Diagnosis and Treatment of Peripheral Arterial Disease 高雄長庚醫院心臟內科...
82
Diagnosis and Treatment of Peripheral Arterial Disease 高高高高高高高高高高 高高高高高
-
Upload
silvia-payne -
Category
Documents
-
view
245 -
download
5
Transcript of Diagnosis and Treatment of Peripheral Arterial Disease 高雄長庚醫院心臟內科...

Diagnosis and Treatment of Peripheral Arterial Disease
高雄長庚醫院心臟內科傅懋洋教授


Leg Ulcers Differential Diagnosis• Vascular Arterial Atherosclerosis obliterans Thromboangiitis obliterans Hypertensive arteriolar Venous• Vasculitis• Diabetic Mellitus• Infection• Pressure (impaired sensation)• Hematological diseases• Neoplastic diseases

Leg Claudication
Unusual causesAortic dissection Temporal arteritisFibromuscular dysplasia Takayasu arteritisRetroperitoneal fibrosis Popliteal cystic diseaseRadiation fibrosis Popliteal entrapmentAbdominal coarctation Ergot intoxicationAortic neurofibromatosis TraumaPrimary artery tumor Miscellaneous

Peripheral Arterial Disease
• Atherosclerotic occlusion of the arteries to the legs• Important manifestation of systemic atherosclerosis• Prevalence : 12% ( Age adjusted)• Affect man and woman equally• Had the same risk of death as patient with CAD• The severity of PAD is closed associated with MI,
CVA and death from vascular causes

Atherosclerosis Obliterans
• Responsible to etiology in 50-90% of patients• Patients may have multiple risk factors• Two types of involvement• Patients with diffuse involvement have a high incidence of coronary artery disease and death from myocardial infarction
Chronic Occlusive Arterial Diseases

Prevalence of Peripheral Arterial Disease, Claudication and Associated Cardiovascular Diseases
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

Risk of Death from All Causes and from Cardiovascular Causes in Patients with Peripheral Arterial Disease
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

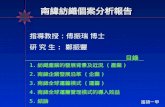
Atherothrombosis: a Generalized and Progressive ProcessAtherothrombosis: a Generalized and Progressive Process
NormalNormalFattyFattystreakstreak
FibrousFibrousplaqueplaque
Athero-Athero-scleroticscleroticplaqueplaque
PlaquePlaquerupture/rupture/fissure &fissure &
thrombosisthrombosis MIMI
IschemicIschemicstroke/*TIA stroke/*TIA
Critical leg Critical leg ischemiaischemia
Clinically silentClinically silent
CardiovascularCardiovasculardeathdeath
Increasing ageIncreasing age
Intermittent claudicationIntermittent claudication
UnstableUnstableanginaangina
*ACS, acute coronary syndrome; TIA, transient ischemic attack
Stable anginaStable angina

Major Clinical Manifestations of Atherosclerotic Disease
Major Clinical Manifestations of Atherosclerotic Disease
TIA, Ischemic stroke
Unstable angina pectorisQ-wave & none Q-wave MI
Renovascular diseaseRenovascular disease
- Cold sensation, numbness - Intermittent claudication - Rest pain, gangrene, amputation- Critical limb ischemia
- Cold sensation, numbness - Intermittent claudication - Rest pain, gangrene, amputation- Critical limb ischemia
Intestinal IschemiaIntestinal Ischemia
Erectile dysfunctionErectile dysfunction
Peripheral Arterial Occlusive Disease (PAOD)

重松宏 ( 東京大 ), Therapeut. Res., 13, 4099, 1992
HypertensionDM
IHDCVD
22.5%
49.7%
28.2%
23.2%
PAOD 與相關疾病之合併率PAOD 與相關疾病之合併率
PAOD

Associated Cardiovascular Conditions• History of MI/Angina• Recent onset or difficult to control H/T ( renovascular hypertension ) • Postprandial pain, weight loss, change in bowel habits ( mesenteric ischemia )• Impotence in man ( Leriche syndrome )• History of stroke / TIA
Atherosclerosis Obliterans

