
FullText.99pdf
31
Title Bacille calmette-Guerin (BCG) associated lymphadenitis Author(s) Ho, Po-ki, Polly; 何寶琪 Citation Issued Date 2011 URL http://hdl.handle.net/10722/173732 Rights Creative Commons: Attribution 3.0 Hong Kong License
description
theses
Transcript of FullText.99pdf
Title Bacille calmette-Guerin (BCG) associated lymphadenitis
Author(s) Ho, Po-ki, Polly; 何寶琪
Citation
Issued Date 2011
URL http://hdl.handle.net/10722/173732
Rights Creative Commons: Attribution 3.0 Hong Kong License
1
Bacille Calmette-Guérin(BCG) associated lymphadenitis
By
Ho Po Ki
1999119193
Department of Paediatrics
Queen Elizabeth Hospital
This work is submitted to
Faculty of Medicine of The University of Hong Kong
In partial fulfillment of the requirements for
The Postgraduate Diploma in Infectious Diseases, PDipID (HK)
Date: 30.6.2011
Supervisor: Dr V Cheng
2
Declaration
I, Ho Po Ki, declare that this dissertation represents my own work and that it has not
been submitted to this or other institution in application for a degree, diploma or any
other qualifications.
I, Ho Po Ki, also declare that I have read and understand the guideline on “What is
plagiarism?” published by The University of Hong Kong (available at
http://www.hku.hk/plagiarism/) and that all parts of this work complies with the
guideline.
Candidate: Ho Po Ki
Signature:
Date:
30.6.2011

3
Abstract
Background: Excluding local reaction, regional lymphadenitis is the most common
adverse events after BCG vaccination. It is the development of ipsilateral regional
lymph node enlargement following BCG vaccination. Some progress to suppuration.
If left untreated, suppurative lymphadenitis frequently ruptures with sinus formation,
ending in prolonged course of illness and scaring.
Objective: To describe the clinical features and outcome of children with suppurative
lymphadenitis after BCG vaccination. To identify factors associated with the duration
of healing and scarring formation.
Method: Patients diagnosed suppurative BCG lymphadenitis in a tertiary paediatric
centre from January 2004 to April 2011 were identified. Data on demographics,
clinical features, treatment received and outcomes were retrieved from medical
records.
Results: There were 15 cases of BCG suppurative lymphadenitis during the period.
11(73.3%) were males. All had their BCG vaccinated at birth. The mean age of
presentation was 5.8±6.6 months (median 3 months). All presented with a solitary
swelling over ipsilateral axilla(80%) or supraclavicular region without systemic
symptom. The mean size of lymph nodes were 2.1cm±0.8cm times 1.8cm±0.8cm. All
except 1 had a normal chest X-ray. The mean total white cell counts and mean

4
lymphocyte counts were 13.0x109/L and 7.3x109/L respectively. 7/13(53.8%) patients
were smear positive for acid-fast bacilli and 2/13(15.4%) were culture positive for
Mycobacterium bovis. 12(80%) patients had single needle aspiration performed while
the other 3 patients did not receive intervention. No patient required surgical excision.
5(33.3%) patients had spontaneous rupture and discharge. 2(13.3%) patients had sinus
formation with persistent discharge for long duration. All patients completely healed
subsequently. The mean duration of complete healing was 4.5 ± 1.7 months.
8/13(61.5%) patients had subsequent scarring. The duration of healing was not
associated with sex, age, time since BCG vaccination, white cell and lymphocyte
count, site of lymph node, size of lymph node, presence of spontaneous rupture, sinus
formation or needle aspiration. The size of lymph node at presentation was
significantly larger in patients with scarring (2.4±0.8cm vs. 1.3±0.4cm, p=0.026). On
the other hand, sex, age, site of lymph node, white cell and lymphocyte count,
presence of sinus formation, spontaneous rupture, needle aspiration and duration of
healing showed no correlation with scarring.
Conclusion: Suppurative lymphadenitis is not an uncommon complication of BCG
vaccination. The diagnosis is clinical and should be suspected in children present with
ipsilateral axilla, occasionally supraclavicular lymph node enlargement with history of
BCG vaccination. A chest X-ray is recommended for all patients while tuberculin skin
5
test has no diagnostic use. The low positive microbiological yield in aspirate
highlights that negative smear or culture does not rule out the diagnosis. Needle
aspiration is safe and is the main stay of treatment. Surgical excision is reserved for
those who failed repeated needle aspirations. The size of lymph node was
significantly associated with subsequent scarring formation.
