

F. benvenuti healthcare policy in the area of stroke experiences of tuscany
44
Healthcare policy in the area of stroke: experiences of Tuscany Francesco Benventi Dipartimento Territorio-Fragilità AUSL11 Empoli, Italy Łódź 26-27 February 2013
-
Upload
wydzial-ds-ezdrowia-departament-polityki-zdrowotnej-urzad-marszalkowski-w-lodzi -
Category
Documents
-
view
473 -
download
4
Transcript of F. benvenuti healthcare policy in the area of stroke experiences of tuscany

Healthcare policy in the area of stroke: experiences of Tuscany
Francesco Benventi
Dipartimento Territorio-Fragilità
AUSL11 Empoli, Italy
Łódź 26-27 February 2013

Str
oke i
n T
uscan
y
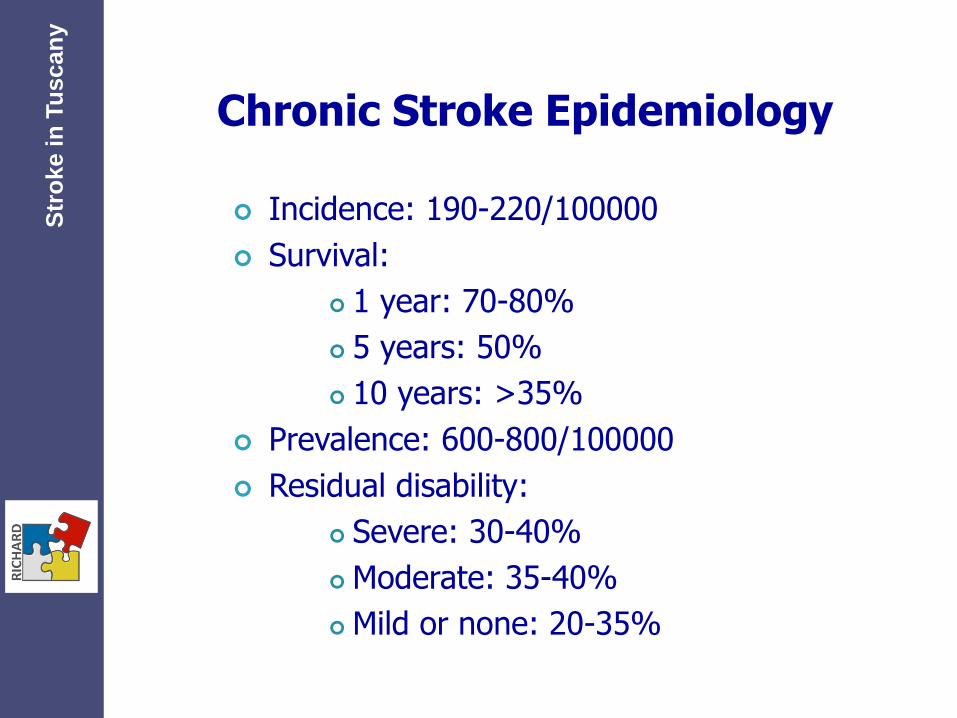
Chronic Stroke Epidemiology
Incidence: 190-220/100000
Survival:
1 year: 70-80%
5 years: 50%
10 years: >35%
Prevalence: 600-800/100000
Residual disability:
Severe: 30-40%
Moderate: 35-40%
Mild or none: 20-35%
Str
oke i
n T
uscan
y

Source
AUSL11, 2012
Str
oke i
n T
uscan
y Hospital admissions for stroke (DRG14)
0
100
200
300
400
500
600
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
years
nu
mb
er
Deaths after stroke
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2002 2003 2004 2005 2006 2007 2008 2009 2010
year
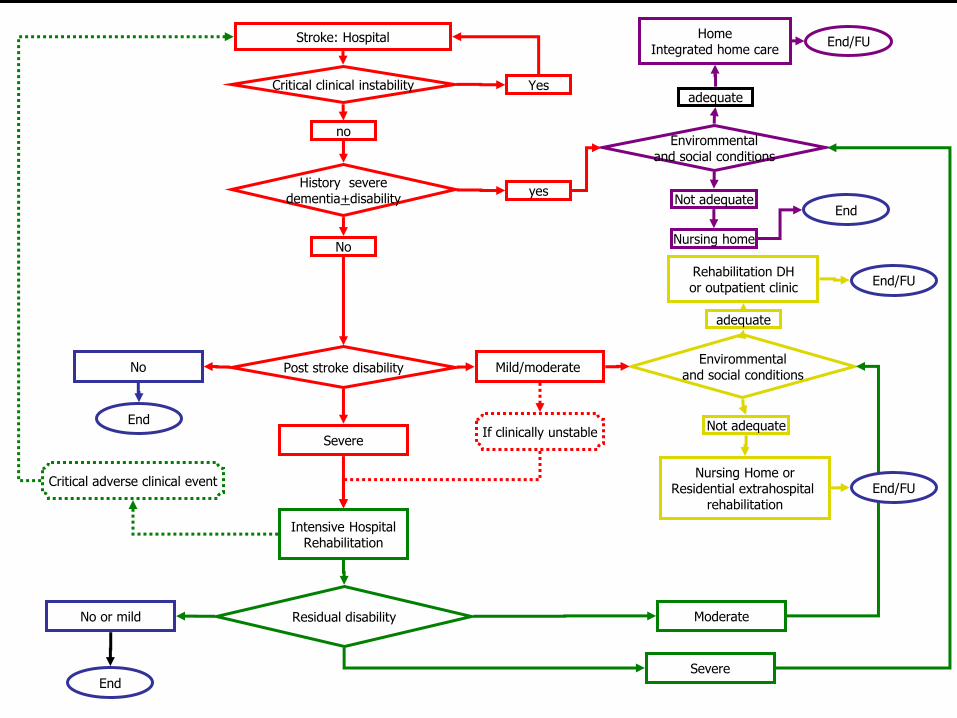
Stroke: Hospital
Critical clinical instability Yes
History severe dementia+disability
no
yes
No
Envirommental and social conditions
adequate
Not adequate
Home Integrated home care
Nursing home
Post stroke disability Mild/moderate Envirommental
and social conditions
adequate
Not adequate
Rehabilitation DH or outpatient clinic
Nursing Home or Residential extrahospital
rehabilitation
Severe
Intensive Hospital Rehabilitation
No
End If clinically unstable
End/FU
End
Residual disability No or mild
End
Moderate
Severe
