ASSOCIATION OF PHYSICIANS
59
Transcript of ASSOCIATION OF PHYSICIANS


ASSOCIATION OF PHYSICIANS
OF BANGLADESH
JOURNAL COMMITTEE
ADVISORY BOARD
National Prof. Nurul IslamNational Prof. Brig. (Retd.) Abdul Malik
Prof. M. Amanullah
Prof. M. Nurun Nabi
Maj. Gen. (Rtd.) A. R. Khan
Prof. M.A. Mannan
Prof. A.K.M. Nazimuddowla Chowdhury
Prof. Akhtar Hossain
Prof. R. K. Khondokar
Prof. A. Q. M. B. Chowdhury
Prof. Md. Tahir
Prof. A. F. M. Aminul Islam
Prof. Enayet Ullah
Prof. A. K. Azad Khan
Prof. A. Q. M. Qamaruzzaman
Prof. Hazera Mahtab
Prof. Ferdous Ara J. Janan
Prof. P. Purkayastha
EDITORIAL BOARD
Editor : Prof. Mahmud Hasan
Assistant Editors : Prof. Projesh Kumar Roy
Prof. Khan Abul Kalam Azad
Dr. A.K.M. Mosharraf Hossain
Members : Prof. Fazlul Haque
Prof. Tofayel Ahmed
Prof. Naseem Akhter Chowdhury
Prof. A. K. M. Rafiqueuddin Ahmed
Prof. Anisul Haque
Major Gen. (Retd.) Md. Abdul Moyeed Siddiqui
Prof. Zafar A. Latif
Prof. M.A. Faiz
Prof. Syed Atiqul Haq
Prof. Md. Salimur Rahman
Prof. Chandanendu Bhushan Sarker
Prof. Md. Golam Rabbani
Prof. Md. Abu Siddique
Prof. M. A. Jalil Chowdhury
Prof. Muhammad Rafiqul Alam
Prof. Baren Chakroborty
Dr. Md. Abdur Rahim Miah

ASSOCIATION OF PHYSICIANS
OF BANGLADESH
EXECUTIVE COMMITTEE 2009-2011
President : Professor AKM Rafique Uddin
Vice-Presidents : Professor Syed Atiqul Haq
Professor Md. Abdul Jalil Chowdhury
Secretary General : Dr. AKM Mosharraf Hossain
Joint Secretary : Professor Md. Golam Rabbani
Treasurer : Professor Md. Mujibur Rahman
Secretary for Scientific Affairs : Dr. Abdul Wadud Chowdhury
Organizing Secretary : Professor MA Rashid
Members : Professor Mahmud Hasan
Professor Mobin Khan
Professor AZM Maidul Islam
Professor Md. Abul Kashem Khandaker
Professor Shahana Rahman
Professor Muhammad Rafiqul Alam
Professor Firoz Ahmed Quraishi
Professor Quazi Tariqul Islam
Professor Azizul Kahhar
Ex-officio
Professor Quazi Deen Mohammad
Professor Khwaja Nazimuddin

CONTENTS
Original Articles
Comparative Prevalence of Irritable Bowel Syndrome (IBS) Using Multiple Diagnostic Criteria 1-6
Irin Perveen, Mahmud Hasan
Azithromycin Versus Ciprofloxacin for the Treatment of Uncomplicated 7-13
Enteric Fever In Bangladesh - A Randomized Trial
Durba Halder, Samir Kumar Kundu, M Matiur Rahman, MA Azhar
Serum Zinc Level in Patients with Vitiligo in a Tertiary Hospital in Bangladesh 14-18
Rubaiya Ali, Nargis Akhtar, Mohammad S. Ahsan, Ayesha Hassan, Mohammad Asifuzzaman
Feeding Practice among Anemic and Non-Anemic Infants and Young Children in 19-24
A Selected Rural Area
Mithun Alamgir, Jannatara Shefa, Khan Shakil Ahmed, Shafinaz Gazi,
Mohammad Ferdous Ur Rahaman, Md. Abul Kalam Azad
Clinico-Epidemiological Profile of Seborrheic Dermatitis 25-28
Lubna Khondker, Md Abdul Wahab, Md Shirajul Islam Khan
Study on Aetiology and Outcome of Fulminant Hepatic Failure in Bangladeshi Patients 29-33
Swadesh Kumar Chakrovortty, Rajib Barua, Dewan Saifuddin Ahmed,
Mohammad Abul Kalam Azad, Abu Bakar Siddique, Md. Abul Kalam Azad
Oral Hygiene Among Type 2 Diabetes Patients: A Study of 276 Cases 34-36
Kulsum Umme, Mahmud A, Azam MG, Ahmed JU, Nazimuddin K
Psychiatric Morbidity among Women Whose Husbands are Living Abroad 37-40
M A Salam, Mohammad S. Ahsan, Nafia F. Chowdhury, Syed F. Shams,
Nahid M. Morshed, Mohsin Ali Shah, Monirul Islam
Review Article
Evidence Based Non Pharmacologic Management of Osteoarthritis: A Review 41-45
Rowsan Ara, Md Zahid Alam, Mohammad Ferdous Ur Rahaman,
Monzoor Quader, Jannatara Shefa
Case Reports
Calf Muscle Myokymia - A Brief Review 46-48
Monzoor Quader, Md Abul Kalam Azad, Md. Abdur Rahim, Syedul Islam,
Akhtarul Islam Chowdhury, Mohammad Ferdous Ur Rahaman
Chest Wall Deformity With Severe Respiratory Distress- A Rare Presentation 49-52
of Parathyroid Adenoma
A K M Motiur Rahman Bhuiyan, Monzoor Quader, Nizam Uddin Ahmed,
Mohammad Abul Kalam Azad, Md Zilan Miah Sarker, Mohammad Mobarock Hossain
Septic Arthritis in a Renal Transplant Patient 53-54
Pradip Kumar Dutta, Sayed Md Jabed, Saibal Das, Md Nurul Huda,
Md Maminul Islam, Dipen Chowdhury,Md Shariful Islam, Abul Kashem, Dipti Chowdhury

numerical order corresponding to the orders of
citation in the text. All authors should be quoted for
papers with upto six authors, for papers with more
than six authors the first six only should be quoted
followed by et al.
