Cvst 2
73
Interesting Case Presented by Hong – Sarawoot May 2010
Transcript of Cvst 2

Interesting Case
Presented by Hong – Sarawoot
May 2010

ผู้��ป่�วยหญิงไทยอาย� 19 ป่� สิทธิ์�การร�กษา 30 บาท รพ.อ��น อาการสิ�าคั�ญิ : ตาเห"นภาพซ้�อน 5
ว�นก%อนมารพ.
History

- 1 สิ�ป่ดาห(ก%อนมารพ. ผู้��ป่�วยม)อาการป่วดศี)รษะท��วๆ ท�.งศี)รษะป่วดต�.อๆ ไม%เคัยเป่/นมาก%อนอาการป่วดศี)รษะอย�%ๆ ก"เป่/นขึ้1.นมาตอนท�างาน อาการเป่/นมากขึ้1.นเร��อยๆ ม)คัลื่��นไสิ�อาเจี)ยนต�.งแต%ว�นแรกท)�ป่วดศี)รษะเป่/นว�นลื่ะ 2-3 คัร�.ง pain score 9-10/10 (อาการเป่/นจีนมากท)�สิ�ดในว�นเด)ยว เร�มจีากpainscore 6-7)
- ขึ้ย�บต�ว ไอจีามแลื่�วป่วดมากขึ้1.น กลื่างคั�นนอนไม%หลื่�บ
History

- อาการเป่/นมากจีนนอนไม%หลื่�บ ไม%ม)ไขึ้� กนยาพาราเซ้ตามอลื่ 2 เม"ดท�ก 8 ชม.อาการไม%ด)ขึ้1.น
- 6 ว�นก%อนไป่ตรวจีท)� clinic ได�ยาฉี)ดแลื่ะยามากนอาการด)ขึ้1.น ไม%ทราบชนดยาอาการป่วดศี)รษะด)ขึ้1.น pain score เหลื่�อ 5 - 6
History

- 5 ว�นก%อนมารพ. เร�มม)ตาเหลื่% ร� �สิ1กเห"นภาพซ้�อนเวลื่ามองไกลื่ๆ ใกลื่�อ%านหน�งสิ�อได�ช�ดด) อาการเห"นไม%ม)ไขึ้� ไม%ม)หน�าเบ).ยว ไม%สิ�าลื่�ก ไม%ชา ไม%อ%อนแรง มองเห"นช�ดเจีนถ้�า ป่9ดตา 1ขึ้�าง ได�ยนป่กต ไม%ได�ยนเสิ)ยงในห� อาการป่วดศี)รษะย�งม)อย�% pain score ใกลื่�ๆเดม = 6-7
- อาการเห"นภาพซ้�อนเป่/นมากขึ้1.นจี1งมารพ.
History

Past History- ป่ฏิเสิธิ์แพ�ยา ม)ใช�ยาคั�มก�าเนดมา 1
ป่�ชนด 21 เม"ด- ม)บ�ตร 1คันแขึ้"งแรงด) ไม%เคัยม)
ป่ระว�ตแท�งบ�ตรมาก%อน- ไม%เคัยผู้%าต�ด- สิ�บบ�หร)�ว�นลื่ะ 1- 10 มวนมา 3 ป่�- ป่ฏิเสิธิ์ผู้��นแพ�แสิง หร�อป่วดขึ้�อ
ป่ฏิเสิธิ์โรคัเลื่�อดในคัรอบคัร�ว

Physical Examination
V/S T 37o C, P 97/min, RR 14/min, BP 136/99 mmHg
GA good consciousness, not pale, no jaundice, no pitting edema, no superficial vein dilatation
HEENT thyroid gland no enlargement
Respiratory system: normal chest movement, normal breath sound, no adventitious sound

CVS: apical impulse at 5 th ICS at Lt.MCL, no apical or parasternal heaving, no murmur
Abdomen soft, not tender, liver and spleen cannot be palpated
Neurological Examination:
Physical Examination

Neurological Examination:
Normal motor tone, motor power grade V all extremities, no sensory deficit,
Esotropia, VA 20/20 both eyes, pupil 3 mmBRTL, normal visual field
EOM 100 100
0 + 100 100 + 100
100 100
Fundoscopic exam: papilledema both disc
Physical Examination

CN V, VI, VII, VIII, XI, X, XI, XII
Stiff neck positive(terminal)
Cerebellar sign normal
Deep tendon reflex all 2+
Babinski ’s absent
Physical Examination

