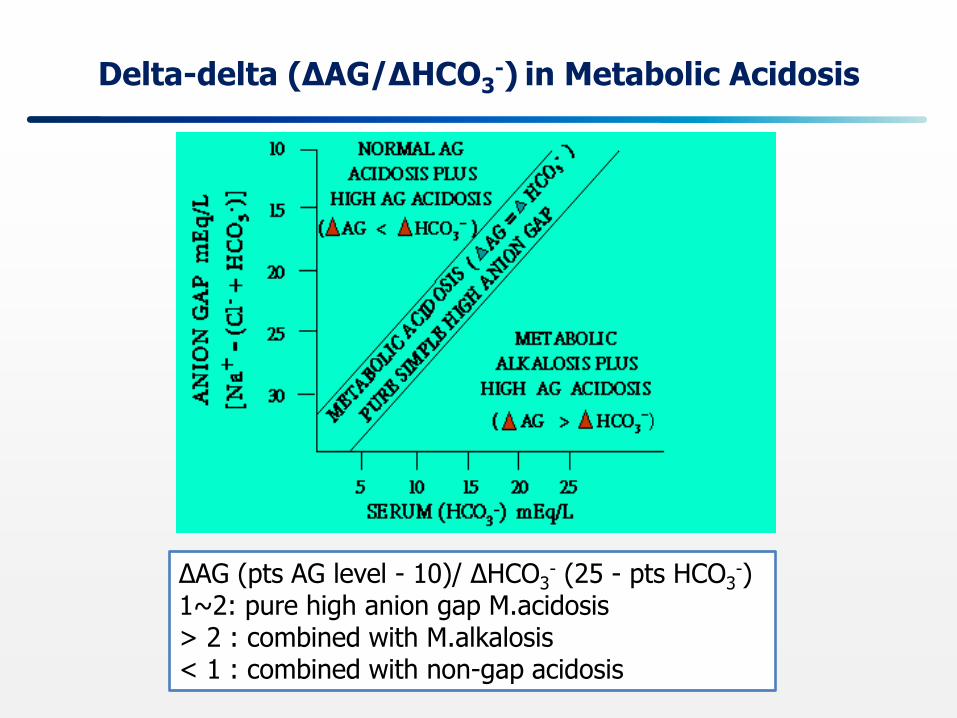
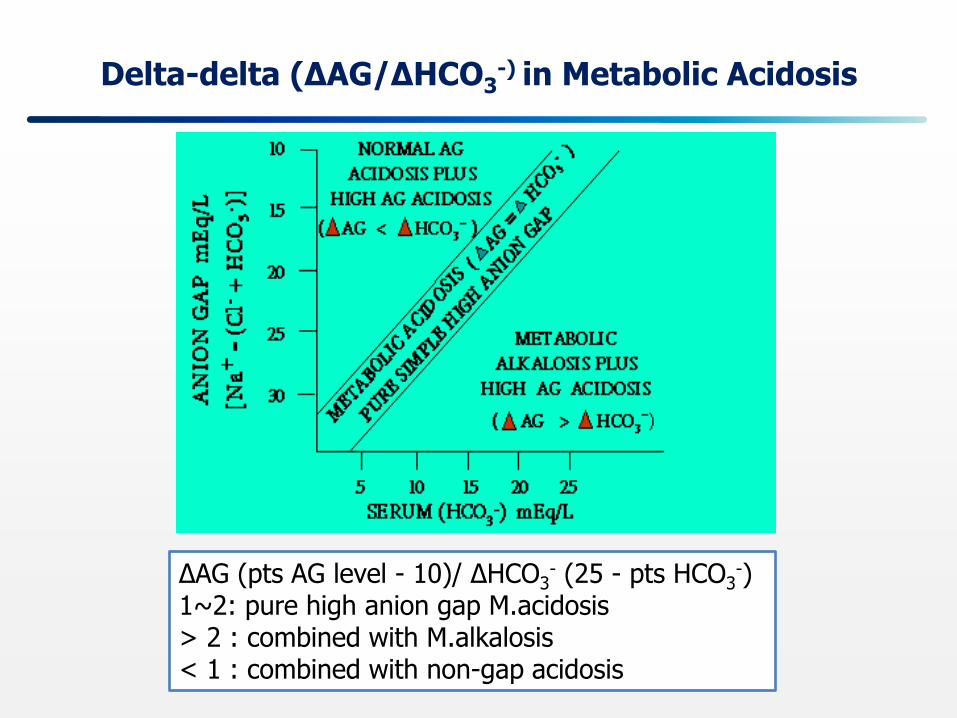
Delta-delta (ΔAG/ΔHCO3-) in Metabolic Acidosis
∆AG (pts AG level - 10)/ ∆HCO3- (25 - pts HCO3
-) 1~2: pure high anion gap M.acidosis > 2 : combined with M.alkalosis < 1 : combined with non-gap acidosis
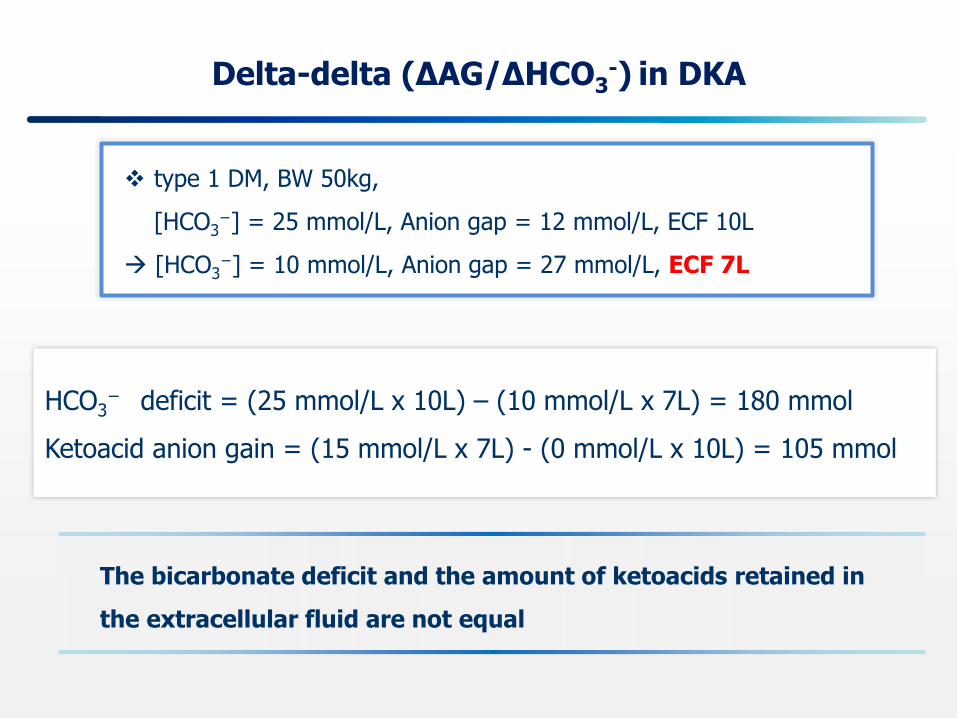
Delta-delta (ΔAG/ΔHCO3-) in DKA
HCO3− deficit = (25 mmol/L x 10L) – (10 mmol/L x 7L) = 180 mmol
Ketoacid anion gain = (15 mmol/L x 7L) - (0 mmol/L x 10L) = 105 mmol