Abbreviations for titles of medical periodicals should
conform to those used in the latest edition of Index
Medicus. The first and last page numbers for each
reference should be provided. Abstracts and letter
must be identified as such. Authors must check
references against original sources for accuracy.
Examples of reference are given below:
Articles in Journals :
1. Paganini Hill A, Chao A, Ross Rk, Henderson BE.
Aspirin use and chronic disease : a cohort study of
the elderly. BMJ 1989; 299: 1247-50.
2. Parkin DM, Clayton D, Blook RJ, Massyer E, Fried
HP, Iranov E, et al. Childhood Leukaemia in Europe
after Chernobyl : 5 years follow-up. Br J Cancer 1996;
73 : 1006-12.
Chapter in a Book :
1. Phyllyps SJ, Whisnant JP. Hypertension and Stroke.
In : Lurgh JH, Brennes BM, editors. Hypertension :
Pathophysiology, diagnosis and management. 2nd ed.
New York : Raven Press; 1995. p. 465-78.
Tables should be as few as possible and should
present only essential data. Each table should be
type-written on separate sheets, have a title or
caption with Roman numbers. All photographs,
graphs, diagrams should be referred to as figures and
should be numbered consecutively in the text in
Arabic numericals. The legends for illustrations
should be typed on separate sheets. Photographs
and photomicrographs should be unmounted glossy
prints. Photomicrographs should have internal scale
markers, include in the legend the original
magnification and the stain used. Line diagrams and
graphs should be on separate sheets drawn with black
Indian ink on white paper. A photocopy of all
illustrations should be submitted.
Proofs :
Two marked copies of the proofs may be sent to the
principle author which should be read carefully for
error. One corrected copy must be returned to the
editor within the next three days. Major alteration in
the text cannot be accepted.
Editorial Mail :
Manuscripts and other communication for the editors
should be addressed to Prof. M N Alam, The Editor,
Bangladesh Journal of Medicine and Professor of
Medicine, Bangabandhu Sheikh Mujib Medical
University, Shahbagh, Dhaka, Bangladesh.
INSTRUCTION TO AUTHORS
The Journal of Association of Physicians of
Bangladesh publishes original papers, reviews
concerned with recent practice and case reports of
exceptional merit. The Journal considers manuscripts
prepared in accordance with the guidelines laid down
by the international committee of Medical Journal
Editors (BMJ 1988; 296: 401-405). A covering letter
signed by all authors must state that the data have
not been published elsewhere in whole or in part
and all authors agree their publication in Journal of
Association of Physicians of Bangladesh. If the work
has been conducted abroad then the article must be
accompanied by certificate from head of the institute
where the work has been done.
Type scripts :
Three typed copies of the article and one copy in a
3.5" high density floppy diskette processed in
Wordperfect 6.0 or MS Word 6.0 should be submitted
to the Editor. The text should be type-written in double
space on one side of the paper not larger than ISO
A4 with a 5 cm margin and paper should be numbered
consecutively. The first page of the type script should
bear the names of the author(s) and the name and
address of the laboratory or institution where the
work has been carried out, in addition to the title of
the paper. The full address of the principal author to
whom proofs will be sent should be given as footnote,
as should any permanent change of address and/or
appointment. A short (running) title of not more than
45 characters should be given. Please write as
concisely as possible. Amendments should be made
in the texts and not in the margins. All submitted
manuscripts are reviewed by the editors and rejected
manuscripts will not be returned. Ethical aspects will
be considered in the assessment of the paper.
Arrangement :
Papers should be divided into: (a) Title page (b)
Summary (c) Introduction (d) Materials and methods
(e) Results (f) Discussion (g) Acknowledgement (h)
Reference (i) Tables (j) Figures and Captions. The
summary should not exceed 250 words and should
state concisely what was done, the main findings and
how the work was interpreted.
Style :
Abbreviations and symbols must be standard and SI
units should be used throughout. Whenever possible
drugs should be given their approved generic name.
Acronyms should be used sparingly. Statistical
analysis must explain the methods used. Reference
should follow the Vancouver format. In the text they
should appear as numbers starting at 1. At the end
of the paper they should be listed (double spaced) in

AZITHROMYCIN VERSUS CIPROFLOXACIN FOR THE
TREATMENT OF UNCOMPLICATED ENTERIC FEVER
IN BANGLADESH - A RANDOMIZED TRIAL
DURBA HALDER1, SAMIR KUMAR KUNDU2, M MATIUR RAHMAN3, M A AZHAR4
Abstract
Objectives: The study was carried out in Sir Salimullah Medical College and Mitford Hospital,
Dhaka, in the last one and half year to see the efficacy of azithromycin in treatment of enteric fever
and to compare the clinical efficacy of azithromycin with ciprofloxacin in enteric fever.
Methods: One hundred and twenty eight patients (> 12 years) admitted for a period of January
2006- June 2007, with symptoms and signs of uncomplicated enteric fever were initially enrolled
for study. They were entered into a randomized trial and were treated with either oral azithromycin
(Igm on the 1st day followed by 500 mg for the next 6 days) or oral ciprofloxacin (500 mg twice daily
for 14 days). Blood culture for Salmonella typhi or Salmonella paratyphi were done in all cases.
Total sixty patients were culture positive for either S. typhi or S. paratyphi which were finally
studied. Out of sixty patients fifty three were culture positive for salmonella typhi and seven were
culture positive for Salmonella paratyph. Multiple drug resistance (MDR: resistance to two or more
antibiotics) was found in more than seventy percent patients.
