Does the anti-β2-glycoprotein I antibody provide additional information in patients with...
4
Regular Article Does the anti-h 2 -glycoprotein I antibody provide additional information in patients with thrombosis? Eun Young Lee, Chang-Keun Lee, Tae Hoon Lee, Son Mi Chung, Seong Ho Kim, You Sook Cho, Bin Yoo * , Hee-Bom Moon Division of Allergy and Rheumatology, Department of Internal Medicine, University of Ulsan College of Medicine, Asan Medical Center, 388-1 Pungnap-Dong, Songpa-Gu, Seoul 138-736, South Korea Received 2 June 2003; received in revised form 30 July 2003; accepted 1 August 2003 Abstract Objective: To investigate whether the anti-h 2 -glycoprotein I (anti-h 2 GPI) antibody may provide additional information in patients with thrombosis in conjunction with the lupus anticoagulant (LAC) or anticardiolipin (aCL) antibody. Methods: We selected 235 patients whose plasma were tested for the presence of all three antiphospholipid (aPL) antibodies (LAC, aCL, and anti-h 2 GPI) and were positive for at least one aPL antibody from January 2000 to December 2001. The LAC test was performed using dilute activated thromboplastin time reagent (dAPTT) and dilute Russell viper venom time reagent (dRVVT). ACL (IgG/IgM) and anti-h 2 GPI (IgG/IgM) were detected by enzyme-linked immunosorbent assay (ELISA). Clinical data were collected and analysed in all patients with aPL antibody. Results: Of the 235 patients with aPL, thrombosis was detected in 76 patients (28.0%). Of the 76 patients with thrombosis, 29 were positive for LAC, 9 for aCL, 7 for anti-h 2 GPI, 3 for LAC + aCL, 9 for aCL + anti-h 2 GPI, 11 for LAC + anti-h 2 GPI, and 8 for LAC + aCL + anti-h 2 GPI. The rate of thrombosis was significantly different ( p = 0.01) among single positive patients (45/163, 27.6%), double positive patients (23/60, 38.3%), and triple positive patients (8/12, 66.7%). In single positive patients, the rate of thrombosis was highest in LAC positive patients (29/85, 34.1%). In double positive patients, the LAC + anti-h 2 GPI positive group (11/24, 45.8%) and aCL + anti-h 2 GPI positive group (9/22, 40.9%) had higher rates of thrombosis than the LAC + aCL positive group (3/14, 21.4%). Conclusion: Single positivity for anti-h 2 GPI explained 9.2% of thrombotic events in the absence of LAC or aCL. Double or triple positivity for aPLs were associated with a higher rate of thrombosis than single positivity for aPL. Our results suggest that anti-h 2 GPI provides additional information in patients with thrombosis in conjunction with LAC or aCL. D 2003 Elsevier Ltd. All rights reserved. Keywords: Antiphospholipid antibody; Anti-h 2 -glycoprotein I antibody; Thrombosis 1. Introduction Antiphospholipid (aPL) antibodies are a family of auto- antibodies that exhibit a broad range of target specificities and affinities, all recognizing various combinations of phos- pholipids, phospholipid-binding proteins, or both. It origi- nally included the anticardiolipin (aCL) antibody, detected by enzyme-linked immunosorbant assay (ELISA), and the lupus anticoagulant (LAC), detected by clotting tests. These antibodies are associated with the clinical manifestations of venous or arterial thrombosis and recurrent fetal losses. To diagnose antiphospholipid syndrome (APS), the association of one clinical criterion with one biological criterion (aCL and/or LAC on two or more occasions at least six weeks apart) is needed [1]. However, recent advances have shown that most pathogenic antiphospholipid antibodies are direct- ed to phospholipid-binding proteins such as h 2 -glycoprotein I(h 2 GPI) [2,3] and prothrombin [4]. The aim of our study was to (i) investigate whether the anti-h 2 GPI antibody may provide additional information in patients with thrombosis in the absence the LAC or aCL antibody, and (ii) determine the clinical significance of the double or triple positivity of aPL antibodies in thrombosis. 2. Patients and methods 2.1. Patients We consecutively selected 527 patients whose plasma were tested for all three aPL antibodies (LAC, aCL anti- 0049-3848/$ - see front matter D 2003 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2003.08.023 * Corresponding author. Tel.: +82-2-3010-3282; fax: +82-2-3010-6969. E-mail address: [email protected] (B. Yoo). Thrombosis Research 111 (2003) 29 – 32
-
Upload
eun-young-lee -
Category
Documents
-
view
227 -
download
8
Transcript of Does the anti-β2-glycoprotein I antibody provide additional information in patients with...