type 1 DM, BW 50kg,
[HCO3−] = 25 mmol/L, Anion gap = 12 mmol/L, ECF 10L
[HCO3−] = 10 mmol/L, Anion gap = 27 mmol/L, ECF 7L
The bicarbonate deficit and the amount of ketoacids retained in
the extracellular fluid are not equal
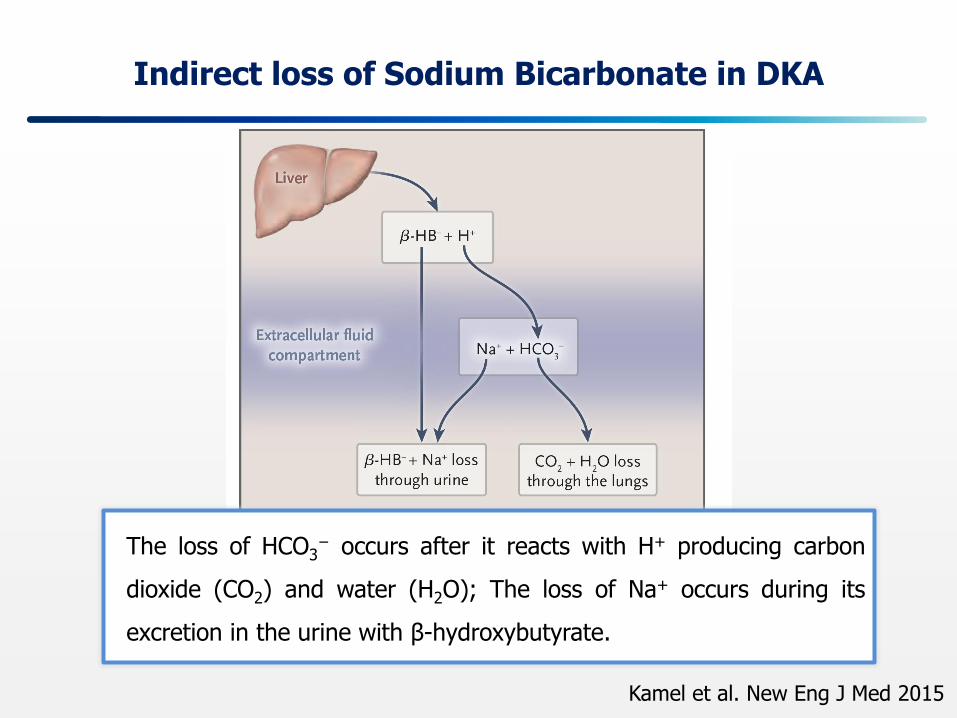
Indirect loss of Sodium Bicarbonate in DKA
The loss of HCO3− occurs after it reacts with H+ producing carbon
dioxide (CO2) and water (H2O); The loss of Na+ occurs during its
excretion in the urine with β-hydroxybutyrate.
