Capstone Project..YF .8.17.2014 (1)
25
MPH and MD/MPH Degree Program 1 Yendi Fontenard THE HEMOPHILIA TRIUMPH THE SOLUTION TO SICKLE CELL DISEASE CHAGRIN Foundation for Sickle Cell Disease Research August 2014
-
Upload
yendi-fontenard -
Category
Documents
-
view
63 -
download
11
Transcript of Capstone Project..YF .8.17.2014 (1)

MPH and MD/MPH Degree Program
1
Yendi Fontenard
THE HEMOPHILIA TRIUMPH -‐ THE SOLUTION TO SICKLE CELL DISEASE CHAGRIN
Foundation for Sickle Cell Disease Research
August 2014

MPH and MD/MPH Degree Program
2
ABSTRACT
Hemophilia and Sickle Cell Disease (SCD), both inherited blood disorders meet the criteria for
rare diseases in the United States with respective prevalence of approximately 20,000 and
100,000. An examination of the infrastructure as well as intangible resources facilitating care
coordination and standardization of care of both diseases shows a skewed reality, in favor of
Hemophilia. For both diseases, care coordination is paramount to ensuring quality of life; yet to
date, this has only come to fruition for Hemophilia through a federally funded nationwide
network of established comprehensive treatment centers. The disconnect among stakeholders
in the SCD community has repeatedly been highlighted as a contributing factor. As a result, the
Foundation for Sickle Cell Disease Research (FSCDR) is striving to address the ineptitude of the
existing SCD climate through their grant proposal to United Health Foundation for support for a
Sickle Cell Care Network (SCCN) -‐ Certification Makes a Difference Program. The goal of this
paper is to make an argument in support of this program by highlighting the unmet needs of
the SCD population as well as the success of Hemophilia Treatment Centers.

MPH and MD/MPH Degree Program
3
Table of Contents
Summary Statement ..................................................................................................................... 4
Capstone Project Objectives ......................................................................................................... 5
Sickle Cell Disease .......................................................................................................................... 6
Hemophilia .................................................................................................................................. 13
FSCDR’s proposed program ......................................................................................................... 16
Conclusion ................................................................................................................................... 21
Reference List .............................................................................................................................. 22

MPH and MD/MPH Degree Program
4
SUMMARY STATEMENT
The Foundation for Sickle Cell Disease research (FSCDR) is a non-‐profit organization located in
Florida, committed to sickle cell disease research to confer the highest quality of life possible to
these patients. Their hope is to establish a robust research and funding portfolio for sickle cell
disease but their efforts transcend a typical research organization as their mission also supports
non-‐clinical sickle cell work. Of note, FSCDR serves physicians, allied health professionals,
pharmaceutical companies, biotechnology companies as well as patients. Their work has
inspired me to support one of their recent proposals, a Sickle Cell Care Network (SCCN) -‐
Certification Makes a Difference Program. This paper will add to the body of literature
highlighting the dearth of resources hampering improvements in the quality of life of SCD
patients and will hopefully facilitate a break in the cycle of mediocrity that continues to plague
this population.

MPH and MD/MPH Degree Program
5
OBJECTIVES
This project will address the following:
1. Highlight the current deficits in care provided to sickle cell patients
2. Compare and contrast the current Sickle Cell Disease climate with that of Hemophilia
3. Examine FSCDR’s proposed solution: “Sickle Cell Advisory Council, the Sickle Cell Care
Network™ (SCCN) – Certification Makes a Difference program”