Peripheral Arterial Occlusive DiseasesPeripheral Arterial Occlusive Diseases
患者背景
糖尿病高血壓高脂血症老年人
血流量低下 機能低下 組織壞死
Fontaine I Fontaine II Fontaine III Fontaine IVFontaine I Fontaine II Fontaine III Fontaine IV
血小板
動脈管壁損傷
於損傷處聚集 形成血塊 管徑 50% 狹窄
面積 75% 狹窄
Resting Pain
IntermittentClaudication
NumbnessCold sensationRaynauld’s syndrome
管徑 60% 狹窄面積 82% 狹窄
Ulcer
Gangrene
Fontaine’sFontaine’s
ClassificationClassification

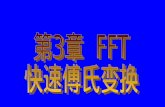
Weighted mean prevalence of intermittent claudication in large population-based studies
Weighted mean prevalence of intermittent claudication in large population-based studies
0
1
2
3
4
5
6
7
8
30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74
Age-group
Prev
alen
ce (
%)
* Overall prevalence for men and women aged 55~74: 4.5%

Thromboangiitis Obliterans Buerger Disease• Occurs in young ( 30 - 40 years old )• Man : women = 95 : 5• Heavy smoker• Affects small arteries and vein• Upper and lower extremities involvement• Progresses proximally• More prevalent in oriental population• Cessation of smoking will arrest it

Thromboangiitis ObliteransBuerger Disease

Differential Diagnosis Atherosclerosis Thromboangiitis
Artery large smallCourse slow rapidSymptoms less severe more severeClaudication calf, thigh, hip foot, archArm usually not often Phlebitis not may involveRevascularization possible notAmputation may occur often occurAssociated CAD often notDeath from MI often rare
Chronic Occlusive Arterial Diseases

Atherosclerosis Obliterans Risk Factors• Cigarettes smoking• Diabetic Mellitus• Hyperlipidemia• Hypertension• Family History• Oral contraceptives
Chronic Occlusive Arterial Diseases

PAODPAOD 的臨床診斷的臨床診斷PAODPAOD 的臨床診斷的臨床診斷自覺症狀 :
1. cold sensation ( 冷感 ), numbness( 酸麻 ), pain( 疼痛 )
2. Intermittent claudication ( 間歇性跛行 )
醫師診斷 :
1. 視診:下肢體表溫差、色差及毛髮生長狀況 2. 血管脈搏觸診: Dorsal pedis 、 Posterior tibial artery 、 Popliteal artery 、 Radial artery
3. 間歇性跛行問卷 4. 周邊血管超音波檢查 : ABI index (Ankle-Brachial Index)
5. PVR or PWV
6. Treadmill Exercise Tests
7. Angiography 或 MRI/MRA

Chronic Occlusive Arterial Diseases Manifestations• Claudication• Ischemia Resting pain Ischemic neuropathy Ulcerations Gangrene• Microcirculatory lesions• Impotency

Claudication• Sterotyped distress• Exercise - induced• Reproducible• Relieved by rest
Chronic Occlusive Arterial Diseases

Intermittent Claudication : 患者於步行 100~200 m 後,因下肢肌肉疼痛而無法繼續行走,但於坐下休息一會兒後,疼痛即自行消失
病患自覺症狀 (Subjective symptoms)
病患自覺症狀 (Subjective symptoms)

Pseudoclaudication• Exercise or position induced• Discomfort often dysthetic• Clumsiness may accompany• Specific position may relieve• Reset relief slow
Chronic Occlusive Arterial Diseases

Claudication Variants• ?Vasospastic • Pseudoclaudication Neurologic Myogenic
Chronic Occlusive Arterial Diseases

Arteries of the Pelvis and Lower ExtremityArteries of the Pelvis and Lower Extremity
Aorta or Iliac Artery
Femoral Artery or Branches
Popliteal Artery
Obstruction in:Obstruction in: Ischemia in:Ischemia in:
Buttock Hip Thigh
Thigh Calf
Calf Ankle Foot
Common Sites of ClaudicationCommon Sites of Claudication

Vascular Examination
• Pulses• Bruit• Color Changes• Trophic changes

Posterior tibial arteryPosterior tibial arteryPopliteal arteryPopliteal artery
PAODPAOD 的臨床診斷的臨床診斷 -- 血管脈搏觸診PAODPAOD 的臨床診斷的臨床診斷 -- 血管脈搏觸診
Dorsal pedisDorsal pedis

Grade system of pulses 0 = absent 1 = markedly decreased 2 = moderately decreased 3 = mildly decreased 4 = normal 5 = aneurysm( 0 - 4 : 2 = mildly decreased, 3 = normal, 4 = aneurysm )
The Arterial Examination

