Developmental - ערוץ המו"פ | דף הביתweb.macam.ac.il/~offprint/79898.pdf · and...
5
" Developmental dyscalculia: a prospective six-year follow-up -. Ruth S Shalev* MD, Neuropaediatric Unit, Shaare Zedek , Medical Centre; OrlyManor PhD, Braun School of Public Health and Community Medicine, Hebrew University, Hadassah; Varda Gross-Tsur MD, Neuropaediatric Unit, Shaare Zedek :~-MedicalCentre, Jerusalem, IsraeL , *Correspondence tofirst author at Neuropaediatric Unit, . Shaare Zedek Medical Centre, PO Box 3235, Jerusalem 91031, IsraeL E-mail:[email protected] .. To determine the natural history of developmental dyscalculia (DC)and factors impacting on its prognosis, we performed a prospective six-year longitudinal study. One hundred and forty children of normal intelligence diagnosed with DC in the fifth grade of elementary school were re-examined for dyscalculia three and six years later, in eighth (n=123) and eleventh (n=104; 41 males, 63 females) grades respectively. Mean age of the children in fifth grade was 11 years 1 month (SD4 months), in eighth grade 14 years 2 months (SD 1 month), and in eleventh grade 17 years 2 months (SD 5 months). The assessment included standardized arithmetic, reading and writing tests, behavioural rating scales, information on socioeconomic status, educational interventions, and familial learning problems. Participants in eleventh grade were recategorized as having DC if their score on the arithmetic test was not more than the fifth centile for grade. At the six-year follow-up, 99/104 (95%) children diagnosed with dyscalculia in fifth grade were still performing poorly in arithmetic, scoring within the lowest quartile for their grade, and 42/104 (40%) were recategorized with DC. Chronicity of DC was associated with severity of the dyscalculia in fifth grade (p<0.05), lower IQ (p<0.01), inattention (p<0.01), and writing problems (p<0.01). Thns, DCis an enduring specific learning difficulty,* persisting into late adolescence in almost half of affected individuals. *Developmental dyscalculia is a 'specific learning difficulty', rather than a 'learning disability/mental retardation'. Developmental dyscalculia (DC) is a specific learning diffi- culty manifested by failure to achieve adequate proficiency in arithmetic despite normal intelligence, scholastic opportu- nity, emotional stability, and sufficient motivation (American Psychiatric Association 1994). Epidemiological, genetic, and neurobiological studies indicate that DC, like other specific learning difficulties, is a brain-based disorder affecting as many as 5% of the school-age population (Badian and Ghublikian 1983, Shalev and Gross-Tsur 2001). Despite its prevalence, and the importance of adequate arithmetic skills for everyday life (Geary 1993), there is no information about the long-term outcome of DC. We found, however, that in a short-term follow-up of three years, dyscalculia persists in about half of affected children (Shalev et al. 1998). Because the consequences of specific learning difficulties for the individual and society at large are immeasurable (Lyon 1995), knowledge of the long-term prognosis of DC is important. The objectives of our prospective, six-year fol- low-up study were to determine the natural history of DC and factors impacting on its prognosis in a large cohort of affected individuals. Method Three thousand and twenty-nine fourth-grade children attend- ing mainstream city schools underwent testing of arithmetic skills (Gross-Tsur et al. 1996) 140 were classified as having DC and formed our study group (Fig. 1). DC was determined by using a two-stage screening process. In the first stage, all 3029 fourth-grade children (mean age 10 years) took a group- administered arithmetic achievement test which assessed counting skills, knowledge of number facts, and ability to solve complex arithmetic exercises and word problems (this initial screening device was developed by the Jerusalem School System). Of the 600 children scoring in the lowest 20% on this test, 550 entered the second stage, which took place in fifth grade when the children were aged 11years 1 month (standard deviation [SD]4 months). Each of them was individuallyadmin- istered an arithmetic battery, standardized on age-matched controls (Shalev et al. .1993).Achild was diagnosed as having DC ifhis or her Full-scale IQ was at least 80 and the score achieved on the second arithmetic battery was in the lowest fifth centile for school grade. One hundred and forty children fulfilled the diagnostic criteria for DC and underwent further testing, whi<;h included reading and writing evaluations, an IQ test (Wechsler Intelligence Scale for Children: WISC-R;Wechsler 1974), neuropsychological tests assessing language and sequen- tial skills (ten-word learning test [Christensen-Pisskov 1974], word-fluency test [Spreen and Strauss 1991], Kaufman sequen- tial hand movement tasks [Kaufman and Kaufman 1983], fin- ger tapping [McCarthy 1972]), and non-verbal visuospatial tests (Rey-osterreith Complex Figure Test - copy and mem- ory [Osterreith 1944], Facial Recognition Test [Levin et al. 1965], and a test of executive functioning - trail making form A and B [Golden et al. 1981]). Parents provided information about socioeconomic status, including profession and years of education (Gross-Tsur et al. 1996). Three years later, when the children were aged 14 years 2 months (SD 1 month) and studying in eighth grade, 123/140 (88%) members of the original cohort were re-studied (Shalev et al. 1998). They were evaluated for proficiency in arithmetic, reading, and spelling (Shalev et al. 1998); parent and teacher Abbreviated Behavior Rating Scale (Conners 1973) and a Developmental Medicine & Child Neurology 2005, 47: 121-125 121
Transcript of Developmental - ערוץ המו"פ | דף הביתweb.macam.ac.il/~offprint/79898.pdf · and...
