Attenuated Neuropathology by Nilvadipine After Middle...
6
51 Attenuated Neuropathology by Nilvadipine After Middle Cerebral Artery Occlusion in Rats Shingo Kawamura, MD; Mitsuru Shirasawa, MT; Hitoshi Fukasawa, MD; and Nobuyuki Yasui, MD We investigated the effects of nilvadipine, a calcium antagonist, on cerebral ischemia in rats. Under halothane anesthesia, 30 rats had a 3-0 nylon suture introduced through the ex'tracra- nial internal carotid artery to occlude the left middle cerebral artery. Nilvadipine was dissolved in polyethylene glycol 400. Immediately following occlusion, group 1 rats (n=10) were treated subcutaneously with vehicle and group 2 and 3 rats were treated with 1.0 (n=10) add 3.2 (n = 10) nig/kg nilvadipine, respectively. Pcrfusion fixation was performed 24 hours later, and the histopathologlc outcomes were quantified. In group 1 infarct volume was 28.2 ±11.4% of the total cerebral volume; in groups 2 and 3 infarct volumes were 25.5±11.6% (NS) and 13.9±9.2% (p<0.05 different from group 1),respectively.Nilvadipine decreased ischemic neuronal injury in a dose-dependent manner and may be of use in the treatment of cerebral ischemia. (Stroke 1991^2:51-55) C erebral ischemia causes massive influx of Ca 1+ into neurons, a so-called final common path- way of cell death. 1 Thus, the inhibition of Ca 2+ entry into cells has been proposed as a thera- peutic measure for cerebral ischemia, 2 " 4 and recent evidence suggests that calcium entry blockers atten- uate ischemic neuronal damage through two mecha- nisms: dilation of cerebral vessels and prevention of excessive Ca 2+ influx into cytoplasmic and mitochon- dria! compartments. 2 - 5 ' 6 Nilvadipine (FR 34235) is a new dihydropyridine calcium entry blocker structurally related to nifedi- pine 7 but 5-10 times more potent against KC1- induced vasoconstriction in dog coronary and basilar artery strips. 8 Previous research has shown that nil- vadipine has a potent vasodilator effect similar to that of nifedipine on norepinephrine-induced con- striction in the basilar artery 9 and thoracic aorta 10 of rabbits. Moreover, nilvadipine was effective in reduc- ing ischemia in a dog model of chronic coronary artery occlusion 1 ' and may be a therapeutic agent for cerebral ischemia. 12 We investigated the effects of nilvadipine on focal cerebral ischemia. In an improved rat model of uni- From the Departments of Surgical Neurology (S.K., N.Y.) and Pathology (M.S., H.F.), Research Institute for Brain and Blood Vessels-Akita, Akita Japan. Address for correspondence: Shingo Kawamura, MD, Depart- ment of Surgical Neurology, Research Institute for Brain and Blood Vessels-Akita, 6-10, Senshu-kubota-machi, Akita 010, Japan. Received May 1, 1990; accepted September 20, 1990. lateral middle cerebral artery (MCA) occlusion, we used the intraluminal suture technique 13 - 14 and as- sessed histopathologic outcomes. Materials and Methods Thirty adult male Sprague-Dawley rats weighing 250-340 g were housed at 22±2°C, 50+10% humid- ity, and a 12-hour light/dark cycle with free access to food and water. Halothane was used to induce (4% in a mixture of 75% N 2 O and 25% O 2 ) and maintain (1%) anesthesia; 0.25 mg i.p. atropine sulfate was used for premedication. Each rat was allowed to breathe spontaneously, and rectal temperature was maintained at 37 C C with a heating pad. The tail artery was cannulated for continuous monitoring of mean arterial blood pressure, as well as for repeated blood sampling for serial measurements of Pao 2 , PacO2, pH, hematocrit, hemoglobin concentration, and plasma glucose concentration. Gases were ana- lyzed using the ABL 330 device (Radiometer, Copen- hagen, Denmark); hemoglobin and plasma glucose concentrations were measured with Ektachem DT60 (Eastman Kodak Co., Rochester, N.Y.). We occluded the left MCA using a modification of the method described by Zea Longa et al. 14 Briefly, the left external carotid artery (ECA) was isolated via a ventral midline incision, and the only branch of the extracranial internal carotid artery (ICA), the pterygopalatine artery, was then isolated. The origin of the pterygopalatine artery was occluded with a microvascular clip so that the intraluminal suture was by guest on July 12, 2018 http://stroke.ahajournals.org/ Downloaded from
Transcript of Attenuated Neuropathology by Nilvadipine After Middle...

