Book reading 報告日期 :2012-02-23 指導醫師 : 藺瑞安 醫師 指導老師 : 戴溫然...
32
Book reading Book reading 報報報報 :2012-02-23 報報報報 : 報報報 報報 報報報報 : 報報報 報報 報報報 : 報報報 報報報 、 Chapter 30 CENTRAL NERVOUS SYSTEM DISEASE
-
Upload
richard-harmon -
Category
Documents
-
view
272 -
download
0
Transcript of Book reading 報告日期 :2012-02-23 指導醫師 : 藺瑞安 醫師 指導老師 : 戴溫然...
Book readingBook reading
報告日期 :2012-02-23 指導醫師 : 藺瑞安 醫師指導老師 : 戴溫然 老師報告者 : 黃淑宜、李如萍
Chapter 30 CENTRAL NERVOUS SYSTEM DISEASE
Table of contents
Neuroanatomy NeurophysiologyIntracranial pressureIntracranial pressure-volume relationshipCerebral protection Preoperative assessmentAnesthesia for neurosurgeryClinical cases
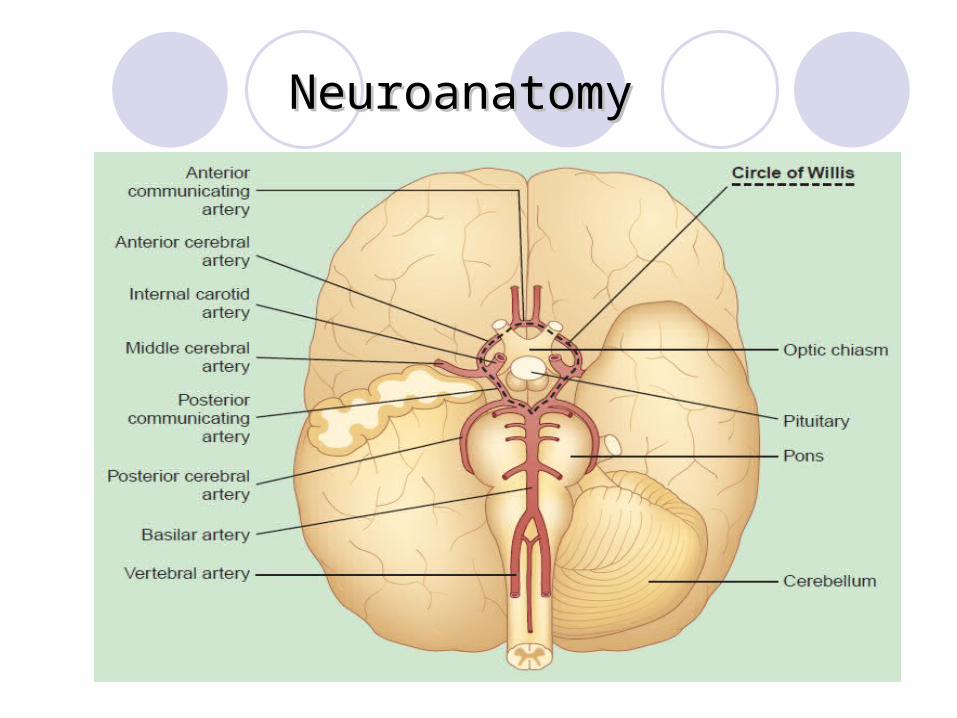
NeuroanatomyNeuroanatomy
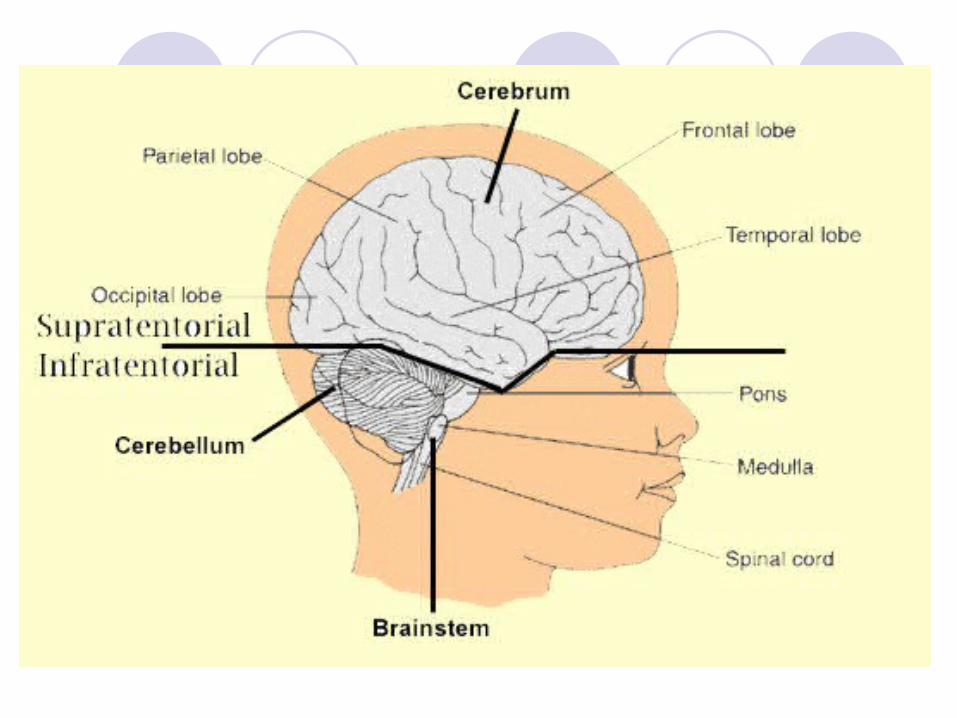
Neuroanatomy
Blood brain barrier disruption Hypertension Trauma Infection Hypoxemia Sever hypercapnia Tumors Seizure
Neurophysiology