(468 words)
6
Background
Bacille Calmette-Guérin (BCG) vaccine is one of the most widely used vaccine
worldwide. It has been used to prevent tuberculosis since 1921 and included as part of
the immunization programme of the World Health Organization since 1974. It was
proven to be effective against tuberculous meningitis and disseminated tuberculosis,
with an estimated efficacy of 64% and 78% respectively. [1] BCG vaccine was
incorporated in Hong Kong’s routine newborn immunization programme. Over 99%
of babies in Hong Kong receive the vaccine at birth. Besides newborns, BCG
vaccination is also recommended for children aged less than 15 who reside in Hong
Kong and do not have BCG vaccination before. [2] BCG vaccine is a live-attenuated
vaccine derived from bacterial isolate of Mycobacterium bovis, which is cultured in
vitro for many years. There are many strains and strength of BCG vaccine. Different
strains were noted to have varied potency and complications rate. One of the common
strains used in Hong Kong is the Copenhagen strain 1331.
BCG vaccine carries a low risk of serious complications and is regarded as a
safe vaccine. [3] Mild local reactions in terms of erythema or induration are the most
common adverse events following BCG vaccine. Ulceration and abscess formation
are serious yet uncommon local complications. Following local reaction, regional
lymphadenitis is the second most common adverse events associated with BCG

7
vaccination. A recent prospective large scale study involving a 12-month cohort
follow up of 2435 BCG-vaccinated children found that the incidence of local
erythema, induration and lymphadenitis were 12.4%, 12.2% and 0.1% respectively.
[4]
BCG lymphadenitis is the development of ipsilateral regional lymph node
enlargement following BCG vaccination. Indeed, the BCG starts to multiply quickly
at the site of infection and transported through the lymphatic systems to regional
lymph nodes after inoculation, causing enlargement of the corresponding lymph
nodes. Slight subclinical enlargements of lymph nodes are common after BCG
vaccination and they regress spontaneously without treatment. Unfortunately,
standardized criteria to define what constitutes a pathological BCG lymphadenitis are
lacking. It is commonly regarded as the enlargement of lymph nodes that are large
enough to be easily felt and cause parental concern. [5] BCG lymphadenitis can be
broadly classified into two groups: non-suppurative and suppurative. Non-suppurative
lymphadenitis either regresses spontaneously within weeks without medical
intervention, or progresses to development of suppuration to form the latter. Singla
and coworkers found 85% of patients had spontaneous regression of BCG
lymphadenitis while the remaining 15% progress to suppuration. [6] If left untreated,
suppurative lymphadenitis frequently ruptures with sinus formation, leaving scaring

8
and even keloid formation. Moreover, it is associated with an unpleasant and
prolonged course of illness. In the present study, we focus on the analysis of
suppurative BCG lymphadenitis in our locality, as non-suppurative lymphadenitis
carries little clinical significance.
9
Objective
The present study aims to describe the clinical features and outcome of children
with suppurative lymphadenitis complicating BCG vaccination. The factors
associated with the duration of healing and subsequent formation of scarring are also
explored. Furthermore, current literature on BCG lymphadenitis is reviewed.
10
Methodology
We identified patients with suppurative BCG lymphadenitis in a tertiary
paediatric centre Queen Elizabeth Hospital from January 2004 to April 2011. The
diagnosis of suppurative BCG lymphadenitis was clinical, by paediatric infectious
disease specialists in the department. Data on demographics, clinical features,
treatment received and outcomes were retrieved from medical records. Copenhagen
1331 strain were universally used in the hospital, of which 1 ml reconstituted vaccine
contains 2 to 8 million colony forming units of Mycobacterium bovis. The dosage was
0.05ml administered intradermally.
Descriptive data are expressed as mean ± standard deviation. Categorical
variables are compared by Chi-square test or fisher exact test where appropriate.
Independent sample T-test or Mann-Whitney U test is used to compare variables
between patient with and without scarring. Pearson’s correlation coefficient or
Spearman correlation coefficient is used to explore associations between variables and
healing time. SPSS 16.0 is used for statistically analysis. A p value of <0.05 is
regarded as statistically significant.