" Developmentaldyscalculia: aprospective six-yearfollow-up
-. Ruth S Shalev* MD, Neuropaediatric Unit, Shaare Zedek, MedicalCentre;
OrlyManor PhD, Braun School of Public Health andCommunity Medicine, Hebrew University, Hadassah;VardaGross-Tsur MD, Neuropaediatric Unit, Shaare Zedek
:~-MedicalCentre, Jerusalem, IsraeL
, *Correspondence tofirst author at Neuropaediatric Unit,. Shaare Zedek Medical Centre, PO Box 3235, Jerusalem
91031, IsraeLE-mail:[email protected] ..
Todetermine the natural history of developmental dyscalculia(DC)and factors impacting on its prognosis, we performed aprospective six-year longitudinal study. One hundred andforty children of normal intelligence diagnosed with DCin thefifth grade of elementary school were re-examined fordyscalculia three and six years later, in eighth (n=123) andeleventh (n=104; 41 males, 63 females) grades respectively.Meanage of the children in fifth grade was 11 years 1 month(SD4 months), in eighth grade 14 years 2 months (SD 1month), and in eleventh grade 17 years 2 months (SD 5months). The assessment included standardized arithmetic,reading and writing tests, behavioural rating scales,information on socioeconomic status, educationalinterventions, and familial learning problems. Participants ineleventh grade were recategorized as having DC if their scoreon the arithmetic test was not more than the fifth centile forgrade. At the six-year follow-up, 99/104 (95%) childrendiagnosed with dyscalculia in fifth grade were still performingpoorly in arithmetic, scoring within the lowest quartile fortheir grade, and 42/104 (40%) were recategorized with DC.Chronicity of DCwas associated with severity of thedyscalculia in fifth grade (p<0.05), lower IQ (p<0.01),inattention (p<0.01), and writing problems (p<0.01). Thns,DCis an enduring specific learning difficulty,* persisting intolate adolescence in almost half of affected individuals.
*Developmental dyscalculia is a 'specific learning difficulty',rather than a 'learning disability/mental retardation'.
Developmental dyscalculia (DC) is a specific learning diffi-culty manifested by failure to achieve adequate proficiency inarithmetic despite normal intelligence, scholastic opportu-nity, emotional stability, and sufficient motivation (AmericanPsychiatric Association 1994). Epidemiological, genetic, andneurobiological studies indicate that DC, like other specificlearning difficulties, is a brain-based disorder affecting asmany as 5% of the school-age population (Badian andGhublikian 1983, Shalev and Gross-Tsur 2001). Despite itsprevalence, and the importance of adequate arithmetic skillsfor everyday life (Geary 1993), there is no information aboutthe long-term outcome of DC. We found, however, that in ashort-term follow-up of three years, dyscalculia persists inabout half of affected children (Shalev et al. 1998). Becausethe consequences of specific learning difficulties for theindividual and society at large are immeasurable (Lyon1995), knowledge of the long-term prognosis of DC isimportant. The objectives of our prospective, six-year fol-low-up study were to determine the natural history of DCand factors impacting on its prognosis in a large cohort ofaffected individuals.