Kamel et al. New Eng J Med 2015
Initial Monitoring
Complete initial evaluation
Check capillary glucose
Check serum/urine ketones
Obtain blood metabolic profile: electrolyte, anion gap, plasma
osmolality
Start IV fluids: 1.0 L of 0.9% NaCl per hour
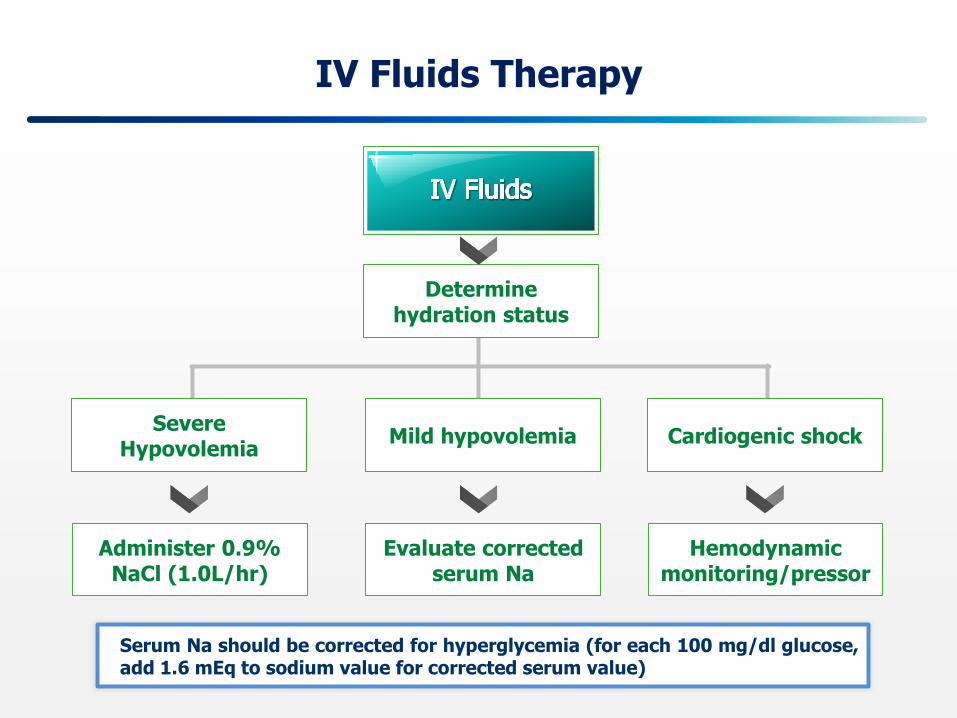
IV Fluids Therapy
Determine hydration status
Severe Hypovolemia
Mild hypovolemia Cardiogenic shock
Administer 0.9% NaCl (1.0L/hr)
Evaluate corrected serum Na
Hemodynamic monitoring/pressor
Serum Na should be corrected for hyperglycemia (for each 100 mg/dl glucose, add 1.6 mEq to sodium value for corrected serum value)
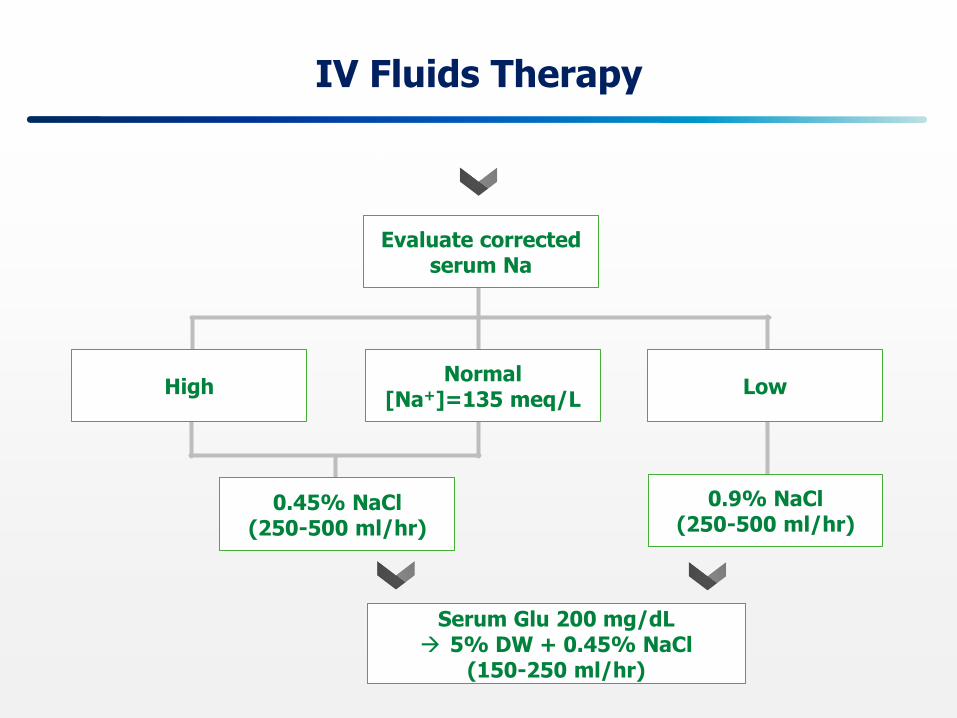
IV Fluids Therapy
Evaluate corrected serum Na
High Normal
[Na+]=135 meq/L Low
0.45% NaCl (250-500 ml/hr)
0.9% NaCl (250-500 ml/hr)
Serum Glu 200 mg/dL 5% DW + 0.45% NaCl