Cerebral Blood Flow Effects of CBF Cerebral Metabolic Rate Cerebral Perfusion Pressure
and Autoregulation. Effects of PaCO2 and PaO2 on CBF Effects of anesthetics
Cerebral Blood Flow
Cerebral Blood Flow= 15% Cardiac outputCBF: 50 ml/100g/minCPP =MAP-ICP (or CVP)
Cerebral Metabolic Rate
Body Temperature 37℃
↓ 1 → CMRO℃ 2↓7 %
Cerebral perfusion and Autoregulation
Autoregulation OK CPP: 50~150mmHg
Autoregulation(-) Trauma ; neurosurgery
Hypertension shifts the auto regulatory curve
Right
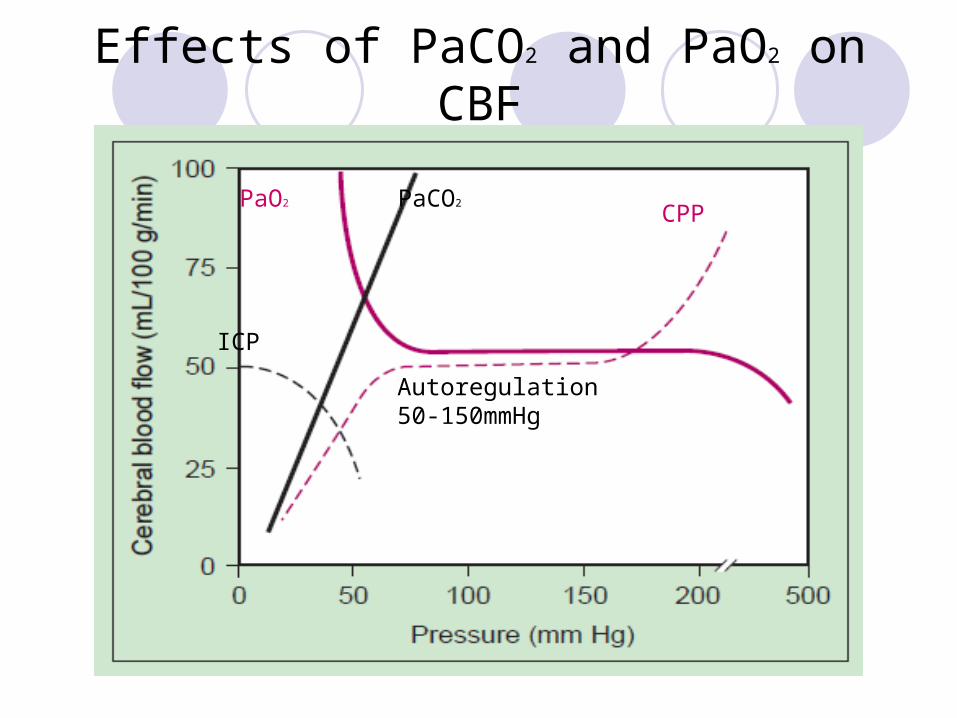
Effects of PaCO2 and PaO2 on CBF
PaCO2PaO2
CPP
ICP
Autoregulation50-150mmHg
Effects of CBF
CMRO2
CPP=MAP-ICP (or CVP)PaCO2: 於 PaCO2 :20~80mmHg 範圍內 , ↑ 1mmHg, CBF ↑ 1-2 ml/100g/minPaO2
Effects of anesthetics
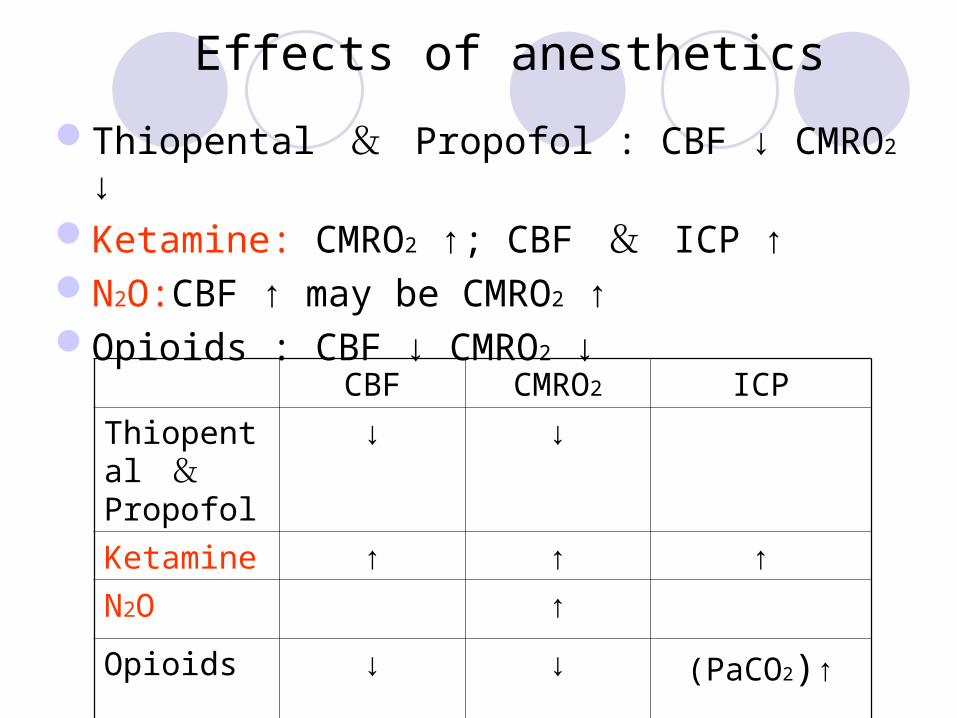
Thiopental & Propofol : CBF ↓ CMRO2 ↓Ketamine: CMRO2 ↑; CBF & ICP ↑ N2O:CBF ↑ may be CMRO2 ↑Opioids : CBF ↓ CMRO2 ↓