Critical adverse clinical event
End/FU
End/FU
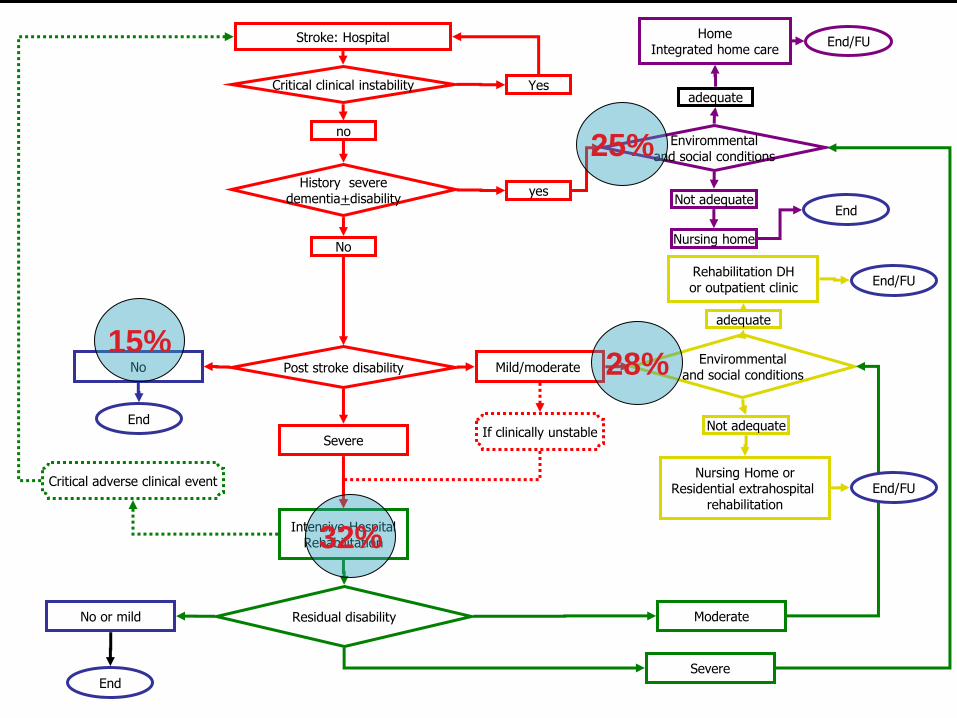
Stroke: Hospital
Critical clinical instability Yes
History severe dementia+disability
no
yes
No
Envirommental and social conditions
adequate
Not adequate
Home Integrated home care
Nursing home
Post stroke disability Mild/moderate Envirommental
and social conditions
adequate
Not adequate
Rehabilitation DH or outpatient clinic
Nursing Home or Residential extrahospital
rehabilitation
Severe
Intensive Hospital Rehabilitation
No
End If clinically unstable
End/FU
End
Residual disability No or mild
End
Moderate
Severe
Critical adverse clinical event
End/FU
End/FU
25%
32%
28% 15%
Sharing information
Galileo Hospital Lab Radiology Hospital specialists outpatient clinics
Patidok Community rehabilitation
Millewin GP records
Aster Home care Nursing homes
Clin
ical P
ath
ways
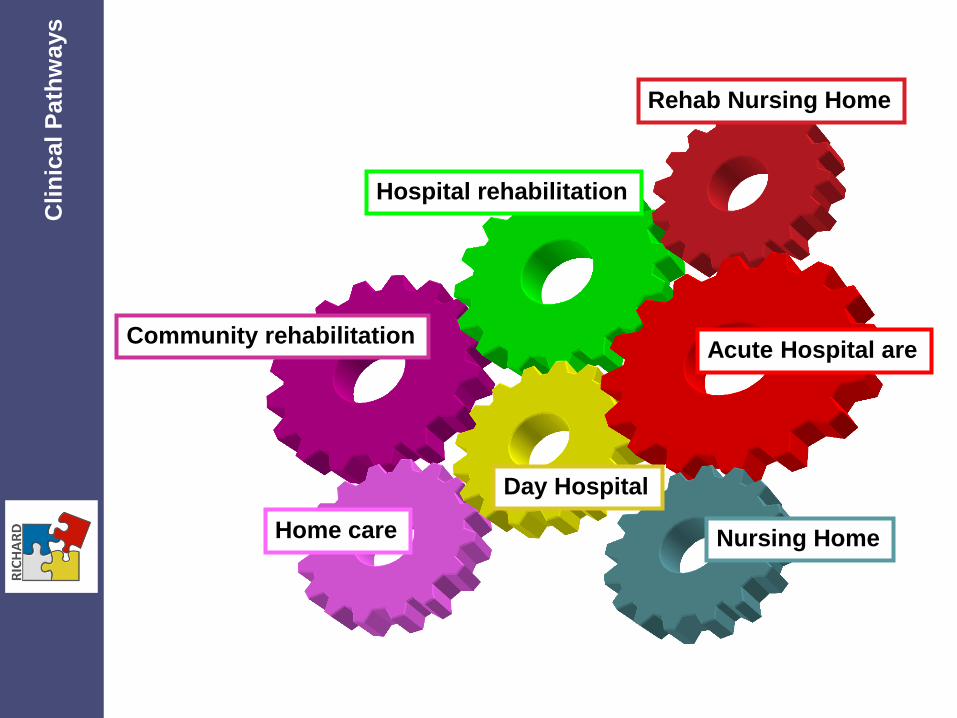
Acute Hospital are
Rehab Nursing Home
Hospital rehabilitation
Community rehabilitation
Home care
Day Hospital
Nursing Home
Clin
ical P
ath
ways
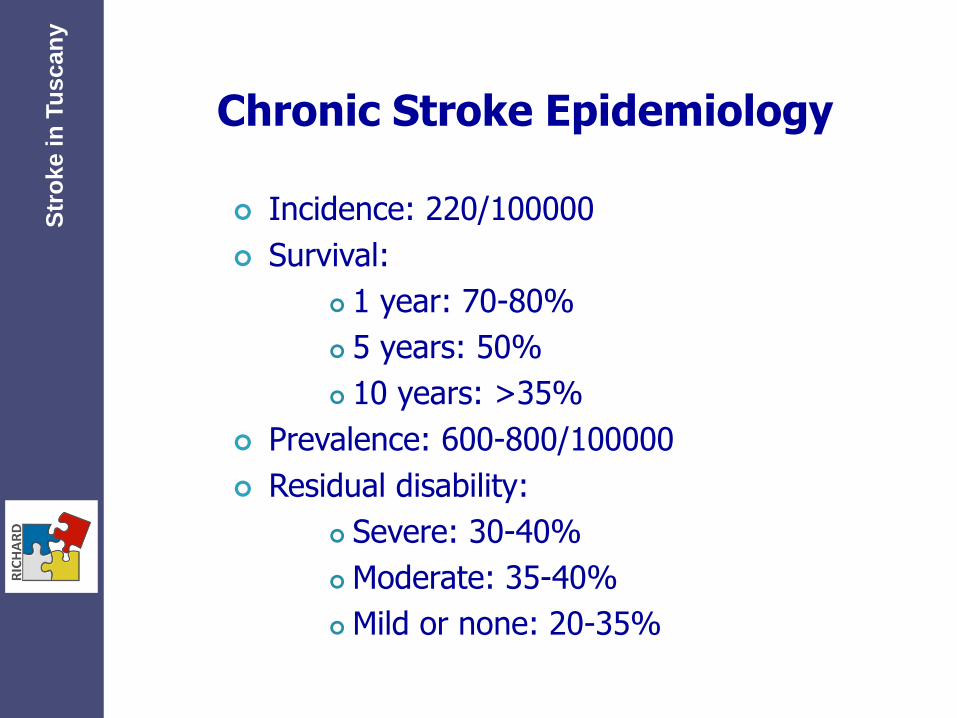
Chronic Stroke Epidemiology
Incidence: 220/100000
Survival:
1 year: 70-80%
5 years: 50%
10 years: >35%
Prevalence: 600-800/100000
Residual disability:
Severe: 30-40%
Moderate: 35-40%
Mild or none: 20-35%
Str
oke i
n T
uscan
y
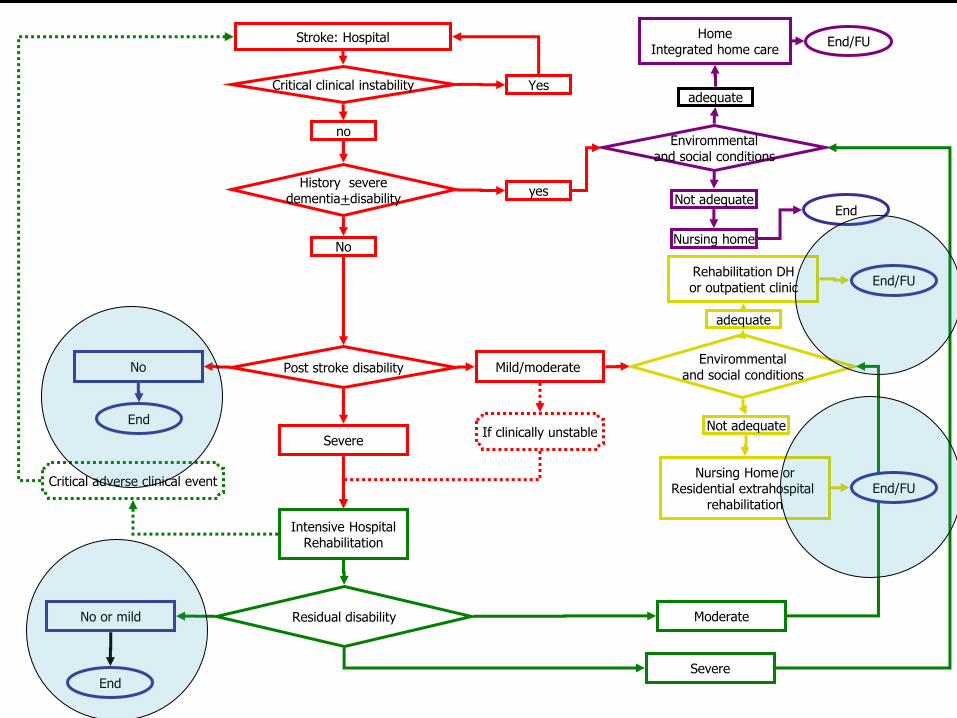
Stroke: Hospital
Critical clinical instability Yes
History severe dementia+disability
no
yes
No
Envirommental and social conditions
adequate
Not adequate
Home Integrated home care
Nursing home
Post stroke disability Mild/moderate Envirommental
and social conditions
adequate
Not adequate
Rehabilitation DH or outpatient clinic
Nursing Home or Residential extrahospital
rehabilitation
Severe
Intensive Hospital Rehabilitation
No
End If clinically unstable