Method
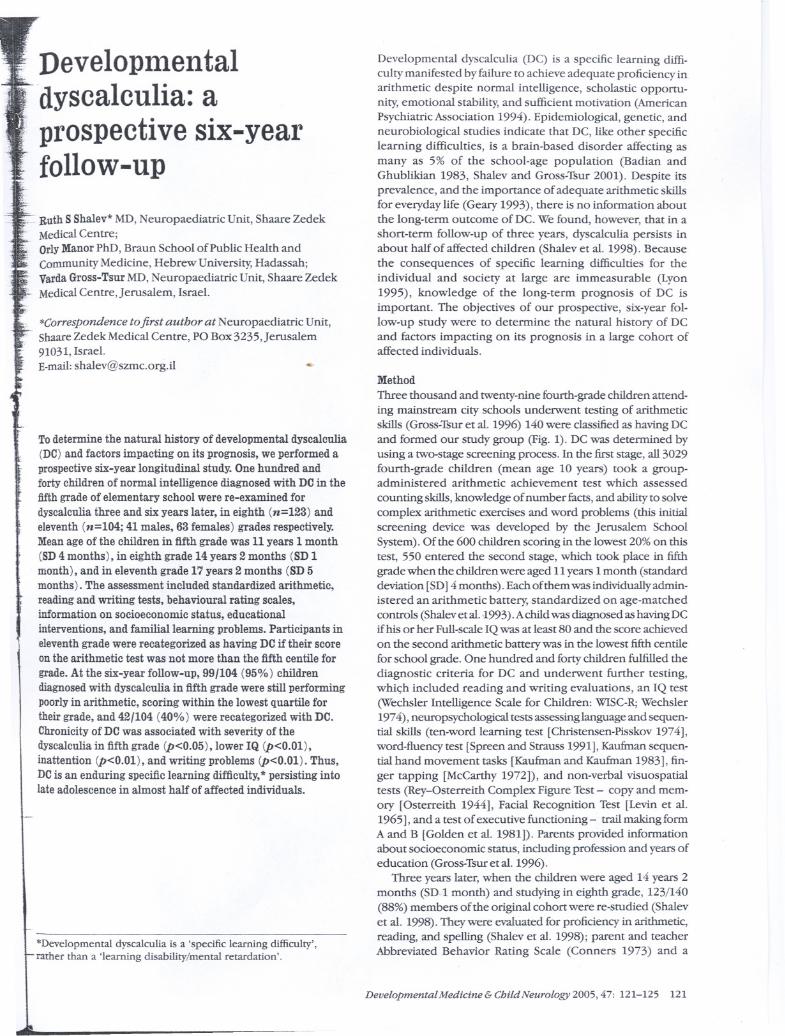
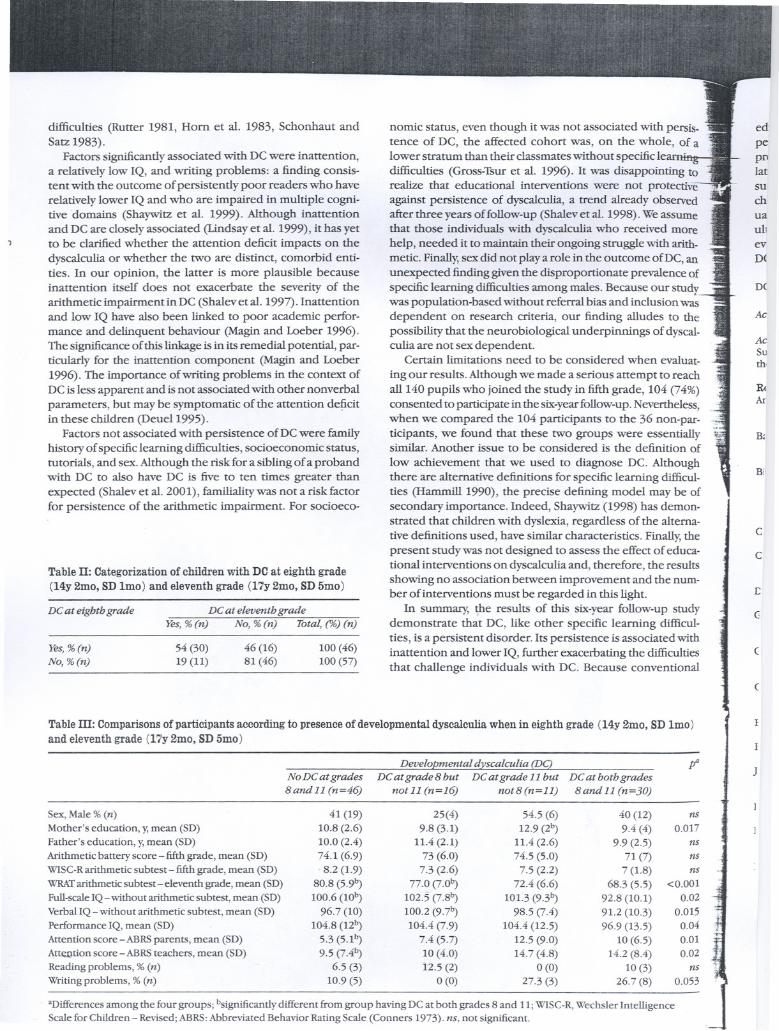
Three thousand and twenty-nine fourth-grade children attend-ing mainstream city schools underwent testing of arithmeticskills (Gross-Tsur et al. 1996) 140 were classified as having DCand formed our study group (Fig. 1). DC was determined byusing a two-stage screening process. In the first stage, all 3029fourth-grade children (mean age 10 years) took a group-administered arithmetic achievement test which assessed
counting skills, knowledge of number facts, and ability to solvecomplex arithmetic exercises and word problems (this initialscreening device was developed by the Jerusalem SchoolSystem). Of the 600 children scoring in the lowest 20% on thistest, 550 entered the second stage, which took place in fifthgrade when the children were aged 11years 1 month (standarddeviation [SD]4 months). Each of them was individuallyadmin-istered an arithmetic battery, standardized on age-matchedcontrols (Shalevet al. .1993).Achild was diagnosed as having DCifhis or her Full-scale IQ was at least 80 and the score achievedon the second arithmetic battery was in the lowest fifth centilefor school grade. One hundred and forty children fulfilled thediagnostic criteria for DC and underwent further testing,whi<;h included reading and writing evaluations, an IQ test(Wechsler Intelligence Scale for Children: WISC-R;Wechsler1974), neuropsychological tests assessing language and sequen-tial skills (ten-word learning test [Christensen-Pisskov 1974],word-fluency test [Spreen and Strauss 1991], Kaufman sequen-tial hand movement tasks [Kaufman and Kaufman 1983], fin-ger tapping [McCarthy 1972]), and non-verbal visuospatialtests (Rey-osterreith Complex Figure Test - copy and mem-ory [Osterreith 1944], Facial Recognition Test [Levin et al.1965], and a test of executive functioning - trail making formA and B [Golden et al. 1981]). Parents provided informationabout socioeconomic status, including profession and years ofeducation (Gross-Tsur et al. 1996).
Three years later, when the children were aged 14 years 2months (SD 1 month) and studying in eighth grade, 123/140(88%) members of the original cohort were re-studied (Shalevet al. 1998). They were evaluated for proficiency in arithmetic,reading, and spelling (Shalev et al. 1998); parent and teacherAbbreviated Behavior Rating Scale (Conners 1973) and a
Developmental Medicine & Child Neurology 2005, 47: 121-125 121
questionnaire to identify other family members with specif-ic learning difficulties were administered. The results of thisthree year follow-up demonstrated the short-term persis-tence of DC: the arithmetic scores of 95% of the 123 chil-dren fell within the lowest quartile for their class and 57(47%) were re-ascertained as having DC according to theresearch criterion of the lowest fifth centile of their grade(Shalev et al. 1998).