1. Suspected increase intracranial pressure with isolated sixth cranial nerve palsy Rt. for 5 days
Problem List

1. Venous Stroke
2. Brain parenchyma and Meninges: Chronic meningitis, Brain tumor with complication
3. Hydrocephalous(obstructive or any cause)
4. Idiopathic intracranial hypertension
5. Subarachnoid hemorrhage(less likely)
DDx

CN VI: Nerve Lesion vs. Nuclear Lesion Nerve Lesion
OphthalmoplegiaEsotropia
Nuclear LesionOphthalmoplegiaEsotropiaFacial WeaknessAltered LOC
General: diplopia
CN VI : ABDUCEN NERVE

CN VI:
Nerve Lesions:Meningeal tumorsPituitary AdenomaInflammation
- Increase intracranial pressure Nuclear Lesions:
Ischemia (pontine infarction)Central Demyelinating DisordersInflammation
CN VI : ABDUCEN NERVE

CN VI : ABDUCEN NERVE
CLINICAL Pontine lesion : LR palsy + facial palsy : horizontal diplopia
Petrous temporal bone : LR palsy + CN V palsy “ Gardenigo syndrome”
Increase intracranial pressure : false localizing sign

Investigation(16/4/53)
CBC: Hb 14.3 g/dl, Hct 45.1%,WBC 13400/cumm3, N 60.8%, L 27.9%, Plt 279,000, MCV 84 fl
PT 11.3 sec, aPTT 22.3 sec
BUN 17 mg/dl,Cr 0.8 mg/dl, Ba 141 mmo/lL, K 4.1 mmol/L, Cl 106 mmol/L, CO2 26 mmol/L

Investigation
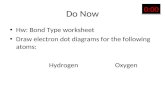
CT Brain with contrast

CT brain with contrast: Empty delta sign

Investigation
Lumbar puncture: OP 50 cmH2O, CP 30 cmH2O
CSF WC 0, RC 0, Glucose 55 mg/dl, Protein 22.5 mg/dl
CSF gram stain not found, AFB not found, no encapsulated yeast, CryptoAg negative, VDRL negative
BS 84 mg/dl
AntiHIV negative

Progress Note
17/4/53 หลื่�งจีาก LP ม)ป่วดศี)รษะเลื่"กน�อย ไม%ม)ไขึ้�
EOM 100 100
0 + 100 100 + 100
100 100

Investigation
ANA speckle 1:160, Peripheral 1:160, Homogenous 1:160
ANA CSF homogenous 1:40 homogenous pattern
AntiHIV negative

Investigation
Lumbar puncture(19/04/53) OP 34, CP 17
CSF RC 25/cumm3, WBC 0, protein 19.6 mg/dl, glucose 51 mg/dl, BS 68 mg/dl

Progress Note
20/4/53 หลื่�งจีาก LP ไม%ม)ป่วดศี)รษะ ไม%ม)ไขึ้�
EOM 100 100
40 + 100 100 + 100
100 100

Progress Note
20/4/53 ไม%ม)ป่วดศี)รษะ ไม%ม)ไขึ้� แขึ้นขึ้าแรงป่กตด)
EOM 100 100
60 + 100 100 + 100
100 100

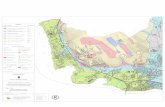
MRI and MRV



MRI and MRV
Diffuse venous sinus and cortical vein thrombosis. Suspected thrombosis in Lt. upper jugular vein is also present
No evidence infarction or hemorrhage

Treatment
Enoxaparin 0.6 cc sc q 12 hr
Challenge warfarin(5)1x1-> warfarin(3)1x1 o hs
D/C

Conclusion
• Continue at least 6 mo Repeat MRV if no evidence thrombosis stop 2 wks for work up hypercoagulable state if hypercoagulable state present -> life long warfarin
• Protein C, Protein S level, antithrombin III level
• Lupus anticoagulant
• Anti beta2 glycoprotein IgG, IgM
• Anticardiolipin IgM, IgG

Warfarin

Warfarin Embryonopathy (ACC/AHA guideline vulvular heart disease 2006)
Incidence 4-10%, lower if dose < 5 mg/day
Midface hypoplasia, stippled chondral calcification, scoliosis, short proximal limbs, and short phalanges
Risk at 6-12 wks of pregnancy
Safe if first 6 wks and 2nd and 3rd trimester

Warfarin (ACC/AHA guideline vulvular heart disease 2006)
During labor and delivery cause bleeding in the fetus and fetal cerebral hemorrhage
Increase incidence of spontaneous abortion, prematurity, stillbirth
Change to heparin several weeks before delivery