End/FU
End
Residual disability No or mild
End
Moderate
Severe
Critical adverse clinical event
End/FU
End/FU

Acute Hospital Care
Rehab Nursing Home
Hospital rehabilitation
Community rehabilitation
Home care
APA
Upper limb care
CLEAR
Day Hospital
Nursing Home
Clin
ical P
ath
ways
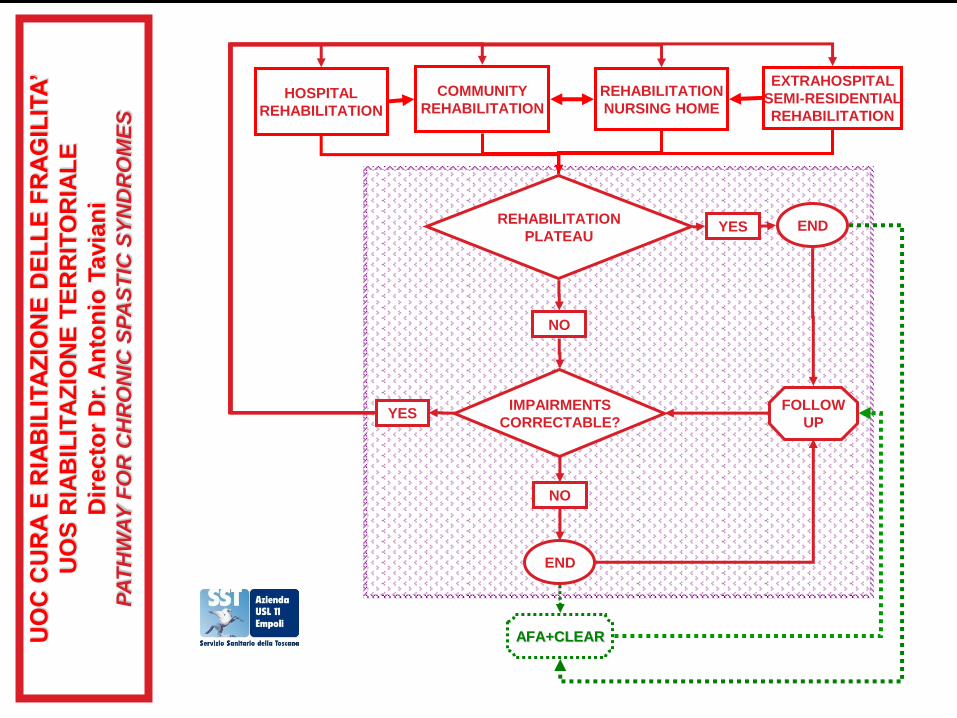
UO
C C
UR
A E
RIA
BIL
ITA
ZIO
NE
DE
LL
E F
RA
GIL
ITA
’
UO
S R
IAB
ILIT
AZ
ION
E T
ER
RIT
OR
IAL
E
Dir
ecto
r D
r. A
nto
nio
Tavia
ni
PA
TH
WA
Y F
OR
CH
RO
NIC
SP
AS
TIC
SY
ND
RO
ME
S
REHABILITATION
PLATEAU
IMPAIRMENTS
CORRECTABLE?
HOSPITAL
REHABILITATION
COMMUNITY
REHABILITATION
REHABILITATION
NURSING HOME
EXTRAHOSPITAL
SEMI-RESIDENTIAL
REHABILITATION
YES
NO
END
NO
YES
END
AFA+CLEAR
FOLLOW
UP

APAs
Physical activity programs, carried out in group, adapted to chronic alterations of functional status
for tertiary prevention of disability
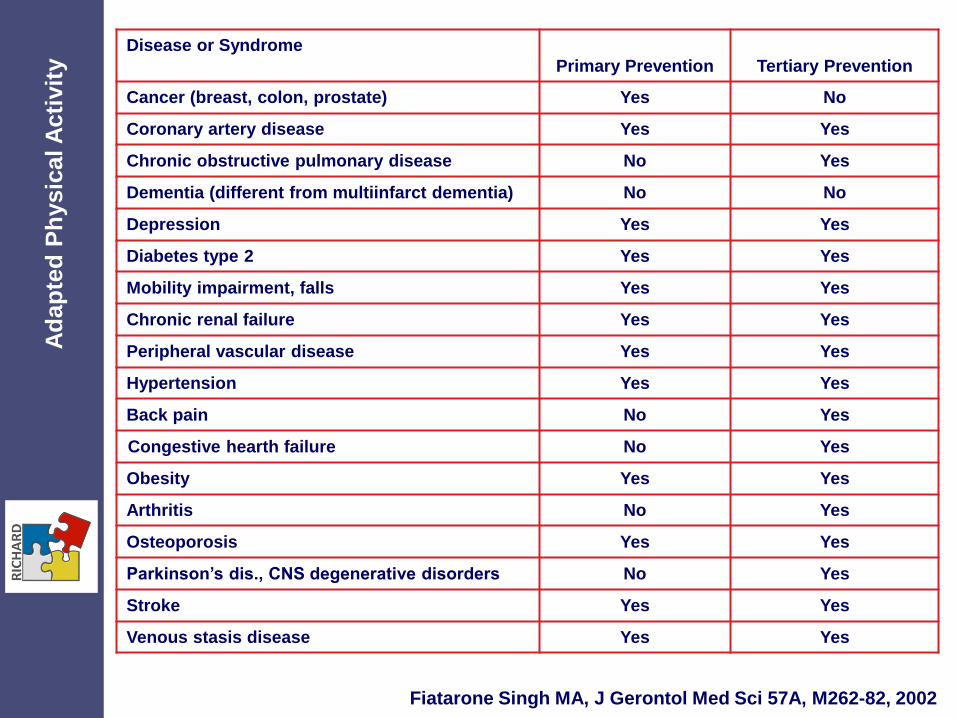
Disease or Syndrome
Primary Prevention
Tertiary Prevention
Cancer (breast, colon, prostate) Yes No
Coronary artery disease Yes Yes
Chronic obstructive pulmonary disease No Yes
Dementia (different from multiinfarct dementia) No No
Depression Yes Yes
Diabetes type 2 Yes Yes
Mobility impairment, falls Yes Yes
Chronic renal failure Yes Yes
Peripheral vascular disease Yes Yes
Hypertension Yes Yes
Back pain No Yes
Congestive hearth failure No Yes
Obesity Yes Yes
Arthritis No Yes
Osteoporosis Yes Yes
Parkinson’s dis., CNS degenerative disorders No Yes
Stroke Yes Yes
Venous stasis disease Yes Yes
Fiatarone Singh MA, J Gerontol Med Sci 57A, M262-82, 2002
Ad
ap
ted
Ph
ysic
al A
cti
vit
y
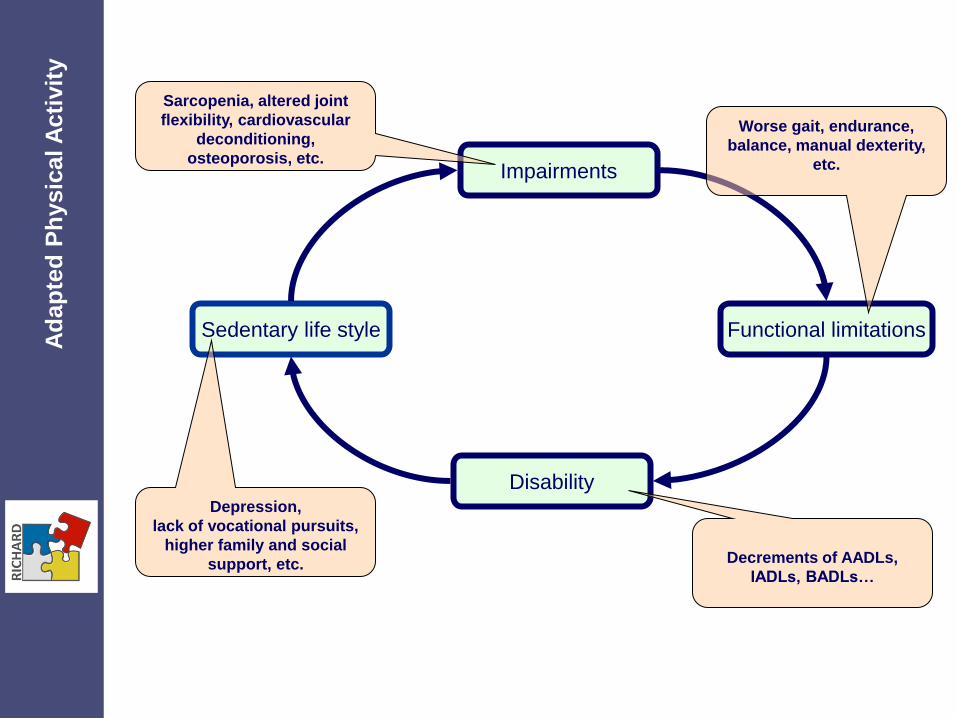
Impairments
Functional limitations
Disability
Sedentary life style
Depression,
lack of vocational pursuits,
higher family and social
support, etc.