51
Attenuated Neuropathology byNilvadipine After Middle Cerebral
Artery Occlusion in RatsShingo Kawamura, MD; Mitsuru Shirasawa, MT;
Hitoshi Fukasawa, MD; and Nobuyuki Yasui, MD
We investigated the effects of nilvadipine, a calcium antagonist, on cerebral ischemia in rats.Under halothane anesthesia, 30 rats had a 3-0 nylon suture introduced through the ex'tracra-nial internal carotid artery to occlude the left middle cerebral artery. Nilvadipine was dissolvedin polyethylene glycol 400. Immediately following occlusion, group 1 rats (n=10) were treatedsubcutaneously with vehicle and group 2 and 3 rats were treated with 1.0 (n=10) add 3.2 (n = 10)nig/kg nilvadipine, respectively. Pcrfusion fixation was performed 24 hours later, and thehistopathologlc outcomes were quantified. In group 1 infarct volume was 28.2 ±11.4% of thetotal cerebral volume; in groups 2 and 3 infarct volumes were 25.5±11.6% (NS) and 13.9±9.2%(p<0.05 different from group 1), respectively. Nilvadipine decreased ischemic neuronal injuryin a dose-dependent manner and may be of use in the treatment of cerebral ischemia. (Stroke1991^2:51-55)
Cerebral ischemia causes massive influx of Ca1+
into neurons, a so-called final common path-way of cell death.1 Thus, the inhibition of
Ca2+ entry into cells has been proposed as a thera-peutic measure for cerebral ischemia,2"4 and recentevidence suggests that calcium entry blockers atten-uate ischemic neuronal damage through two mecha-nisms: dilation of cerebral vessels and prevention ofexcessive Ca2+ influx into cytoplasmic and mitochon-dria! compartments.2-5'6
Nilvadipine (FR 34235) is a new dihydropyridinecalcium entry blocker structurally related to nifedi-pine7 but 5-10 times more potent against KC1-induced vasoconstriction in dog coronary and basilarartery strips.8 Previous research has shown that nil-vadipine has a potent vasodilator effect similar tothat of nifedipine on norepinephrine-induced con-striction in the basilar artery9 and thoracic aorta10 ofrabbits. Moreover, nilvadipine was effective in reduc-ing ischemia in a dog model of chronic coronaryartery occlusion1' and may be a therapeutic agent forcerebral ischemia.12
We investigated the effects of nilvadipine on focalcerebral ischemia. In an improved rat model of uni-
From the Departments of Surgical Neurology (S.K., N.Y.) andPathology (M.S., H.F.), Research Institute for Brain and BloodVessels-Akita, Akita Japan.
Address for correspondence: Shingo Kawamura, MD, Depart-ment of Surgical Neurology, Research Institute for Brain and BloodVessels-Akita, 6-10, Senshu-kubota-machi, Akita 010, Japan.
Received May 1, 1990; accepted September 20, 1990.
lateral middle cerebral artery (MCA) occlusion, weused the intraluminal suture technique13-14 and as-sessed histopathologic outcomes.
Materials and MethodsThirty adult male Sprague-Dawley rats weighing
250-340 g were housed at 22±2°C, 50+10% humid-ity, and a 12-hour light/dark cycle with free access tofood and water. Halothane was used to induce (4% ina mixture of 75% N2O and 25% O2) and maintain(1%) anesthesia; 0.25 mg i.p. atropine sulfate wasused for premedication. Each rat was allowed tobreathe spontaneously, and rectal temperature wasmaintained at 37CC with a heating pad. The tailartery was cannulated for continuous monitoring ofmean arterial blood pressure, as well as for repeatedblood sampling for serial measurements of Pao2,PacO2, pH, hematocrit, hemoglobin concentration,and plasma glucose concentration. Gases were ana-lyzed using the ABL 330 device (Radiometer, Copen-hagen, Denmark); hemoglobin and plasma glucoseconcentrations were measured with Ektachem DT60(Eastman Kodak Co., Rochester, N.Y.).