Results: During the study period out of sixty patients, thirty three were receiving azithromycin and
twenty seven were receiving ciprofloxacin. Clinical cure was achieved in thirty (90.90%) patients in
the azithromycin group and in twenty one (77.78%) patients in the ciprofloxacin group. Mean fever
clearance time in the azithromycin group was 4 ± 1.4 days and was 4 ± 1.55 days for ciprofloxacin
group. There was no significant difference of clinical cure between the two treatment groups (p >
0.05). No clinical relapses were detected in any study subject. No major side effects of both drugs
occurred in any study subject.
Conclusion: These results indicated that azithromycin and ciprofloxacin were effective against
enteric fever caused by both sensitive organisms and MDR S. typhi & S. paratyphi. It is concluded
that azithromycin is effective and can be a convenient alternative for the treatment of enteric fever,
especially in developing countries like us where medical resources are scarce.
1. Registrar, Department of Medicine, Sir Salimullah Medical College, Dhaka.
3. Assistant Registrar, NICVD, Dhaka
2. Associate Professor, Department of Medicine, Sir Salimullah Medical College, Dhaka.
3. Professor. Department of Medicine, Sir Salimullah Medical College, Dhaka
Introduction
Enteric fever (typhoid fever) is an acute systemic
illness caused by bacterium Salmonella typhi, S.
paratyphi A, B, sometimes C and occasionally by S.
typhimurium.
The incidence of enteric fever has declined greatly
with the provision of clean water and good sewage
systems in Europe and the USA since the early 20th
century, but the disease remains a serious public-
health problem in developing countries, including
Bangladesh. Poor water supply and sanitation
systems are responsible for its prevalence throughout
the year, either sporadically or epidemically in
Bangladesh1-3.
It remains an underestimated important health
problem in the developing countries4.
Enteric fever is estimated to have caused 21.6 million
illness and 2,16,500 deaths globally in 2000 affecting
all ages5. There is also one case of paratyphoid fever
for every four of typhoid.
For decades chloramphenicol has been highly effective
against S. typhi and S. paratyphi and it often remained
the antibiotic of choice for the treatment of enteric
fever6-7. In late 1980s and 1990s outbreaks of typhoid
caused by organism resistant to chloramphenicol, co-
trimoxazole, ampicillin, and amoxycillin were
reported8.
MDR strains of Salmonella typhi (resistant to two or
more than two antibiotics) have emerged in many
countries, in many areas of Asia and have
necessitated the search for other therapeutic
options9. In 1992, a study in Bangladesh10 showed
Bangladesh J Medicine 2010; 21 : 7-13

Salmonella were sensitive to ciprofloxacin and to
pefloxacin in 100% cases and to ceftriaxone in 97.54%
cases and sensitivity to amoxycillin, co-trimoxazole
and chloramphenicol were about 50% of cases. This
study showed emergence of multidrug-resistant
enteric fever in Bangladesh with changing antibiotic
sensitivity pattern. Since then, ciprofloxacin or third
generation cephalosporins (namely ceftriaxone) have
become the first line of treatment of enteric fever11.
However, isolates of Salmonella typhi and paratyphi-A
with reduced susceptibility to fluoroquinolones and
also resistant to fluoroquinolones have been reported
in Bangladesh, India, Thailand and Vietnam and
Tajikistan 11-13.
In this situation ceftriaxone, cefixime and other 3rd
generation cephalosporins are still highly effective
against S. typhi but high cost and parenteral
administration associated with ceftriaxone, renders
them impractical for some patients. Furthermore, in
a report from Bangladesh shows isolates of S. typhi
with high level of resistance (MIC > 256.0 ug/ml) to
ceftriaxone14. Reports of infection with MDR and
fluoroquinolone resistant Salmonella species have
raised concern that soon no available oral medication
will exist to treat the infection15-16.
Azithromycin, the first drug of azalide class, has in
vitro activity against many enteric intracellular
pathogens, including S. typhi17-19. Previous studies
done in other countries demonstrated that a seven-
day treatment of azithromycin was highly effective
against uncomplicated enteric fever in adults and
children 20-21.
We therefore, want to make a comparative study of
ciprofloxacin and azithromycin in treating
uncomplicated enteric fever. If azithromycin proves
to be effective in treatment of enteric fever, it could
be a promising alternative antibiotic for treatment of
enteric fever. Since azithromycin is an oral drug,
relatively cheaper, can be given to all age group
including pregnant woman, it will be very useful for
our people, particularly, poor rural community.
Materials and Methods
Patients: This study was conducted at the
department of Medicine, Sir Salimullah Medical
College and Mitford Hospital, Dhaka for a period of
one and half years (from January 2006 to June 2007).
Both males and females over 12 years of age admitted
to this hospital with documented fever (oral
temperature > 38.5°c) plus a history of fever for at
least 4 days in addition to two or more of the following
symptoms: abdominal tenderness, hepatomegaly,
splenomegaly, coated tongue with sparing of margins,
toxic physical appearance, relative bradycardia, rose
spots, were eligible for enrollment in the study. Only
patients with blood culture positive for salmonella typhi
or S. paratyphi were finally evaluated. Patient’s
informed consent was obtained before randomization
of the study drug.
Patients were excluded from the study if any of the
following criteria were present: pregnancy or lactation,
allergy to ciprofloxacin or azithromycin, associated
complications of enteric fever like severe
gastrointestinal bleeding, intestinal perforation,
visible jaundice, myocarditis, pneumonia, renal
failure, shock, or coma etc., where oral medication
was not suitable or inability to swallow oral
medication, and treatment within the past 4 days
with an antibiotic.
Methods: After study eligibility was determined and
informed consent was obtained, patients were
randomized to one of the two treatment groups.
