Impact of DM and its control on the risk of developing TB in Taiwan
44
The Impact of Diabetes Mellitus and Its Control on Developing Tuberculosis: A Nationwide Longitudinal Study in Taiwan 加加加加加加加加 1
-
Upload
ming-chia-lee -
Category
Health & Medicine
-
view
301 -
download
2
Transcript of Impact of DM and its control on the risk of developing TB in Taiwan

The Impact of Diabetes Mellitus and Its Control on Developing Tuberculosis: A
Nationwide Longitudinal Study in Taiwan
加護病房查房日誌
1

Outlines
• Background• Material and methods• Results• Discussion• Conclusions• Future works
2

Background
3

Global Burden of Tuberculosis
4
2 billion people are estimated to be infected with Mycobacterium tuberculosis (TB).
1/3
In 2014, estimated 9.6 million new cases of TB,1.5 million people died from TB.
Reference: World Health Organization: Global Tuberculosis Report. In Book Global Tuberculosis Report City: World Health Organization; 2015.
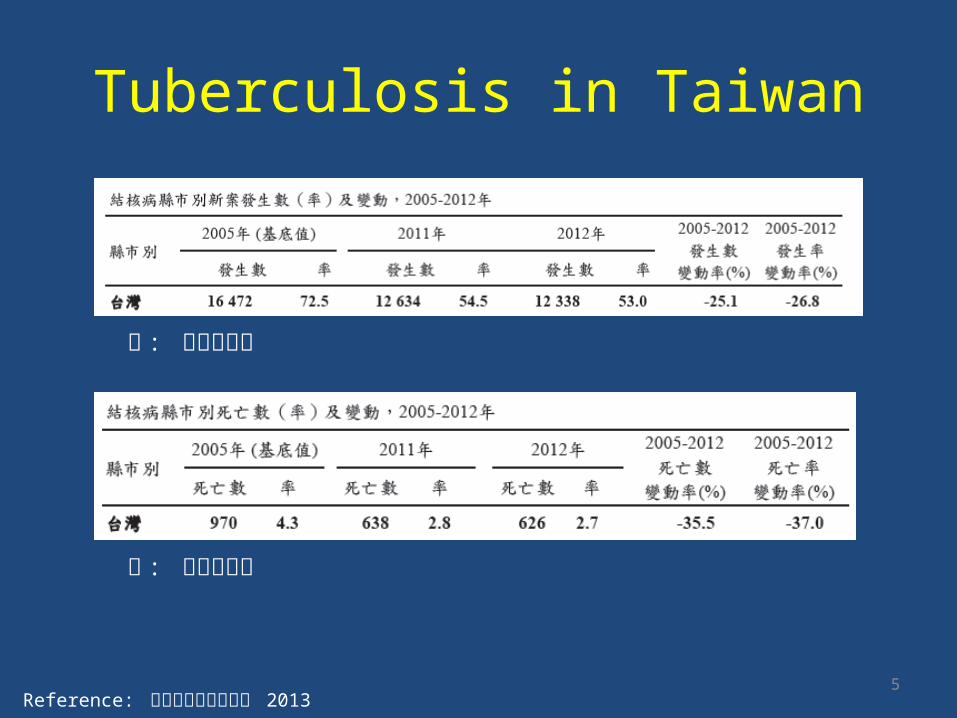
Tuberculosis in Taiwan
5Reference: 台灣結核病防治年報 2013
率 : 每十萬人口
率 : 每十萬人口

Risk Factors of TB
• Age• Male gender• Low socioeconomic
status• Malnutrition• Substance abuse• Silicosis• Human
immunodeficiency virus infection (HIV infection)
• Malignancy• Diabetes
• Relative risk or hazard ratio: 1.6 to 6.8
• Renal disease• Celiac disease• Gastrectomy• Transplant• Corticosteroids• Tumor necrosis factor
inhibitors
6Reference: C Robert Horsburgh Jr. MD, MUS. Epidemiology of turberculosis. In: UpToDate, Elinor, LB MD (Ed), UpToDate, Waltham, MA, 2013

Epidemiology of Diabetes Mellitus (DM)
7
422 million adults had diabetes, Prevalence Rate: 8.5 % 8.4 % in W Pacific
8.3 % in the Americas 7.1 % in Africa 8.6% in South-East Asia
7.3 % in Europe
Reference: World Health Organization: Global Report on Diabetes; 2016.
10 % in Taiwan, 2015

DM control vs. TB-1
The evidence is lacking
Reference: CC Leung et al, American Journal of Epidemiology 2008, 167: 1486-1494
HbA1C >=7% vs. no DM: Active TB: RR 1.97 (95% CI 1.51-2.57)