We occluded the left MCA using a modification ofthe method described by Zea Longa et al.14 Briefly,the left external carotid artery (ECA) was isolatedvia a ventral midline incision, and the only branch ofthe extracranial internal carotid artery (ICA), thepterygopalatine artery, was then isolated. The originof the pterygopalatine artery was occluded with amicrovascular clip so that the intraluminal suture was
by guest on July 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from

52 Stroke Vol 22, No 1, January 1991
TABLE 1. Values of Physiological Variables in Rats Daring and After Middle Cerebral Artery Occlusion
Group
Group 1 (n=10)
During surgery
15 min after surgery
24 hr after surgery
Group 2 (n = 10)
During surgery
15 min after surgery
24 hr after surgery
Group 3 (n = 10)
During surgery
15 min after surgery
24 hr after surgery
MABP(mm Hg)
81±8
88+17
96±13
83±9
75±10
86+7
87+12
61±10*t86±8
Pao?(mmHg)
106±13101±13114±18
106±7100±6112±9
105+10102±8112±10
Paco^(mmHg)
49.2±6_5
49.3±7.3
48.2±8.4
48.5±3.8
48.4±4.1
48.3±6.0
49.0±5.8
49.1 ±3.8
46.1±4.0
pH
737±0.04
7.37±0.04
7.36±0.O6
737+0.03
7.37±0.03
7.38±0.04
7.39±0.03
7.37±0.02
7.40+0.03
Glucose(mg/dl)
209±15
128±13
209±9
133±13
204±18
141±16
Hematocrit(%)
41±2
44±2
41±2
43±2
42±2
42±4
Hemoglobin(g/dl)
12±1
14±1
12±1
14±1
13±1
13±2
Values are mean±SD. MABP, mean arterial blood pressure.*p<0.05 different from Group 1 or 2 by SchefW's multiple-comparison procedure.tp<0.05 different from during surgery by repeated-measures analysis of variance and Dunnett's test.
never introduced erroneously into the pterygopala-tine artery (we have since learned that the pterygo-palatine artery can be clipped without dissecting thestylohyoid muscle). Next, the ECA was ligated and a20-mm 3-0 monofiJament nylon suture with its tiptapered and rounded with fine sand paper was intro-duced into the ECA stump. Approximately 17.5 mmof the nylon suture was advanced into the ICA, andfaint resistance was then felt, indicating that the tipof the suture had entered the anterior cerebralartery. The origin of the MCA was thus occluded bythe intraluminal suture, and blood flow from theICA, the anterior cerebral artery, and the posteriorcerebral artery to the MCA was blocked at the circleof Willis.
Nilvadipine was dissolved in polyethylene glycol400. This drug is photoresistant in solution (unpub-lished data, Fujisawa Pharmaceutical Co. Ltd., Os-aka, Japan). The rats were randomly divided intothree groups of 10 rats each. Group 1 (control) ratswere treated with 1 ml/kg s.c. vehicle immediatelyafter MCA occlusion; groups 2 and 3 rats weretreated with 1 ml/kg s.c. nilvadipine solution (1.0 and3.2 mg/ml, respectively). The skin incision was thenclosed. The catheter in the tail artery was filled withheparin and heat-sealed by a flame. The N2O/O2
mixture was switched to room air 20 minutes afterMCA occlusion, and the rats were then returned toindividual cages. No rat showed signs of distress orpain during the postoperative period.