(150-250 ml/hr)
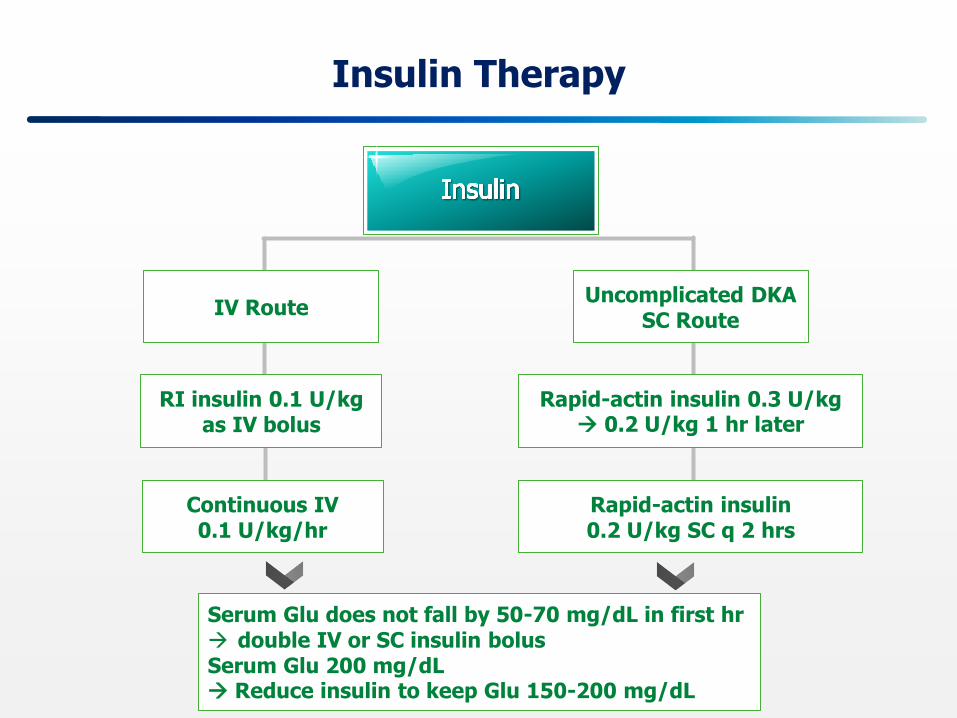
Insulin Therapy
Serum Glu does not fall by 50-70 mg/dL in first hr double IV or SC insulin bolus Serum Glu 200 mg/dL Reduce insulin to keep Glu 150-200 mg/dL
IV Route Uncomplicated DKA
SC Route
RI insulin 0.1 U/kg as IV bolus
Rapid-actin insulin 0.3 U/kg 0.2 U/kg 1 hr later
Continuous IV 0.1 U/kg/hr
Rapid-actin insulin 0.2 U/kg SC q 2 hrs
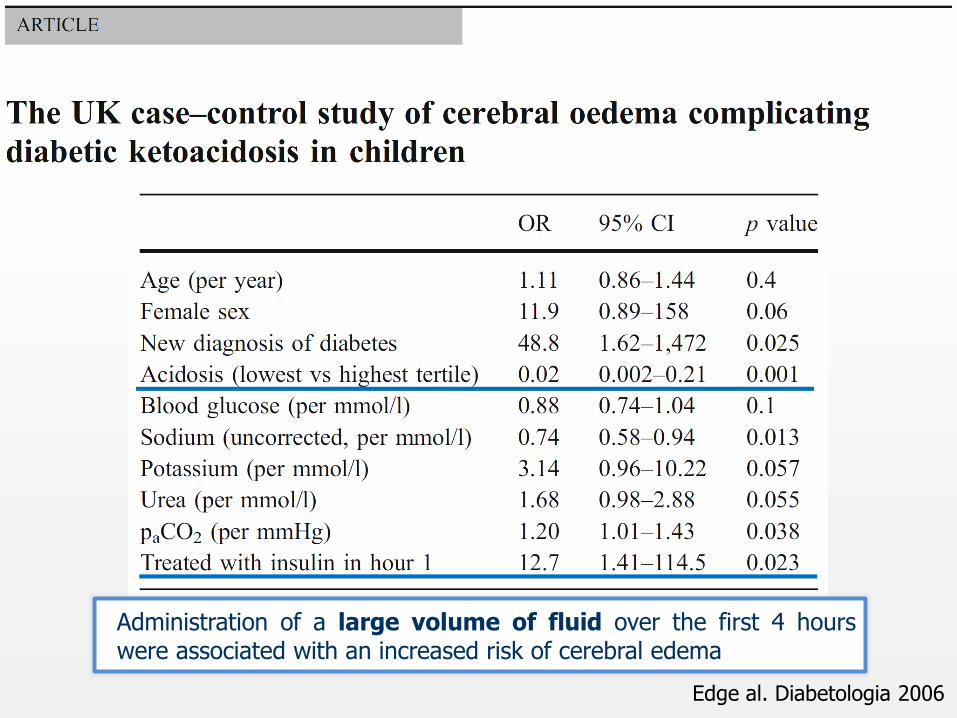
Edge al. Diabetologia 2006
Administration of a large volume of fluid over the first 4 hours were associated with an increased risk of cerebral edema
Plasma Osmolality
Urea
- Transported across most cell membranes
- Achieves equal concentrations in ECF and ICF
Total osmolality in plasma
= 2 × [Na+] + [Glucose]/18 + [BUN] /2.8
Effective osmolality in plasma