11
Results
There were 15 cases of BCG suppurative lymphadenitis presented during the
period from January 2004 to April 2011. 11(73.3%) of them were males. All of them
received BCG vaccination at birth. The mean age of presentation was 5.8±6.6 months
(median 3 months). The mean duration of onset after vaccination was 5.8±6.6 months
(median 3 months). The age of presentation ranged from 2 months to 26 months of
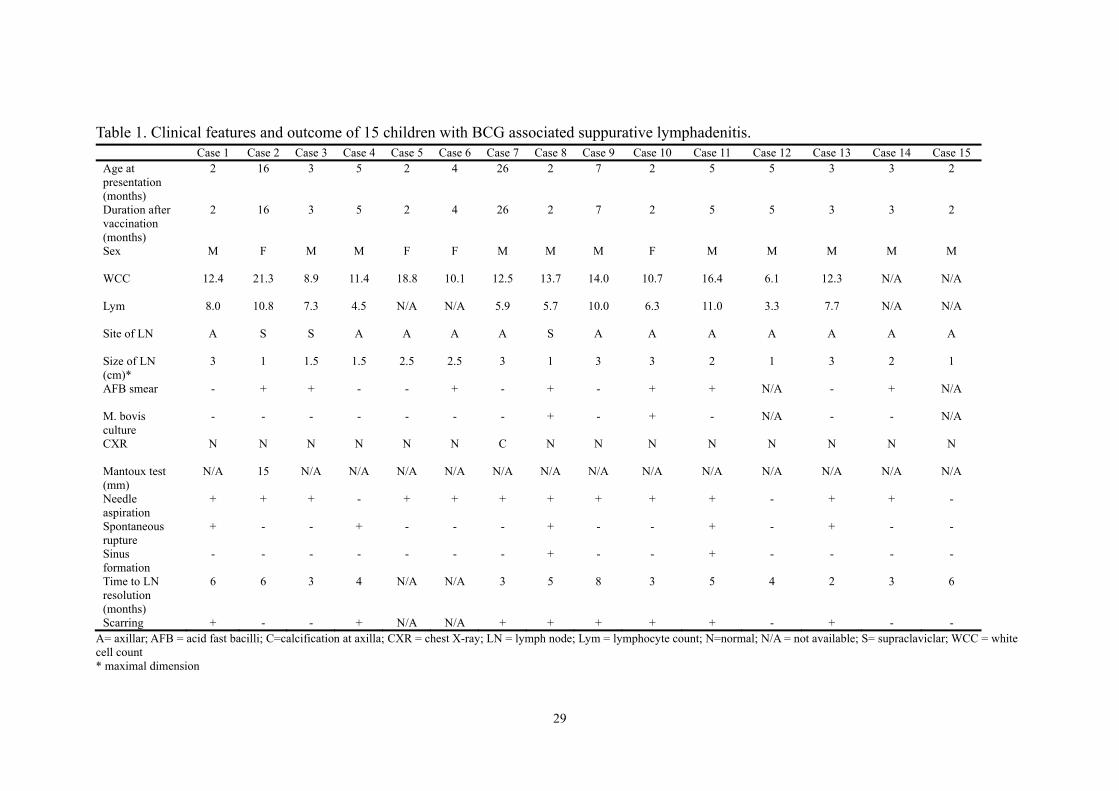
age. Table 1 summarized the clinical characteristics of the 15 patients with BCG
suppurative lymphadenitis. All patients presented with a swelling either over axilla or
supraclavicular region. The duration of symptoms of presentation ranged from 1 day
to 4 weeks. All patients were afebrile and did not have other constitutional symptom.
Their growths were normal.
Concerning about the characteristics of lymph nodes, all of them were located
over the ipsilateral side (left side) of BCG inoculation. All patients presented with a
solitary lymph node. 12 (80%) were in the axilla region, while the remaining 3 were
in the supraclavicular region. All the lymph nodes were soft, fluctuant and
accompanied with local erythema. All had absence of tenderness and local increase in
temperature. The mean 2-dimensional size of lymph nodes were 2.1cm±0.8cm and
1.8cm±0.8cm. Figure 1 demonstrated the typical appearance of a BCG associated
suppurative lymphadenitis.
12
All patients had chest X-ray performed. All chest X-rays showed no abnormal
pulmonary infiltrate or intrathoracic lymph node enlargement. 1 patient (case 7) had
calcification identified in the left axilla region from the chest X-ray. (Figure 2) The
mean total white cell counts were 13.0x109/L, while the mean lymphocyte counts
were 7.3x109/L. All cases’ C-reactive protein levels were within normal range.
Tuberculin skin test was performed in 1 patient only, which yielded a positive result at
48 hours(15mm induration). 2 patients’ lymph node discharges were unavailable for
microbiological tests as needle aspiration were not done and the lymph nodes healed
without spontaneous rupture. Among the remaining 13 cases where their discharge
were tested, 7(53.8%) were smear positive for acid-fast bacilli and 2(15.4%) yielded
positive culture for Mycobacterium bovis. No immune workup was performed in our
cases.
Referring to the treatment received, 12(80%) patients had needle aspiration
performed while the other 3 patients did not receive intervention. None had
complication regarding needle aspiration and the procedure was well tolerated. No
patient required surgical excision. None of the patients were given anti-tuberculous
drug except 1 patient whom was given 3 weeks of isoniazid by a private doctor (case
14). The anti-tuberculous drug was discontinued upon referral to our hospital.
Among the 15 cases, 5(33.3%) patients had spontaneous rupture and discharge.