Patients were hospitalized during the entire treatment
period and at admission evaluation was made by
history and physical examination in a structured
format. Culture of blood (15 ml) was performed prior
to initiation of antibiotic therapy. After
randomization, subjects were treated in an open label
format with either azithromycin (1 g given orally on
the 1st day followed by 500 mg given orally once daily
for the next six days) or ciprofloxacin (500 mg given
orally twice daily for fourteen days ). Azithromycin
was given one hour before or two hour after eating
food. Blood were obtained for haematologic
measurements like TC of WBC, Hb, ESR, platelet
count, blood film for malarial parasite and biochemical
measurements like S. bilirubin, AST, serum
creatinine and urine was obtained for urine analysis
before subjects receives a study drug. Chest x-ray
and other radiological investigations including
abdominal ultrasound, were performed as clinically
indicated. Subjects were asked regarding changes in
symptomatology and possible adverse events of the
study drugs like nausea, anorexia, vomiting,
diarrhoea, abdominal pain etc. During hospitalization,
vital signs (including body temperature) were
measured at every 8 hours, and thorough clinical
examination based on a structured format was
performed daily. Patients were discharged from the
hospital after they became afebrile for at least two
days. All patients were asked to return to the hospital
after two weeks and four weeks for follow up or early
if they became sick.
For blood culture 5-8 ml specimen of blood was
inoculated into Bactec 6B aerobic bottles (Becton
Dickinson) and incubated in the Bactec incubator
system. Bottles giving a positive signal were
subcultured onto Macconkey and blood agar.
Nonlactose - fermenting colonies were then
biochemically identified and were typed for Salmonella
O antigen by slide agglutination with specific
antisera. Antimicrobial susceptibilities was
determined by disk diffusion. Strains were considered
susceptible when zone diameters for azithromycin
disks containing 15 ug were > 13 mm and those for
ciprofloxacin disks containing 5 ug were > 21 mm.
8
Azithromycin Versus Ciprofloxacin for the Treatment of Uncomplicated Enteric Fever BJM Vol. 21 No. 1

Responses of patients to treatment were classified
by clinical cure, which was defined as the resolution
of all typhoid related symptoms within seven days of
initiating antibiotic therapy. Clinical failure was
defined as the persistence of > 2 typhoid related
symptoms or signs present at study entry or as the
development of a typhoid related complication.
Clinical improvement was defined as partial resolution
of illness.
Clinical relapse was defined as recurrence of fever
and clinical features of typhoid within thirty days of
completing therapy, along with isolation of S. typhi
from the blood.
Defervescence was defined as the first day on which
the maximum temperature was < 38.0°c with
maintenance of the temperature at this level for at
least 48 hours.
Statistical Analysis: The numerical data obtained
from study were analyzed and significance of difference
was estimated by using the statistical methods. Data
were expressed in frequency, percentage, mean, and
standard deviation as applicable. Comparison between
groups were done by standard ‘t’ test, chi-square test
as applicable. Proportions were compared with the
chi-square test with yates’ correction. Normally
distributed data were compared using the student t
test. Variable with a p value of <0.05 were counted as
significant & p value of > 0.05 were counted as
insignificant. All statistics were calculated with SPSS
software version 11.5.
Results and Observations
During the period from January 2006 to June 2007,
one hundred twenty-eight patients (33 male, 23
females) ranging in age from 12 to 45 years (mean, 20
years) were enrolled in the study and randomly
assigned to one of the two treatment groups. A total
of 60 subjects had blood cultures from which S. typhi
or S. paratyphi was isolated, and these subjects
comprised the basis for analysis.
Among 60 (sixty) patients 33 (thirty three) were
receiving azithromycin and 27 (twenty seven) were
receiving ciprofloxacin. 53 (fifty three) patients grew
S. typhi and 7 (seven) patients grew S. paratyphi from
their blood samples. Demographic and pretreatment
laboratory evaluations of the subjects with positive
blood cultures are shown in Table 1.There were no
significant differences between the treatment groups
(Table-I).
In this study, according to culture report Salmonella
typhi was sensitive to azithromycin in 90% cases and
to ciprofloxacin in 78 % cases. Ceftriaxone was
sensitive to 100% cases. Ampicillin/amoxycillin was
sensitive only in 21% of cases, and co-trimoxazole
was only in 27% cases. Nalidixic acid was resistant
to all cases.
Clinical responses were cures or improvements within
5 days of starting treatment in 90.1% of patients
treated with azithromycin and 77.7% of patients
treated with ciprofloxacin (table-2). In both treatment
groups response to treatment were significant, that
means both the trial drugs were effective in treating
enteric fever. Difference in response to both groups
was statistically insignificant (p > 0.05).
Those patients of azithromycin group, who failed to
respond at day 5 after starting treatment, we
continued the same treatment. 1 patient had clinical
improvement on day 7, but other 2 patients showed
no further improvement. So we switched over the
treatment to inj. ceftriaxone (2 gm/day intravenously
for 10 days). No patients in azithromycin group developed
complication. Among the ciprofloxacin group 6 patients
Table-I
Demographic and pretreatment laboratory evaluations of Azithromycin and Ciprofloxacin Groups
Parameter Azithromycin Ciprofloxacin
No of patients 33 27
Age(yrs) Range 16-45 16-45
Mean + SD 20 + 6.38 24 + 3.87
Sex Male 20 13
Female 13 14
Duration of fever before admission(days)
Mean + SD 8.18 + 4.64 6.70 + 4.30
No. of patients with positive blood culture with S. typhi 30 23
No. of patients with positive blood culture with S. paratyphi 3 4
Laboratory values in Mean + SD
Haemoglobin (g/dl) 11.89 + 1.15 11.73 + 1.17
Total count of WBC (×103/cmm) 6.01 + 1.53 5.52 + 1.19
Platelet count (×103/cmm) 231.36 + 33.37 239.88 + 36.49
Aspertate aminotransferase (IU) 46 + 34 41 + 21
Serum creatinine (mg/dl) 0.75 + 0.12 0.73 + 0.13
9
BJM Vol. 21 No. 1 Azithromycin Versus Ciprofloxacin for the Treatment of Uncomplicated Enteric Fever

had no response at day 5 after starting treatment.
For non responders we continued the same treatment
for another 2 days. Subsequently 2 patients became
afebrile on day 7. Two patients in ciprofloxacin group
developed complication. One patient developed
Intestinal perforation and another patient developed
meningitis. For those patients we switched over the
treatment to inj. ceftriaxone (1 to 2 gm/day
intravenously for 10 days).