Sarcopenia, altered joint
flexibility, cardiovascular
deconditioning,
osteoporosis, etc.
Worse gait, endurance,
balance, manual dexterity,
etc.
Decrements of AADLs,
IADLs, BADLs…
Ad
ap
ted
Ph
ysic
al A
cti
vit
y
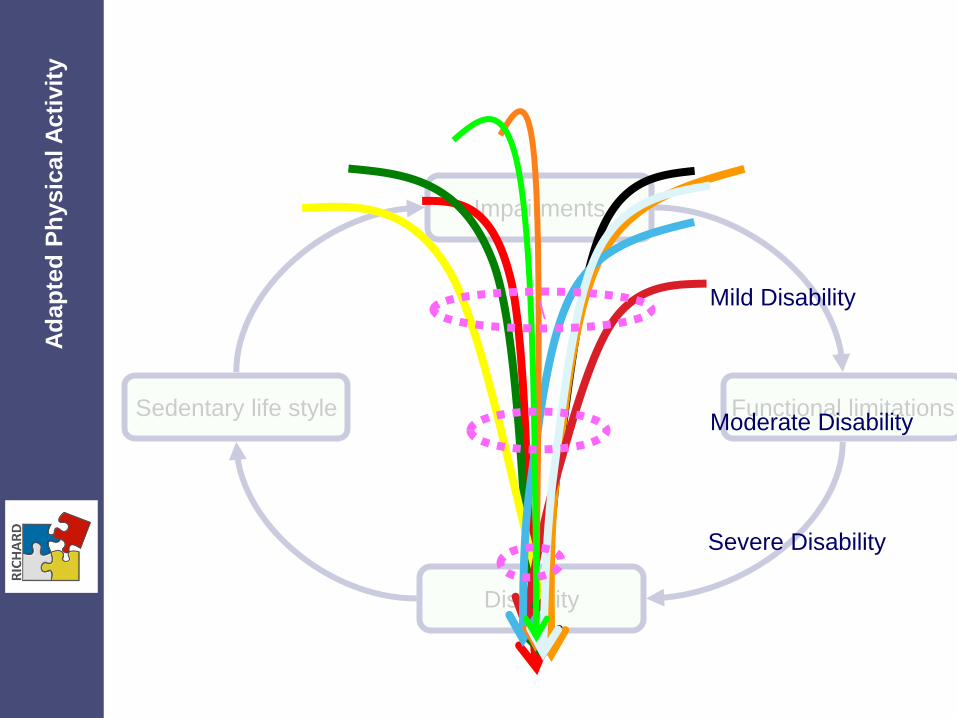
Sedentary life style
Impairments
Functional limitations
Disability
\
Moderate Disability
Severe Disability
Mild Disability
Ad
ap
ted
Ph
ysic
al A
cti
vit
y

Impairments
Functional limitations
Disability
Active life-style
Better integration in the
community, lower family and
social support,
Preservation of vocational
pursuits, QoL, etc.
Better muscle and joint
function, endurance,
increased BMD, etc. Easier focused
interventions for
improving gait, balance,
manual dexterity, etc.
Less disability for
AADLs, IADLs, BADLs…
Ad
ap
ted
Ph
ysic
al A
cti
vit
y
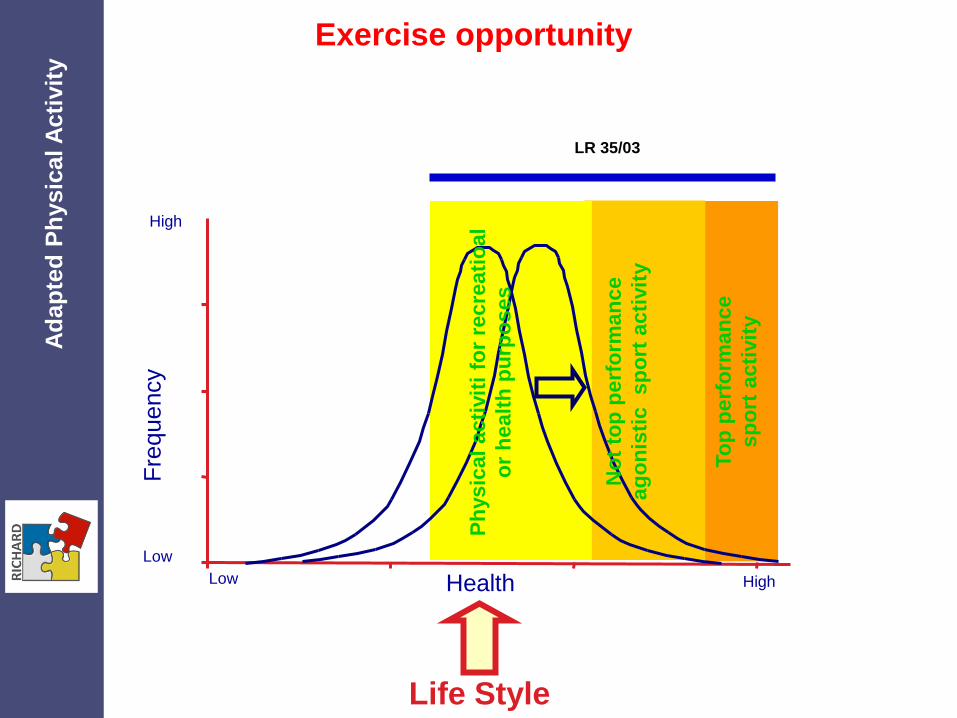
Life Style
Fre
quency
Health Low High
Low
High
Ph
ysic
al
acti
vit
i fo
r re
cre
ati
oal
or
healt
h p
urp
oses
LR 35/03
No
t to
p p
erf
orm
an
ce
ag
on
isti
c
sp
ort
acti
vit
y
To
p p
erf
orm
an
ce
sp
ort
acti
vit
y
Exercise opportunity A