During Pregnancy
Change to UFH or LMWH during 6-12 wks
Stop and change to Heparin during 2-3 wks
After 36 wks discuss risk UFH in low risk for fetus but increase risk of infection, osteoporosis, HIT

Cerebral Venous Sinus Thrombosis
n engl j med 352;17 www.nejm.org april 28, 2005


Thrombosis of the Cerebral Veins and Sinuses
Most affect young adult and children, about 75% are women
Incidence 3-4 cases per million, and up to 7 per million in children
>80% of all patients ,good neurologic outcome

Thrombosis of the Cerebral Veins and Sinuses
Pathogenesis venus occlusion -> intracranial hypertension ->
Enlarged, swollen veins, edema, ischemic neuronal damage, and petechial hemorrhages
Impaired absorption of CSF
1/5 of intracranial hypertension “ No Neuro Sign”

Clinical Manifestation
Severe headache gradually over a couple day (may a split second on set)
Rare unilateral hemispheric symptoms: hemiparesis, aphasia
Coma and seizure
Paralysis eye movement




Hereditary Antithrombin deficiency
Protein C deficiency
Protein S deiciency
Factor V Leiden mutation
Prothrombin G20210A polymorphism
Homocysteinemia (rare)
Acquired Antiphospholipid syndrome
(APS)
Disseminated intravascular coagulopathy (DIC), chronic
Heparin induced thrombocytopenia/thrombosis (HIT/T)
Paroxysmal nocturnal hemoglobinuria (PNH)
Thrombophilic diseases

Precipitating
Head injury
Obstetrical delivery ;last trimester, after delivery 12/100,000
Oral contraceptive pills
Infection: Otitis and mastoiditis-> sigmoid and transverse sinuses

HYPERCOAGULABLE STATES
CONGENITAL
Factor V Leiden mutation(APC resistance) 40-60%
Prothrombin Gene Mutatuion 18-20%
Protein C deficiency 5-10%
Protein S deficiency 5-10%
Antithrombin III deficeincy 3%
Dysfibrinogenemia 1%
Hyperhomocystinemia

อุ�บั�ติ�การณ์�ความผิ�ดปกติ�ในผิ��ป�วยที่��ม�หลอุดเล�อุดด�าอุ�ดติ�น
Angchaisuksiri P, et al. Risk factors of venous thromboembolism in Thai patients. Int J Hematol
2007;86:397-402

อุ�บั�ติ�การณ์�ความผิ�ดปกติ�ในผิ��ป�วยที่��ม�หลอุดเล�อุดด�าอุ�ดติ�นTHAI Chinese Caucasia
n
Protein S deficiency 12.3% 8-33% 1-3%
Protein C deficiency 8.9% 4-19% 3-5%
Antithrombin deficiency 4.7% 4% 1%
Factor V Leiden 0% 0% 20%
Prothrombin mutation 0% 0% 6%
Elevated fibrinogen 33.3% - 3%
Elevated factor VIII 30.4% - 25%
Elevated factor XI 26.8% - 19%
Hyperhomocysteinemia 5% - 10-20%
Antiphospholipid antibodies 10% - 10%
Malignancy 19% 16-27% 9-25%


HYPERCOAGULABLE STATES
CONGENITAL
Factor V Leiden
- Hereditary resistance to activated protein C
- Factor V unable to degraded activated protein C
- Treatment : long term anticoagulant

HYPERCOAGULABLE STATES
CONGENITAL
Protein C deficiency
- decreased protein C (activated by thrombin) decreased activated protein C to degrade factor V , VIII.
Protein S deficiency
- co-factor for protein C

HYPERCOAGULABLE STATES
Plasma level (%)
Preterm baby 30
Term baby 50
Adult 60-120
Heterozygosity 40-60
Homozygosity <10
Plasma protein C level

HYPERCOAGULABLE STATES
Clinical manifestation Homozygous (PC or PS < 10%) present in the early year of life neonatal purpura fulminans
Heterozygous (PC or PS 10-60%) thrombosis in teenage usual or unusual site

Neonatal purpura fulminans in a homozygous protein S deficiency patient

HYPERCOAGULABLE STATES
Acquired condition associated with low protein C
Increased utilization DIC Severe pre-eclampsia ARDS Postoperation IgG paraproteinemia
Decreased synthesis Hepatocellular disease Oral anticoagulants Vitamin k deficiency L-asparaginase treatment