MPH and MD/MPH Degree Program
6
SICKLE CELL DISEASE
Sickle Cell Disease (SCD), deemed the most common inherited blood disorder in the
United States (US), is the umbrella term for a group of inherited red blood cell disorders.
Although the exact prevalence in the US is unknown, it affects approximately 90,000-‐100,000
with a predilection for Blacks (Centers for Disease Control and Prevention, CDC 2014). The
incidence of the disease is 1 in every 500 and 1 in 36,000 Black Americans and Hispanic
Americans respectively, with the Sickle Cell Trait occurring 1 in 12 Blacks (CDC, 2014).
Although type and severity of presentation is diverse, SCD is the result of inheritance of
Sickle (S) Hemoglobin (Laurence, George, and Woods, 2006) through a single point mutation in
the sixth position of the Beta Hemoglobin chain (Carroll, Haywood, Hoot, and Lanzkron, 2013).
Sickle Cell Anemia, the most common form of the disease, and more scientifically, SS genotype,
is the result of the inheritance of two abnormal hemoglobin alleles. This lends itself to
significant polymerization of hemoglobin and distortion of red blood cells into sickle-‐shaped
cells under certain conditions. A cascade of events and interactions, including hemolysis, hyper-‐
viscosity and hypo-‐perfusion has the potential to impede the function of every major organ
system (Carroll et al., 2013). Notably, the phenotypic variability of the disease is significant
ranging from relatively mild and asymptomatic to clinically severe with multi-‐organ failure
including; strokes, limb ulcers, acute chest syndrome, infections, avascular necrosis,
retinopathy, priapism, pulmonary embolism renal failure, and untimely death (CDC, 2014;
Sheth, Licursi, & Bhatia, 2013).

MPH and MD/MPH Degree Program
7
Regardless of phenotypic expression, SCD is typically progressive with irreversible organ
damage (Sheth et al., 2013). Often, chronic anemia, impaired growth, episodic pain crises, renal
dysfunction, neuro-‐psychiatric abnormalities and life threatening complications (acute chest
syndrome, splenic sequestration, infarctive strokes) present themselves in infancy and
childhood. Thereafter, adolescence and adulthood are plagued with a myriad of complications
including chronic pain, leg ulcers, pulmonary embolism, hemorrhagic strokes and organ failure
(Sheth et al., 2013). Figure (1) below, puts the scope of clinical manifestations from childhood
through adulthood into further perspective.
Figure 1. Complications of SCD: childhood and adulthood. Reprinted from “Management of sickle cell disease
from childhood through adulthood by J. Kanter & R. Kruse-‐Jarres 2013, Blood Reviews, 27(2013) 279-‐287:
Copyright (2013) by Elsevier. Reprinted with permission.

MPH and MD/MPH Degree Program
8
A hallmark of SCD is pain (Kanter & Kruse-‐Jarres 2013); medically described as vaso-‐
occlusive crises (VOCs), its unpredictability and potentially crippling nature has made it the best
described phenomenon associated with the disease (Carroll et al.,2013). Further, it is
undisputed that high utilization of emergency rooms and significant morbidity are attributed to
these painful phenomena (Okam, Shaykevich, Ebert, Zaslavsky, and Ayanian, 2014). Some
patients have expressed these crises as a daily battle; one that many have difficulty
comprehending which leads to them being branded as fabulists and drug-‐addicts (Weisberg,
Balf-‐Soran, Becker, Brown, and Sledge, 2013). Needless to say, patients and providers have an
onerous task managing this disease. The clinical course notably diverse, calls for comprehensive
care that is ongoing, patient-‐centered and delivered by a multidisciplinary team (Raphael &
Oyeku 2013).
Improvement in Life expectancy is a matter of utmost concern for any chronic disease,
SCD being no exception. Hassell (2010) demonstrated in Figure (2) below, that due to progress
made in treatment of the disease, a comparison of mortality rates in individuals with SCD
between 1979 vs. 2006 shows: 1) a shift in the mortality curve to the right and 2) that the shape
of the curve has remained the same.

MPH and MD/MPH Degree Program
9
Figure 2. Age at death for individuals with SCD in 1979 and 2006. Reprinted from “Population estimates of sickle
cell disease in the U.S. by K.L.Hassell,2010, American Journal of Preventive Medicine, 38(4 Suppl):S512-‐21.
Copyright (2010) by Elsevier. Reprinted with permission.
Due to increased infection prophylaxis (penicillin antibiotics) against opportunistic infections
(e.g. streptococcus pneumonia) in childhood, mortality rates in early childhood have improved.
Of note, the dramatic rise in mortality rates previously occurring in infancy and the second
decade of life has merely shifted to the third decade. While over 90% of children are
progressing to adulthood, this elucidates health care providers’ incompetence and or neglect in
ensuring seamless pediatric to adulthood transition and care (Sheth et al., 2013). Does rarity of
the disease have anything to do with it or has ignorance allowed an exploitation of a subset of
our population?