Patients in both azithromycin and ciprofloxacin
treatment groups who responded to therapy, the mean
times to defervescence was more or less same ( Table-
2). It was 4 ± 1.4 days for azithromycin group and was
4.1 ± 1.55 days for ciprofloxacin group. Though
percentage of response to treatment was 90.1% for
azithromycin group and 77.8% for ciprofloxacin group
was different, but there was no statistically significant
difference in both treatment groups. There was no
statistically significant difference in fever clearance
time in both treatment groups.
Table-III
Comparison of Adverse Effect of Azithromycin and
Ciprofloxacin Groups of Enteric Fever Patients
Adverse Effects Azithromycin Ciprofloxacin
Group (n=33) Group (n=27)
Vomiting and Nausea 6 7
Diarrhoea g 5
Abdominal Pain 5 5
Anorexia 7 9
Some adverse effects (table-3) of both study drugs,
like vomiting, nausea and anorexia, diarrhoea,
abdominal pain, were reported in both treatment
groups. The adverse effects were not severe and did
not result in change of study medication.
A total 47 of 60 (78%) patients returned for follow up
at 2 weeks and 34 of 60 (57%) patients returned for
follow up at 4 weeks. No patients developed clinical
relapse on follow up. Twenty seven patients were
communicated over telephone at six months after
completion of treatment. but none complained of
development of fever within that period. So it has
been presumed that all of them were healthy.
Discussion
Enteric fever is one of the common health problems
of Bangladesh. Reports of infections with
fluoroquinolone resistant Salmonella species have
raised concern that soon no available oral medication
will exist to treat the infection15-16.
Multi-drug resistant enteric fever is now emerging
throughout the world and more common in Indian
subcontinent including Bangladesh 9, 22. Enough
research work has not been done to find out
alternative antimicrobials for treatment of multi-drug
resistant enteric fever in Bangladesh.
The present study was done to see the efficacy of
azithromycin in treating uncomplicated enteric fever
and it’s comparison with ciprofloxacin. Enteric fever
may occur at any age, but the commonest age is
between 10-30 years 23. In this present study the
age of the patients was between 12-45 years.
Maximum number of patients was in the age group of
18 years. This age group of people goes more outside
home and eats frequent outside foods. That may led
to development of enteric fever due lack of proper
hygiene. This result is comparable to other workers1, 24. This study shows overall preponderance of male
over female (1.2: 1). Similar results were also found
in other studies in Bangladesh and India3,25. The
higher number of cases among male is probably due
to the fact that females are brought less frequently
to hospitals because of various social, financial and
religious bars in our male dominated society and also
due to the fact that male goes outside more, takes
outside food more frequently than female.
All the patients in this study came with fever, and,
the duration of fever varied from 3 days to 3 weeks.
Maximum cases presented in the 2nd week. This is
Table-II
Comparison of Clinical Response of Azithromycin and Ciprofloxacin Groups
Variables Azithromycin Group(n = 33) Ciprofloxacin Group(n = 27)
Patients No. Percentage Patients No. Percentage
(%) (%)
Clinical cure on or or before dav 5 30 90.90 21 77.78
No. of days to defervescence after start 4 ±1.4 4±1.55
of treatment (Mean SD >)
X Value =1.095, P>0.50
10
Azithromycin Versus Ciprofloxacin for the Treatment of Uncomplicated Enteric Fever BJM Vol. 21 No. 1

similar to the findings of another study in Bangladesh,
where 13.1% of patients of enteric fever had presented
during the 1st week of illness2. In this study, according
to culture report Salmonella typhi was sensitive to
azithromycin in 90% cases and to ciprofloxacin in 78
% cases. Ceftriaxone was sensitive to 100% cases.
Ampicillin/amoxycillin was sensitive only in 21% of
cases, co-trimoxazole was only in 27% cases. Nalidixic
acid was resistant to all cases. In a study 10 performed
by Alam et al. in Bangladesh 14 years back Salmonella
were sensitive to ciprofloxacin and pefloxacin in 100%
cases and to ceftriaxone in 97.54% cases and
sensitivity to amoxycillin. co-trimoxazole and
chloramphenicol in about 50% of cases. The present
study and the study of Alam et al in 1992 showed the
emergence of multi drug-resistant enteric fever in
Bangladesh with the changing antibiotic sensitivity
pattern. Since 1992, ciprofloxacin or third generation
cephalosporin (namely ceftriaxone) have become the
first line of treatment of enteric fever 8. But in 1999,
ceftriaxone resistant Salmonella typhi was detected
in Bangladesh 14. Ciprofloxacin resistant enteric fever
was found in the western country in 2001 26.
Ciprofloxacin or multi-drug resistant enteric fever
seems to be on increase particularly in the developing
countries including China, India and Pakistan25,27-30.
In this study comparative randomized trial of
azithromycin and ciprofloxacin for treatment of
enteric fever indicates that the two treatments were
effective and comparable. In azithromycin group 90.1%
patients became clinically cured & in ciprofloxacin
group 77% became clinically cured. In this study both
the drugs were effective and comparable and it took
average 5 days for remission of fever. Only few
differences between the two treatment groups were
observed. Though percentage responded to treatment
were different in azithromycin (90.1%) and
ciprofloxacin (77%) group, but they were statistically
insignificant (p>0.05). Fever clearance time in both
treatment groups was also similar. For azithromycin
group it was 4 ±1.4 days and for ciprofloxacin it was
4.1 ±1.55 days. This differences were also statistically
insignificant. Adverse effects of nausea or vomiting,
lightheadedness, dry throat, etc. were reported
occasionally in the both treatment groups. These
events were mild or moderate and did not result in
interruption of therapy and could be attributed in part
to the enteric infections.
Though there is limitation of frequent culture to
confirm relapse, by doing frequent clinical follow up
it was assumed that in both azithromycin and
ciprofloxacin group there was no relapse.
In the present study the two study drugs were very
different in regard to their administration,
pharmacokinetics, and therapeutic principles.