= 2 × [Na+] + [Glucose]/18
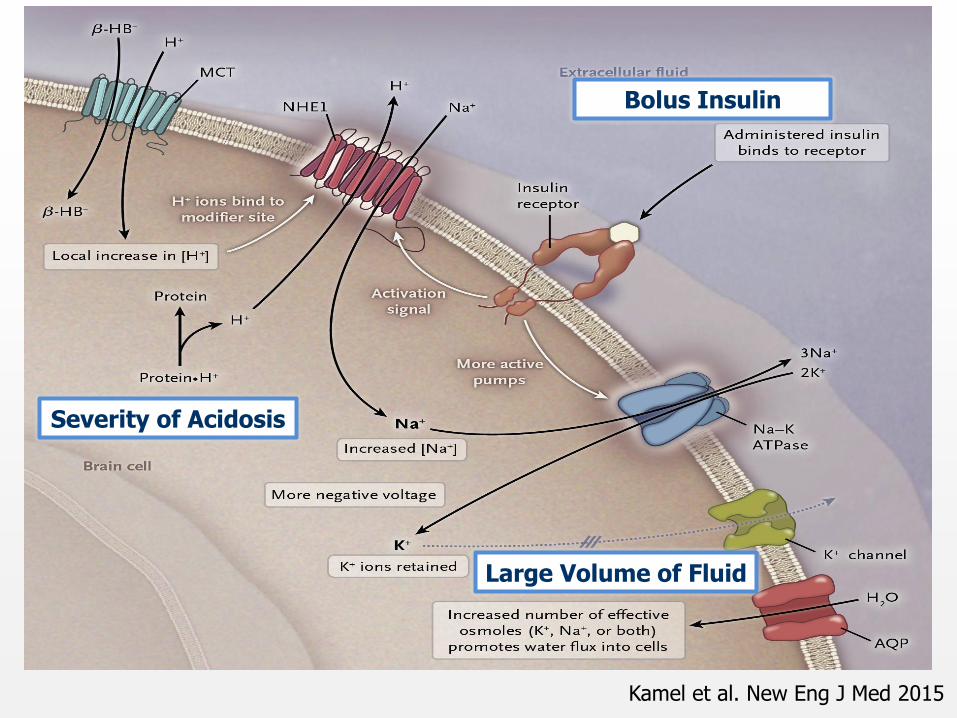
Kamel et al. New Eng J Med 2015
Severity of Acidosis
Bolus Insulin
Large Volume of Fluid
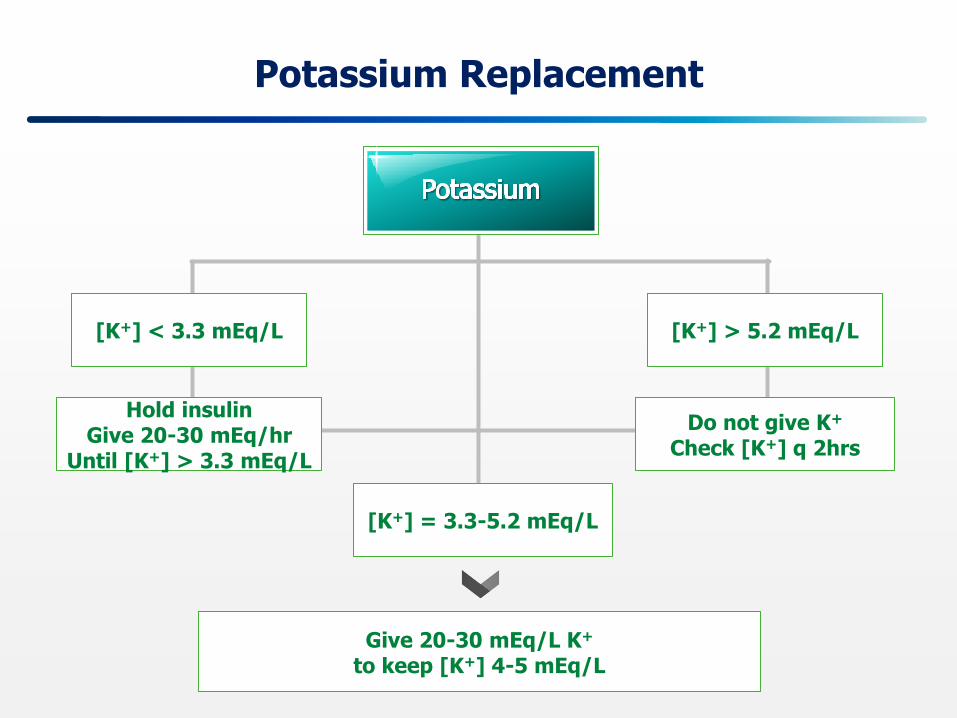
Potassium Replacement
Give 20-30 mEq/L K+
to keep [K+] 4-5 mEq/L
[K+] < 3.3 mEq/L
[K+] = 3.3-5.2 mEq/L
[K+] > 5.2 mEq/L
Hold insulin Give 20-30 mEq/hr
Until [K+] > 3.3 mEq/L
Do not give K+
Check [K+] q 2hrs
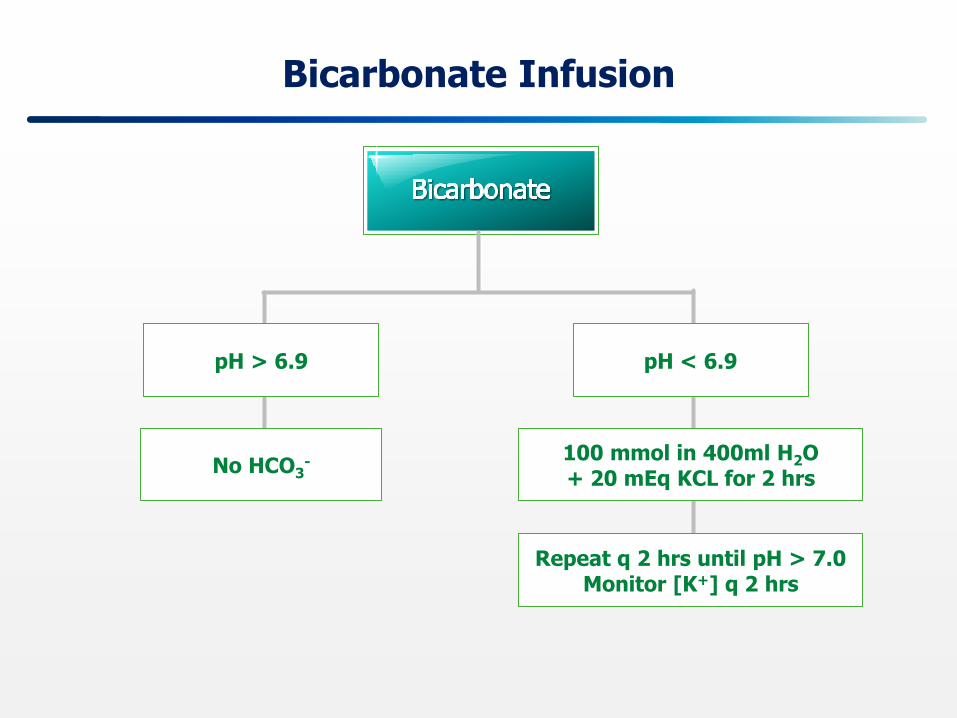
Bicarbonate Infusion
pH > 6.9 pH < 6.9
No HCO3- 100 mmol in 400ml H2O
+ 20 mEq KCL for 2 hrs
Repeat q 2 hrs until pH > 7.0 Monitor [K+] q 2 hrs
Severe Acidemia
Decreased cardiac contractility
Diminished responses to catecholamines
Predisposition to cardiac arrhythmias
Hemodynamic instability
Impair the capacity of insulin to slow the rate of ketoacid
production