13
2(13.3%) patients had sinus formation with persistent discharge for long duration. 2
patients defaulted follow up after initial presentation. All the other patients were
regularly followed up till complete resolution of the enlarged lymph nodes. The mean
duration of complete healing was 4.5±1.7 months. 8(61.5%) among the 13 patients
were complicated with scarring.
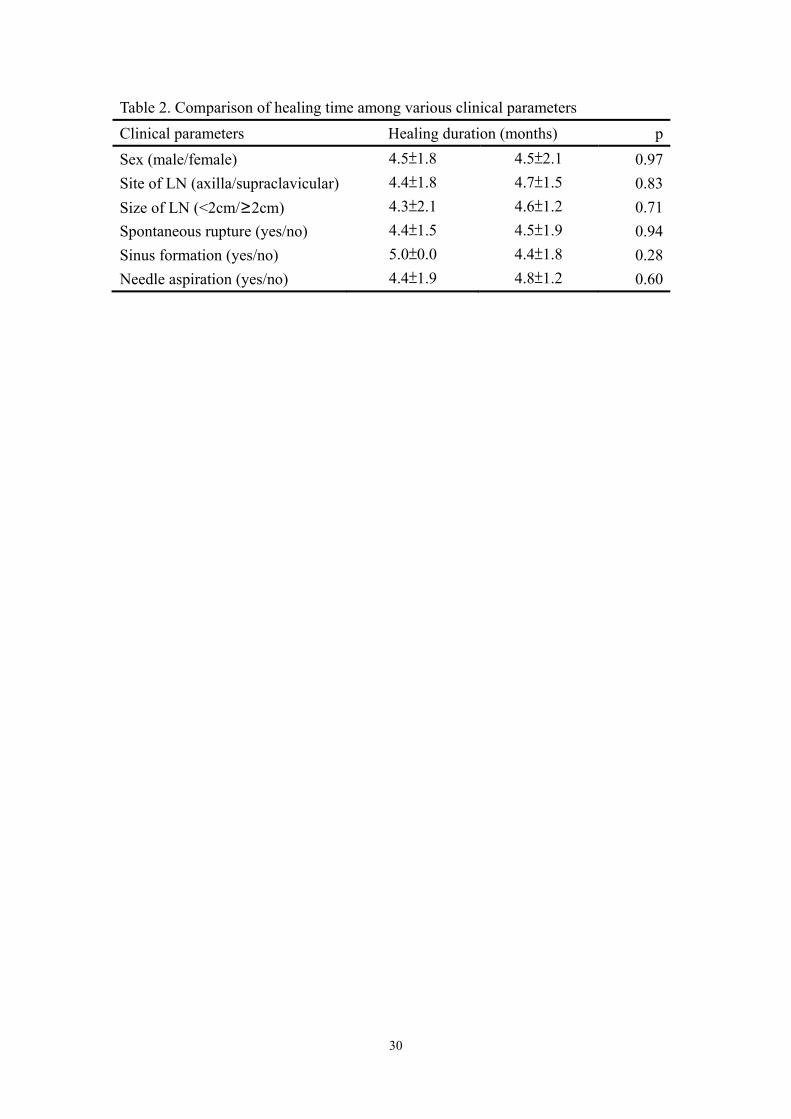
The factors associated with the duration of healing and subsequent formation of
scarring were explored. As shown in table 2, the duration of healing were compared
between patient groups stratified by sex, site of lymph nodes (axilla vs. supravicular),
size of lymph nodes (<2cm vs. ≥2cm), presence of spontaneous rupture, sinus
formation and needle aspiration. All the healing times were not significantly different
among these group stratifications. On further statistical correlation, the size of lymph
node at presentation (p = 0.66), age at presentation (p=0.96), duration since BCG
vaccination (p=0.96), white cell count (p=0.13) and lymphocyte count (p=0.10) did
not correlate with the duration of healing.
Clinical parameters were compared among patients who left with scarring and
those without. The size of lymph node at presentation was significantly larger in
patients complicated with scarring (2.4±0.8cm vs. 1.3±0.4cm, p=0.026). On the other
hand, sex(p=1.00), age at presentation(p=0.87), site of lymph node(p=0.51), white cell
count(p=0.83), lymphocyte count(p=0.89), presence of sinus formation(p=0.49),

14
presence of spontaneous rupture(p=0.075), needle aspiration done(p=0.51) and
duration of healing(p=0.92) were similar among the 2 groups. The results were shown
in details in table 3.
15
Discussion
Bacille Calmette-Guérin(BCG) lymphadenitis is one of the commonest
complication of BCG vaccination. The present study described the clinical features
and outcome of children with suppurative lymphadenitis after BCG vaccination. The
factors associated with the duration of healing and subsequent formation of scarring
were also explored.