CBF CMRO2 ICP
Thiopental &
Propofol
↓ ↓
Ketamine ↑ ↑ ↑
N2O ↑
Opioids ↓ ↓ (PaCO2)↑
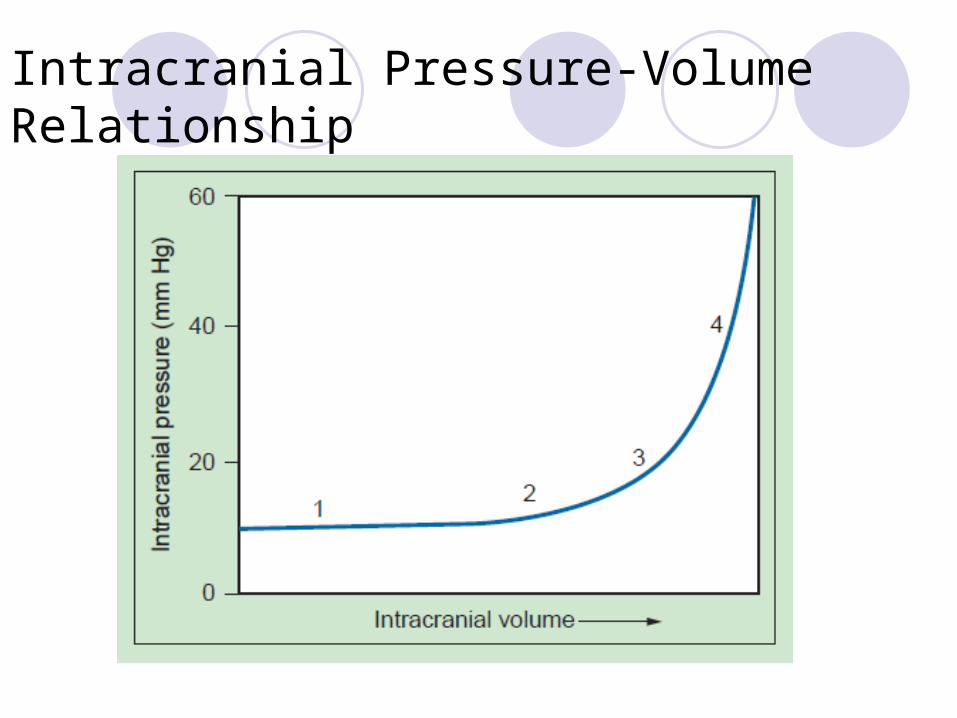
Intracranial Pressure-Volume Relationship
IICP
ICP=5-15mmHg
IICPPositional headacheNausea +VomitingHypertension + BradycardiaConscious changeAltered patterns of breathingPapilledema
Methods to decrease ICP
1.Cerebrospinal fluid ↓ Ventricular drainageLumbar drainageLasix
2.Cerebral blood volume↓ IV anestheticHyperventilationPaCO2 < 30mmHgAvoid hypotension & hypertension
3.Increase venous outflowElevate headAvoid constriction at the neck.Avoid PEEP Avoid airway pressure↑
4.Cerebral edema ↓Mannitol ;CraniectomyResection spaceOccupying lesionsPrevent ischemia
Effect of anesthetic on ICP
Intravenous anesthetic: CMRO2↓CBF ↓ICP ↓Avoid Etomidate (epilepsy history)Opioids: PaCO2↑Neuromuscular blocking drugs(-)
Volatile anesthetic :CBF ↑ CBV ↑ ICP↑ Dose-dependent increase
Cerebral protection
Cerebral protection
Barbiturates
Hypothermia
Intracranial Aneurysms
Pre-op Neurologic evaluation
IICP?
Vasospasm?EKGHHH therapy if vasospasm
Calcium channel blockers.
Induction Avoid ↑SBP. Maintain CPP
Avoid ischemia
HHH: Hypertension, Hypervolemia, Hemodilution
Intracranial Aneurysms
MaintenanceOpioid plus propofol or
volatile anesthetic Mannitol (0.25-1 g/kg IV) Normal or ↑systemic
blood pressure
PostoperativeNormal to ↑ systemic
blood pressure.Early awakening
Neurologic assessmentHHH therapy
HHH: Hypertension ,Hypervolemia Hemodilution
Preoperative Assessment
Altered level of consciousnessHeadachesMotor or sensory deficits IICP?Cranial nerve abnormalitiesCompression of the optic chiasm focal deficits or visual impairmentSeizuresSteroid/Diuretic/Anti-convulsion drug…etc.CT/MRI for mass lesion. Mid-line shift?