dap
ted
Ph
ysic
al A
cti
vit
y
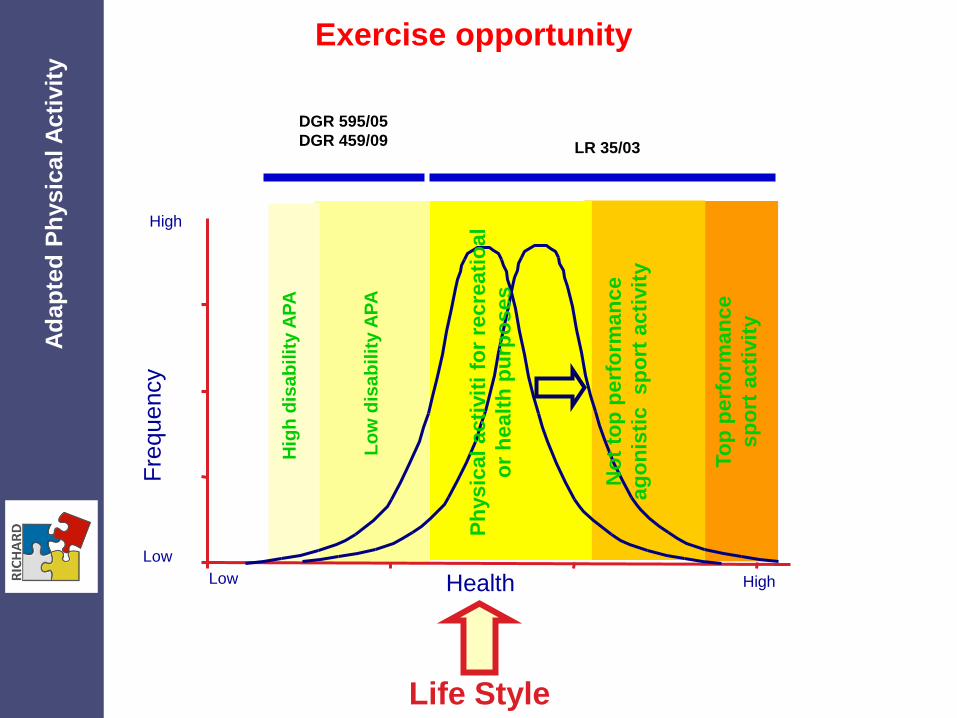
Life Style
Fre
quency
Health Low High
Low
High
Hig
h d
isa
bilit
y A
PA
Ph
ysic
al
acti
vit
i fo
r re
cre
ati
oal
or
healt
h p
urp
oses
LR 35/03
DGR 595/05
DGR 459/09
No
t to
p p
erf
orm
an
ce
ag
on
isti
c
sp
ort
acti
vit
y
Lo
w d
isa
bil
ity A
PA
To
p p
erf
orm
an
ce
sp
ort
acti
vit
y
Exercise opportunity A
dap
ted
Ph
ysic
al A
cti
vit
y

2.20 €
per session
Ad
ap
ted
Ph
ysic
al A
cti
vit
y
( ) + = 2.20 €
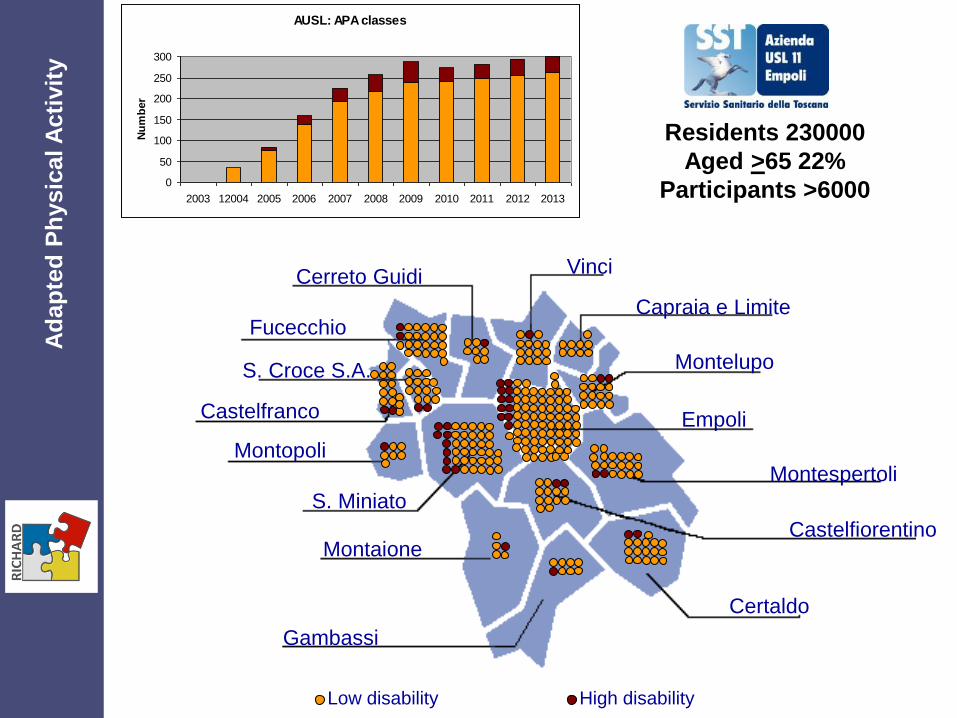
Fucecchio
S. Croce S.A.
Castelfranco
Montopoli
S. Miniato
Gambassi
Montaione
Montelupo
Empoli
Montespertoli
Certaldo
Capraia e Limite
Cerreto Guidi Vinci
Castelfiorentino
Low disability High disability
AUSL: APA classes
0
50
100
150
200
250
300
2003 12004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Nu
mb
er
Residents 230000
Aged >65 22%
Participants >6000
Ad
ap
ted
Ph
ysic
al A
cti
vit
y
Ad
ap
ted
Ph
ysic
al A
cti
vit
y
FOR HYPOMOBILITY SYNDROMES AND OSTEOPOROSIS
AND CHRONIC SYNDROMES STABILIZED IN THE
OUTCOMES APA PROGRAMS ARE APPROPRIATE…..