MPH and MD/MPH Degree Program
10
Aside from ensuring longevity, ensuring a high quality of life is imperative. A review of
this metric utilizing 39 studies was quite alarming, concluding that “adults and children with
sickle cell disease have significantly impaired health-‐related quality of life that is comparable to
or worse than other chronic diseases…even in their baseline state of health (Panepinto &
Bonner, 2012).” Many echo that compared to their unaffected peers, their physical, social and
school functioning is significantly lower; one study stating that functionality is lower by 58%,
70% and 48% respectively (Roth, Krystal, Manwani , Driscoll, and Ricafort 2012).
Additionally, to date, there is one curative therapy, namely Hematopoietic Stem Cell
Transplantation (HSCT) (Kanter & Kruse-‐Jarres 2013). Why then is there not 100% cure rate?
HSCT, requires transplantation of bone marrow of a patient with SCD with healthy bone
marrow from a donor, largely limited to individuals with a matched sibling donor (MSD)
(Shenoy, 2011), with only 14-‐20% of individuals with SCD have a matched sibling donor. First
performed in a patient with both SCD and leukaemia, its widespread use has been hindered
understandably so by the lack of a suitable donor and the risk of transplant associated
morbidity and mortality (Sheth et al., 2013). While there is no unanimity regarding indications
for HCST, it has historically been administered to patients with debilitating symptomology with
children being favored. The rationale is that they have less end-‐stage organ damage and lower
risk for transplant-‐related morbidity (Sheth et al., 2013). As a result, a mere 600 individuals
have undergone HSCT despite a marked reduction in transplant related infections, graft failure,
graft-‐versus host disease, long-‐term organ toxicity and death (Sheth et al., 2013).

MPH and MD/MPH Degree Program
11
With the possibility of a cure improbable for the majority, the approach to SCD patients
involves precautionary, supportive and reactionary management (Sheth et al, 2013). The
mainstay of treatment involves relief of pain, prevention of likely infections, organ damage,
strokes and the control of any complications (Kanter & Kruse-‐Jarres 2013). Complicating
management further is the fact that there is no conclusive way to predict the clinical trajectory
in any one patient (Sheth et al., 2013).From infancy and childhood, prophylaxis generally
involves routine vaccinations, antibiotics, monitoring of growth and their academic
achievement (Kanter & Kruse-‐Jarres 2013).
Pain, an often recurring event as highlighted earlier, may require care in an urgent care
setting, as an in-‐patient, or if mild enough, at-‐home or as an outpatient. Pharmacological and
non-‐pharmacological modalities of treatment are often utilized; Severe pain requires parenteral
infusions of opioid analgesics (morphine) in tandem with non-‐opioids such as non-‐steroidal
anti-‐inflammatory drugs (NSAIDS), acetaminophen and psychotropic drugs (tranquilizers,
stimulants) (Raphael & Oyeku 2013). Warm compresses and relaxation techniques may also be
used (Kanter & Kruse-‐Jarres 2013).
If the complexity of the disease was not realized prior to reading this brief, there is no
question that by now it is. What then is the status quo of provision of care and utilization of
care in the United States? Available data suggests that SCD-‐related complaints account for
approximately 113,000 admissions per year with an estimated cost of approximately 488
million in-‐patient costs alone, in the United States (Steiner & Miller, 2006). Further, the disease
has resulted in 30% of individuals on disability and a startling 50% unemployment rate