The present follow-up took place sixyears after the diagno-sis of DC was first given, and included 104/140 (74%) partici-pants (41 males and 63 females, aged 17years 2 months (SD 5months) now in eleventh grade; 103 of the participants hadalso been tested at eighth grade. A serious attempt was madeto contact all 140 participants; 19 could not be located and 17refused to participate. To ascertain whether the 36 who didnot participate in the six-year follow-up were similar to thosewho did, we compared their IQ and scores on the arithmeticbattery administered in fifth grade (Le. aged lly 1 mo, SD 4mo). No significant difference was found on Full-scale IQ(mean 96.5, SD 7.4 versus mean 98.3, SD 9.9) or on the arith-metic test (mean 72.9, SD 8.1 versus mean 73, SD 6.8). '
The assessment at the six-year follow-up included stan-dardized arithmetic battery, and reading, and writing tests,Wide Range Achievement Test ID arithmetic subtest (Jastakand Wtlkinson 1984), parent and teacher Abbreviated BehaviorRating Scale, and a questionnaire about educational inter-ventions (tutoring after school hours, school tutorials, orattendance at the resource room). The arithmetic batterywas based on the neurocognitive model of McCloskey et al.(1985), which evaluates number comprehension, numberproduction, number calculation, and arithmetic error types(Shalev et al. 1993, 1998). The arithmetic battery given at the
Figure 1: Six-year follow-up of population with DC.
different grades was essentially identical with the following :;exceptions: at the three- and six-year follow-up, questions Onnumber comprehension and production that had been asSQ:,ciated with small variances at the three-year follow-up werenot included and questions on fractions and decimals were-added for eighth- and eleventh-grade children. A cut-off atthe fifth centile was used to delineate DC so that the resultscould be compared with those of the first two assessments atfifth grade and eighth grade.
For the follow-up, the arithmetic, reading, and spellingevaluations were standardized on 120 tenth-grade childrenwithout specific learning difficulties who served as a controlgroup. The method we used to choose controls ensured rep:-resentation of the populations' diverse socioeconomic sta-tus (Shalev et al. 1993).
Institutional review board approval was received for the study,and informed consent was obtained from the participants.
STATISTICAL ANALYSIS
For statistical analysis, t-tests or X2tests (or Fisher's exact test -,when appropriate) were used to assess the association between ,-
DC classification at eleventh grade and the following poten-tial predictors: sociodemographic characteristics, results ofneuropsychological tests at fifth grade, IQ scores, readingand writing, attention problems, and scores on arithmetictests at fifth grade and eighth grade. Logistic regression wasused for multivariate modeling. ANOVA(including multiplecomparisons using Dunnett's statistic) or X2tests were usedto examine the association between the above-mentioned
predictors and trajectories in DC classifications; polyto-mous regression was used for multivariate examination oftrajectories.
Results
Individuals diagnosed with DC in fifth grade were still perform-ing poorly in arithmetic sixyears later when in eleventh grade,unable to solve even simple arithmetic exercises. Thus, 51% ofthe cohort in eleventh grade (versus 17%of controls) could notsolve '7x8', 71% (versus 27%) could not solve '37x24', 49%(versus 15%) could not solve '45+3', and 63% (versus 17%)were unable to solve '5/~H219'. Furthermore, 40% (n=42) ofthese eleventh-grade pupils scored in the lowest fifth centilefor their grade, meeting the stringent diagnostic criterion ofDC Although the remaining 62 participants scored above thefifth centile, and therefore did not meet the research criterionfor DC, their performance in arithmetic was poor. Most of '
them (57/62) achieved scores within the lowest quartile fortheir grade.
The severity of dyscalculia in eleventh-grade children withDC was reflected in other measures of arithmetic perfor-mance. They achieved significantly lower scores on the stan-dardized arithmetic battery used for diagnosis at grades fiveand eight, on the IQ arithmetic subtest (Wechsler 1974), andon the Wide Range Achievement Test III arithmetic subtest(Jastek and WIlkinson 1984; Table I).
Factors recognized to influence specific learning difficultieswere investigated for their role in the persistence of DC Wefound that lower IQ, inattention, and poor writing were allassociated With persistence of DC (Table I). Thus, Full-scaleIQscores (calculated without the arithmetic subtest) were, onaverage, six points lower in individuals with DC in eleventhgrade. The results of the attention rating scale, scored by
parenDCAtencereadit
bal p~1965)1944)ated ,socic><familJ
w(
ouslyprobJfactO)at ele
val [(IQ,b:the Awas ~ingp
WCtimeachieeleve0.57mod,lowemorttwo I
Fe
grad5ixteeighlwhogradscor.