Elevation Dependence Test
Elevation: 60 degree for 60 seconds
Dependence: Venous filling time Dependent Rubor


Elevation Pallor 60 degrees elevation for 60 seconds
0 No pallor 60 1 Pallor 60 2 Pallor 30 - 60 3 Pallor under 30 4 Pallor leg level
The Arterial Examination

Venous Filling Time
0-15? Normal
15-30? Mild - good healing
30-45? Moderate - slow healing
>60? Severe - healing rare
The Arterial Examination

Arterial Vascular Laboratory
• Doppler signal• Pulse trace• Segmental systolic pressure• Segmental pressure indices• Exercise • Color flow mapping• Duplex scan• Arteriography

Ankle Brachial Index
Ankle Systolic Blood Pressure
Brachial Systolic Blood Pressure
= ABI

非侵入性動脈硬化篩檢儀 (VP-1000)非侵入性動脈硬化篩檢儀 (VP-1000)
ABI : stenosis of lower limb.
ABI =Ankle Systolic Blood Pressure
Brachial Systolic Blood Pressure
PWV =Distance between two sites
Pulse wave Transmit Time(PTT)
PWV : Arterial Stiffness
< 0.9
>1400cm/s

Segmental Systolic Pressure

Right ABIHigher right-ankle pressure
Higher arm pressure
Left ABIHigher left-ankle pressure
Higher arm pressure
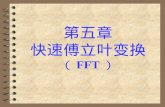
Interpretation of ABI
Noncompressible
Normal
Mild-to-moderate peripheralarterial disease
Severe peripheral arterialdisease
> 1.30
0.91–1.30
0.41–0.90
0.00–0.40
Left-armsystolic pressure
Right-armsystolic pressure
DP
PT
Right-anklesystolic pressure
DP
PT
Left-anklesystolic pressure
Measurement of the Ankle–Brachial Index (ABI)Measurement of the Ankle–Brachial Index (ABI)
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

Symptoms SLP, mmHg ABI
Claudication 70 - 100 0.5 - 0.8 Rest pain < 50 0.3 Gangrene 0 - 30 < 0.2SLP = Segmental limb pressureABI = Ankle brachial index
The Arterial Examination

Angiography

Uncomplicated Claudication
Natural History
Authors Cases Unchanged Worse Amputation Followed
Imperato 104 82% 22% 6% 5 - 8 yrs
Richards 106 69% 24% 7% 5 + yrs
Juergens 104 93% 7% 7% 5 + yrs
Framingham 4% 8.3 yrs
Boyd 1440 7% 5 + yrs

Uncomplicated Occlusive Femoral Artery 5 - 9 years Follow Up
Diabetics Non-diabeticsUlceration 12% 5%Gangrene 40% 5%Amputation 27% 7%5 yr survival 54% 75%9 yr survival 38% 59%
Chronic Occlusive Arterial Diseases

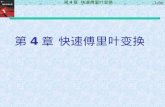
Adapted from Weitz Jl. Circulation. 1996;94:3026-49.
Population >55 y
Intermittent claudication40%
PAD outcomes
Cardiovascular
morbidity/mortality
Worsening claudication
16%
Leg bypass surgery
7%
Major amputation
4%
Nonfatal events
(MI/stroke) 20%
Mortality 30%
Critical leg ischemia
10%
Asymptomatic 50%
Stable claudication 73%
(5-year outcomes)
Clinical Outcomes in Patients With PAODClinical Outcomes in Patients With PAOD

Atherosclerosis Obliterans
Conservative Treatment
Definite value Probable value No proven value
General measures Control of Fibrinolytic therapyStop smoking Diabetics Mellitus Anticoagulant RxExercise regimens Hypertension Vasodilators Hyperlipidemia Calcium blocker Antiplatelet Rx ?