MPH and MD/MPH Degree Program
12
(Ballas, Bauserman, McCarthy, Waclawiw; Multicenter Study of Hydroxyurea in Sickle Cell
Anemia, 2010). If an accurate numerical value could be given for loss of productivity secondary
to hospitalizations and morbidity, it would surely surpass the aforementioned millions (Sheth et
al., 2013). Additionally, analysis of data from the National Hospital Ambulatory Medical Care
Survey (NHAMCS) from 1999-‐2007 stated approximately 197,333 emergency room (ER) visits
with SCD listed as a diagnosis occurred each year. This pales in comparison to the total number
of ER visits per year but yet still, Lanzkron, Carroll, and Haywood (2010) demonstrated that
“charges for hospital admissions from emergency departments for SCD are on a similar order of
magnitude to conditions over 100 times more common.” This is a significant contribution for a
“rare disease” and makes this a matter of utmost public health concern.
To avert these high hospitalization patterns for SCD and many other chronic illness, a
push for patient-‐centered medical homes (PCMH) are at the forefront of health care reform
(Raphael & Oyeku 2013). As described by Raphael & Oyeku (2013), “the PCMH can be
envisioned as a multidisciplinary team of providers focused on the patient’s needs, with care
functions and team processes coordinated through integrated health information technology.”
While this may not be a panacea for decreasing the burden SCD has on the health care system,
its adoption and implementation nationwide are sin qua non. If the cited facts throughout this
paper aren’t cause for heightened efforts to improve the status of SCD nationwide, a glimpse
into the success of hemophilia will surely do so.

MPH and MD/MPH Degree Program
13
HEMOPHILIA
Hemophilia is the umbrella term for a group of rare inherited bleeding disorders due to
a mutation in the genes responsible for the production of blood clotting factor proteins
(Franchini and Mannucci, 2012). Hemophiliacs have lower than normal levels of either Factor
VIII (Hemophilia A) or Factor IX (Hemophilia B), both integral for blood clotting. Like SCD, the
clinical manifestations of Hemophilia are varied, and more specifically classified as mild,
moderate and severe. (Franchini and Mannucci 2012). The inheritance mechanisms, causes the
disease to have a predilection for males with the prevalence in females much lower (CDC,
2013). In the United States, the disease prevalence is estimated at 20,000 (significantly lower
than SCD) with an incidence of 1 in 5,000 male births and approximately 400 afflicted births per
year (CDC, 2013).
Hemophiliacs are at risk for spontaneous bleeding or bleeding at a site of injury with the
potential for marked disability and mortality if left unchecked (Soucie, Nuss, Evatt, Abdelhak,
Cowan, Hill, Kolakoski, and Wilber, 2000). Similar to SCD is the potential for multi-‐organ
involvement with bleeding sites including the nose, the skin, the mouth, joints and internal
organs (CDC, 2013). Ironically, complications may arise from the disease itself as well as its
treatment (infusions of replacement factor concentrates and other clotting agents) (Soucie et
al., 2000). Advancements in care over the years have led to increased longevity but with
concomitant complications including: joint damage from recurrent hemarthroses, transfusion-‐
transmitted infections, increased risk of development of inhibitors secondary to transfusions,

MPH and MD/MPH Degree Program
14
adverse reactions from clotting factor treatments, and brain damage secondary to intracranial
bleeding (Philipp, 2010).
The complexity and chronicity of the disease requires comprehensive treatment with a
multidisciplinary approach (CDC, 2013). Advocacy for this disease resulted in the initiation of
the national Hemophilia Treatment Center (HTC) program in 1975. And today, there is a
network of over 100 HTCs throughout the United States and its territories, providing a host of
services including: diagnosis, clinical management, individual treatment plans, orthopedic care,
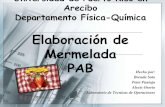
dental care, patient education and counseling (Soucie et al., 2000). Figure (3) below shows the
distribution of these centers.
Figure 3.Distribution of Hemophilia Treatment Centers. Reprinted from Hemophilia Management: Collaborating
in a new era to optimize by the National Hemophilia Foundation,2006. Retrieved from
http://www.managedcarehemo.com/resources.html#2. Reprinted with permission.