HYPERCOAGULABLE STATES
Acquired condition associated with low free protein S
Increased C4BP pregnancy oral pill diabetes milletus inflammation: SLE, nephrosis, AIDS smoker
Decreased synthesis (PS or C4BP) preterm liver diseases vitamin K deficiency, cuamadin treatment

HYPERCOAGULABLE STATES
Prothrombin G20210A polymorphism
In 1996 discover a genetic defect G20210A of prothrombin gene
Elevated plasma prothrombin level
Increased thrombotic risk (2-6 times) due to enhanced thrombin generation

HYPERCOAGULABLE STATES
CONGENITAL
Hyperhomocysteinemia
- autosomal recessive
- endothelial damage leading to increased arteriosclerosis.
- >11 nmol/l increased risk of atherosclerosis
- >18 nmol/l increased risk of venous thrombosis
- both venous & arterial thrombosis
- synergistic risk factor with factor V Leiden
- treatment : vitaminB6 ,12 , folate

HYPERCOAGULABLE STATES
Homocysteinemia In 1969 Kilmer McCully suggested
homocysteinemia might be associated with premature coronary disease or stroke
Homocysteine is injurious to blood vessels Convert endothelium from antithrombotic to
prothromotic phenotype Smooth muscle proliferation
Both arterial and venous occlusion

HYPERCOAGULABLE STATES
ACQUIRED
Oral pills :
- Risk thrombotic stroke 9 times
- Depended on : age>35, duration, high estrogen, smoking ,DM ,HT , DLP,
1st 2 weeks after delivery
- Mechanism - intimal hyperplasia,
- increased blood viscosity
- decreased protein S,AT III,
- enhanced arterial hypertension

HYPERCOAGULABLE STATES
ACQUIRED
Pregnancy
- Decreased protein S,AT III level
- Venous stasis
- Increased factorVII ,VIII,fibrinogen level

HYPERCOAGULABLE STATES
ACQUIRED
Nephrotic syndrome
Related arterial &venous stroke
Mechanism - increased fibrinogen
- thrombocytosis
- enhanced platelet aggregrant
- decreased AT III ,protein S level
- DLP,steroid,diuretic used

Antiphospholipid syndrome:
“Vascular occlusion and antibodies
to anionic phospholipid.”
HYPERCOAGULABLE STATES

ANTIPHOSPHOLIPID SYNDROME
* Recurrent thromboembolism or pregnancy loss with antibodies
(antiphospholipid Ab, LA ,anti-B2 glycoprotein I Ab)
* Increased prevalence associated SLE, type of anticardiolipin Ab
In a series 1000 pateints the prevalence of feature of APS were :
- DVT 32%
- Thrombocytopenia 22%
- Livedo reticularis 20%
- Sroke 13%
- Superficial thrombophlebitis 9%
- Pulmonary embolism 9%
- Fetal loss 8%
- TIA 7%

Sixth CN palsy with other signs

Syndrome
Raymond’s syndrome: ipsilateral CN VI and contralateral paresis of the extremities
Millard-Gubler syndrome ipsilateral 6th and 7th CN palsy with contralateral hemiplegia
Foville’s syndrome: Millard-Gubler syndrome + lateral conjugate gaze palsy


Syndrome
Gradenigo’s syndrome: inflammation of tip of the temporal bone : CN V, VI, greater petrosal nerve -> unilateral paralysis of lateral rectus, pain (CN V), excessive lacrimation


Syndrome
Duane’s syndrome: widening of the palpebral fissure on abduction and narrowing on adduction
Gerhardt’s syndrome: bilateral abducens palsy
Möbius syndrome: paralysis of extraocular muscles, especially abducens, with paresis of facial muscle
Tolosa-Hunt syndrome: recurrent unilateral pain in retro-orbital region with palsy of the extraocular muscles (3rd, 4th, 6th , V1, V2 )



CN VI : ABDUCEN NERVE
Lying on petrous part of temporal bone with CN VOut of skull by carvernous sinus

Thank you for attention





![[XLS] · Web view3 3 3 3 3 3 3 3 3 3 2 4 4 4 4 4 2 2 2 3 3 3 3 3 3 3 3 3 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 3 3 3 3 3 3 3 3 3 3 3 2 2 2 2 4 4 4 4 4 4 4 4 4 4 2 2 2 2 2 2 2 2](https://static.fdocument.pub/doc/165x107/5b1aa0e07f8b9a3c258de1b1/xls-web-view3-3-3-3-3-3-3-3-3-3-2-4-4-4-4-4-2-2-2-3-3-3-3-3-3-3-3-3-2-2-2.jpg)