Thrombosis Research 111 (2003) 29–32
Regular Article
Does the anti-h2-glycoprotein I antibody provide additional information
in patients with thrombosis?
Eun Young Lee, Chang-Keun Lee, Tae Hoon Lee, Son Mi Chung, Seong Ho Kim,You Sook Cho, Bin Yoo*, Hee-Bom Moon
Division of Allergy and Rheumatology, Department of Internal Medicine, University of Ulsan College of Medicine,
Asan Medical Center, 388-1 Pungnap-Dong, Songpa-Gu, Seoul 138-736, South Korea
Received 2 June 2003; received in revised form 30 July 2003; accepted 1 August 2003
Abstract
Objective: To investigate whether the anti-h2-glycoprotein I (anti-h2GPI) antibody may provide additional information in patients with
thrombosis in conjunction with the lupus anticoagulant (LAC) or anticardiolipin (aCL) antibody. Methods: We selected 235 patients whose
plasma were tested for the presence of all three antiphospholipid (aPL) antibodies (LAC, aCL, and anti-h2GPI) and were positive for at least one
aPL antibody from January 2000 to December 2001. The LAC test was performed using dilute activated thromboplastin time reagent (dAPTT)
and dilute Russell viper venom time reagent (dRVVT). ACL (IgG/IgM) and anti-h2GPI (IgG/IgM) were detected by enzyme-linked
immunosorbent assay (ELISA). Clinical data were collected and analysed in all patients with aPL antibody. Results: Of the 235 patients with
aPL, thrombosis was detected in 76 patients (28.0%). Of the 76 patients with thrombosis, 29 were positive for LAC, 9 for aCL, 7 for anti-h2GPI,
3 for LAC+ aCL, 9 for aCL + anti-h2GPI, 11 for LAC+ anti-h2GPI, and 8 for LAC+ aCL+ anti-h2GPI. The rate of thrombosis was
significantly different ( p = 0.01) among single positive patients (45/163, 27.6%), double positive patients (23/60, 38.3%), and triple positive
patients (8/12, 66.7%). In single positive patients, the rate of thrombosis was highest in LAC positive patients (29/85, 34.1%). In double positive
patients, the LAC+ anti-h2GPI positive group (11/24, 45.8%) and aCL+ anti-h2GPI positive group (9/22, 40.9%) had higher rates of
thrombosis than the LAC+ aCL positive group (3/14, 21.4%). Conclusion: Single positivity for anti-h2GPI explained 9.2% of thrombotic
events in the absence of LAC or aCL. Double or triple positivity for aPLs were associated with a higher rate of thrombosis than single positivity
for aPL. Our results suggest that anti-h2GPI provides additional information in patients with thrombosis in conjunction with LAC or aCL.
D 2003 Elsevier Ltd. All rights reserved.
Keywords: Antiphospholipid antibody; Anti-h2-glycoprotein I antibody; Thrombosis
1. Introduction apart) is needed [1]. However, recent advances have shown
Antiphospholipid (aPL) antibodies are a family of auto-
antibodies that exhibit a broad range of target specificities
and affinities, all recognizing various combinations of phos-
pholipids, phospholipid-binding proteins, or both. It origi-
nally included the anticardiolipin (aCL) antibody, detected
by enzyme-linked immunosorbant assay (ELISA), and the
lupus anticoagulant (LAC), detected by clotting tests. These
antibodies are associated with the clinical manifestations of
venous or arterial thrombosis and recurrent fetal losses. To
diagnose antiphospholipid syndrome (APS), the association
of one clinical criterion with one biological criterion (aCL
and/or LAC on two or more occasions at least six weeks
0049-3848/$ - see front matter D 2003 Elsevier Ltd. All rights reserved.
doi:10.1016/j.thromres.2003.08.023
* Corresponding author. Tel.: +82-2-3010-3282; fax: +82-2-3010-6969.
E-mail address: [email protected] (B. Yoo).
that most pathogenic antiphospholipid antibodies are direct-
ed to phospholipid-binding proteins such as h2-glycoprotein
I (h2GPI) [2,3] and prothrombin [4].