Monitoring
Standard monitors,ex:EKG,NIBP,SpO2
A-Line, CVP(not routinely used)Capnography, GASNMT (peripheral nerve stimulator)Foley catheter ICP or EVD monitor
Positioning- Supratentorial tumors
Intracranial vascular lesions
→Supine
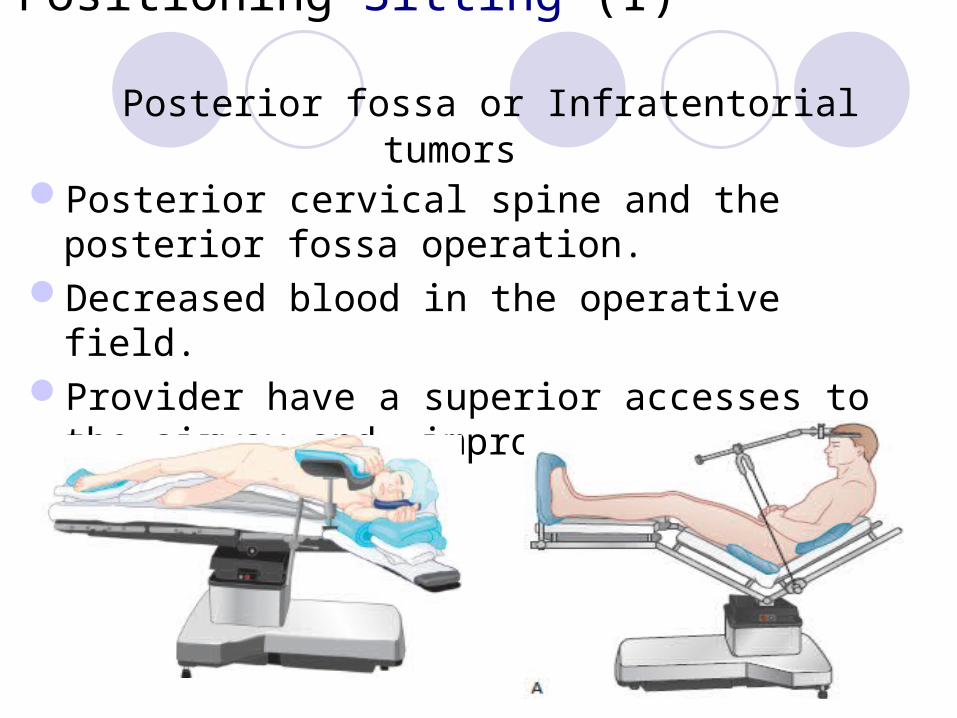
Positioning-Sitting (I) Posterior fossa or Infratentorial tumors
Posterior cervical spine and the posterior fossa operation.
Decreased blood in the operative field.Provider have a superior accesses to the airway
and improved ventilation.
Venous Air Embolism (I)Increased risk for venous air embolism
Significant elevation of the head
The operative site above the level of the heart
The venous sinuses in the cut edge of bone
or dura may not collapse when transected.
Venous Air Embolism (II)
ETCO2↓ 、 SpO2 ↓ 、 PaCO2 ↑
Arterial hypoxemia 、 Cardiovascular collapse
Transesophageal echocardiographyCentral venous catheter
Induction of Anesthesia
The Goal of induction Avoid Hyper/Hypotension As close as possible to and certainly within 10% of average awake values Avoid Cough Avoid ICP↑or MAP↓→CBF↓ Avoid use of PEEP PaCO2:Keep 30 and 35 mmHg
Common clinical cases
Intracranial Aneurysms Intracranial Masses Arteriorvenous Malformation (AVM)
Carotid Stenosis
Intracranial Masses
Pre-opIICP? Avoid sedatives
and opioidsCT/MRI Anxiolytics
MonitorsSupratentorial masses Standard ASA monitors,
A-line, Foley catheterInfratentorial masses depend on positioning
Induction+MaintenanceInduction+MaintenanceAvoid increasing ICPDeep anesthesia Skeletal muscle paralysis
Nitrous oxide (X)Mannitol (0.25-1g/kg IV)
Arteriorvenous Malformation (AVM)
Pre-opIs similar to that for
aneurysms.
Intra-op↓Blood lossA-line, IVHyperventilationMannitol
Resection
Embolization
Stereotactic Radiosurgery
(gamma knife).
Carotid Stenosis-Carotid Endarterectomy (CEA)
Pre-opNeurologic
examination is indicated to look for preoperative deficits.
Screen for associated CAD.
Anxiolytics may be useful.
Induction+ Maintenance
Avoid increases in mean arterial pressure
Maintain adequate CPP (baseline to 20% above)
during carotid clampingNitrous oxide.(X)
謝謝聆聽 !!
QUESTIONS OF THE DAY
1. What is cerebral autoregulation? Under what circumstances is it altered? What is the impact of intravenous (IV) or inhaled anesthetics on cerebral autoregulation? 2. What are the effects of changes in PaCO 2 or PaO 2 on cerebral blood flow? 3. What are the effects of IV or inhaled anesthetics on cerebral blood flow? 4. What are the manifestations of venous air embolism in a patient undergoing craniotomy under general anesthesia? What is
the appropriate management? 5. During craniotomy for tumor resection, the surgeon notes “brain swelling” in the operative field. What are the initial steps in management? 6. A patient with subarachnoid hemorrhage (SAH) pre-sents for intracranial aneurysm clipping. What complications of SAH may develop in the perioperative period?