uInitial assessment3029 fourth-grade children evaluated on group-
administered arithmetic achievement test
t555/600 in lowest 20% of class tested individually on
standardized arithmetic battery
t140 diagnosed with developmental dyscalculia entered
study when in fifth grade (11y 1mo, SO 4mo)(Gross-Tsur et al. 1996)
+
Three-year follow-up123/140 restudied when in eighth grade (14y 2mo,
SO 1 mo). 47% (n--57) were reclassified as dyscalculic(Shalev et al. 1998)
.Six-year follow-up
104/140 restudied when in eleventh grade(17y 2mo, SO 5mo)
40% (n=42) were reclassified as dyscalculic
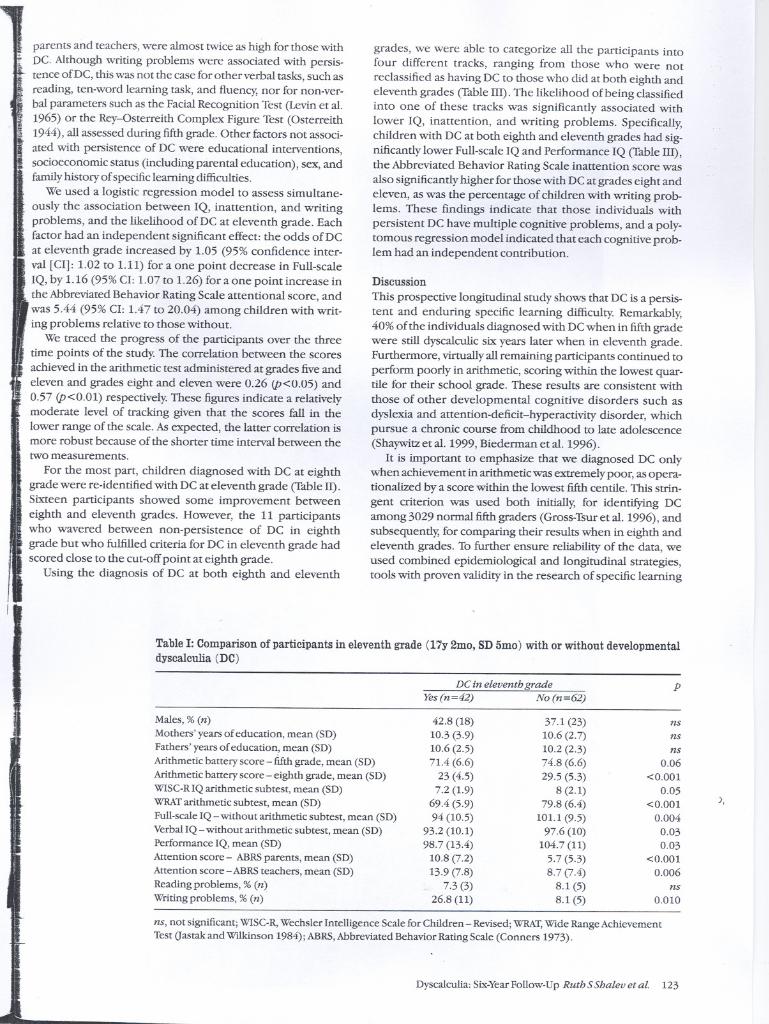
parents and teachers, were almost twice as high for those with,~ DC.Althoughwriting problems were associatedwith persis-
tence of DC, this was not the case for other verbal tasks, such asreading, ten-word learning task, and fluency, nor for non-ver-bal parameters such as the FacialRecognition Test (Levinet al.1965) or the Rey-osterreith Complex Figure Test (Osterreith1944), all assessed during fifth grade. Other factors not associ-ated with persistence of DC were educational interventions,socioeconomic status (including parental education), sex, andfamilyhistory of specific learning difficulties.
We used a logistic regression model to assess simultane-ously the association between IQ, inattention, and writingproblems, and the likelihood of DC at eleventh grade. Eachfactor had an independent significant effect: the odds of DCat eleventh grade increased by 1.05 (95% confidence inter-val [Cl]: 1.02 to 1.11) for a one point decrease in Full-scaleIQ, by 1.16 (95% Cl: 1.07 to 1.26) for a one point increase inthe Abbreviated Behavior Rating Scale attentional score, andwas 5.44 (95% Cl: 1.47 to 20.04) among children with writ-ing problems relative to those without.
We traced the progress of the participants over the threetime points of the study. The correlation between the scoresachieved in the arithmetic test administered at grades five andeleven and grades eight and eleven were 0.26 (p<0.05) and0.57 (p<0.01) respectively. These figures indicate a relativelymoderate level of tracking given that the scores fall in thelower range of the scale. As expected, the latter correlation ismore robust because of the shorter time interval between thetwo measurements.
For the most part, children diagnosed with DC at eighthgrade were re-identified with DC at eleventh grade (Table ll).Sixteen participants showed some improvement betweeneighth and eleventh grades. However, the 11 participantswho wavered between non-persistence of DC in eighthgrade but who fulfilled criteria for DC in eleventh grade hadscored close to the cut-off point at eighth grade.
Using the diagnosis of DC at both eighth and eleventh
grades, we were able to categorize all the participants intofour different tracks, ranging from those who were notreclassified as having DC to those who did at both eighth andeleventh grades (Table Ill). The likelihood of being classifiedinto one of these tracks was significantly associated withlower IQ, inattention, and writing problems. Specifically,children with DC at both eighth and eleventh grades had sig-nificantly lower Full-scale IQ and Performance IQ (Table Ill),the Abbreviated Behavior Rating Scale inattention score wasalso significantly higher for those with DC at grades eight andeleven, as was the percentage of children with writing prob-lems. These findings indicate that those individuals withpersistent DC have multiple cognitive problems, and a poly-tomous regression model indicated that each cognitive prob-lem had an independent contribution.
Discussion
This prospective longitudinal study shows that DC is a persis-tent and enduring specific learning difficulty. Remarkably,40% of the individuals diagnosed with DC when in fifth gradewere still dyscalculic six years later when in eleventh grade.Furthermore, virtually all remaining participants continued toperform poorly in arithmetic, scoring within the lowest quar-tile for their school grade. These results are consistent withthose of other developmental cognitive disorders such asdyslexia and attention-deficit-hyperactivity disorder, whichpursue a chronic course from childhood to late adolescence(Shaywitz et al. 1999, Biederman et al. 1996).