Azithromycin was given once daily in a dose of 1000
mg at 1st day, then 500 mg daily for next 6 days, where
as ciprofloxacin was given 500 mg twice a day for 14
days. Both drugs penetrate cells effectively, and this
intracellular penetration explains the effective
therapeutic activity against the predominantly
intracellular pathogen S. typhi.
In azithromycin group 15% patients showed moderate
sensitivity in culture sensitivity report. Despite
moderate sensitivity in sensitivity reports those
patients got azithromycin and became cured. On the
other hand in spite of 78% disc sensitivity of
ciprofloxacin, 6 patients among ciprofloxacin groups
(out of 27 patients) were not clinically cured.
Ciprofloxacin in spite of disc sensitivity showed poor
clinical response than azithromycin. This indicates
differences of in vitro & in vivo sensitivity in both
treatment groups.
Another interesting finding was that in vitro
resistance to azithromycin did not correlate well with
it’s in vivo effectiveness against enteric fever. This
is possibly because susceptibility testing is based
on serum drug levels, where as for enteric fever, a
major mechanism of action is thought to be
intracellular killing, in which the azithromycin levels
may be 100-fold greater than serum levels 31-33.
Several studies have demonstrated the effectiveness
of azithromycin for the treatment of uncomplicated
enteric fever in children, adolescents, and adults 20-
21, 33. In each of the studies, clinical and
microbiological cure rates have exceeded 90% without
any serious adverse effects or relapses of enteric
fever. The present study also gives the same type
result.
However complete clinical response at discharge and
no relapse on follow up was considered as cure.
During treatment, at the end of treatment and at
follow-up, blood cultures were not done due to
financial constraints. This is the major limitation of
this study.
The result of this comparative randomized trial of
azithromycin and ciprofloxacin for enteric fever
indicated that the two treatments were effective and
comparable by giving clinical cures and improvements.
A 7 day course of azithromycin is effective against
uncomplicated enteric fever in adults. Cost and
compliance, as well as safety and efficacy, need to be
considered when choosing regimens for treating
enteric fever in countries with limited resources
where the disease is endemic. Ciprofloxacin is
cheaper than azithromycin, but due to emergence of
11
BJM Vol. 21 No. 1 Azithromycin Versus Ciprofloxacin for the Treatment of Uncomplicated Enteric Fever

drug resistance, the optimum ciprofloxacin regimen
for these resistant infections will require an increase
in the dose and possibly also the duration of
treatment. This will increase the cost. Patients with
multi drug resistant enteric fever have been treated
successfully with costly drugs like ceftriaxone,
cefixime, aztreonam,6,33-34. On the other hand
azithromycin is much less expensive than the third
generation cephalosporins. The once daily
administration of azithromycin, with the short
duration of therapy, may improve compliance and also
ease treatment of enteric fever. More over
azithromycin will be cost effective and suitable for
use in areas where medical resources are limited.
Conclusion
In this study, azithromycin appears to be as effective
as ciprofloxacin in treating enteric fever. Further study
with repeated culture facilities to prove both
microbiological as well as clinical cure will be very
much helpful for establishing azithromycin in
treatment of enteric fever and testing whether the
duration of therapy can be further shortened to
minimize costs while maintaining efficacy.
References:
1. Stoll BJ, Glass TI, Banu H, Enteric fever in patients
admitted to a diarrhoeal disease hospital in
Bangladesh. Trans Roy Soc Trop Med Hyg 1983;
77: 548-51.
2. Akbar MS, Khan N, Shaha SK. Evaluation of
chloramphenicol and co-trimoxazole in the
treatment of enteric fever. Bangladesh J
ChildHealth1986:10;11-14.
3. Roy Sk, Speelman P, Butler T, Samir N, Thaman H,
stoll BJ. Diarrhoea associated with typhoid fever. J
Infect Dis 1985; 151: 1138-43.
4. Ivanoff B, Levine MM, Lanbert PH. Vaccination
against Typhoid fever ; present status. Bull. Wd
Helh Org 1994; 72: 957-71.
5. Crump JA, Luby SP, Mintz ED. The global burden
of typhoid fever. Bull World Health Organ 2004;
82: 346-53.
6. Acharya G, Butler T, Ho M, Sharma PR, Tiwari M,
Adhikari RK, Khagda JK , Pathak UN. Treatment
of typhoid fever; randomized trial of a three day
course of ceftriaxone versus a fourteen-day course
of chloramphenicol. Am J Trop Med Hyg 1995;
52:162-5.
7. Islam A, Buttler T, Kabir I, Alam NH. Treatment of
enteric fever with ceftriaxone for 5 days or
Chloramphenicol for 14 days: a randomized clinical
trial. Antimicrob Agents Chemother 1993; 37: 1572-
5.
8. Mirja SH, Beeching NJ, Hart CA, Multi-drug
resistant typhoid; a global problem. J Med Microbial
1996; 44: 317-9.
9. White NJ, Parry CM. The treatment of typhoid fever.
Curr Opin Infect Dis 1996; 9: 298-302.
10. Alam MN, Haq SA, Das KK, Mazid MN, Hasan Z,
Ahsan SA,et al. Multi-drug resistant enteric fever
in Bangladesh. Bangladesh Medical Journal 1992;
3:38-41.
11. Asna SM, Haq JA. Decrease of antibiotic resistance
in salmonella typhi isolated from patients attending
hospitals of Dhaka city over a three year period. Int
J Antimicrob Agents 2000; 16:249-51.
12. Nath, G, Tikko A, Manocha H, Tripathi, AK, Gulati
AK. Drug resistance in Salmonella typhi in north
India with special reference to ciprofloxacin J.
Antimicrob. Chemother, 2000; 46: 149-50.
13. Parry C, Wain J, Chinh NT, Vinh Hand, Farrar JJ.
Quinolone-resistant Salmonella typhi in Vietnam.
1998; Lancet; 351: 1289.