The diagnosis of BCG lymphadenitis is largely clinical. It was suggested that
with a background history of BCG vaccination, the finding of an ipsilateral lymph
node enlargement without other identifiable cause of lymphadenitis rendered
sufficient grounds to make the diagnosis. [7] One of the major differentials is
pyogenic adenitis. The absence of increase in local temperature, tenderness,
constitutional symptoms and fever point away from the diagnosis of pyogenic adenitis,
although one should bear in mind that superimposed bacterial infection or
co-infection in BCG lymphadenitis does happen rarely. Differentiation from
non-tuberculous mycobacterial or tuberculous lymphadenitis can be challenging, but
fortunately cases presented as solitary lymph node are very scarce. The main stay of
presentation of BCG lymphadenitis is a swelling over ipsilateral lymphatic drainage
region. Multiple lymph nodes are found in rare occasions. Our findings of all patients
being presented with a solitary lymph node over ipsilateral side without systemic
16
symptom corroborated with previous studies. Previous data suggested that the mean
age of onset of BCG suppurative lymphadenitis was 2 to 4 months after BCG
vaccination, although cases presented at 24 months post-vaccination had been
reported. [5] The current study’s finding of a median duration of presentation of 3
months after vaccination, ranging from 2 months to 26 months, is consistent with the
literature. Interestingly, our study noted the supraclavicular lymph node was involved
in 20% of cases, in contrast to previous reports which stated axilla lymph node being
involved in over 95% of cases. [5] It may partly be related to the easier and earlier
identification of supraclavicular lymph nodes due to its explicit location. It had also
been proposed that the higher the BCG injection site above the level of deltoid tendon
insertion, the more likely the involvement of cervical and supraclavicular lymph
nodes. In fact, BCG injection site should always be over the insertion of the deltoid
muscle where the drainage from this region only reaches the axilla lymph nodes. The
finding of lymphadenitis in other areas like cervical or supraclavicular region signifies
faulty site of injection. However, this is difficult to verify in our study as there is no
clear documentation of site of injection in the cases.
Further investigations added little diagnostic information. Tuberculin skin test is
not helpful in making the diagnosis of BCG lymphadenitis as the test is positive with
recent history of BCG vaccination in immunocompetent patient, which corresponds to
17
the most commonly affected patient group. Furthermore, it cannot differentiate
Mycobacterium tuberculosis and Mycobacterium bovis infection as both induce a
positive tuberculin skin test result. On the other hand, the absence of tuberculin skin
test reaction in a patient with recent history of BCG inoculation should prompt
workup for underlying immunodeficiency. Indeed, routine immune workup is not
required unless in disseminated BCG infection or atypical features present. [8] A
simple chest X-ray is recommended in all cases to look for abnormal pulmonary
infiltrate or intrathoracic lymph node enlargement, which suggested disseminated
BCG disease or tuberculosis. In our study, chest X-rays were universally performed in
all our patients and were normal except 1 which we previously described. Lymph
node aspirate occasionally has positive microbiological yield, yet bacteriological
confirmation is not required to make the diagnosis. Smear of aspirate from lymph
nodes may yield acid-fast bacilli and culture may yield Mycobacterium bovis.
Although the yield of positive smear and culture is generally commented as low, the
exact data is limited. We reported a rate of 53.8% for positive AFB smear and 15.4%
for positive Mycobacterium bovis culture. These data reinforces the important concept
that a negative smear or culture cannot rule out the diagnosis of BCG lymphadenitis.