Twenty-four hours after MCA occlusion, the ratswere anesthetized with 40 mg/kg i.p. pentobarbitalsodium. Each rat was breathing spontaneously, andits rectal temperature was controlled at 37°C. Hep-arin (1,000 IU/kg) was administered intravenously,and the tail artery again served for the continuousmonitoring of mean arterial blood pressure and serialblood sampling. The heart was exposed via a midlineincision, and a cannula was inserted into the ascend-ing aorta via the left ventricle. The inferior vena cava
was occluded with an aneurysm clip, and the rightatrium was then incised. Perfusion fixation was per-formed with 10% buffered formalin. The brain wasremoved from the skull and stored in 15% bufferedformalin.
The forebrain was embedded in paraffin wax.Coronal sections 5 /xm thick were obtained andstained with hematoxylin and eosin. Area was mea-sured in eight coronal sections 1.5 mm apart, the firstsection 2.5 mm posterior to the frontal tip. Areas ofthe hemisphere and areas of ischemic neuronal death(infarction) were plotted on tracings from projectionsof the coronal sections. Areas of infarction were thenmeasured using an image analyzer (Texture Analyz-ing System, Leitz, Wetzlar, F.R.G.) separately for thestriatum, pallium, and each hemisphere. The volumeof infarction was calculated with a computer programusing numerical integration of the areas of infarctionfor the eight coronal sections and the distancesbetween them. At the same time, the volume of eachhemisphere was calculated using the hemisphericareas measured. Infarct volume was expressed bothas a percentage of the total cerebral volume and inabsolute terms as cubic millimeters.
Prior to perfusion fixation, blood was aspiratedfrom the right atrium of the heart, immediatelycooled in an ice bath, and then centrifuged at 3,000rpm and 4°C for 10 minutes. To inhibit enzymaticdegradation of nilvadipine, 10~3 M bis-p-nitrophenylphosphate (Nakarai, Kyoto, Japan), an esterase in-hibitor, was added to the plasma obtained. Thisplasma (2.5 ml) was stored at -20°C until the plasmaconcentration of nilvadipine (pCN) was measuredusing gas chromatogTaphy.15
We calculated mean, standard deviation (SD), andstandard error of the mean (SEM) for all data. Forbetween-group comparisons, we used Scheff6's multi-ple-comparison procedure. For within-group compari-sons of physiological values, we used repeated-measureanalysis of variance and Dunnett's test. We compared
by guest on July 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Kawamura et al Ca2+ Antagonist in Rat MCA Occlusion 53
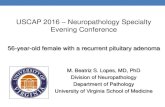
FIGURE 1. Representative pho-tomicrographs of ischemic braindamage in (top) vehicle-treatedcontrol rat and (bottom) rattreated with 3.2 mglkg nilvad-ipine. Hematoxylin and eosinstain.
pCN between groups 2 and 3 using Student's unpaired ttest. We considered p<0.05 to be significant.
ResultsIn groups 1 and 2 mean arterial blood pressure
remained stable (Table 1). However, in group 3blood pressure decreased by approximately 25mm Hg after the administration of nilvadipine(p<0.05) and was lower than that in groups 1 and 2(p<0.05). Several rats developed mild hypercapniadue to surgical anesthesia. All other values werewithin normal ranges.
Prior to sacrifice, several rats again exhibited mildhypercapnia under anesthesia (Table 1). All othervalues were within normal ranges. Groups 2 and 3
had similar mean arterial blood pressures, both lowerthan that of group 1. However, these values did notdiffer significantly among the groups.
There was a remarkably consistent pattern ofischemic brain damage, and typical examples in ratsfrom groups 1 and 3 are shown in Figure 1. Lesionswere seen in the dorsolateral frontopanetal cortex,the caudoputamen, and the globus pallidus. Theboundaries between areas of infarction and adjacentnormal areas were sharply delineated.
