BLOOD AND BLOOD PRODUCTS TRANSFUSION IN OBSTETRICS AND GYNECOLOGY

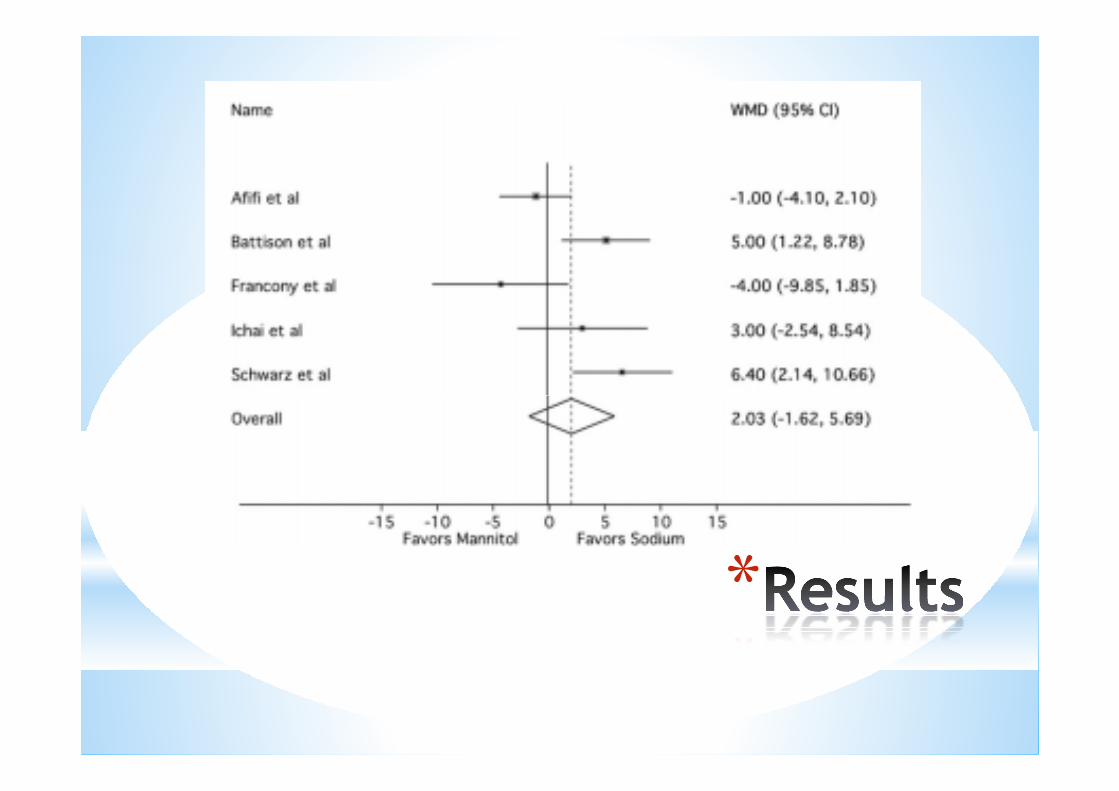
Hypertonic saline versus mannitol for the treatment of elevated intracranial pressure: A meta-analysis of randomized clinical trials
Hooman Kame et al. Crit Care Med 2011 Vol. 39, No. 3本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權
*Mannitol, recommended first-line osmotic agent for the treatment of intracranial hypertension
*Numerous studies have shown that mannitol is effective in decreasing ICP
*Reduces mortality compared to barbiturates in patients with elevated ICP from TBI
*
*Adverse effects: renal failure & hypovolemia
*Hypertonic saline (HS), can reduce ICP without causing volume contraction and with less risk
of nephrotoxicity
*Several RCTs have suggested that sodium-based hypertonic solutions may be superior to
mannitol in reducing ICP
*
*
*Limited impact on clinical practice
* different specific formulations, small size studies
*To better understand the relative efficacy of these two forms of osmotic therapy, we
performed a meta-analysis of randomized
clinical trials comparing hypertonic sodium
solutions and mannitol for the treatment of
elevated ICP
*
*Inclusion Criteria:
*Randomized clinical trials
*Quantitative ICP measurement
* IICP without regard for the underlying cause
*Formulation containing at least 3% sodium chloride or equivalent
*Exclusion criteria:
*
*Exclusion criteria:
*varying doses or varying infusion times
*Data Sources:
*Various databases