Ad
ap
ted
Ph
ysic
al A
cti
vit
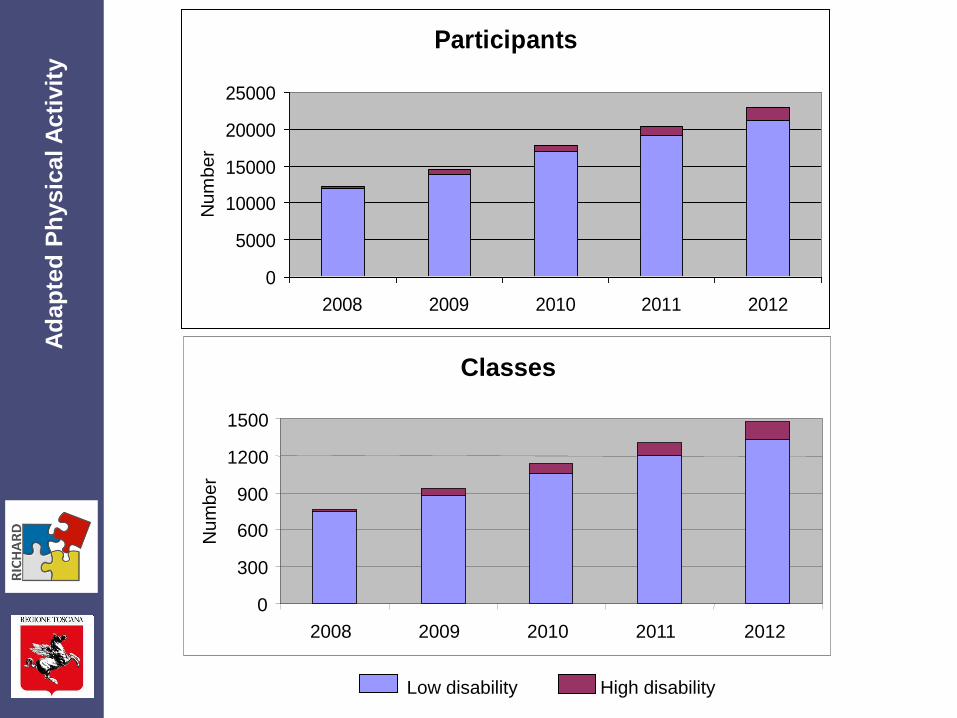
y Participants
0
5000
10000
15000
20000
25000
2008 2009 2010 2011 2012
Num
ber
High disability Low disability
Classes
0
300
600
900
1200
1500
2008 2009 2010 2011 2012
Nu
mb
er
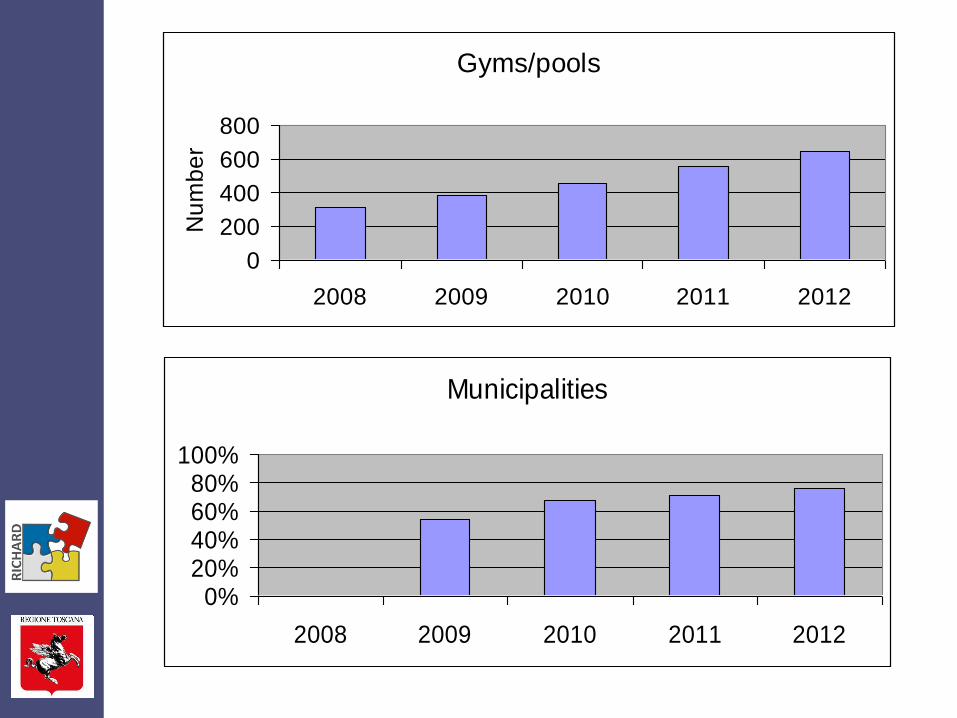
Gyms/pools
0
200
400
600
800
2008 2009 2010 2011 2012
Nu
mb
er
Municipalities
0%20%40%60%80%
100%
2008 2009 2010 2011 2012
Conferenze Stato Regioni ed Unificata
Adapted Physical Activity
for chronic stroke survivors
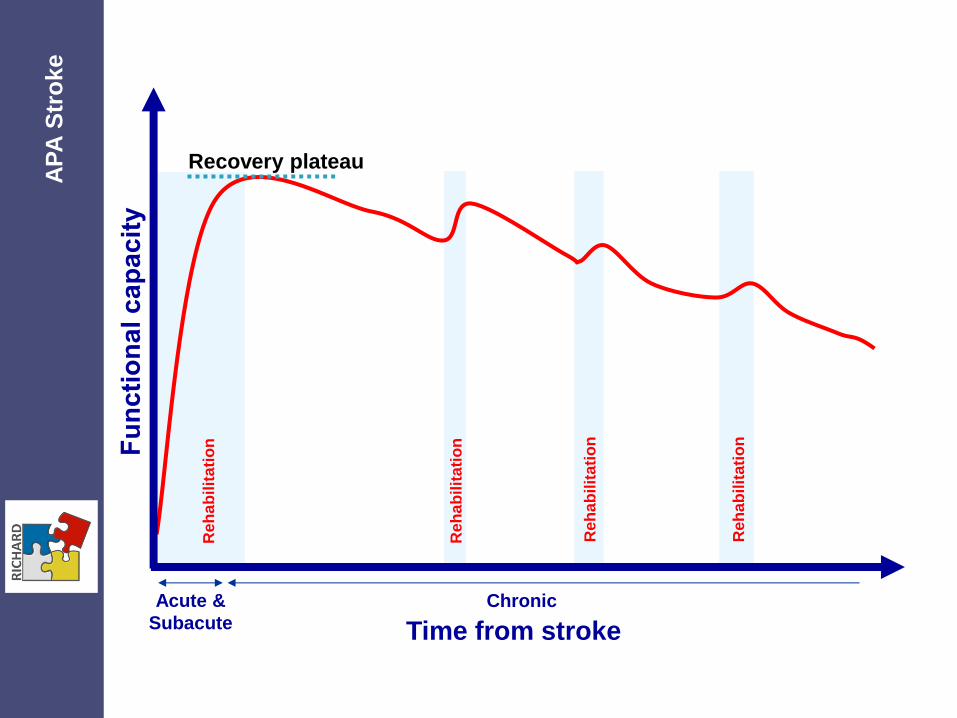
Recovery plateau
Reh
ab
ilit
ati
on
Reh
ab
ilit
ati
on
Re
ha
bil
ita
tio
n
Re
ha
bil
ita
tio
n
Time from stroke
Acute &
Subacute
Chronic
AP
A S
tro
ke
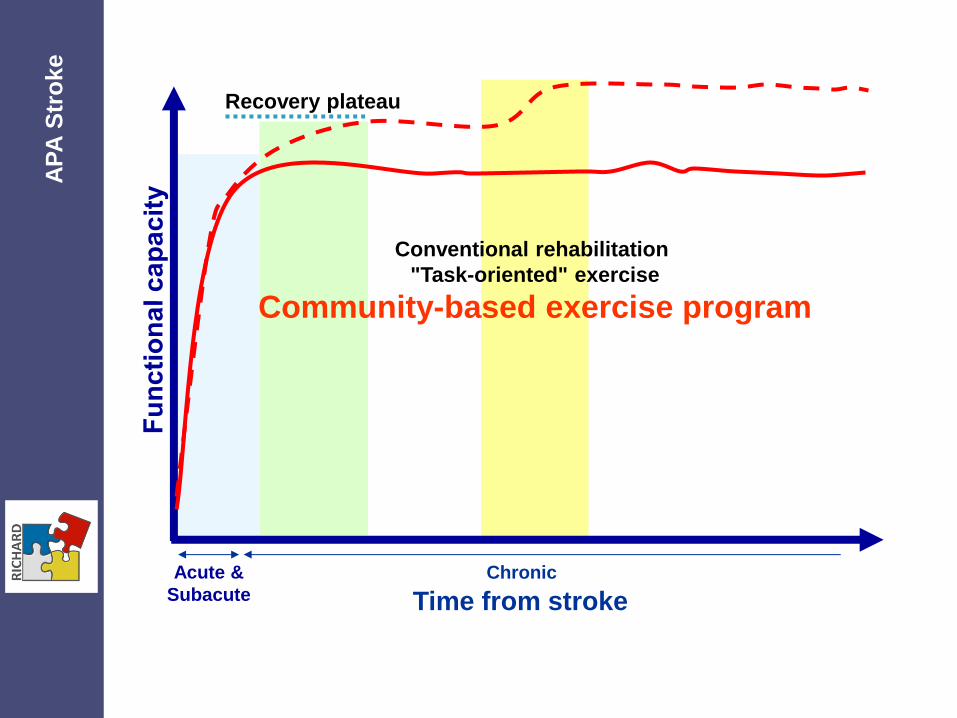
Recovery plateau
Conventional rehabilitation
"Task-oriented" exercise
Community-based exercise program
Time from stroke
Acute &
Subacute
Chronic
AP
A S
tro
ke
23:726-734;2009
Inclusion criteria
Time from stroke >8 months
Age >40 years
Able to walk independently for 6 minutes (also with walking aids) at a velocity 0,2-0,6 stature/sec
No critical comorbidity or severe dementia
AP
A S
tro
ke
METHODS
Duration 6 months
APA group recruited in Empoli Health Authority area