MPH and MD/MPH Degree Program
15
Figure (3) reminds us that rarity of a disease is not synonymous with lack of awareness
and lack of advancement. The success of these programs is laudable as the socioeconomic
benefits to hemophiliacs utilizing their services are substantive (Smith and Levine, 1984; Soucie
et al., 2000). Longevity has been afforded to many through improvements in care as evident by
the proportion of hemophilia A and B patients recently surveyed at HTCs that are 65 years and
older (2%) and 45 years and older (15%) (Philipp, 2010). Further, hemophiliacs who utilize an
HTC have a 40% reduction in risk of death compared to those who do not, which is “even more
remarkable because HTCs provide health care services to a higher proportion of severely
affected patients as well as to a disproportionate share of patients with severe liver disease,
HIV infection, and AIDS-‐the primary risk factors for mortality in this population (Soucie et al.,
2000).”
Healthcare is very costly for any Hemophiliac and even further for those with certain
nuances to the typical disease manifestation. In 2008, mean health care expenditures for all
males averaged US $155,136 and costs for individuals with Hemophilia A with an inhibitor (to
the blood clotting factor) were 4.8 times higher than that for non-‐inhibitor patients ($696,279
versus $144,306) (Guh, Grosse, McAlister, Kessler, and Soucie, 2012). In light of this, HTCs
individualize treatment plans for their patients and place a premium on preventive medicine
service (Soucie et al., 2000). Improvement in mortality has also been attributed more
specifically to HTCs’ emphasis on prevention, through their promotion and facilitation of “home
factor-‐infusion” as prophylaxis and early treatment of bleeding episodes. Home factor-‐infusions

MPH and MD/MPH Degree Program
16
have also been recognized for their role in reducing hemophilia-‐related musculoskeletal
damage, pain, school absenteeism and under-‐treatment associated with hospital care. This
practice is pervasive among patients who receive care at HTCs (61%) compared to those who do
not (25%) (Soucie et al., 2000).
Additionally, it is well documented that insurance is a predictor of health outcomes for
individuals with special healthcare needs. Of note, higher levels of insurance coverage have
been documented among Hemophilia patients seen at HTCs (Baker, Riske, Voutsis, Cutter,
and Presley, 2011). And the provision of social services as part of HTCs’ multidisciplinary team
surely plays an integral role here.
FSCDR’s PROPOSED PROGRAM
HTCs have undoubtedly been crucial in the progress made with Hemophilia and FSCDR
recognizes the potential to achieve similar successes with SCD through a similar concept. The
foundation is seeking funding for the development of a Sickle Cell Advisory Council, Sickle Cell
Care Network™ (SCCN) – Certification Makes a Difference Program. The foundation’s rationale
is that presently there is no single organization with regulatory power in the United States
overseeing the many private and hospital affiliated treatment centers in individual states.
Comprehensive care is a model of health care facilitating the coordinated interaction of medical
and non-‐medical services with patients. FSCDR believes that an agency providing oversight is
indispensable for any comprehensive program especially one involving geographically dispersed
centers. The goal of this project, if funded, is to improve the current delivery of care for
patients, and address the disadvantages accompanying “a rare disease” namely: 1) lack of

MPH and MD/MPH Degree Program
17
standardized care, 2) national data rigged with inconsistencies that lack external validity and 3)
funding shortage.
The goal of Sickle Cell Care Network™ (SCCN) – Certification Makes a Difference
Program is to create a national sickle cell disease comprehensive care network of certified
programs for the entire East coast of the US including 3 Florida centers, as this coast accounts
for the majority of the SCD population. Figure (4) below illustrates the estimated distribution of
SCD in the United States with clear indication of its heightened prevalence along the East Coast.
Figure 4. Estimated number of individuals with SCD, based on state-‐specific African-‐American and Hispanic birth-‐
cohort disease prevalence and 2008 U.S. Census population, corrected for early mortality. Reprinted from
“Population Estimates of Sickle Cell Disease in the U.S.,” by K.L. Hassell, 2010, American Journal of Preventive
Medicine, 38(4), S512–S521. Copyright 2010 by Elsevier Inc. Reprinted with permission.