The common cytology patterns of BCG lymphadenitis are the identification of
acid-fast bacilli(AFB) in a necrotic background, granulomas with necrotic areas and

18
granulomas in a reactive lymphoid background. However, these features cannot help
distinguish BCG lymphadenitis from tuberculosis lymphadenitis as the
cytomorphologic patterns are similar in both groups. [9] As the management approach
in these 2 disease entities are entirely different, their differentiation carries significant
clinical implication. If the differentiation is difficult clinically, genetic analysis has
been tested to be helpful. It was reported that molecular assay of either oxyR or pncA
gene could be a rapid and useful tool to distinguish BCG lymphadenitis from
tuberculosis. [10]
There are several risk factors for the formation of BCG lymphadenitis. These
can broadly be divided into host related factors and vaccine related factors. The age of
vaccination is closely related to the incidence of BCG lymphadenitis. Vaccine
inoculated in neonatal period carries higher risk. [3] The presence of underlying
immunodeficiency largely increases the risk of severe BCG lymphadenitis. [11] In
fact, genetic defects in the interleukin-12 and interferon-gamma pathway have been
implicated in patients susceptible to mycobacterial cervical lymphadenopathy
secondary to BCG vaccination. [12] Another study demonstrated a significantly lower
level of total lymphocytes, natural killer cells and definite lymphopenia in patients
with BCG lymphadenitis. [13] However, we failed to demonstrate this trend as the
mean white cell count and lymphocyte count in our patients were within normal range
19
and there was no case of lymphopenia. Nonetheless, patients with severe, multiple or
recurrent BCG lymphadenitis should have their immune status investigated. Besides
immune competency, clustering of BCG suppurative lymphadenitis has been reported
in family. [14] Although congenital immunodeficiency may partly account the
association, the role of genetic factors in familial susceptibility to mycobacterial
infection needs to be addressed as well. The observed wide discrepancy in the
incidence of BCG lymphadenitis in various countries further supported the role of
genetic predisposition. Vaccine dosage, vaccine strain and vaccine administration
technique have been shown to be related to risk of BCG lymphadenitis. A classical
example was the outbreak of BCG regional lymphadenitis in Gaza in 2001. The surge
of incidence of BCG associated lymphadenitis was found to be related to the
virulence and viability of the Pasteur strain of BCG used and the faulty intradermal
injection technique. [15] The dose-response relationship was nicely demonstrated in a
Germany incident where soar in regional suppurative lymphadenitis cases was noted
after introduction of a new BCG vaccine strain (Copenhagen 1331), and it dropped
significantly after subsequent dose reduction. [16] The identification of such risk
factors plays an important role in early identification of at risk patients and
implementation of preventive measures to lower the risk.
Untreated suppurative lymphadenitis frequently ruptures with sinus formation.
20
Healing is mediated through cicatrisation and closure of the sinus. However, it is
associated with an unpleasant and prolonged course of illness, and at risk of scaring
and keloid formation. [5,17] Therefore, suppurative BCG lymphadenitis warrants
medical intervention to hasten recovery and decrease morbidity. Antibiotics like
erythromycin, [18] anti-tuberculous drugs like isoniazid and rifampicin[19] have been
found to be useful in hastening the recovery. However, these studies were
non-randomized and uncontrolled studies. Experts believe that the apparent effect of
erythromycin is probably related to its effect on gram positive cocci, which could
have complicated the infection. In fact, a meta-analysis of 4 randomized controlled
trials showed no significant difference in outcome in usage of erythromycin or
isoniazid. [20] Notwithstanding the side effects of these medications, medical therapy
is not recommended for treatment of BCG lymphadenitis. Complying with medical
evidences, use of anti-tuberculous drugs is no longer a recommended practice in our
locality. The role of needle aspiration in hastening recovery and reducing sinus
formation was verified in randomized controlled trial. As compared to controls, the
regression rate at 2 months and 6 months after presentation were significantly higher
in patients where their lymph nodes were aspirated. The rate of spontaneous drainage
with sinus tract formation was also significantly lower in the aspirated group at 6
months. [21] Needle aspiration also offers opportunity to obtain samples for

21
microbiological tests. Repeated needle aspirations were shown to be effective in
patients who failed the initial aspiration attempt. [22] In our study, the duration of
healing was shorter in the aspirated group than non-aspirated group. However, the
difference did not reach a statistical significance probably related to the limited
sample size and power of the study. Surgical excision of whole lymph node was
shown to be effective in shortening the duration of illness. [23] However, the surgical
and anaesthetic risks outweigh its benefits that it should not be regarded as the first
line treatment for suppurative BCG lymphadenitis and generally reserved for cases
who failed repeated needle aspiration attempts, the lymph nodes were multiloculated
or matted, or when draining sinus already established. [7] Incision and drainage is not
recommended as this modality is associated with inadequate clearance of
inflammatory materials, persistent drainage, delayed healing and scarring. [24]
The present study offers an overview of the clinical features and outcomes of
BCG associated suppurative lymphadenitis in our locality which is previously limited.
We found that the median time of onset was 3 months after BCG vaccination and the
mean duration for complete healing was 4.5 months. Solitary palpable mass without
systemic symptom was the universal presentation. The commonest site involved was
ipsilateral axilla region, while supraclavicular lymph nodes were occasionally seen.
Most patients did not have positive smear or culture proof. Previous studies found

22
treatment with needle aspiration significantly shorten recovery time yet other
parameters were not examined. In our study, we explored the relationship between
various clinical parameters and the duration of healing. We demonstrated that sex, age
at presentation, duration since vaccination, lymphocyte count, site and size of lymph
node, presence of spontaneous rupture or sinus formation did not correlate with
duration of healing. On the other hand, we further explored the clinical determinants
for subsequent scarring and found that the size of lymph node at presentation was
significantly associated with scarring, which have not been reported previously.