*any language
*January 1967 ~ April 2010
*Primary outcome:
*
*Primary outcome:
*proportion of cases in which randomized drug administration resulted in control of ICP
*Five studies
*112 patients
*184 episodes of IICP were treated
*absence of blinding
*

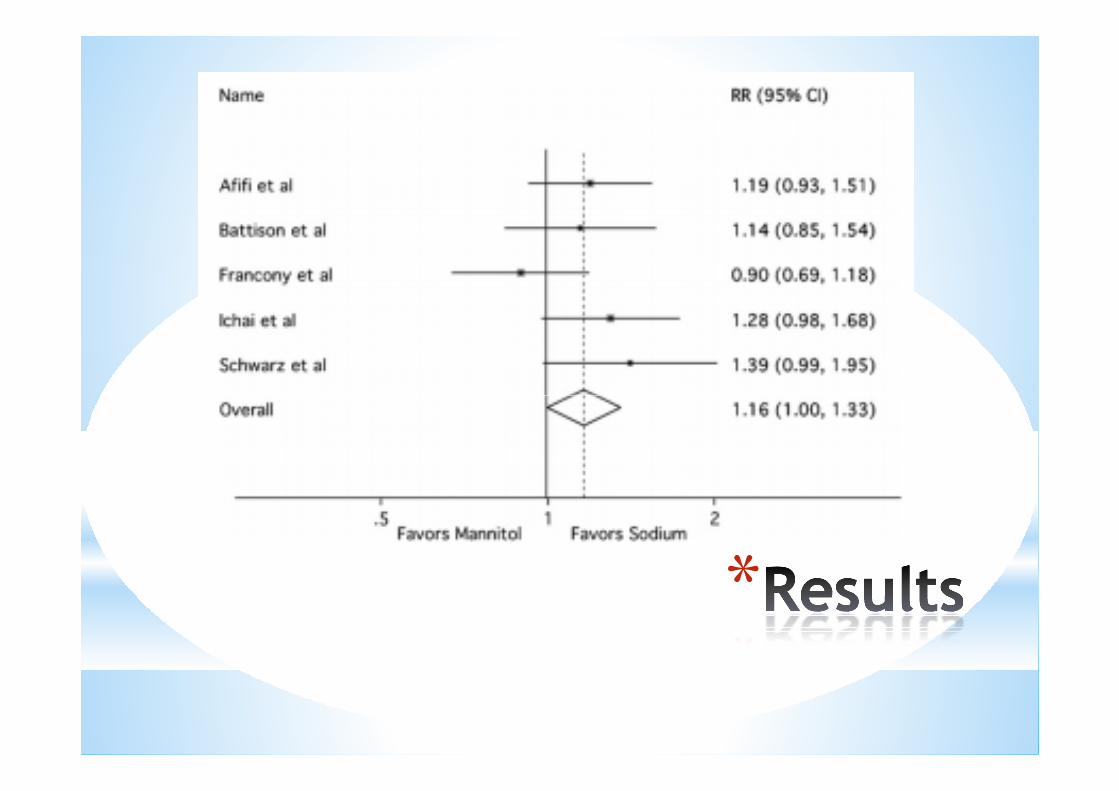
*IICP control:
Mannitol - 69 / 89 (78%)
HS - 88 / 95 (93%)
*
*
*Prespecified tests indicated a mild degree of heterogeneity
*No pediatric trials
*Did not perform subgroup analysis based on the type of intracranial pathology
*Another prespecified subgroup analyses: no clear differences in effect size
*
differences in effect size
*Hypertonic sodium solutions are more effective than mannitol in controlling episodes of
elevated ICP
*greater quantitative ICP reduction
*Quantitative ICP reduction:
*HS: 2, 1 trend
*
*HS: 2, 1 trend
*Mannitol: 1
*Equivalent: 1None individually were sufficiently powered to show a difference
*Primary outcome: clinical definition of ICP control
*a more clinically relevant end point than the mean quantitative decrease in ICP
*Lack of a uniform treatment effect among all the trials is not surprising
*

*1 trial failed to show a trend favoring HS
*no obvious methodological differences
*smallest study
*effect of chance
* 7 observational studies demonstrating the effectiveness of HS in lowering ICP after failure of
standard mannitol therapy
*

*Another observational study found no significant difference between the efficacy of
mannitol and hypertonic saline, but the latter