DM control vs. TB-2No evidence for any association between TB and dysglycemiaIn the low TB-burden country of Denmark
Reference: A Leegaard et al, Diabetes Care 34:2530–2535, 2011

Taiwan’s National Health Insurance Research Databases
Strength• Large sample size
– 97% of Taiwan’s population
• Relatively inexpensive• Real-world practice
– Medical service utilization– Prescription drug use
• Longitudinal histories
Weakness• Over-the-counter drugs?• A secondary database• Lag time• Disease severity?• Laboratory data?
10Ref: Journal of Food and Drug Analysis, Vol 15, No. 2, 2007, Pages 99-108

11
Impact factor: 2.908, Ranking: Pharmacology & Pharmacy 81 out of 253, 32 %

Purpose
• To investigate the impact of DM and its control on the risk of developing active TB– The National Health Insurance Research
Databases(NHIRD)– Time-dependent Cox proportional hazards models
12

Materials and Methods
Approved by the Research Ethics Committee (REC) of National Taiwan
University Hospital(NTUH REC: 201112111RIC)
13

Data Source
14
the Longitudinal Health Insurance Database (LHID) 2005From 1996 to 2007
DM vs. non-DM(case-control study, Age, sex and time of entry,1:1 in case number) DM and co-morbidities
The risk factors for developing TB
Among DMA Time-dependent approach DM medications adherence(weakness: no lab data (HbA1c) )
All selected cases were followed up until active TB developed, 31 Dec. 2007 or lost to follow up
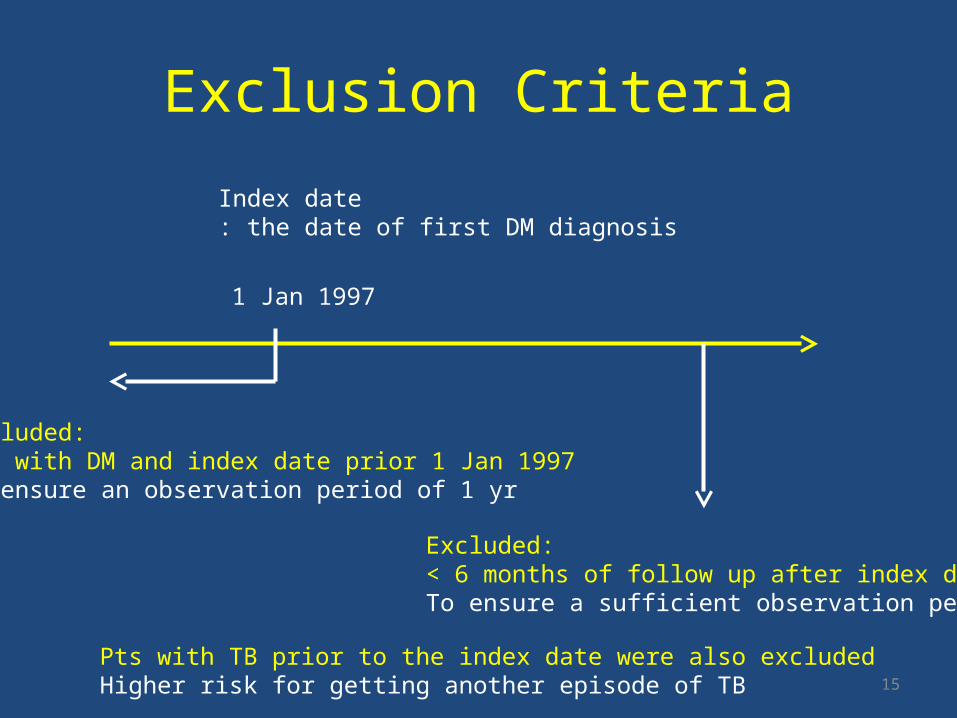
Exclusion Criteria
15
Index date: the date of first DM diagnosis
1 Jan 1997
Excluded: Pts with DM and index date prior 1 Jan 1997To ensure an observation period of 1 yr
Excluded: < 6 months of follow up after index dateTo ensure a sufficient observation period
Pts with TB prior to the index date were also excludedHigher risk for getting another episode of TB

Definition of DM or TB
16
ICD9: 250A code: A181Exclude gestational diabetes
ICD9: 010-018A code: A020,A021
Anti-TB medications:Isoniazid, ethambutol, rifampicin, pyrazinamide…etc.

Co-morbidities• Malignancy• End-stage renal disease (ESRD)• Chronic obstructive pulmonary disease (COPD)• Pneumoconiosis• Liver cirrhosis• Autoimmune diseases• Acquired immunodeficiency disese• The low income group
– Annual household income < 4,500 US dollars
17Ref: PLoS One 2012; 7: e37978.