From 508 potentially relevant articles, 44 were included
Two RCTs demonstrated transient improvement in metabolic
acidosis with bicarbonate treatment within the initial 2 hours.
There was no evidence of improved glycemic control or
clinical efficacy.
Increased risk for cerebral edema and prolonged
hospitalization in children who received bicarbonate
Chua et al. Annals of Intensive Care 2011
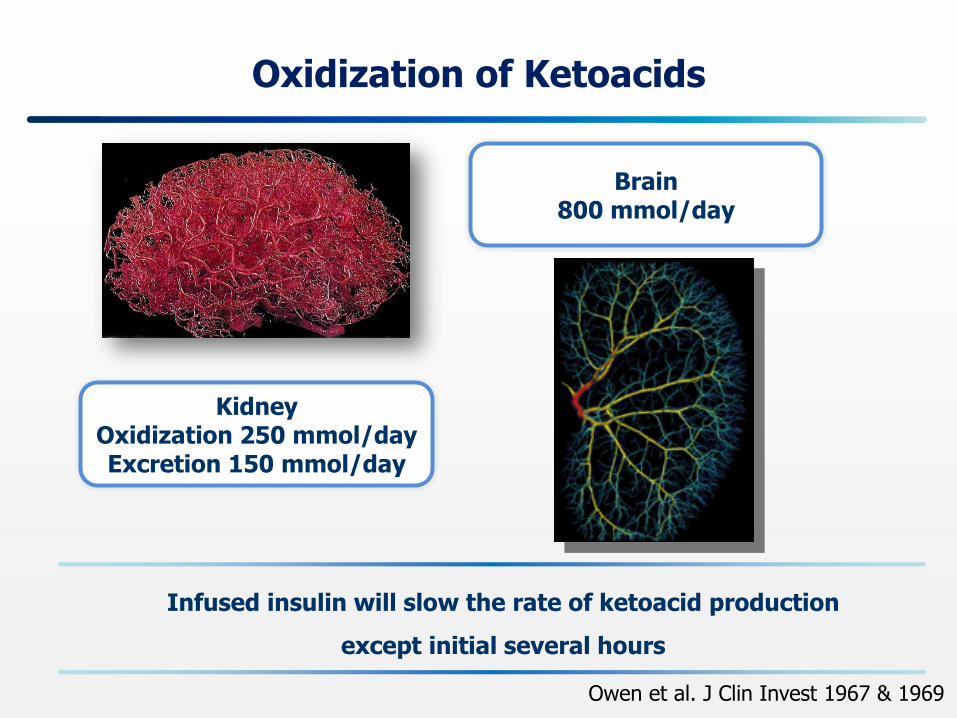
Oxidization of Ketoacids
Brain 800 mmol/day
Kidney Oxidization 250 mmol/day Excretion 150 mmol/day
Owen et al. J Clin Invest 1967 & 1969
Infused insulin will slow the rate of ketoacid production
except initial several hours
Bicarbonate Therapy
Considered in the initial treatment of a subgroup
Patients who are expected to have a low rate of ketoacid removal