MPH and MD/MPH Degree Program
18
The outcomes that this program hopes to fulfill are a reflection of the current SCD climate in
the United States, one in which patients are disadvantaged by a highly fragmented system and
include: 1) evaluation, improvement and standardization of sickle cell treatment facilities, 2)
establishment of a Sickle Cell Disease Registry, 3) development of a relevant education program
for patients, health care professionals and the public to create informed participation and
support treatment centers and, 4) establishment of a healthcare expected value analysis model
to follow Sickle Cell Disease throughout the lifespan.
A decision is as good as the information that informs it, and without a national registry
in particular, progress with sickle cell disease will remain stagnant. How do we truly make
strides with prevention and control of the disease, if nationally we lack accurate health
statistics (disease prevalence, morbidity, mortality)? Recognized nationally as an issue
perpetuating health disparities among individuals with Sickle Cell Disease the US Department of
Health and Human Services, outlined a number of objectives in “Healthy People 2020” related
to this. The result was a collaborative effort among the CDC, NIH and 7 states (California,
Florida, Georgia, North Carolina, New York, Michigan and Pennsylvania) called “Registry and
Surveillance System for Hemoglobinopathies (RuSH)” project launched in 2010 (CDC, 2014).
RuSH was designed to collect prevalence, morbidity and mortality data for SCD and
Thalassemia. (CDC, 2014). FSCDR was the designated Florida organization so continuing this
effort beyond RuSH seems logical.

MPH and MD/MPH Degree Program
19
FSCDR hopes that the registry will capture additional information including; patient
distribution, social assimilation of patients, availability of treatment and other patient services,
qualification and availability of appropriate human resources and payment mechanisms. The
data collected will allow the foundation to serve as an advisory council to establish protocol for
standardization of sickle cell centers. This protocol will include metrics such as: 1) numbers of
patients to be served, 2) types of treatments available, 3) professional staff required 4)
reciprocal relationships with multiple disciplines-‐ hospitals, social services, employment, and
insurers.
This may seem insurmountable, but the foundation has all intent on seeking external
expertise. For instance, one consulting institution would be the Florida Institute for Health
Innovation’s (FIHI) Center for Collective Impact. They will provide FSCDR with the planning,
implementation strategy, facilitation and technical assistance for the different states. FSCDR’s
call for action has been endorsed by a number of stakeholders and Table (1) below gives insight
into the location and target population of potential participants of the proposed program.

MPH and MD/MPH Degree Program
20
Table 1. Sickle Cell Programs to participate in FSCDR’s
INSTITUTION SCD POPULATION
Georgia Regents University (Georgia) 650 children
adolescents-‐adults
St. Jude Children’s Research Hospital (Tennessee) 900 children
University of Alabama Division of Pediatric Hematology and
Oncology (Alabama)
>1300 patients
University of Miami Miller School of Medicine Sickle Cell Center
(Miami, Florida)
500 children
400 adults
Jawan Ayer-‐Cole Private Practice (Tampa, Florida) Not indicated
Diggs Kraus Sickle Cell Center (Tennessee) 650 patients
Bronx-‐Lebanon Hospital Center (New York) primarily pediatric, small
adult component
University of Louisville Division of Hematology/Oncology and
Sickle Cell Transplantation (Kentucky)
250 children
Carolinas Healthcare System (North Carolina) not indicated
Medical University of South Carolina (MUSC)
(South Carolina)
children
Children’s Healthcare of Mississippi (Mississippi) 1000 children, 600 adults