Statistical Analysis-1• Part 1 (case control)
– Inter-group differences• Numerical variables: independent samples t-test• Categorical variables: chi-square or Fisher’s exact test
– Curves of time-to-active TB• Kaplan-Meier method and the log-rank test
– Factors for developing TB• Cox-regression analysis
– Sensitivity analysis• In different sub-population with different follow-up duration
18

Statistical Analysis-2• Part 2 (Among DM patients)
– Factors for developing TB• The time-dependent Cox proportional hazards model
– Time-dependent variables: » Age, co-morbidities, use of systemic corticosteroids, oral
hypoglycemic agents (OHAs), and insulin, » Adherence to anti-DM medications, DM associated admissions
– Time-independent variables: sex
– Sensitivity analysis• DM pts need > 90 days of DM medications
• All analyses were performed by using the SAS
19

Factors During Time Segment
20
TB event date-90 days-270 days
• OHAs: defined daily doses (DDDs)• Adherence to anti-DM medication, continuous variable, 0 to 1
• The proportion of days covered by anti-DM medication prescribed at the outpatient clinic within 270-day time segment
• The average OHA daily dose• The number of days covered by systemic corticosteroids• The maximum average daily dose (MADD)
• The maximum of the average doses of OHAs and insulin for every 90 consecutive days
• Insulin use• Insulin dose during admission and the outpatient clinic (continuous variable)• Insulin use during admission and at the outpatient clinic (categorical variable)
• The number of admissions with compatible DM diagnoses

Delayed Diagnosis of TB and Reactive Hyerglycemia
• Two sensitivity analyses– Risk factors for developing of TB > one years after
the diagnosis of DM– The 270-day time segment
• 360 to 90 days, 450 to 180 days prior to each outcome event
21

Results
22

Selected Sample Size
23

Part 1
DM vs. non DM
24

Characteristics of Patients with DM and the Control Subjects
25
Age 61.9±14.2 yrsMore DM patientsdeveloped TB

Curves of time to active TB among DM patients and control
26

Factors associated with TB in DM patients
27

Sensitivity Analysis
28

Part 2
Among DM patients
29

DM cases with or without TB
30
Age 63.6±13.2 yrsMale dominance
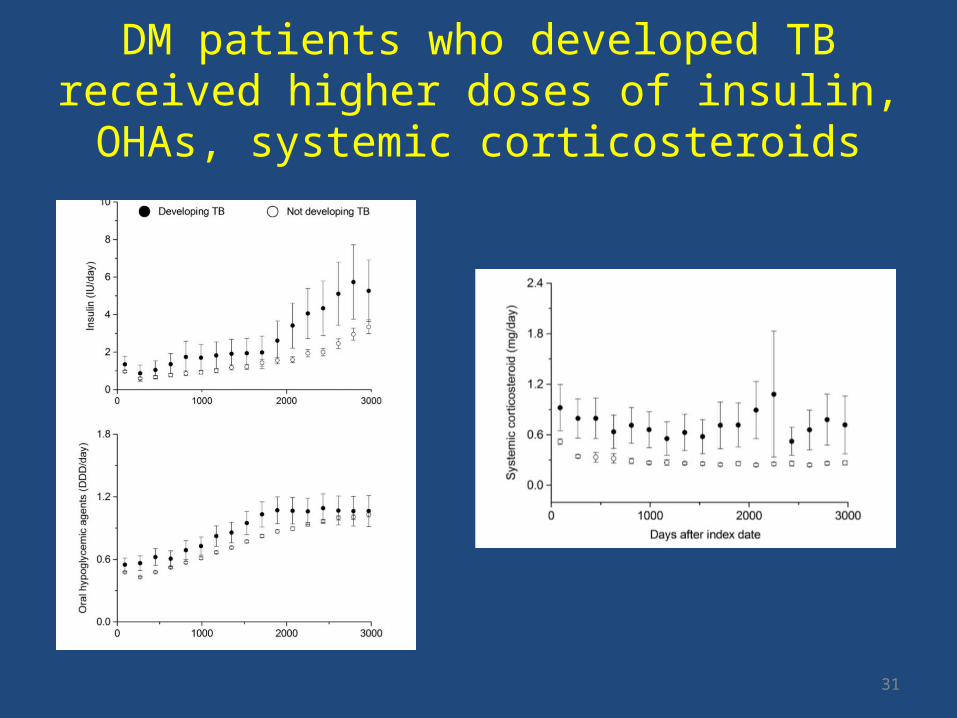
DM patients who developed TB received higher doses of insulin, OHAs, systemic corticosteroids
31