No symptoms Symptoms or signs at rest Disabled for occupation
Conservative treatment
Symptoms improved Progression Surgery or stabilize of symptoms Angioplasty
Atherosclerosis Obliterans

Foot CareTrauma causes more than 50% of amputation Avoid trauma: mechanical, thermal, chemical Keep foot warm, clean, dry Nails: trim straight across Callouses: podiatry whetstone Dry skin: simple emollients Socks: comfortable, absorbent Shoes: comfortable, break in Tinea: control Wound: prompt care
Chronic Occlusive Arterial Diseases

Claudication
Role of Exercise 129 patients 30 - 60 min/day, 3x week Results of 3 months % Treadmill Location improvement Aortic-iliac 205 Distal 247 Combined 230

Role of Cigarette Smoking at 5 years
Amputation %
Aortic-iliac Femoral
Continued 5.9 14.8
Ceased 0 0
Claudication

Aggressive Treatments• Percutaneous transluminal angioplasty• Atherectomy: rotational directional• Intraarterial stent• Laser angioplasty• Surgical revascularization• Sympathectomy ( periarterial )• Amputation
Atherosclerosis Obliterans

Percutaneous Transluminal Angioplasty

Peripheral Arterial Stent

Percutaneous Transluminal Angioplasty
Results
Iliac Femo-PoplitealImmediate 85-90% 80-90%1 year 75-80% 60-65%2 year 65-75% 50-55%5 year 50% -

Indications for Surgery• Limiting claudication• Progression of symptoms• Resting pain• Ulcer and gangrane change• Distal microembolization
Atherosclerosis Obliterans

Atherosclerosis Obliterans Drug TreatmentModification of risk factors: Smoking cessation Treatment of Hyperlipidemia Treatment of Diabetic Mellitus Treatment of Hypertension• Antiplatelet drug therapy Aspirin Ticlopidine Clopidogrel• Vasodilator drug• Pentoxifyline• Cilostazol• Naftidrofuryl• Levocarnitine and Propionyl Levocarnitine• Prostagladins
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

Drug Therapy for Claudications
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

Drug Therapy for Claudications
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

Cilostazol• Inhibit phosphodiesterase type 3
• Increase intrcellular concentration of cyclic AMP
• Inhibit platelet aggregation
• Inhibit formation of arterial thrombi
• Inhibit vascular smooth muscle proliferation
• Produce vasodilation
Drugs Therapy for Claudications
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

Drugs Therapy for Claudications
Side Effects of Cilostazol
• Headache
• Transient diarrhea
• Palpitation
• Dizziness
Hiatt,W.R.: N Engl J Med, 344(21), 1608, 2001

Evaluation of Patients in Whom PAD is Suspected

Evaluation and Treatment of Patients with Proved Peripheral Arterial Disease
Peripheral arterial diseasePeripheral arterial disease
Assess cardiovascular risk factors
Assess cardiovascular risk factors
Assess severity of claudication Treadmill MWD and PFWD SF-36 and WIQ questionnaires
Assess severity of claudication Treadmill MWD and PFWD SF-36 and WIQ questionnaires
Critical leg ischemiaCritical leg ischemia
Risk-factor modification Smoking cessation LDL cholesterol < 100 mg/dl Glycosylated hemoglobine < 7.0% Blood pressure < 130/85 mmHg Angiotensin-converting- enzyme inhibition Antiplatelet therapy Aspirin or clopidogrel
Risk-factor modification Smoking cessation LDL cholesterol < 100 mg/dl Glycosylated hemoglobine < 7.0% Blood pressure < 130/85 mmHg Angiotensin-converting- enzyme inhibition Antiplatelet therapy Aspirin or clopidogrel
Therapy for claudication Supervised exercise CilostazolCilostazol
Therapy for claudication Supervised exercise CilostazolCilostazol
Symptoms improve
Symptoms improve
Symptoms worsen
Symptoms worsen
ContinueContinue Localize the lesion Hemodynamic localization Duplex ultrasonography Magnetic resonance angiography Conventional angiography
Localize the lesion Hemodynamic localization Duplex ultrasonography Magnetic resonance angiography Conventional angiography
Revascularization
Angioplasty
Bypass surgery
Revascularization
Angioplasty
Bypass surgeryHiatt WR. N Engl J Med, Vol. 344, No. 21, May, 2001

Acute Arterial Occlusion

Acute Arterial Occlusion
Pulseless Pale Pain Paresthesia Paraplegia

Acute Arterial Occlusion
PresentationAsymptomatic loss of pulse
Reduction of claudication distance
Tissue ischemia

Acute Arterial Occlusion
Determinants of PresentationSite of occlusion
Status of collaterals
Status proximal, distal beds
Subsequent clot propagation
Suddenness of occlusion
Duration of ischemia