There are several limitations of the study which warrant comment. This
retrospective study is bound to the inherit shortcomings of missing and incomplete
data. There is also potential measurement and detection bias as there is no standard
criteria in diagnosing BCG associated lymphadenitis and no standardized
measurement method of lymph node and qualification of symptoms and signs.
However, we believe these biases have limited detrimental effects as all cases were
assessed and diagnosed by designated paediatric infectious disease specialists of the
department. Another limitation of our study is the small sample size, which render the
limited power and failure to detect significant correlates of healing duration such as
treatment with needle aspiration. A prospective cohort study involving collaboration
with different centres in Hong Kong can optimize the study and generate higher

23
impact results.

24
Conclusion
BCG associated suppurative lymphadenitis is not an uncommon complication
of BCG vaccination. The present study described the clinical features, investigations,
treatment and outcomes of suppurative BCG lymphadenitis. The diagnosis is clinical
and should be suspected in children present with ipsilateral regional lymph node
enlargement with history of BCG vaccination, even months afterwards. A basic chest
X-ray is the investigation recommended for all patients while tuberculin skin test has
no diagnostic use. The current study also illustrated the low positive microbiological
yield in aspirate, highlighting that negative smear or culture results do not rule out the
diagnosis. Good immunization technique, correct dosage and cautious use in
immunocompromised hosts are important measures to decrease risk. As evident by
randomized controlled trials, anti-tuberculous treatment has no role in the
management of BCG associated suppurative lymphadenitis, and needle aspiration
remains to be the safe and effective way of treatment. Surgical excision is reserved for
those who failed repeated needle aspiration attempts.
(Word count: 3294)
25
References
1. Colditz GA, Brewer TF, Berkey CS, Wilson ME, Burdick E, Fineberg HV, et al.
Efficacy of BCG vaccine in the prevention of tuberculosis. Meta-analysis of the
published literature. JAMA. 1994 Mar 2;271(9):698-702.
2. Department of Health, HKSAR. Annual Report of Tuberculosis and Chest
Service, 2000.
3. Milstien JB, Gibson JJ. Quality control of BCG vaccine by WHO: a review of
factors that may influence vaccine effectiveness and safety. Bull World Health
Organ. 1990;68(1):93-108.
4. Dommergues MA, de La Rocque F, Guy C, Lécuyer A, Jacquet A, Guérin N, et
al. Local and regional adverse reactions to BCG-SSI vaccination: a 12-month
cohort follow-up study. Vaccine. 2009 Nov 23;27(50):6967-73.
5. Victoria MS, Shah BR. Bacillus Calmette-Guérin lymphadenitis: a case report
and review of the literature. Pediatr Infect Dis. 1985 May-Jun;4(3):295-6.
6. Singla A, Singh S, Goraya JS, Radhika S, Sharma M. The natural course of
nonsuppurative Calmette-Guérin bacillus lymphadenitis. Pediatr Infect Dis J.
2002 May;21(5):446-8.
7. J Goraya, V Virdi. Bacille Calmette-Guérin lymphadenitis. Postgrad Med J. 2002
June; 78(920): 327–329.
26
8. Talbot EA, Perkins MD, Silva SF, Frothingham R. Disseminated bacille
Calmette-Guérin disease after vaccination: case report and review. Clin Infect
Dis. 1997 Jun;24(6):1139-46.
9. Gupta K, Singh N, Bhatia A, Arora VK, Singh UR, Singh B. Cytomorphologic
patterns in Calmette Guerin bacillus lymphadenitis. Acta Cytol. 1997
Mar-Apr;41(2):348-50.
10. Yan JJ, Chen FF, Jin YT, Chang KC, Wu JJ, Wang YW, et al. Differentiation of
BCG-induced lymphadenitis from tuberculosis in lymph node biopsy specimens
by molecular analyses of pncA and oxyR. J Pathol. 1998 Jan;184(1):96-102.
11. Santos A, Dias A, Cordeiro A, Cordinhã C, Lemos S, Rocha G, et al. Severe
axillary lymphadenitis after BCG vaccination: alert for primary
immunodeficiencies. J Microbiol Immunol Infect. 2010 Dec;43(6):530-7.
12. Serour F, Mizrahi A, Somekh E, Feinberg J, Picard C, Casanova JL, et al.
Analysis of the interleukin-12/interferon-gamma pathway in children with
non-tuberculous mycobacterial cervical lymphadenitis. Eur J Pediatr. 2007
Aug;166(8):835-41. Epub 2006 Nov 21.
13. Samileh N, Ahmad S, Farzaneh A, Shahnaz R, Lida F, Mohammad N. Immunity
status in children with Bacille Calmette-Guerin adenitis. A prospective study in
Tehran, Iran. Saudi Med J. 2006 Nov;27(11):1719-24.