Time-dependent Cox proportional hazards analysis
32
Sensitivity analysis
•Sensitivity analyses revealed the same results1. developing TB more than 1 year after the diagnosis of DM2. the 270-day time segment to from 450 days to 180 days prior to each outcome
Discussion
• Three major findings– DM is an important risk factor of TB, and its effect
persists for at least 5 yrs– The risk of TB parallels the severity of DM
• Measured by the number of DM-related admissions, MADD of OHA and insulin use during admission
– Some cases of TB may be prevented by promoting adherence to anti-DM medication
33

Increased the Risk of TB in DM Patients
• Risk in previous studies: 1.48 to 6.8– Our study: 1.293 (1.154-1.449)– Taiwan’s 2001 National Health Interview Survey: 2.09
(1.10-3.95)• Pros: including environmental, educational and socio-
economic conditions• Cons: no autoimmune disease, malignancy, ESRD, liver
cirrhosis
• Mechanisms– The compromised immune response in diabetic pts
34Ref: 1. Lancet Infect Dis 2009; 9: 737–746. 2. Clin Infect Dis 2012; 54: 818–825. 3. Clin Infect Dis 2008; 47: 634–641

OHA and insulin
• Previous studies:– Insulin dependence is a marker of disease severity
and predictive of increased risk of TB• The daily dose of OHA and insulin continued to
increase after DM was diagnosed.• Higher daily dose of OHA
– Worse therapeutic response and longer duration of DM
– Increase the risk of developing TB
35Ref: Am Rev Tuberc 1952; 65: 1–50.. Trop Doct 1990; 20: 147–150.

DM-associated Admissions and Insulin
• Higher HbA1c: higher risk of admissions • Insulin use during admission
– A surrogate maker of poorly controlled DM• DM-associated admissions
– Diabetic ketoacidosis and non-ketotic hyper-osmolar syndrome
– Poor DM control– Increase the risk of contact with TB cases
36Ref: 1. Arch Intern Med 1999; 159: 2053–2057. 2. Arch Intern Med 1997; 157: 669–675. 3. Clin Chest Med 1989;10: 397–405.

Insulin Dose during Admission or the Outpatient Clinic
• Those are not independent risk factors– Higher dose reflects a more aggressive use of
insulin– A higher probability of good sugar control
37

Delayed TB Diagnosis
• Similar final statistical models: – Sensitivity analysis of developing TB > one years
after diagnosis of DM– Adjusting the 270-day time segment prior to each
outcome event• Suggest that delayed TB diagnosis and
reactive hyperglycemia – NOT alter the impact of DM and its control on the
risk of TB
38
The Protective Effect of Adherence to Anti-DM Medications
• Even greater in DM pts frequently requiring anti-DM medication
• Poor adherence to anti-DM treatment– Poor diabetes control– Increased susceptibility to infection
• Similar results in Hong Kong– HbA1c > 7 %
39Ref: 1. Clin Ther 2011; 33: 74–109 . 2. Diabetes Care 2008; 31: 916–921 3. QJM 2007;100: 345–350 4. Am J Epidemiol 2008; 167: 1486–1494.

Other Risk Factors
• Age: lower HR than that of Baker’s study– The prevalence of underlying co-morbidity and
the number of DM-associated admissions often increased as age increases
• Male sex, COPD, DM, ESRD and the use of systemic corticosteroids are also well-known predisposing factors of TB– Smoking (not available in NHIRD), TB and COPD
40Ref: 1. Clin Infect Dis 2012; 54: 818–825. 2. Am J Respir Crit Care Med 2009; 180: 475–480. 3. Am J Respir Crit Care Med 2007; 176: 532–555 4. Semin Dial 2003; 16: 38–44.

Limitations• Lack of culture and laboratory data for the diagnosis
of TB– Diagnosis of TB has been verified– Sensitivity analysis
• Without lifestyle information– DM patients may quit smoking and drinking after diagnosis– It may reduce the risk of TB
• Using adherence, not HbA1c to measure DM control– Prospective clinical studies
41Ref: PLoS One 2012; 7: e37978.

Conclusions
• This study confirms the association of DM and TB and complements previous reports by showing that the risk of developing TB parallels the severity of DM.
• Some cases of TB can be prevented by promoting adherence to anti-DM medication.
• Healthcare providers should keep a high index of suspicion and periodically screen for active TB in DM patients.
42

Another Study
43Ref: PLOS Medicine | DOI:10.1371/journal.pmed.1002072 August 9, 2016

Thank you for your listening
44