Inflammatory Bowel Diseases and Apheresis · Inflammatory Bowel Diseases Pro-Inflammatory Mediators...
21
Inflammatory Bowel Diseases and Apheresis Maurizio Vecchi University of Milan Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico
Transcript of Inflammatory Bowel Diseases and Apheresis · Inflammatory Bowel Diseases Pro-Inflammatory Mediators...

Inflammatory Bowel Diseasesand Apheresis
Maurizio Vecchi
University of Milan
Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico

Immune Response Alteration
Chronic Inflammation
Dam
age
Increase of Pro-Inflammatory
Response
Disease
Dam
age
Weak Intestinal Barrier
Intestinal Barrier Integrity Loss
Disrupted Protective Barrier Layer
Pro-Inflammatory Cytokines
Inflammatory Bowel Diseases
Pro-Inflammatory
Mediators
Anti-Inflammatory Mediators

IBD: a relapsing-remitting, possibly severe and life-threatening, chronic inflammatory disease
• Diarrhea
• Abdominal pain
• Rectal bleeding
• Extraintestinal manifestations
• Dehydration, electrolyte imbalance
• Anemia
• Perforation
• Cancer

IBD: Treatment Options
MAIN GOALS
- Induce remission (periods of time that are symptom-free);
- Maintain remission (preventingflare-ups of disease);
- Improve patient's quality of life.

IBD: Treatment Options
Infliximab
Adalimumab
Golimumab
Vedolizumab Anti-α4β7 integrin
Ustekinumab Anti-IL23/IL12
Anti TNF

Role of MAdCAM-1 and α4β7 in lymphocyterecruitment at intestinal level

IBD & APHERESIS
Leukocytapheresis - anti-inflammatory andimmunomodulatory therapy, aimed at the removal fromthe bloodstream of cells responsible for the inflammatorystate in IBD.
Leukocytes, mainly Neutrophils and MonocytesGranulocytes, and also a part of Platelets are removedfrom the blood.
Many studies have investigated the efficacy ofLeukocytapheresis as an alternative or adjuvant therapy tothe conventional pharmacological treatments of IBD.
It is currently applied in the treatment of patients withmild to moderate IBD, non-responding / intolerant or inthose with contraindications to conventional therapies.

Leukocytapheresis with Hydrophilic Polysulfone
Why Hydrophilic Polysulfone?
• Resin coated with Polyvinilpirrolidone High Hemocompatibility.
• Resin already largely used in other clinical fields: widespread use of specific resinconfigurations in nephrology.
WINCHESTER JF et al. Replacement of Renal Function by Dialysis. Springer 2002.
• Specific structure based on short hollow fibers defined for Granulocyte, Monocyteand Platelet Adsorption.

ADSORPTION CAPACITY: IN VITRO TESTS
- 9 repeated tests with healthy human blood, single- Single pass treatments- Blood sampling catridge inflow and catridge outflow.
Percentage of Reduction % :(Cout / Cin) * 100
- Cout: target population’s blood concentration in thecatridge’s outflow, after 15 min of treatment,- Cin: target population’s blood concentration in thecartridge’s inflow.
Leukocytapheresis with Hydrophilic Polysulfone
M. Di Girolamo et al. Ther Apher Dial. 2016 Dec;20(6):668-676

IN VITRO AND EX VIVO STUDIES OF TWO LEUKOCYTAPHERESIS MATERIALSHYDROPHILIC POLISULFONE AND CELLULOSE ACETATE
HAEMOCOMPATIBILITY EVALUATION
Polysulfone effects were compared to the effects of one of the most used materials in leukocytapheresis’ therapies.

Experimental SettingIn vitro tests included healthy blood, while ex vivo evaluation was performed on IBD patients’ blood
POOL
No Treat(NT)
No Treat(NT)
Acetate(AC)
Polysulfone(PS)

2,32,0
0,5
2,5 2,4
0,5
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
4,0
NT AC PS NT AC PS
30 MIN 1 H
TNFa
(p
g/m
l)
Plasma TNFa
After 1 hour contact, PS exhibited lower monocyte activationas compared to AC and NT.
Av 3 tests ± s.e.m.
6,88,3
11,0
13,612,3
7,2
0
5
10
15
20
NT AC PS NT AC PS
30 MIN. 1 H
% M
ON
OC
YTE
S C
D8
6 p
os.
BUFFY COAT
IN VITRO TESTMonocytes Activation