MPH and MD/MPH Degree Program
21
Support of Sickle Cell Care Network™ (SCCN) – Certification Makes a Difference
Program needs to go beyond the aforementioned institutions and be nationwide. The
cooperation of stakeholders as well as sustainable funding is necessary to catapult progress
with the management of SCD. We cannot attribute the dearth of successes to rarity of the
disease, as success with Hemophilia dispels this. Let us not allow this disease to be another
prime example of health disparities experienced by U.S census defined racial minority groups. It
is irrefutable that social constructs (race, socio-‐economic status) form part of the web of
causation of health disparities, but this FSCDR endorsed program gives an opportunity to
dampen its influence.
CONCLUSION
Improved well-‐being of SCD patients on the population level will ultimately be a
reflection of successful implementation of Sickle Cell Care Network™ (SCCN) – Certification
Makes a Difference Program. Previously unmeasurable and/or inaccurate, the program
components will allow measurement of this indicator. As I see it, support for this program
would be mutually beneficial. My advice to anyone who frowns upon this proposal is to first
have a conversation with those individuals who inadvertently inherit the disease and those
passionate about its eradication. The public health costs of the disease outlined are nothing
short of alarming and refusal to support this proposed program will allow crippling of
potentially able-‐bodied individuals in our society.

MPH and MD/MPH Degree Program
22
REFERENCE LIST
References
Baker, J. R., Riske, B., Voutsis, M., Cutter, S., & Presley, R. (2011). Insurance, home therapy, and
prophylaxis in U.S. youth with severe hemophilia. American Journal of Preventive Medicine,
41(6 Suppl 4), S338-‐45. doi:10.1016/j.amepre.2011.09.002.
Ballas, S. K., Bauserman, R. L., McCarthy, W. F., Waclawiw, M. A., & Multicenter Study of
Hydroxyurea in Sickle Cell Anemia. (2010). The impact of hydroxyurea on career and
employment of patients with sickle cell anemia. Journal of the National Medical
Association, 102(11), 993-‐999.
Carroll, P. C., Haywood, C. J., Hoot, M. R., & Lanzkron, S. (2013). A preliminary study of
psychiatric, familial, and medical characteristics of high-‐utilizing sickle cell disease
patients. The Clinical Journal of Pain, 29(4),317-‐23. doi:10.1097/AJP.0b013e3182579b87.
Centers for Disease Control Prevention. (2011). Sickle cell disease: Data & statistics. Retrieved,
2014, Retrieved from http://www.cdc.gov/ncbddd/sicklecell/data.html
Centers for Disease Control Prevention. (2013). Hemophilia: Data & statistics. Retrieved, 2014,
Retrieved from http://www.cdc.gov/ncbddd/hemophilia/data.html
Centers for Disease Control Prevention. (2014). Hemophilia treatment centers. Retrieved, 2014,
Retrieved from http://www.cdc.gov/ncbddd/hemophilia/HTC.html
Centers for Disease Control Prevention. (2014). Registry and surveillance system for
hemoglobinopathies (RuSH). Retrieved, 2014, Retrieved from
http://www.cdc.gov/ncbddd/hemoglobinopathies/rush.html

MPH and MD/MPH Degree Program
23
Franchini, M., & Mannucci, P. M. (2012). Past, present and future of hemophilia: A narrative
review. Orphanet Journal of Rare Diseases, 7, 24-‐1172-‐7-‐24. doi:10.1186/1750-‐1172-‐7-‐24.
Franchini, M., & Mannucci, P. M. (2014). The history of hemophilia. Seminars in Thrombosis and
Hemostasis, 40(5), 571-‐576. doi:10.1055/s-‐0034-‐1381232.
Guh, S., Grosse, S. D., McAlister, S., Kessler, C. M., & Soucie, J. M. (2012). Healthcare
expenditures for males with haemophilia and employer-‐sponsored insurance in the united
states, 2008. Haemophilia : The Official Journal of the World Federation of Hemophilia,
18(2), 268-‐275. doi:10.1111/j.1365-‐2516.2011.02692.x.
Hassell, K. L. (2010). Population estimates of sickle cell disease in the U.S. American Journal of
Preventive Medicine, 38(4 Suppl), S512-‐21. doi:10.1016/j.amepre.2009.12.022.
Kanter, J., & Kruse-‐Jarres, R. (2013). Management of sickle cell disease from childhood through
adulthood. Blood Reviews, 27(6), 279-‐287. doi:10.1016/j.blre.2013.09.001.
Lanzkron, S., Carroll, C. P., & Haywood, C.,Jr. (2010). The burden of emergency department use
for sickle-‐cell disease: An analysis of the national emergency department sample database.
American Journal of Hematology, 85(10), 797-‐799. doi:10.1002/ajh.21807.
Laurence, B., George, D., & Woods, D. (2006). Association between elevated depressive
symptoms and clinical disease severity in african-‐american adults with sickle cell
disease. Journal of National Medical Association, 98(3), 365-‐9. PMID: 16573300.
Okam, M. M., Shaykevich, S., Ebert, B. L., Zaslavsky, A. M., & Ayanian, J. Z. (2014). National
trends in hospitalizations for sickle cell disease in the united states following the FDA