Absolute and percentage infarct volumes in eachgroup are shown in Figures 2 and 3, respectively. Ingroup 1, mean±SD absolute infarct volume was42±10 mm3 in the striatum and 124±65 mm3 in thepallium, for a total of 166±73 mm3; mean±SD
by guest on July 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from

54 Stroke Vol 22, No 1, January 1991
so-i s>
o
FIGURE 2. Bar graphs of mean±SEM absolute infarctvolume in striatum (top), pallium (middle), and total brain(bottom) of vehicle-treated control rats (open bars), ratstreated with 1.0 mglkg nilvadipine (shaded bars), and ratstreated with 3.2 mglkg nilvadipine (filled ban). Ten rats ineach group. -kp<0.05 by Scheffis multiple-comparison proce-dure.
percentage infarct volume was 28.2± 11.4%. In group2, mean ± SD absolute infarct volume was 41 ± 12 mm3
in the striatum and 107±64 mm3 in the pallium, for atotal of 14#±71 mm3; mean±SD percentage infarctvolume was 25.5 ±11.6%. All of these values forgroup 2 were lower than those for group 1, but notsignificantly so.
On the contrary, in group 3 the total absoluteinfarct volume (77±50 mm3) was less than that ofgroup 1 (/?<0.05). Absolute infarct volume in thestriatum (31 ±16 mm3) was less than, but not signifi-cantly different from, that of group 1. Absoluteinfarct volume in the pallium (46±37 mm3) was alsoless than that of group 1 (p<0.05). Therefore, thesignificant difference in total absolute infarct volumeresulted from a decrease in absolute infarct volumein the pallium. As shown in Figure 1, bottom, infarctvolume decreased in the peripheral area of thefrontoparietal cortex. The percentage infarct volumeof group 3 was 13.9±9.2% (/><0.05 different fromgroup 1).
No nilvadipine was detected in plasma obtainedfrom group 1 rats. Mean±SD pCn in group 2 was0.38±0.27 ng/ml, and that in group 3 was morevariable (1.67 ±2.00 ng/ml). There was no significantdifference between groups 2 and 3 (/;<0.06).
DiscussionOur results clearly demonstrate that nilvadipine
reduces infarct volume in rats in a dose-dependent
2 0 -
FlGURE 3. Bar graphs of mean±SEM percentage infarctvolume of vehicle-treated control rats (open bars), rats treatedwith 1.0 mglkg nilvadipine (shaded bars), and rats treatedwith 3.2 mglkg nilvadipine. Ten rats in each group. -kp<0.05by Scheffis multiple-comparison procedure.
manner when given just after MCA occlusion. Asignificant decrease in infarct volume was observed inthe periphery of the pallium. In addition, nilvadipinelowered mean arterial blood pressure 15 minutesafter its administration in a dose-dependent manner.Twenty-four hours after the administration of asingle dose, nilvadipine was detected in the systemiccirculation.
Calcium entry blockers are widely used in thetreatment of such cardiovascular diseases as coronaryartery disease, arrhythmias, cerebral vasospasm, andhypertension. The therapeutic effects of these agentshave been attributed to inhibition of the influx ofCa2+ into cells in both myocardial tissue and vascularsmooth muscle.16 However, this inhibitory action mayinduce adverse side effects on cardiac functions (e.g.,negative inotropy and chronotropy). Nilvadipine wasdeveloped to minimize these undesirable effects; itshows high specificity for vascular smooth muscle andhas long-lasting effects.81017
In spite of extensive investigation, the mechanismof action of calcium entry blockers on cerebral isch-emia is still unclear. Several possible mechanismssuggest that such drugs ameliorate ischemic cerebraldamage by affecting cerebral vasoconstriction,518
platelet aggregation,19 and neuronal membrane andmitochondrial functions.20 Recent investigations intobrain ischemia in several animal species2-4-21-22 andstroke patients23-24 have shown that calcium entryblockers may improve cerebral blood flow and me-tabolism. Improvements in neurologic and neuro-pathologic outcomes have also been observed inother studies.325 The results of Germano et al3
indicate that nimodipine improved neurologic out-come and decreased the size of infarcts when admin-istered up to 6 hours after MCA occlusion in rats. Onthe other hand, dihydropyridine calcium entry block-ers may increase the susceptibility of brain tissue toischemic damage in baboons26 and did not attenuatebrain damage after focal cerebral ischemia in cats.27
The reasons for these differences in the effects ofdihydropyridine calcium entry blockers are unclear,but they may be due to differences in species or themethods of inducing cerebral ischemia.