It is important to emphasize that we diagnosed DC onlywhen achievement in arithmetic was extremely poor, as opera-tionalized by a score within the lowest fifth centile. This strin-gent criterion was used both initially, for identifying DCamong 3029 normal fifth graders (Gross-Tsur et al. 1996), andsubsequently, for comparing their results when in eighth andeleventh grades. To further ensure reliability of the data, weused combined epidemiological and longitudinal strategies,tools with proven validity in the research of specific learning
Table I: Comparison of participants in eleventh grade (17y 2mo, SD 5mo) with or without developmentaldyscalculia (DC)
DC in eleventh grade
Ths (n=42) No (n=62)
Males, % (n)
Mothers' years of education, mean (SD)
Fathers' years of education, mean (SD)
Arithmetic battery score - fifth grade, mean (SD)
Arithmetic battery score - eighth grade, mean (SD)
WISC-RIQ arithmetic subtest, mean (SD)
WRAT arithmetic subtest, mean (SD)
Full-scale IQ -without arithmetic subtest, mean (SD)
Verbal IQ - without arithmetic subtest, mean (SD)Performance IQ, mean (SD)
Attention score - ABRS parents, mean (SD)
Attention score - ABRS teachers, mean (SD)
Reading problems, % (n)Writing problems, % (n)
42.8 (18)10.3 (3.9)10.6 (2.5)71.4 (6.6)
23 (4.5)7.2 (1.9)
69.4 (5.9)94 (10.5)
93.2 (10.1)98.7 (13.4)
10.8 (7.2)13.9 (7.8)
7.3 (3)26.8 (11)
37.1 (23)10.6 (2.7)10.2 (2.3)74.8 (6.6)29.5 (5.3)
8 (2.1)79.8 (6.4)
lOLl (9.5)97.6 (10)
104.7 (11)5.7 (5.3)8.7 (7.4)
8.1 (5)8.1 (5)
ns, not significant; WISC-R, Wechsler Intelligence Scale for Children - Revised; WRAT, Wide Range Achievement
Test Oastak and W1lkinson 1984); ABRS, Abbreviated Behavior Rating Scale (Conners 1973).
Dyscalculia: Six-Year Follow-Up Ruth SShalev et al. 123
p
-
nsnsns
0.06<0.001
0.05<0.001 ),
0.0040.030.03
<0.0010.006
ns0.010
difficulties (Rutter 1981, Horn et al. 1983, Schonhaut andSatz 1983).
Factors significantly associated with DC were inattention,a relatively low IQ, and writing problems: a finding consis-tent with the outcome of persistently poor readers who haverelatively lower IQ and who are impaired in multiple cogni-tive domains (Shaywitz et al. 1999). Although inattentionand DC are closely associated (Lindsayet al. 1999), it has yetto be clarified whether the attention deficit impacts on thedyscalculia or whether the two are distinct, comorbid enti-ties. In our opinion, the latter is more plausible becauseinattention itself does not exacerbate the severity of thearithmetic impairment in DC (Shalev et al. 1997). Inattentionand low IQ have also been linked to poor academic perfor-mance and delinquent behaviour (Magin and Loeber 1996).The significance of this linkage is in its remedial potential, par-ticularly for the inattention component (Magin and Loeber1996). The importance of writing problems in the context ofDC is less apparent and is not associated with other nonverbalparameters, but may be symptomatic of the attention de~citin these children (DeueI1995).
Factors not associated with persistence of DC were familyhistory of specific learning difficulties, socioeconomic status,tutorials, and sex. Although the risk for a sibling of a probandwith DC to also have DC is five to ten times greater thanexpected (Shalevet al. 2001), familiality was not a risk factorfor persistence of the arithmetic impairment. For socioeco-
Table n: Categorization of children with DC at eighth grade(14y 2mo, BDlmo) and eleventh grade (17y 2mo, BD5mo)
DC at eighth grade DC at eleventh grade
Ths, % (n) No, % (n) Tota~ (%) (n)
Ths,%(n)No, %(n)
54 (30)19 (11)
46 (16)81 (46)
100 (46)100 (57)
nomic status, even though it was not associated with persis.tence of DC, the affected cohort was, on the whole, of alower stratum than their classmates without specific Idifficulties (Gross-Tsur et al. 1996). It was disappointing torealize that educational interventions were not protectiVe-against persistence of dyscalculia, a trend already observedafter three years of follow-up (Shalev et al. 1998). We assumethat those individuals with dysca1culia who received morehelp, needed it to maintain their ongoing struggle with arith-metic. Finally;sex did not play a role in the outcome of DC, anunexpected finding given the disproportionate prevalence ofspecific learning difficulties among males. Because our study.was population-based without referral bias and inclusion wasdependent on research criteria, our finding alludes to thepossibility that the neurobiological underpinnings of dyscal-culia are not sex dependent.
Certain limitations need to be considered when evaluat-ing our results. Although we made a serious attempt to reachall 140 pupils who joined the study in fifth grade, 104 (74%)consented to participate in the six-yearfollow-up. Nevertheless,when we compared the 104 participants to the 36 non-par-.~.ticipants, we found that these two groups were essentially 'i:similar. Another issue to be considered is the definition of
low achievement that we used to diagnose DC. Althoughthere are alternative definitions for specific learning difficul-ties (Hammill1990), the precise defining model may be ofsecondary importance. Indeed, Shaywitz (1998) has demon-strated that children with dyslexia, regardless of the alterna-tive definitions used, have similar characteristics. Finally; thepresent study was not designed to assess the effect of educa-tional interventions on dysca1culia and, therefore, the resultsshowing no association between improvement and the num-ber of interventions must be regarded in this light.