MPH and MD/MPH Degree Program
24
approval of hydroxyurea, 1998-‐2008. Medical Care, 52(7), 612-‐618.
doi:10.1097/MLR.0000000000000143.
Panepinto, J. A., & Bonner, M. (2012). Health-‐related quality of life in sickle cell disease: Past,
present, and future. Pediatric Blood & Cancer, 59(2), 377-‐385. doi:10.1002/pbc.24176 [doi]
Philipp, C. (2010). The aging patient with hemophilia: Complications, comorbidities, and
management issues. Hematology / the Education Program of the American Society of
Hematology.American Society of Hematology.Education Program, 2010, 191-‐196.
doi:10.1182/asheducation-‐2010.1.191.
Raphael, J. L., & Oyeku, S. O. (2013). Sickle cell disease pain management and the medical
home. Hematology / the Education Program of the American Society of
Hematology.American Society of Hematology.Education Program, 2013, 433-‐438.
doi:10.1182/asheducation-‐2013.1.433.
Roth, M., Krystal, J., Manwani, D., Driscoll, C., & Ricafort, R. (2012). Stem cell transplant for
children with sickle cell anemia: Parent and patient interest. Biology of Blood and Marrow
Transplantation : Journal of the American Society for Blood and Marrow Transplantation,
18(11), 1709-‐1715. doi:10.1016/j.bbmt.2012.05.013.
Shenoy, S. (2011). Hematopoietic stem cell transplantation for sickle cell disease: Current
practice and emerging trends. Hematology / the Education Program of the American
Society of Hematology.American Society of Hematology.Education Program, 2011, 273-‐
279. doi:10.1182/asheducation-‐2011.1.273.

MPH and MD/MPH Degree Program
25
Sheth, S., Licursi, M., & Bhatia, M. (2013). Sickle cell disease: Time for a closer look at treatment
options? British Journal of Haematology, 162(4), 455-‐464. doi:10.1111/bjh.12413 [doi]
Smith, P. S., & Levine, P. H. (1984). The benefits of comprehensive care of hemophilia: A five-‐
year study of outcomes. American Journal of Public Health, 74(6), 616-‐617.
Soucie, J. M., Nuss, R., Evatt, B., Abdelhak, A., Cowan, L., Hill, H.… Wilber, N. (2000). Mortality
among males with hemophilia: Relations with source of medical care. the hemophilia
surveillance system project investigators. Blood, 96(2), 437-‐442.
Steiner, C. A., & Miller, J. L. (2006). Sickle cell disease patients in U.S. hospitals, 2004: Statistical
brief #21. Healthcare cost and utilization project (HCUP) statistical briefs (). Rockville (MD):
doi:NBK63489 [bookaccession] .
Weisberg, D., Balf-‐Soran, G., Becker, W., Brown, S. E., & Sledge, W. (2013). "I'm talking about
pain": Sickle cell disease patients with extremely high hospital use. Journal of Hospital
Medicine : An Official Publication of the Society of Hospital Medicine, 8(1), 42-‐46.
doi:10.1002/jhm.1987.