92,6 92,8 96,6 94,6 95,9 93,5
0
20
40
60
80
100
120
NT AC PS NT AC PS
30 MIN 1 H
% G
ran
ulo
cyte
s M
PO
Po
s.
Granulocytes – Buffy Coat
15,7 15,9 15,4 15,316,4 15,8
0
5
10
15
20
25
NT AC PS NT AC PS
30 MIN. 1H
% B
Lym
ph
ocy
tes
CD
25
Po
s.
B Lymphocytes – Buffy Coat
24,1
36,5 35,6 34,3 35,8 35,9
0
10
20
30
40
50
60
NT AC PS NT AC PS
30 MIN. 1 H
%Ly
mp
ho
cyte
s T
CD
25
Po
s.
B Lymphocytes – Buffy Coat
71,0 71,9 74,5
63,3 62,5 64,5
0
10
20
30
40
50
60
70
80
90
NT AC PS NT AC PS
30 MIN 1 H
% L
ymp
ho
cyte
s In
t. b
7 P
os.
Gut Homing Lymphocytes
NO differences between AC, PS and NT. IL-4, IFNg, IL-17, IL.-10 levels
IN VITRO TESTLymphocytes and Granulocytes Activation
Ave 3 tests. ± s.e.m.

A strong platelets reduction in PS treated samples.
PLATELETS ACTIVATION
Ave 3 tests. ± s.e.m.
55,5
67,4
25,1
54,660,3
16,3
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
NT AC PS NT AC PS
30 MIN 1 H
%C
ells
CD
62
p P
OS.
Buffy Coat
IN VITRO TEST

The Ex Vivo Results confirm minor complement systemactivation with PS, both on buffy coat and plasma C3alevels.
No differences between the treatments in terms oflymphocytes and granulocytes activation.
The capacity of PS to determine markedly reducedplatelet activation confirmed PS vs AC vs NT (46.4±9.3vs. 69.3±6.8 vs. 70.8±5.6%)
EX VIVO TEST
68,6
55,567,4
25,1
54,6
60,3
16,3
0
10
20
30
40
50
60
70
80
TO NT AC POLI NT AC POLI
30 MIN 1 H
% P
late
lets
CD
62
p P
OS.
Platelets Activation – Buffy Coat
Ave 3 tests. ± s.e.m.

And what about clinical experience of polysulfone Leukocyteapheresis in IBD?

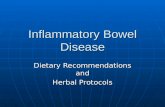
Leukocytapheresis with Polysulfone in IBDPROMISING CLINICAL RESULTS: PILOT STUDY
- 10 UC, 8 CD non-responder to conventional therapy (CCS, Tiopurine, Anti-TNFα) with mild/moderate activity.
-8/18 with Extra-Intestinal manifestations
- Standard Protocol (1 session/week for 5 weeks; 30 ml/min blood flow for 60 min); 1 year follow up.
M. Di Girolamo et al. Ther Apher Dial. 2016 Dec;20(6):668-676
Efficacy of a Novel Granulocyte Monocyte Apheresis Adsorber Device in the treatment of Inflammatory Bowel Diseases: a Pilot Study

Leukocytapheresis with Polysulfone
M. Di Girolamo et al. Ther Apher Dial. 2016 Dec;20(6):668-676
*2 drop out
0,00
2,00
4,00
6,00
8,00
10,00
12,00
14,00
16,00
1 2 6 7 8 11 13 14 16 17
MAYO SCORE Baseline
T3
F1S
F1M
F6M
F12M
0,00
50,00
100,00
150,00
200,00
250,00
300,00
350,00
3 4 9 10 12 15
CDAI SCORE Baseline
T3
F1S
F1M
F6M
F12M
- Clinical Benefits achieved in all (16) patients who completed the treatment during the study
- Diseases Activity Indexes Reduction registered (Mayo Score 9,4±1,43 vs 5,1±1,44; CDAI 209,5±31,36 vs 68,33±24,83)
- No adverse effects registered
PROMISING CLINICAL RESULTS: PILOT STUDY

Leukocytapheresis with PolysulfonePROMISING CLINICAL RESULTS: Case Report
Patient Profile
45 y-old woman with UC
Steroid dependency & Failure to anti-TNFs
Treatment Protocol
Vedolizumab monotherapy maintenance +
Leukocytapheresis standard protocol
Results
No adverse events.
Azathioprine stopped.
Clinical Symptoms Improvement after 4th apheresis session.
Steriod-free remission at 6th month of follow-up
The adjunct of apheresis to biologics could represent a valid option in UC patients
difficult to treat.

Therapy Administration
Standard Treatment Schedule:1 session/week60 min/session, 30 ml/min -> 1.8L/session of blood5 weeks
Attempt to personalized management based on patients’ profiles
IBD & APHERESIS
CONVENTIONAL STANDARD THERAPY SCHEDULE
A need to use Different Treatment Doses in order to obtainbetter Efficacy

Tomorrow Insights
Beyond the current knowledge….
…….Patient-Tailored, Diversified, Treatment Schedules:
1. The Dose-Effect Concept validation: towards thePersonalization of Leukocytapheresis Treatment.
2. Use of Leukocytapheresis in a Combination therapy with mAb:
a Synergistic action of pharmacological and apheretictreatment.