Marked decrease in their level of consciousness
Preexisting advanced renal dysfunction
Combined with normal anion gap metabolic acidosis
The decision in adult patients with diabetic ketoacidosis should be individualized and not based solely on an arbitrary blood pH value
Kamel et al. New Eng J Med 2015
Delta-delta (ΔAG/ΔHCO3-) in Metabolic Acidosis
∆AG (pts AG level - 10)/ ∆HCO3- (25 - pts HCO3
-) 1~2: pure high anion gap M.acidosis > 2 : combined with M.alkalosis < 1 : combined with non-gap acidosis
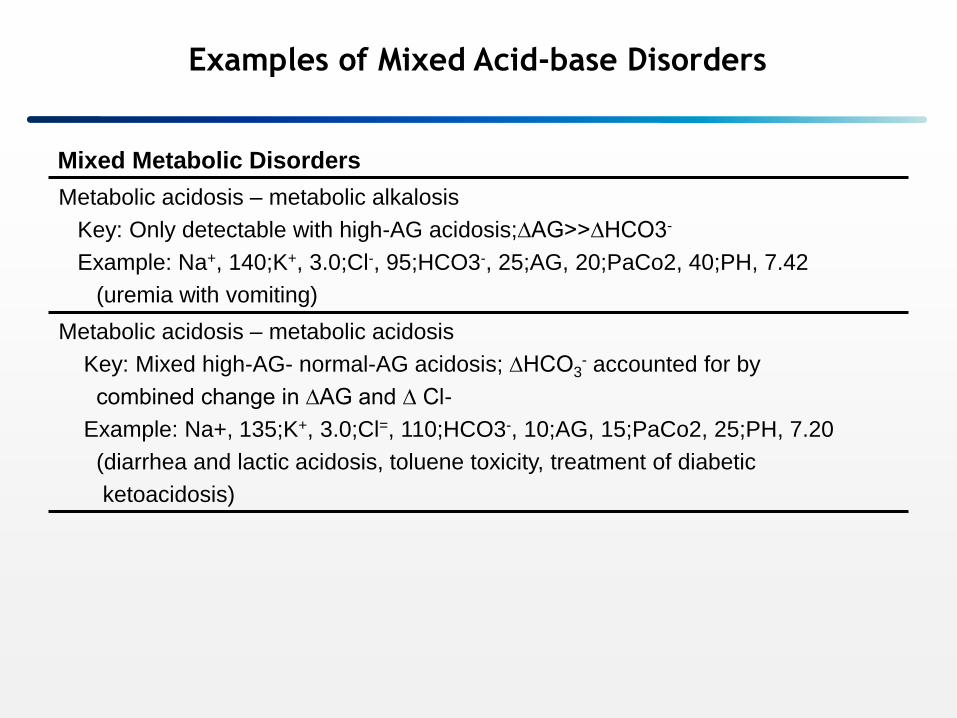
Metabolic acidosis – metabolic alkalosis
Key: Only detectable with high-AG acidosis;∆AG>>∆HCO3-
Example: Na+, 140;K+, 3.0;Cl-, 95;HCO3-, 25;AG, 20;PaCo2, 40;PH, 7.42
(uremia with vomiting)
Metabolic acidosis – metabolic acidosis
Key: Mixed high-AG- normal-AG acidosis; ∆HCO3- accounted for by