The aim of our study was to (i) investigate whether the
anti-h2GPI antibody may provide additional information in
patients with thrombosis in the absence the LAC or aCL
antibody, and (ii) determine the clinical significance of the
double or triple positivity of aPL antibodies in thrombosis.
2. Patients and methods
2.1. Patients
We consecutively selected 527 patients whose plasma
were tested for all three aPL antibodies (LAC, aCL anti-

Table 1
Site of thrombosis among single, double, or triple aPL positive patients
Artery Vein Both Fetal loss
Single positive patients 21 13 9 2
Double positive patients 13 6 3 1
Triple positive patients 3 4 1
Total 37 23 13 3
Values are absolute number of subjects in each group.
Statistical analysis was performed by using v2 test ( P= 0.69).
E.Y. Lee et al. / Thrombosis Research 111 (2003) 29–3230
body, and anti-h2GPI antibody) at Asan Medical Center
from January 2000 to December 2001. APL antibodies were
checked in these patients under the suspicion of aPL
associated disease such as systemic lupus erythematosus
(SLE), APS, avascular necrosis (AVN), stroke in young age,
pulmonary hypertension, thrombosis, fetal loss, etc. Clinical
data were collected from 235 patients who were positive for
at least one aPL antibody: positive LAC test and/or raised
IgG (z 12 U GPL/ml)/IgM (z 6 U MPL/ml) aCL anti-
bodies and/or raised IgG (z 20 SMU)/IgM (z 20 SMU)
anti-h2GPI antibodies.
Patients with the aPL antibody included those with SLE
(N = 52), primary APS (N = 34), AVN (N = 27), malignancy
(N = 21), atherosclerotic cerebrovascular disease (N = 21),
infectious disease (N = 10), deep vein thrombosis (N = 8),
primary pulmonary hypertension (N = 5), and others
(N = 57). All SLE patients fulfilled four or more criteria of
the American College of Rheumatology for the classifica-
tion of SLE [5]. Diagnosis of APS was made according to
preliminary criteria for the classification of APS [1]. Throm-
bosis was confirmed by venography, arteriography, Doppler
ultrasonography, or magnetic resonance (MR) angiography
in each patient.
Table 2
Antibody profiles in patients with the aPL antibody with or without
thrombosis
Thrombosis
(N= 76)
No thrombosis
(N= 159)
Single positive LAC 29 (38.2%) 56 (35.2%)
patients aCL 9 (11.8%) 26 (16.4%)
anti-h2GPI 7 (9.2%) 36 (22.6%)
Double positive LAC+ aCL 3 (3.9%) 11 (6.9%)
patients LAC+ anti-h2GPI 11 (14.5%) 13 (8.2%)
aCL+ anti-h2GPI 9 (11.8%) 13 (8.2%)
Triple positive
patients
LAC+ aCL+
anti-h2GPI
8 (10.5%) 4 (2.5%)
3. Methods
All three aPL antibody tests were performed simulta-
neously in each patient. As recommended by the Interna-
tional Society of Thrombosis and Hemostasis (ISTH), the
screening tests for LAC were performed using dilute acti-
vated thromboplastin time (dAPTT) reagent (Diagnostica
Stago, France) and dilute Russell viper venom time
(dRVVT) reagent (Gradipore, North Ryde, Australia) [6].
To confirm the presence of LAC, dRVVT confirm test
(Gradipore) was performed. ACL antibodies (IgG/IgM)
were detected by enzyme-linked immunosorbent assay
(Pharmacia Diagnostics, Freiburg, Germany). Results were
expressed in IgG and IgM units, and reported as positive for
raised IgG (z 12 U GPL/ml)/IgM (z 6 U MPL/ml) aCL
antibodies. Anti-h2GPI antibodies (IgG/IgM) were detected
by enzyme-linked immunosorbent assay (INOVA Diagnos-
tics, San Diego, CA, USA). Results were expressed in
standard h2GPI Ig units (SMU) and reported as positive
for raised IgG (z 20 SMU)/IgM (z 20 SMU) anti-h2GPI
antibodies.
Single aPL positivity was determined when only one aPL
test was positive, double positivity was determined when
two aPL tests (LAC+ aCL or LAC+ anti-h2GPI or anti-
h2GPI + aCL) were positive, and triple positivity was deter-
mined when all three aPL tests (LAC+ aCL + anti-h2GPI)
were positive.