had a longer lasting effect
*2 randomized trials that did not meet our inclusion criteria support the superiority of
hypertonic saline therapy
*
hypertonic saline therapy
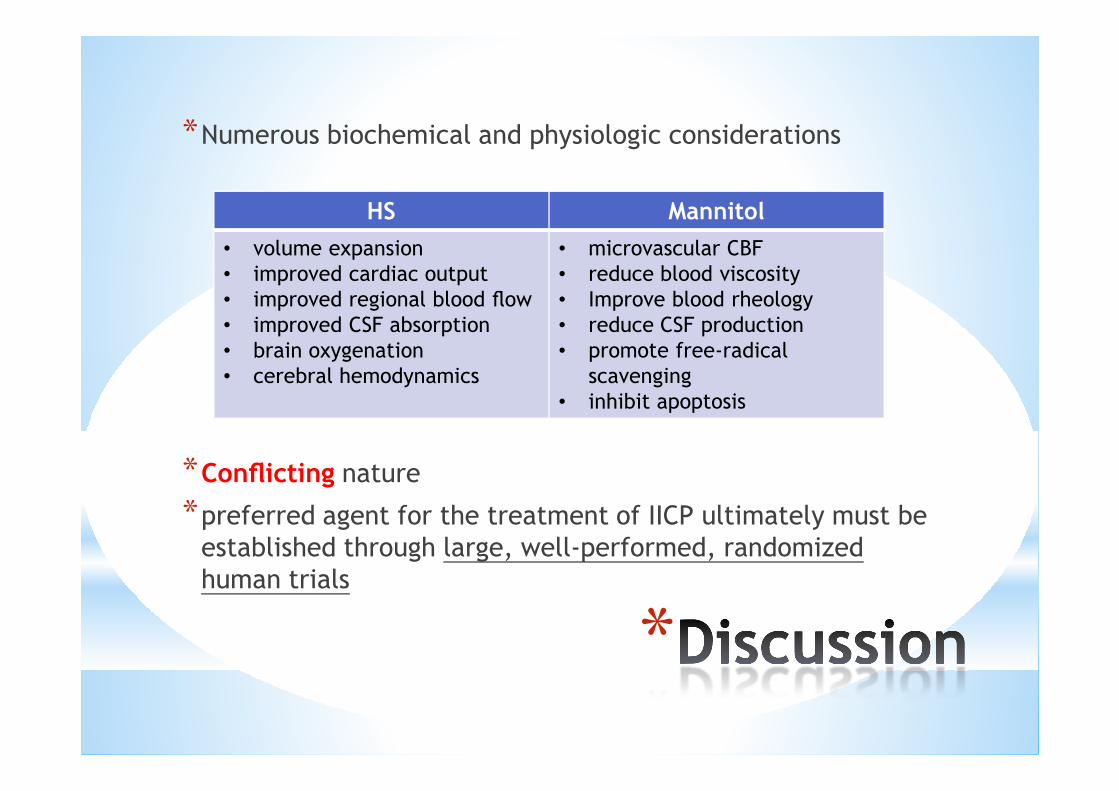
*Numerous biochemical and physiologic considerations
HS Mannitol
• volume expansion
• improved cardiac output
• improved regional blood flow
• improved CSF absorption
• brain oxygenation
• cerebral hemodynamics
• microvascular CBF
• reduce blood viscosity
• Improve blood rheology
• reduce CSF production
• promote free-radical
scavenging
• inhibit apoptosis
*
*Conflicting nature
*preferred agent for the treatment of IICP ultimately must be established through large, well-performed, randomized
human trials
• inhibit apoptosis
*Limitations
* small number and size of eligible trials
* methodological differences
* lack of rigorous adverse event reporting
* failure to control for clustering among patients
receiving multiple doses of study drug
*
*Preclude a firm recommendation to
preferentially use hypertonic saline as first-line
therapy
*hypertonic sodium solutions are, on average, superior to mannitol for the treatment of
elevated ICP
* large multicenter study comparing these two
therapies
*
*absolute effect size: 15% in favor of HS
*100 patients in each arm
* 80% power to detect this difference in the rate
of ICP control between the two groups
* uniform hypertonic sodium solution
* include assessment of long-term neurologic
*
* include assessment of long-term neurologic
outcomes
Discussion