Usual care group (control group) recruited in Pisa and Florence Health Authorities
Project approved by Local Ethical Committee
AP
A S
tro
ke
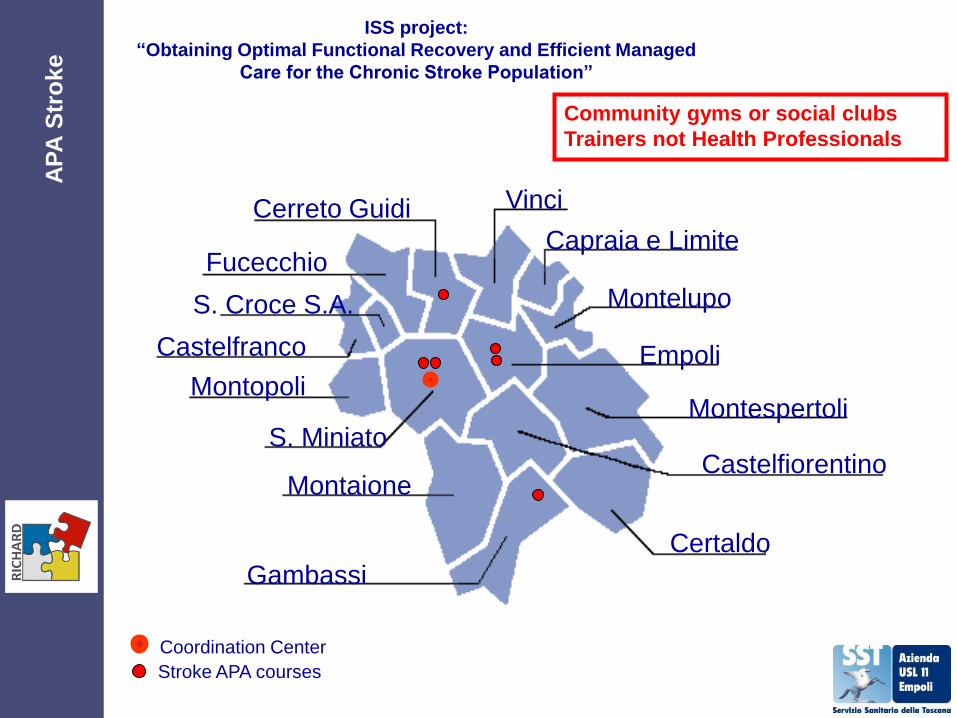
Coordination Center
Stroke APA courses
ISS project:
“Obtaining Optimal Functional Recovery and Efficient Managed
Care for the Chronic Stroke Population”
Fucecchio
S. Croce S.A.
Castelfranco
Montopoli
S. Miniato
Gambassi
Montaione
Montelupo
Castelfiorentino
Empoli
Montespertoli
Certaldo
Capraia e Limite
Cerreto Guidi Vinci
Community gyms or social clubs
Trainers not Health Professionals
AP
A S
tro
ke

1,90 €
per session
No transportation provided by LHA
AP
A S
tro
ke
( ) + = 1.90 €
Safety
No adverse clinical
event in gymnasiums
AP
A S
tro
ke
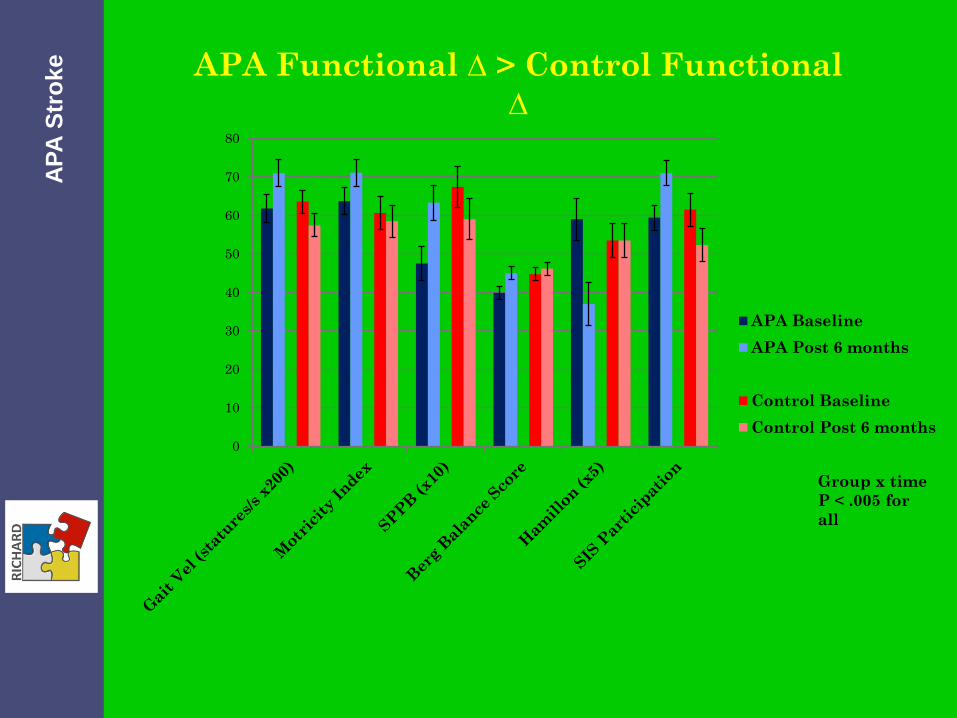
0
10
20
30
40
50
60
70
80
APA Functional ∆ > Control Functional
∆
APA Baseline
APA Post 6 months
Control Baseline
Control Post 6 months
Group x time
P < .005 for
all
AP
A S
tro
ke
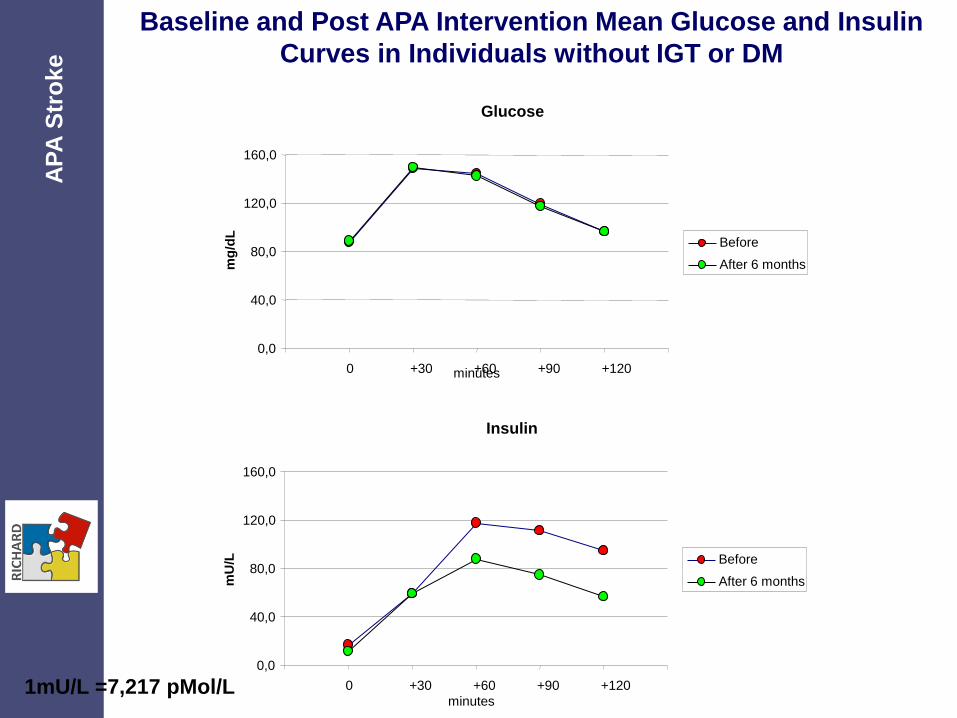
Glucose
0,0
40,0
80,0
120,0
160,0
0 +30 +60 +90 +120
mg
/dL
Before
After 6 months
Insulin
0,0
40,0
80,0
120,0
160,0
0 +30 +60 +90 +120
mU
/L
Before
After 6 months
minutes
minutes
1mU/L =7,217 pMol/L
Baseline and Post APA Intervention Mean Glucose and Insulin