We observed a decrease in infarct volume in theperiphery of the pallium, where there was collateral
by guest on July 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Kawamura et al Ca2+ Antagonist in Rat MCA Occlusion 55
circulation from the anterior and posterior cerebralarteries. This area appears to correlate anatomicallywith the ischemic penumbra, the area of nonfunc-tioning but structurally preserved brain tissue at theperiphery of infarction. Infarct volume in the isch-emic core (i.e., the basal ganglia and internal cap-sule) did not decrease significantly (Figure 2) al-though infarct volume tended to decrease in themedial areas of the striatum (Figure 1).
Our results suggest that nilvadipine provides apossible measure for the treatment of cerebral isch-emia. However, we administered nilvadipine onlyimmediately following an ischemic insult. Furtherstudy is needed to determine whether this treatmenthas beneficial effects when initiated up to severalhours following the insult.
Acknowledgments
We gratefully acknowledge the technical assistanceof Yozo Ito and Ryoetu Sato, the secretarial assist-ance of Maki Kan and Kimio Yoshioka, and thephotography of Yoshitaka Tozawa. Fujisawa Phar-maceutical Co. Ltd., Osaka, Japan, provided thenilvadipine (Lot No. 505145P).
References1. Schanne FA, Kane AB, Young EE, Farber JL: Calcium
dependence of toxic cell death: A final common pathway.Science 1979;206:700-702
2. Meyer FB, Anderson RE, Yaksh TL, Sundt TM Jr: Effect ofnimodipine on intracellular brain pH, cortical blood flow, andEEG in experimental focal cerebral ischemia. / Ncumsurg1986;64:617-626
3. Germano 1M, Bartkowski HM, Cassel ME, Pitts LH: Thetherapeutic value of nimodipine in experimental focal cerebralischemia. Neurological outcome and histopathological find-ings. J Neurosurg 1987;67:81-87
4. Kucharczyk J, Chew W, Derugin N, Moseley M, RoUin C,Berry I, Norman D: Nicaidipine reduces ischemic brain injury.Magnetic resonance imaging/spectroscopy study in cats. Stroke1989;20:268-274
5. Brandt L, Ljunggren B, Andersson K-E, Edvinsson L, Mac-Kenzie E, Tamura A, Teasdale G: Effects of topical applica-tion of a calcium antagonist (nifedipine) on feline cortical pialmicrovasculature under normal conditions and in focal isch-emia. / Cereb Blood Flow Metab 1983^:44-50
6. Rosenblum Wl: Effects of calcium channel blockers on pialvascular responses to receptor mediated constrictors. Stroke1984;15:284-287
7. Ohtsuka M, Ono T, Shibayama F: Nilvadipine. CardiovascDrug Rev 1988;6:97-115
8. Ohtsuka M, Ono T, Hiroi J, Esumi K, Kikuchi H, Kumada S:Comparison of the cardiovascular effect of FR34235, a newdihydropyridine, with other calcium antagonists. J CardiovascPharmacol 1983;5:1074-1082
9. Takagi T, Satake N, Shibata S: The inhibitory action of FR34235 (a new Ca2+ entry blocker) as compared to nimodipineand nifedipine on the contractile response to norepinephrine,potassium and 5-hvdroxytryptamine in rabbit basilar artery.Eur J Pharmacol 1983;90:297-299
10. Furuta T, Shibata S, Kodama I, Yamada K: Cardiovasculareffects of FR34235, a new dihydropyridine slow channel
blocker, in isolated rabbit myocardium and aorta. J CardiovascPharmacol 1983^:836-841
11. Warltier DC, Zyvoloski MG, Brooks HL, Gross GJ: Beneficialeffects of the dihydropyridine calcium antagonist, FR 34235, ina chronic coronary occlusion model. Eur J Pharmacol 1982;80:149-153
12. Kuwaki T, Satoh H, Ono T, Shibayama F, Yamashita T,Nishimura T: Nilvadipine attenuates ischemic degradation ofgerbil brain cytoskeletal proteins. Stroke 1989;20:78-83