Physical FiningsAbsent pulse
Distal ischemia: of varying degree
Skin: cool, pale, mottled
Muscle: weakness, tender
Nerve: sensory? motor loss
Acute Arterial Occlusion

Etiology
Trauma
Embolism
Thrombosis in situ
Acute Arterial Occlusion

Acute Arterial OcclusionCommon Causes
Thrombosis Occlusive arterial disease Aneurysmal arterial disease Embolism Atrial fibrillation, Left atrial thrombus ( MS ) Ventricular thrombus ( MI, cardiomyopathy, aneurysm) Arterial aneurysm Arterial occlusive diseases Endocarditis Prosthetic valve

Acute Arterial OcclusionUnusual Embolic Sources
CardiacMyxomaCardioversionCatheter, etcProsthetic materials
Paradoxical venous Miscellaneous:
Air, BulletsTumorParasites

Acute Arterial OcclusionAcute Arterial Occlusion ThrombosisUsual causes:
Atherosclerotic occlusive diseases
Atherosclerotic aneurysmal diseases
Dissection of aorta
Unusual causes:
Degenerative, dysplatic arteriopathy
Fibromuscular dysplasia
Ehler?Danlos syndrome
Cystic diseases of femoral, popliteal artery

Acute Arterial OcclusionAcute Arterial Occlusion ThrombosisUnusual causes:
Inflammatory Thromboangiitis obliteransGiant cell arteritisNecrotizing arteritis
Polyarteritis nodosaSystemic lupus erythematosus
HematologicPolycythemia vera, DysproteinemiaThrombocytosis, DIC

Acute Arterial OcclusionThrombosis
MechanicalLocal traumaInvasive diagnostic, therapeutic procedureUnusual muscular effort ( anterior compartment syndrome )Entrapment by bone, muscle, ligamentThoracic outlet syndrome
MiscellaneousMaligancyInfection, debilityCongestive heart failure, ShockErgotism

Acute Arterial OcclusionDifferential Diagnosis
Acute aortic dissectionChest painBranch vessel deficitsWide mediastinum
Low cardiac outputFour limbs involveHypotension, tachycardiaClinical settings
Ergot intoxication
Always ask

Acute Arterial Occlusion
Differential DiagnosisDeep vein Acute arterialthrombosis occlusion
Temp. Normal, increased Decreased
Color Normal, cyanotic Pallor
Edema Present Absent
Pulses Present Absent
V. pattern Distended Collapse

Acute Arterial OcclusionThrombosis vs Embolism
Thrombosis in situ
History: Antecedent claudication
Examinations: Proximal vessels or other limb show
occlusive disease Embolism
Exclude thrombosis in situ
Examine: test for embolic sourceAneurysmal disease can occlude locally throw emolic distally
Embolism may be superimposed on thrombosis

Acute Arterial Occlusion
Surgical Approach Thrombosis
Occlusive disease or aneurysm: often requireArteriographyReconstructive surgery
EmbolismWith good inflow, runoff, no proximal aneurysm
Arteriography not needLocal anesthesiaFogarty catheter removal feasible

Acute Arterial Occlusion
Initial Therapy Treat underlying disease Protect collaterals Heparinization immediately Thrombolytic therapy? Protect from trauma
mechanialthermalchemical

Therapeutic Decision Risk of underlying diseases Urgency of surgery Risk of surgery
Risk of amputation
Role of forgarty catheter
Acute Arterial OcclusionAcute Arterial Occlusion

Role of Anticoagulants Prevent clot propagation Control embolic source Minimize venous
thromboembolism
Acute Arterial Occlusion

Paradoxical Emolism
Proved:
Venous clot lodged in the intracardiac
defect at autopsy Presumptive:
Venous thrombosis / embolism
Intracardiac shunt allowing R to L shunt
Arterial embolism without evidence of
origin in left side of heart or systemic
circulation

The Arterial Examination
Pulses
Bruits
Aneurysms

ExtensionsAllen testPerfusion test ( Elevation dependance test )Exercise testThoracic outlet maneuvers
The Arterial Examination

Localization Site Symptoms Aorta Buttocks, back, thighs, calves Iliac Buttocks, thigh, calf Int. Iliac Buttocks C. Femoral Thighs S. Femoral 2/3 calf, foot Popliteal 1/3 calf, foot Tibial Foot, ankle
The Arterial Examination

Thank you for Your Attention