Plasma levels of protein C and protein S were measured
by enzyme immunoassay (EIA) using monoclonal antibody
(Diagnostica Stago) in aPL antibody positive patients to
exclude protein C or protein S deficiency. The activity of
antithrombin III was also measured by colorimetric assay
using commercial kit (Diagnostica Stago).
4. Statistical analysis
Rate of thrombosis in patient groups was compared using
v2 test or logistic regression analysis. Comparisons among
single, double, and triple aPL antibody positive groups were
expressed as an odds ratio with its 95% confidence interval.
P values < 0.05 were considered statistically significant.
5. Results
Of the 235 patients with aPL antibodies, thrombosis was
detected in 76 patients (28.0%). According to the site of
thrombosis, 37 patients had arterial thrombosis (48.7%), 23
had venous thrombosis (30.3%), 13 had arterial and venous
thrombosis (17.1%), and 3 had fetal loss (3.9%). Table 1
shows the relationships of site of thrombosis and the
positive rate of thrombosis. There were no differences in
site of thrombosis among single, double, or triple aPL
positive patients (P= 0.69). According to the number of
total thrombotic events, 51 patients had one episode of
thrombosis (67.1%), 18 patients had two episodes of throm-
bosis (23.7%), 4 patients had three episodes of thrombosis
(5.3%), and 3 patients had four episodes of thrombosis
(3.9%). There was no correlation between the number of
thrombotic events and the positive rate of aPL antibodies
(r =� 0.10, P= 0.39). Plasma levels of protein C or protein

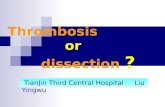
Fig. 1. The rate of thrombosis in single aPL antibody positive patients.
Table 3
The rate of thrombosis in aPL positive patients according to the positive
rate of the aPL antibody
N +Thrombosis �Thrombosis OR (95% CI) P
aPL positivity
Single 163 45 (27.6%) 118 (72.4%)
Double 60 23 (38.3%) 37 (61.7%) 1.63 (0.87–3.04) 0.25
Triple 12 8 (66.7%) 4 (33.3%) 5.24 (1.50–18.28) 0.009
The relative risk based on the single aPL positive group is shown.
OR= odds ratio; 95% CI = 95% confidence interval.
E.Y. Lee et al. / Thrombosis Research 111 (2003) 29–32 31
S and plasma antithrombin III activity in patients with
thrombosis were within normal range.
Table 2 shows antibody profiles of single, double, and
triple positive groups in patients with or without thrombosis.
Of the 76 patients with the aPL antibody and thrombosis, 45
were single aPL antibody positive (59.2%), 23 were double
aPL antibody positive (30.3%), and 8 were triple aPL
antibody positive (10.5%). Of the 76 patients with throm-
bosis, 7 patients were anti-h2GPI only positive (9.2%). Of
the 159 patients with the aPL antibody but no evidence of
thrombosis, 118 were single aPL antibody positive (74.2%),
37 were double aPL antibody positive (23.3%), and 4 were
triple aPL antibody positive (2.5%).
In single aPL positive patients with or without thrombo-
sis, LAC was most frequently detected (51.5%) and the rate
of thrombosis was highest in the LAC positive group (Fig.
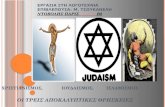
1). In double aPL positive patients, the rate of thrombosis
was highest in the LAC+ anti-h2GPI group (45.8%) and
lowest in the LAC+ aCL group (21.4%) (Fig. 2).
Table 3 shows differences in the rate of thrombosis in
patients according to the positive rate of the aPL antibody.
The rate of thrombosis was higher in triple positive patients
than in single positive patients (odds ratio 5.2, 95% CI 1.5–
18.3; P= 0.009). In double positive patients, rate of throm-
bosis was higher than in single positive patients, but the
Fig. 2. The rate of thrombosis in double aPL antibody positive patients.
difference was not statistically significant (odds ratio 1.6,
95% CI 0.9–3.0; P= 0.125).