27
14. Banac S, Franulović J. Familial liability to complications after BCG vaccination.
Acta Paediatr. 1997 Aug;86(8):899-902.
15. Daoud W. Control of an outbreak of BCG complications in Gaza. Respirology.
2003 Sep;8(3):376-8.
16. Lehmann HG, Engelhardt H, Freudenstein H, Hennessen W, Widmark R. BCG
vaccination of neonates, infants, schoolchildren and adolescents. Part I: Dose
finding studies with BCG strain 1331 Copenhagen. Dev Biol Stand.
1979;43:127-32.
17. Caglayan S, Arikan A, Yaprak I, Aksoz K, Kansoy S. Management of
suppuration in regional lymph nodes secondary to BCG vaccination. Acta
Paediatr Jpn. 1991 Dec;33(6):699-702.
18. Power JT, Stewart IC, Ross JD. Erythromycin in the management of troublesome
BCG lesions. Br J Dis Chest. 1984 Apr;78(2):192-4.
19. De Souza GR, Sant'Anna CC, Lapa e Silva JR, Mano DB, Bethlem NM.
Intradermal BCG vaccination complications--analysis of 51 cases. Tubercle.
1983 Mar;64(1):23-7.
20. Goraya JS, Virdi VS. Treatment of Calmette-Guérin bacillus adenitis: a
metaanalysis. Pediatr Infect Dis J. 2001 Jun;20(6):632-4.
28
21. Banani SA, Alborzi A. Needle aspiration for suppurative post-BCG adenitis.
Arch Dis Child. 1994 Nov;71(5):446-7.
22. Sataynarayana S, Mathur AD, Verma Y, Pradhan S, Bhandari MK. Needle
aspiration as a diagnostic tool and therapeutic modality in suppurative
lymphadenitis following Bacillus Calmette Guerin vaccination. J Assoc
Physicians India. 2002 Jun;50:788-91.
23. Hengster P, Sölder B, Fille M, Menardi G. Surgical treatment of bacillus
Calmette Guérin lymphadenitis. World J Surg. 1997 Jun;21(5):520-3.
24. Caglayan S, Arikan A, Yaprak I, Aksoz K, Kansoy S. Management of
suppuration in regional lymph nodes secondary to BCG vaccination. Acta
Paediatr Jpn. 1991 Dec;33(6):699-702.
29
Table 1. Clinical features and outcome of 15 children with BCG associated suppurative lymphadenitis. Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12 Case 13 Case 14 Case 15
Age at presentation (months)
2 16 3 5 2 4 26 2 7 2 5 5 3 3 2
Duration after vaccination (months)
2 16 3 5 2 4 26 2 7 2 5 5 3 3 2
Sex M F M M F F M M M F M M M M M WCC 12.4 21.3 8.9 11.4 18.8 10.1 12.5 13.7 14.0 10.7 16.4 6.1 12.3 N/A N/A Lym 8.0 10.8 7.3 4.5 N/A N/A 5.9 5.7 10.0 6.3 11.0 3.3 7.7 N/A N/A Site of LN A S S A A A A S A A A A A A A Size of LN (cm)*
3 1 1.5 1.5 2.5 2.5 3 1 3 3 2 1 3 2 1
AFB smear - + + - - + - + - + + N/A - + N/A M. bovis culture
- - - - - - - + - + - N/A - -
N/A
CXR N N N N N N C N N N N N N N N Mantoux test (mm)
N/A 15 N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
Needle aspiration
+ + + - + + + + + + + - + + -
Spontaneous rupture
+ - - + - - - + - - + - + - -
Sinus formation
- - - - - - - + - - + - - - -
Time to LN resolution (months)
6 6 3 4 N/A N/A 3 5 8 3 5 4 2 3 6
Scarring + - - + N/A N/A + + + + + - + - - A= axillar; AFB = acid fast bacilli; C=calcification at axilla; CXR = chest X-ray; LN = lymph node; Lym = lymphocyte count; N=normal; N/A = not available; S= supraclaviclar; WCC = white cell count * maximal dimension
30
Table 2. Comparison of healing time among various clinical parameters
Clinical parameters Healing duration (months) p
Sex (male/female) 4.5±1.8 4.5±2.1 0.97
Site of LN (axilla/supraclavicular) 4.4±1.8 4.7±1.5 0.83
Size of LN (<2cm/≥2cm) 4.3±2.1 4.6±1.2 0.71
Spontaneous rupture (yes/no) 4.4±1.5 4.5±1.9 0.94
Sinus formation (yes/no) 5.0±0.0 4.4±1.8 0.28
Needle aspiration (yes/no) 4.4±1.9 4.8±1.2 0.60


