In summary, the results of this six-year follow-up studydemonstrate that DC, like other specific learning difficul-ties, is a persistent disorder. Its persistence is associated withinattention and lower IQ, further exacerbating the difficultiesthat challenge individuals with DC. Because conventional
Table ill: Comparisons of participants according to presence of developmental dyscalculia when in eighth grade (14y 2mo, BDlmo)and eleventh grade (17y 2mo, BD5mo)
ed
pepolatsuchuaUIIevD<
D(
Ac
AcSuth.
RIAI
Bo
Bi
C
C
:c
<:
(
(
'Differences among the four groups; bsignificantly different from group having DC at both grades 8 and 11; WISC-R, Wechsler IntelligenceScale for Children - Revised; ABRS: Abbreviated Behavior Rating Scale (Conners 1973). ns, not significant.
Developmental dyscalculia (DC) p" I JNo DC at grades DC at grade 8 hut DC at grade 11 but DC at botb grades8 and 11 (n=46) not 11 (n=16) not 8 (n=l1) 8 and 11 (n=30)
Sex, Male % (n) 41 (19) 25(4) 54.5 (6) 40 (12) ns
Mother's education, y,mean (SD) 10.8 (2.6) 9.8 (3.1) 12.9 (2 9.4 (4) 0.017
Father's education, y,mean (SD) 10.0 (2.4) 11.4 (2.1) 11.4 (2.6) 9.9 (2.5) ns
Arithmetic battery score - fifth grade, mean (SD) 74.1 (6.9) 73 (6.0) 74.5 (5.0) 71(7) ns
WISC-Rarithmetic subtest - fifth grade, mean (SD) . 8.2 (1.9) 7.3 (2.6) 7.5 (2.2) 7 (1.8) ns
WRAT arithmetic subtest - eleventh grade, mean (SD) 80.8 (5.9 77.0 (7.0 72.4 (6.6) 68.3 (5.5) <0.001
Full-scale IQ - without arithmetic subtest, mean (SD) 100.6 (lOb) 102.5 (7.8 101.3 (9.3b) 92.8 (10.1) 0.02
Verbal IQ - without arithinetic subtest, mean (SD) 96.7 (10) 100.2 (9.7b) 98.5 (7.4) 91.2 (10.3) 0.015
Performance IQ, mean (SD) 104.8 (12b) 104.4 (7.9) 104.4 (12.5) 96.9 (13.5) 0.04
Attention score - ABRSparents, mean (SD) 5.3 (5.1 7.4 (5.7) 12.5 (9.0) 10 (6.5) 0.01
Atte.Q.tionscore - ABRSteachers, mean (SD) 9.5 (7.4b) 10 (4.0) 14.7 (4.8) 14.2 (8.4) 0.02Reading problems, % (n) 6.5 (3) i2.5 (2) 0 (0) 10 (3) ns
Writing problems, % (n) 10.9 (5) 0 (0) 27.3 (3) 26.7 (8) 0.053
educational interventions did not alter the outcome of DC,perhaps different modes of teaching or early intervention mayprove to be more helpful. In the interim, the use of hand calcu-lators and teaching arithmetic skills necessary for everyday life,such as comprehension of addresses, calendars, or writingcheques, is advisable. Furthermore, focusing on the individ-ual's other strengths may also enhance that individual'sultimate outcome. Hence, our study provides a realistic,evidence-based frame of expectations for those affected withDCas well as for clinicians and educators involved in their care.
DOl: 10.1017/S0012162205000216
Accepted for publication 9th]une 2004.
AcknowledgementsSupported by The Israel Science Foundation, grant No. 74/00 andthe Office of Chief Scientist, Israel Ministry of Health Grant No. 4835.
References
American Psychiatric Association. (1994) Diagnostic and StatisticalManual of Mental Disorders. 4th edn. Washington, DC: AmericanPsychiatricAssodation. p 50-51.
Badian NA, Ghublikian M. (1983) The personal-socialcharacteristics of children with poor mathematical computationskills.] Learn Disabi/l6: 145-157.
BiedermanJ, Faraone S, Milberger S, GuiteJ, MickE, Chen L,Mennin D, MarrsA, Ouellerte C, Moore P,SpencerT, Norman D,Wllens T, Kraus I, PerrinJ. (1996) A prospective 4-year follow-upstUdy of artention-deficit hyperactivity and related disorders.Arch Genpsychiatry 53: 437-446.
Christensen-Pisskov AL. (1974) Luria 's NeuropsychologicalInvestigations. Vojens, Deronark: PJ Schmidts Bogtrykkery.
Conners CK. (1973) Rating scales for use in drug stUdies withchildren. Psychopbarmacol Bull (Special issue: Pharmacotherapyof Children) 9: 24-29.
Deuel RK. (1995) Developmental dysgraphia and motor skillsdisorder.] ChildNeuro/lO (Suppll): S56-558.
Geary DC. (1993) Mathematical disabilities: cognitive,neuropsychological, and genetic components. Psychol Bull114: 345-362.
Golden CJ, OsmanDC, MosesJrJA, BergRA. (1981) Interpretationof the Halstead-Reitan Neuropsychological Test Battery. NewYo~: Grune & Strarton.