6. Discussion
The detection of anti-h2GPI in autoimmune disease has
been the topic of several reports. Its detection in patients
with SLE has been associated with an increased frequency
of a history of thrombosis [3]. In patients with primary APS,
IgG anti-h2GPI that appear to differ from aCL were detected
[2]. These studies were focused on the detection of anti-
h2GPI which recognize cardiolipin and/or its cofactor
h2GPI in patients’ plasma. Although there have been several
reports on the presence of the anti-h2GPI antibody in APS,
international classification criteria for definite antiphospho-
lipid syndrome did not include the test for the anti-h2GPI
antibody because of lack of standardization [1]. The aim of
our study was to investigate whether the conventional anti-
h2GPI antibody test may provide additional information in
patients with thrombosis in conjunction with the LAC or
aCL antibody test.
According to our study, the rate of thrombosis was highest
in LAC positive patients among single aPL positive groups.
This result was consistent with a previous report in which the
LAC test was a more specific test than the aCL test in APS
[7]. Although the rate of thrombosis was lower in anti-h2GPI
positive patients than in aCL or LAC positive patients, single
positivity for the anti-h2GPI antibody explained 9.2% (7/76)
of thrombotic events in the absence of the LAC or aCL
antibody. This result shows the need of the anti-h2GPI
antibody test in patients with thrombosis even in an aCL
or LAC negative state. Previous reports about the anti-h2GPI
antibody test were limited to the detection of the anti-h2GPI
antibody in patients who were diagnosed APS and/or had the
aCL antibody [2,8]. In our study, seven patients with only the
anti-h2GPI antibody and thrombosis included two patients
with SLE, two patients with deep vein thrombosis, two
patients of mesenteric vein thrombosis, and one patient with
recurrent lacunar infarction. If we had added the anti-h2GPI
antibody test to the laboratory criteria for APS, more APS
patients would have been diagnosed.
Another important finding in our study was the relation-
ship between aPL antibody positivity and the rate of
thrombosis. The rate of thrombosis in double or triple aPL

E.Y. Lee et al. / Thrombosis Research 111 (2003) 29–3232
antibody positive patients was higher than in single aPL
antibody positive patients. Moreover, LAC + anti-h2GPI
patients or aCL+ anti-h2GPI patients had a higher rate of
thrombosis than LAC+ aCL positive patients in the double
aPL antibody positive group (45.8%, 40.9% vs. 21.4%).
These results may increase the need for all three aPL
antibody tests, including the anti-h2GPI antibody test, in
patients who have thrombosis or thrombotic risk.
Similar to some previous studies, aPL antibody positive
patients in this study included patients with primary APS,
SLE, malignancy, primary pulmonary hypertension, and
avascular necrosis [9,10]. The rate of thrombosis was 28%
of all aPL positive patients in our retrospective study, which
was much lower than a previous study in SLE patients [11].
This difference may be associated with two factors: First, our
study cohort included SLE and nonSLE patients. Second, we
added the anti-h2GPI test to the aPL antibody test which was
not included in the previous study. Whether aPL antibody
positive but nonthrombotic patients would have new throm-
botic events in the future should be pursued by further study.
The anti-h2GPI test that we used in this study was
standardized enzyme-linked immunosorbent assays (ELI-
SAs) for anti-h2GPI of the two major immunoglobulin
classes:IgG and IgM. Lewis et al. [12] confirmed the
precision of this test in APS patients and demonstrated the
correlation with other methods. They measured IgG, IgA,
and IgM anti-h2GPI antibodies in APS patients and healthy
controls and demonstrated that APS patients’ anti-h2GPI
levels were significantly different from those of the control
population. We did not measure IgA anti-h2GPI, but the
percentage of increased IgA anti-h2GPI in APS patients was
lower than that of increased IgG and IgM anti-h2GPI with
this method [12].
One of the limitations of this study is that we did not
check other antibodies against phospholipid-binding plasma
proteins such as prothrombin, protein C, protein S, and
annexin V. We measured plasma levels of protein C and
protein S which were within normal range in our patients
with thrombosis. These antibodies against phospholipid-
binding plasma proteins were frequently observed in patients
with SLE in a recent study [13]. Especially, anti-h2GPI and
antiprothrombin antibodies were significant risk factors for
arterial thrombosis, and the presence of antiprotein S anti-
bodies was a significant risk factor for venous thrombosis.
Whether the heterogeneity of these antiphospholipid anti-
bodies may explain the various clinical manifestations in
patients with definite APS or even in seronegative APS will
need to be confirmed through further studies.