combined change in ∆AG and ∆ Cl-
Example: Na+, 135;K+, 3.0;Cl=, 110;HCO3-, 10;AG, 15;PaCo2, 25;PH, 7.20
(diarrhea and lactic acidosis, toluene toxicity, treatment of diabetic
ketoacidosis)
Mixed Metabolic Disorders
Examples of Mixed Acid-base Disorders
DKA에서는 혈장 [HCO3-]의 감소와 Anion gap 상승이 동일한 비율로
일어남에도 불구하고 실제로는 HCO3-의 결핍이 훨씬 더 심각할 수가
있다.
소아에서 뇌부종을 줄이기 위해서는 대부분의 뇌부종이 일어나는 초기의 15시간 동안에 Effective Osmolality가 떨어지지 않도록 [Na+]를 지속적으로 모니터링 하면서 free water 투여는 최소한으로 줄여야 한다.
심각한 산혈증이 나타나는 보다 주된 원인은 간에서 생성되는 Ketoacids의 증가보다는 뇌와 신장에서의 Ketoacids 제거가 감소하는 것이다. 따라서 대부분의 DKA에서 HCO3
- 의 투여는 매우 심한 산혈증이나 혈역학적으로 불안정한 경우에만 신중하게 투여해야 한다.
Summary

Thank you for your attention!
Kyungpook national university hospital since 1907
Kyungpook National University Medical Center since 2010


