Gross- Tsur V,Manor 0, Shalev RS. (1996) Developmentaldyscalculia: prevalence and demographic features. Dev MedChildNeurol38: 25-33.
HammiIl DD. (1990) On defining learning disabilities: an emergingconsensus.] Learn Disabil23: 76-84.
Horn WF, O'DonnellJP, VitUlano lA. (1983) Long-term follow-upstUdies oflearning-disabled persons.] Learn Disabil6: 542-555.
Jastak S, W1lkinson GS. (1984) Wtde Range Achievement TestRevised: Administration Manual. W1lmington, DE: JastakAssociates.
Kaufman AS, Kaufman NL. (1983) KaufmanAssessment Battery forChildren. Circle Pines, MN: American Guidance Service.
Levin HS, Hamsher K de S, BentonAL. (1965) A short form ofthe Test of Facial Recognition for clinical use.] Psychol91: 223-228.
Lindsay RL, Tomazic T, Levine MD, Accardo PJ. (1999) Impact ofattentional dysfunction in dyscalculia. Dev Med Child Neurol41: 639-642.
Lyon GR. (1995) Research initiatives in learning disabilities:contributions from scientists supported by the National InstitUteof Child Health and Human Development.] Child Neurol10 (Suppll): SI20-5126.
Magin E, Loeber R. (1996) Academic performance and itsrelationship to delinquency. In: Cramer SC, Eills W, editors.Learning Disabilities, Lifelong Issues. Baltimore: Paul BrooksPublishing. p 235-240.
McCarthy D. (1972) McCarthy Scales of Children's Abilities. SanAntonio TX: Psychological Corporation.
.
McCloskeyM, CaramazzaA, BasiliA. (1985) Cognitive mechanismsin number processing and calculation: evidence fromdyscalculia. Brain Cogn 4: 171-196.
Osterreith PA. (1944) Le test de copie d'une figure complexe.ArchPsychol30: 206-356. (In French) .
Rutter M. (1981) Epidemiological-LongitUdinal strategies andcausal research in child psychiatry.] AmAcad Child Psychiatry20: 513-544.
Schonhaut S, Satz P. (1983) Prognosis for children with learningdisabilities: a review of follow-up stUdies. In: Rutter M, editor.DevelopmentalNeuropsycholog)l. New York: GuiIford Press,p 542-563.
Shalev RS, Manor 0, Amir N, Gross-Tsur V. (1993) Acquisition ofarithmetic in normal children: assessment by a cognitive modelof dyscalculia. Dev Med Child Neuro135: 593-601.
ShalevRS, Manor 0, Gross-TsurV. (1997) Neuropsychologicalaspects of developmental dyscalculia. Math Cogn 33: 105-120.
Shalev RS, Manor 0, AuerbachJ, Gross- Tsur V. (1998) Persistence ofdevelopmental dyscalculia: what counts? Results from a threeyear prospective follow-up stUdy.] Pediatr 133: 358-362.
Shalev RS, Manor 0, Kerem B, Ayali M, Badihi N, Friedlander Y,Gross- Tsur V. (2001) Familial-genetic facets of developmentaldyscalculia.] Learn Disabil34: 59-65.
Shalev RS, Gross- Tsur V. (2001) Developmental dyscalculia. PediatrNeuro124: 337-342.
Shaywitz SE. (1998) Dyslexia. N Engl] Med 338: 307-312.Shaywitz SE, Fletcher JM, Holahan)M, Shneider AE, Marchione KE,
StUebing KK, Francis DJ, Pugh KR, Shaywitz BA. (1999)Pt'csisten<:e of rlyslt'xia: tht' Connt'ctirut longitUdinal stUdy atadolescence. Pediatrics 104: 1351-1359.
Spreen 0, Strauss E. (1991) A Compendium of NeuropsychologicalTests. New York: Oxford University Press. p 219-227.
Wechsler D. (1974) Manual for the Wechsler Intelligence Scale forChildren - Revised. New York: Psychological Corporation.
I PediatricNeurologist!I Wilmington,Delaware. I
.Nemours is one of the largest established groups of specialistsin children'shealthcarein the U.S.with locationsin Delaware,Aorida,NewJersey,andPennsylvania.
TheAlfred I.duPont Hospital for Children is a 183-bed,fullservicehospitalequippedto careforchildrenwith awiderangeofconditions.Wearea regionalcenterprovidingtreatmentforadiversityofpediatricmedicalandsurgicaldisordersthat requirecomprehensivecare,includingbonemarrow,kidneyandlivertransplantation.Over40 medical,surgicalanddentalsubspecialtyprogramsareofferedon anoutpatientbasis.TheDepartmentof Pediatricsconsistsof90full andpart-timeclinicalfacultyin 19divisions,whoprovidepediatricspecialtycareandareresponsiblefor pediatriceducationprogramsformedicalstudents,andthePediatricresidency-trainingprogramof theThomasjeffersonUniversitySchoolofMedicine.
Interestedcandidates,sendcurriculumvitaeandcoverletterspecifyingpositionto:jan Roberts-jolly,EmploymentManager,Nemours,e.mail:[email protected].(J02)651'5589(phone),(J02)651-6119(fax).EOE
BeginningJanuary2005, 100% freehealthcoverageforchildrenof ourfull-time employees. "'-
N! Alfred L duPont
emours Hospital for Children- Nemours
; Children's Clinic
www.Nemours.org
Dyscalculia: Six-Year Follow-Up Ruth S Shalev et al. 125