13. Koizumi J, Yoshida Y, Nakazawa T, Ooneda G: Experimentalstudies of ischemic brain edema 1. A new experimental modelof cerebral embolism in rats in which recirculation can beintroduced in the ischemic area (in Japanese with Englishabstract). Jpn J Stroke 1986;8:l-8
14. Zea Longa E, Weinstein PR, Carlson S, Cummins R: Revers-ible middle cerebral artery occlusion without craniectomy inrats. Stroke 1989;20:84-91
15. Tokuma Y, Fujiwara T, Sekiguchi M, Noguchi H: Determina-tion of nilvadipine in plasma and urine by capillary column gaschromatography with electron-capture detection. / Chro-matogr 1987;415:156-162
16. Fleckenstein A: Specific inhibitors and promoters of calciumaction in the excitation-contraction coupling of heart muscleand their role in the prevention or production of myocardiallesions, in Harris P, Opie H (eds): Calcium and the Heart.London, Academic Press, 1971, pp 135-188
17. Ohtsuka M, Koibuchi Y, Sakai S, Tsujioka K, Fujiwara T, OzakiT, Maeda K, Motoyama I, Horiai H, Ono T, Shibayama F:Effects of nilvadipine on the cardiovascular system in experi-mental animals. Arzneimittelforschung 1988;38:1605-1618
18. Harper AM, Craigen L, Kazda S: Effect of the calciumantagonist, nimodipine, on cerebral blood flow and metabo-lism in the primate. / Cereb Blood Flow Metab 1981;l:349-356
19. Aiagno R, Doni MG: The exclusion of the cerebral circula-tion: Effect on the "in vivo" platelet aggregation. Thromb Res1976;9:319-327
20. Harris RJ, Symon L, Branston NM, Bayhan M: Changes inextracellular calcium activity in cerebral ischaemia. J CerebBlood Flow Metab 1981;1:203-209
21. Heffez DS, Passonneau JV: Effect of nimodipine on cerebralmetabolism during ischemia and recirculation in the Mongo-lian gerbil. J Cereb Blood Flow Metab 1985^:523-528
22. Mohamed AA, Mendelow AD, Teasdale GM, Harper AM,McCulloch J: Effect of the calcium antagonist nimodipine onlocal cerebral blood flow and metabolic coupling. J CerebBlood Flow Metab 1985^:26-33
23. Gelmers HJ: Effect of nimodipine (Bay e 9736) on post-isch-aemic cerebrovascular reactivity, as revealed by measuringregional cerebral blood flow (rCBF). Ada Neurochir (Wien)1982;63:283-290
24. Hakim AM, Ev.-uis AC, Berger L, Kuwabara H, Worsley K,Marchal G, Biel C, Poknipa R, Diksik M, Meyer E, Gjedde A,Marrett S: The effect of nimodipine on the evolution of humancerebral infarction studied by PET. J Cereb Blood Flow Metab1989;9:523-534
25. Steen PA, Newberg LA, Milde JH, Michenfelder JD: Cerebralblood flow and neurologic outcome when nimodipine is givenafter complete: cerebral ischemia in the dog. J Cereb BloodFbw Metab 1984;4:82-87
26. Harris RJ, Branston NM, Symon L, Bayhan M, Watson A: Theeffects of a calcium antagonist, nimodipine, upon physiologicalresponses of t he cerebral vasculature and its possible influenceupon focal cerebral ischaemia. Stroke 1982;13:759-766
27. Reedy DP, IJttle JR, Capraro JA, Slugg RM, Lasser RP:Effects of veiapamil on acute focal cerebral ischemia. Neuro-surgery 1983; 12:272-276
KEY WORDS • calcium channel blockers • cerebral ischemia •rats
by guest on July 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from

S Kawamura, M Shirasawa, H Fukasawa and N YasuiAttenuated neuropathology by nilvadipine after middle cerebral artery occlusion in rats.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1991 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.22.1.51
1991;22:51-55Stroke.
http://stroke.ahajournals.org/content/22/1/51World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from