Another limitation is the retrospective design of this
study, similarly to the majority of studies on this topic: the
aPL antibodies were measured some time after the throm-
botic episode. This is important because these antibodies
fluctuate over the time. Therefore, it is difficult to assess the
real value of a single determination of aPL some time after
the thrombotic event. However, it would be very interesting
to see how many patients with anti-h2GPI antibody but
without thrombosis at the time of aPL test may develop
thrombosis in the future.
In summary, single positivity for anti-h2GPI explained
9.2% of the thrombotic events in the absence of the LAC or
aCL antibody. Double or triple positivity for aPL antibodies
were associated with a higher rate of thrombosis than single
positivity for the aPL antibody. Our results suggest that anti-
h2GPI antibody provides additional information in patients
with thrombosis in conjunction with the LAC or aCL
antibody.
References
[1] Wilson WA, Gharavi AE, Koike T, Lockshin MD, Branch DW, Piette
JC, et al. International consensus statement on preliminary classifica-
tion criteria for definite antiphospholipid syndrome: report of an in-
ternational workshop. Arthritis Rheum 1999;42(7):1309–11.
[2] Cabral AR, Cabiedes J, Alarcon-Segovia D. Antibodies to phospho-
lipid-free beta 2-glycoprotein-I in patients with primary antiphospho-
lipid syndrome. J Rheumatol 1995;22(10):1894–8.
[3] Tsutsumi A, Matsuura E, Ichikawa K, Fujisaku A, Mukai M, Kobaya-
shi S, et al. Antibodies to beta 2-glycoprotein I and clinical manifes-
tations in patients with systemic lupus erythematosus. Arthritis
Rheum 1996;39(9):1466–74.
[4] Atsumi T, Ieko M, Bertolaccini ML, Ichikawa K, Tsutsumi A, Mat-
suura E, et al. Association of autoantibodies against the phosphatidyl-
serine–prothrombin complex with manifestations of the antiphospho-
lipid syndrome and with the presence of lupus anticoagulant. Arthritis
Rheum 2000;43(9):1982–93.
[5] Hochberg MC. Updating the American College of Rheumatology
revised criteria for the classification of systemic lupus erythematosus
[letter]. Arthritis Rheum 1997;40:1725.
[6] Brandt JT, Barna LK, Triplett DA. Laboratory identification of lupus
anticoagulants: results of the Second International Workshop for Iden-
tification of Lupus Anticoagulants. On behalf of the Subcommittee on
Lupus Anticoagulants/Antiphospholipid Antibodies of the ISTH.
Thromb Haemost 1995;74(6):1597–603.
[7] Amigo MC, Khamashta MA. Antiphospholipid (Hughes) syndrome
in systemic lupus erythematosus. Rheum Dis Clin North Am 2000;
26(2):331–48.
[8] Audrain MA, El-Kouri D, Hamidou MA, Mioche L, Ibara A, Lan-
glois ML, et al. Value of autoantibodies to beta(2)-glycoprotein 1 in
the diagnosis of antiphospholipid syndrome. Rheumatology (Oxford)
2002;41(5):550–3.
[9] Schved JF, Dupuy-Fons C, Biron C, Quere I, Janbon C. A prospective
epidemiological study on the occurrence of antiphospholipid anti-
body: the Montpellier Antiphospholipid (MAP) Study. Haemostasis
1994;24(3):175–82.
[10] Tsutsumi A, Ichikawa K, Matsuura E, Sawada KI, Koike T. Hetero-
geneous behavior of anti-beta2-glycoprotein I antibodies on various
commercially available enzyme immunoassay plates coated with be-
ta2-glycoprotein I. J Rheumatol 2000;27(2):391–6.
[11] Petri M. Thrombosis and systemic lupus erythematosus: the Hopkins
Lupus Cohort perspective. Scand J Rheumatol 1996;25(4):191–3.
[12] Lewis S, Keil LB, Binder WL, DeBari VA. Standardized measure-
ment of major immunoglobulin class (IgG, IgA, and IgM) antibodies
to beta2glycoprotein I in patients with antiphospholipid syndrome.
J Clin Lab Anal 1998;12(5):293–7.
[13] Nojima J, Kuratsune H, Suehisa E, Futsukaichi Y, Yamanishi H,
Machii T, et al. Association between the prevalence of antibodies to
beta(2)-glycoprotein I, prothrombin, protein C, protein S, and annexin
V in patients with systemic lupus erythematosus and thrombotic and
thrombocytopenic complications. Clin Chem 2001;47(6):1008–15.