Curves in Individuals without IGT or DM A
PA
Str
oke
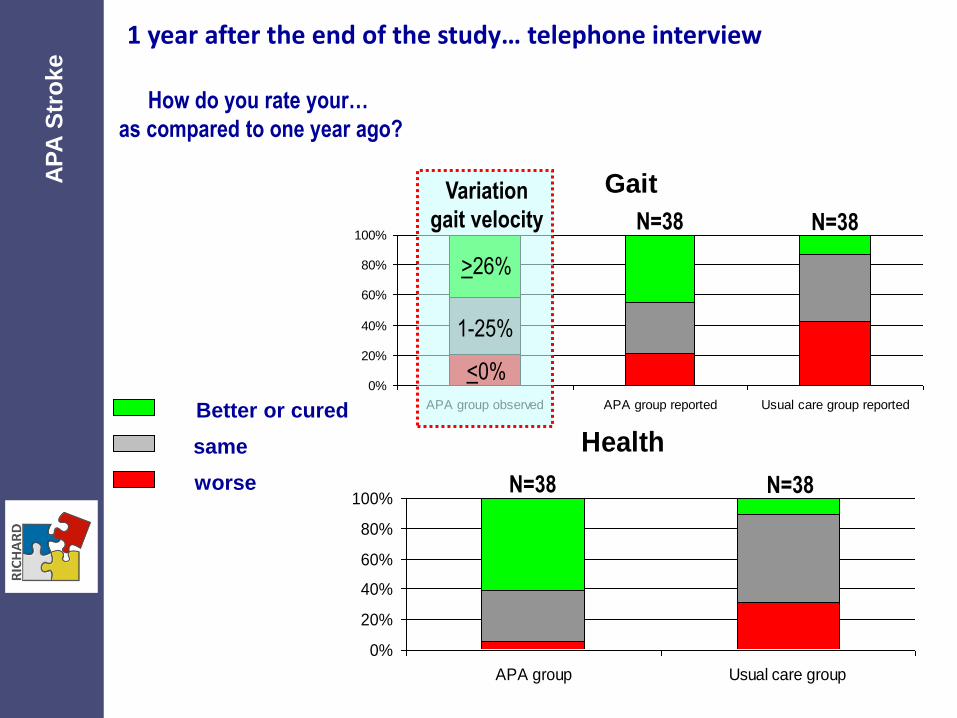
Better or cured
Health
0%
20%
40%
60%
80%
100%
APA group Usual care group
1 year after the end of the study… telephone interview
How do you rate your…
as compared to one year ago?
same
worse N=38 N=38
Gait
0%
20%
40%
60%
80%
100%
APA group observed APA group reported Usual care group reported
1-25%
N=38 N=38
>26%
<0%
Variation
gait velocity
AP
A S
tro
ke
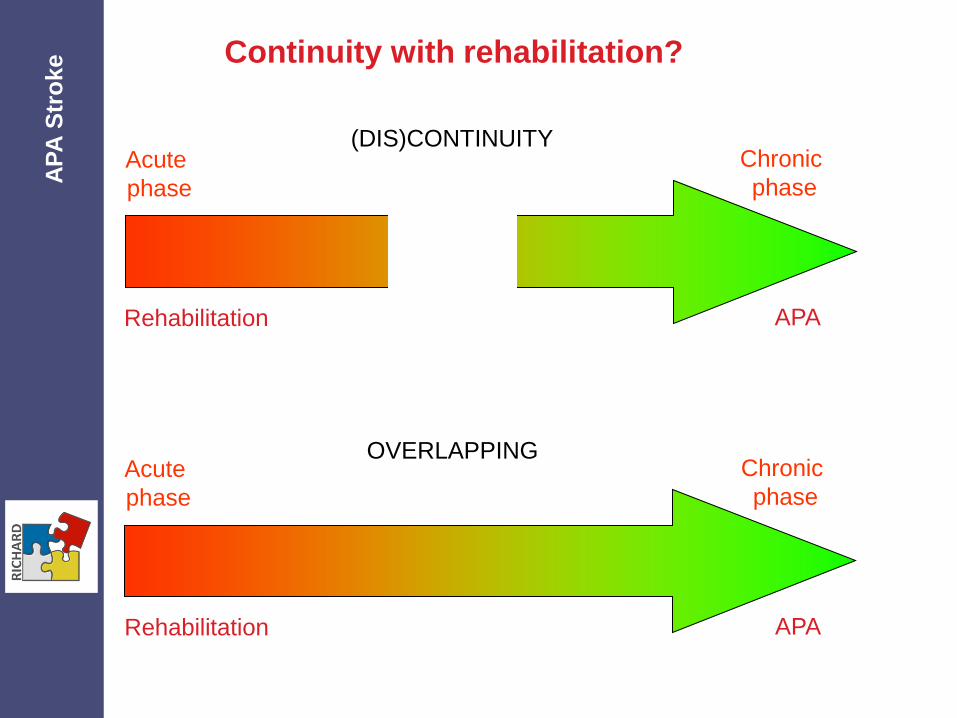
Acute
phase
Chronic
phase
Rehabilitation APA
Continuity with rehabilitation?
Acute
phase
Chronic
phase
Rehabilitation APA
(DIS)CONTINUITY
OVERLAPPING
AP
A S
tro
ke
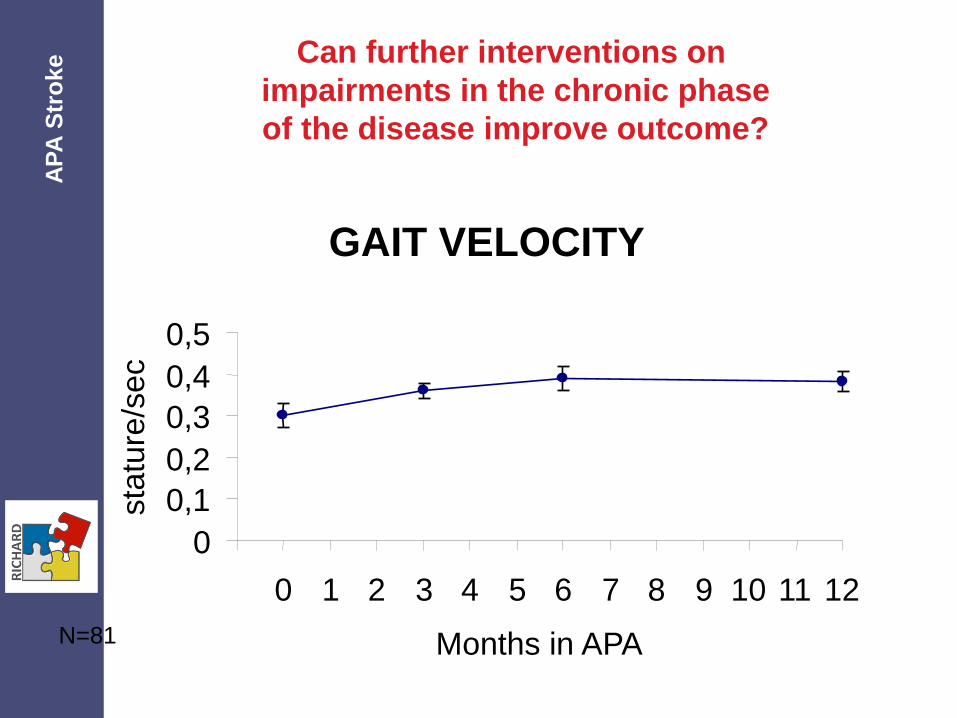
N=81
GAIT VELOCITY
0
0,1
0,2
0,3
0,4
0,5
0 1 2 3 4 5 6 7 8 9 10 11 12
Months in APA
sta
ture
/se
c
Can further interventions on
impairments in the chronic phase
of the disease improve outcome?
AP
A S
tro
ke

Baseline assessment
130
Excluded:
20 refused FU interview
(8 continuing APA)
3 not found
6 dead
1 year FU interview
101
Continuing APA
70
Interrupted APA
30
3 Other
0 Cost
4 Transportation
2 Family/work
6 Health
15 Lack of motivation
Self reported causes of
interruption: N.
Can we improve adherence? A
PA
Str
oke