14. Saha SK, Talukdar SY, Islam M. and Saha S., A
highly ceftriaxone resistant Salmonella typhi in
Bangladesh. Pediatr. Infect. Dis. J. 1999; 18: 387.
15. Brown JC, Shanahan PM, Jesudason MV, Thomson
CJ, Amyes SG, Mutation responsible for reduced
susceptibility to 4- Fluoroquinolones in clinical
isolates of multi-drug resistant Salmonella typhi In
India. J. Antimicrob Chemother 1996; 37: 891-900.
16. Brown NM, Millar MR, Frost JA, Rowe B,
Ciprofloxaein resistance in Salmonella paratyphi A.
J Antimicrob Chemother 1994; 33: 1258-9.
17. Jones K, felmingham D, ridgway G. In vitro activity
of azithromycin (cp-62, 993), a novel macrolide,
against enteric pathogens. Drugs Exp Clin Res.
1998; 14: 613-5.
18. Metchock B. In vitro activity of azithromycin
compared with other macrolides and oral antibiotics
against salmonella typhi. J. Antimicrob. Chemother
1990; 25: 29-31.
19. Gordillo ME, Singh KV, Murray BE. In vitro activity
of azithromycin against bacterial enteric
pathogens. Antimicrob. Agents Chemother 1993;
37: 1203-5.
20. Tribble D, Girgis N, Habib N, Butler T. Efficacy of
azithromycin for typhoid fever Clin Infect Dis 1995;
21 : 1045-6.
21. Frenck RWJr, Nakhla I, Sultan Y, et al.
Azithromycin versus ceflriaxone for the treatment
of uncomplicated typhoid fever in children. Clin
Infect Dis. 2000; 31: 1134-8.
22. Singh M. The challenge of Multi-drug resistant
Typhoid fever. Indian Paediatrics 1991; 28: 329-
31.
12
Azithromycin Versus Ciprofloxacin for the Treatment of Uncomplicated Enteric Fever BJM Vol. 21 No. 1

23. Park JE. Typhoid fever. In; Textbook of preventive
and social Medicine. 12th ed. India: Banarashi Das
Bhnot Publishers, 1989: 160-1.
24. Hoffman SL. Typhoid fever In; Haunters Tropical
medicine. Stricland TG (editor) 6th edition.
Philadelphia. W. B. Saunders Company. 1984: 282-
97.
25. Gupta SP, Gupta MS, Bhardwaj S, Chugh TD.
Current clinical patterns of typhoid fever: A
prospective study. J Trop Med Hyg 1985; 88: 377-
81.
26. Threlfall EJ, Ward LR. Decreased susceptibility to
ciprofloxacin in Salmonella enterica serotype typhi,
United Kingdom. Emerg. Infect. Dis. 2001; 7: 448-
50.
27. Wang Fu. Treatment of typhoid fever with loxacin.
J. Antimicrobial Chemotherapy 1989; 23: 785-8.
28. Jesudason MV, Malathy B, John TJ. Trend of
increasing levels of minimum inhibitory
concentrations of ciprofloxacin to salmonella typhi.
Indian J Med Res. 1996; 103: 247-9.
29. Hafiz S, Hamedani P. Enoxacin. In vitro efficacy
and its future therapeutic role in the Pakistan health
care system. Clinical Therapeutic; 1989; 11: 232-
40.
30. Ananda AC, Kataria VK, Singh W, Chatterjee SK.
Epidemic multi-drug resistant enteric fever in
Eastern India (letter). Lancet 1990; 1: 352.
31. Vaudaux BP, Cherpillod J, Dayer P. Concentrations
of azithromycin in tonsilar and /or adenoid tissue
from paediatric patients. J. Antimicrob Chemother
1996; 37: 45-51.
32. Wildfeuer A, Laufen H, Zimmerman T. Distribution
of orally administered azithromycin in various blood
compartments. Int J Clin Pharmacol Ther 1994;
32: 356-60.
33. Wildfeuer A, Laufen H, Zimmermann T. Uptake of
azithromycin by various cells and its intracellular
activity under in vivo conditions. Antimicrob Agents
Chemother 1996; 40: 75-9.
34. Bhutta, ZA, Khan IA, Mollah AM. Therapy of multi-
drug resistant typhoid fever with oral cefixime vs
intravenous ceftriaxone. Pediatr. Infect. Dis. J.
1994; 13: 990-4.
35. Girgis, NI, Sultan Y, Hammad O, Farid Z.
Comparison of the efficacy, safety and cost of
cefixime, ceftriaxone and aztreonam in the treatment
of multidrug resistant Salmonella typhi septicaemia
in children. Paediatr Infect. Dis. J. 1995; 14: 603-
5.
13
BJM Vol. 21 No. 1 Azithromycin Versus Ciprofloxacin for the Treatment of Uncomplicated Enteric Fever

Introduction
Myokymia, a form of involuntary muscular movement,
usually can be visualized on the skin as vermicular
or continuous rippling movements.
The word myokymia was used first more than 100
years ago, when Schultze described continuous, slow,
undulating muscular contractions in small muscles
of hands and feet.1Kny used the term myoclonus
fibrillaris multiplex to describe similar clinical
manifestations.2 For the past century, different
authors applied the term myokymia to different
involuntary muscular movements. Most of them
showed electromyographic (EMG) changes.
Case Report
This 13-year-old girl presented to us with pain in
the left calf muscle for 2 months witch was 1st started
while playing badminton. Initially she was treated
with different NSAIDs in adequate dose without any
significant clinical improvement. For the last 15 days
she also noticed that her calf was progressively
increasing in size and became stiff with excessive
sweating on overlying skin. On query she complaint
of discomfort feeling of left calf muscle for last 5
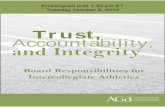
years. On examination her vitals were stable, the
left calf is sweaty, swollen, firm and tender (Fig.-1).
There was frequent rippling movement of the calf
muscles. The other muscles of that limb including
the thigh and leg including knee joint was normal.
Her nervous system examination revealed no
abnormality.
On investigation, CBC was normal. Muscle enzymes
including aminotransferase (SGPT& SGOT),
CALF MUSCLE MYOKYMIA - A BRIEF REVIEWMONZOOR QUADER1, MD ABUL KALAM AZAD2, MD. ABDUR RAHIM3, SYEDUL ISLAM1, AKHTARUL ISLAM
CHOWDHURY1, MOHAMMAD FERDOUS UR RAHAMAN1.
Abstract
Myokymia, a form of involuntary muscular movement, usually can be visualized on the skin as
vermicular or continuous rippling movements in small muscles of hands, limbs, eyes and calf muscles.
Here we present a 13- year-old female who presented with pain and stiffness of left calf muscle for
one month. Her calf muscle was swollen and tender. Muscle enzymes, Electromyography, Nerve
Conduction studies revealed no abnormality. A diagnosis of myokymia of calf muscle was made on
the basis of clinical scenario and exclusion of other relevant diseases and she was on physiotherapy
with partial improvement over a period of 2 months.
Key words: Myokymia
1. Medical Officer, Department of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka.
2. Associate Professor, Department of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka.
3. Professor, Department of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka.
Creatinine kinase and Lactate Dehydrogenase were
normal. S Electrolytes & calcium was also normal.
Thyroid function test was also normal.
USG of the left calf showed oedematous and
thickened both Gastrocnemeus & Soleus. X-ray
chest and X-ray Lumbo-sacral spine was normal. MRI
revealed oedematous and thickened gastrocnemeus
and soleus muscle ( Fig 2a & 2b). Electromyogram
(EMG) & NCV of the left limb was also normal. With
these findings she was diagnosed as myokymia of
the left calf muscle. After counseling the she was
discharged with advice of relevant exercise. On her
follow up after one month, her symptoms partially
subsided.
Fig.-1: Calf hypertrophy on left side
Bangladesh J Medicine 2010; 21 : 46-48
CASE REPORTS

Discussion
Myokymia may present with
• Pain, cramps, spasms, weakness, stiffness, or
twitching of affected muscles.
• Sensory symptoms are reported rarely, unless the
underlying etiology (ies) includes sensory nerve
involvement.
• Typical myokymic discharges also can be seen in
the EMGs of patients referred for totally unrelated
complaints.
Physical
Findings of facial myokymia, segmental or focal
myokymia in other areas of the body, and generalized
myokymia are somewhat different in physical
examination and in their potential etiologies;
therefore, they are discussed separately.
• Facial myokymia
o Affected muscles show slow, undulating, fine
movements on the surface of the skin due to
activation of the most superficial muscle
layers. Facial weakness can be present in the
involved muscles.
o EMG study shows typical myokymic
discharges of spontaneous, rhythmic/
semirhythmic bursts of normal-appearing
potentials of 30-60 Hz. The bursts of each
group of potentials are followed by a period
of silence, with subsequent repetition of
grouped discharges of identical potentials.
The spontaneous activities are not altered
by voluntary activation of the muscles.
• Focal or segmental myokymia
o These types of myokymia commonly are seen
in the limbs or particular segmental level(s).
Physical findings mostly are related to the
underlying etiology(ies), which is usually
asymptomatic and not a major concern of the
patient.
o EMG study shows myokymic discharges
similar to those recorded in facial myokymia.
• Generalized myokymia
o A triad of myokymia, muscular stiffness, and
decreased deep tendon reflexes was first
described by Isaacs in 1961; it also is called
Isaacs syndrome.4
¶ Muscle weakness and atrophy and
excessive sweating are frequently
associated features. Smooth muscles
and cardiac muscles typically are spared.
¶ Sensory symptoms are rarely present.
¶ The muscular stiffness is different than
that seen in myotonia, both clinically and
electrodiagnostically. Although both can
be exacerbated by cold, myokymia can be
detected when the muscle is at rest and
during sleep. Patients with myotonia are
normal at rest; the stiffness is induced
by mechanical stimulation.
o The myotonic discharge recorded by EMG
ceases upon relaxation of the muscle, while
spontaneous grouped discharges of myokymia
persist for some time, well above the
abnormal pattern that was present before the
voluntary contraction.
Fig 2a: Oedematous and thickened gastrocnemeus and
soleus muscle (Coronal segment)
Fig 2b: Oedematous and thickened gastrocnemeus and
soleus muscle ( Cross section)
47
BJM Vol. 21 No. 1 Calf Muscle Myokymia - A Brief Review

¶ The EMG features encountered in
patients with generalized myokymia
include the previously described typical
myokymic discharge or neuromyotonia,
which has a much higher frequency of
discharges (up to 300 Hz).
¶ Generalized myokymia in other clinical
entities shares less consistent clinical
manifestations.
Causes
• Facial myokymia
o This type of myokymia is seen more commonly
than other types.
o Facial myokymia has been reported to be
associated with inflammatory demyelinating
diseases, brainstem neoplasms, Guillain-
Barré syndrome, or other intramedullary
pontine lesions. Facial myokymia also has
been reported in patients with history of
radiotherapy, with findings similar to those
of more common brachial or lumbar radiation
plexopathies.
• Focal or segmental myokymia
o The majority of patients with a history of
radiation therapy have myokymic discharges
detected within the field of radiation.
Metastatic lesions generally are believed to
be less likely to generate myokymia. The
amount of radiation ranges widely, though
myokymia rarely is reported with radiation
doses less than 10 gray (Gy).
o Electrodiagnostic findings are usually
consistent with plexopathy. Other less
common causes include acute or chronic
inflammatory polyradiculoneuropathy5 (with
or without coexistent systemic vasculitis),
ischemic or traumatic focal neuropathy, and
entrapment neuropathy, polyradiculopathy
secondary to torticollis, syringomyelia, and
chronic idiopathic plexopathy.
o Transient myokymia, described in the calf or
hand muscles, was reported after brief
strenuous exercise. It usually resolves
spontaneously over weeks to months
TREATMENT: Most of the cases do not require
treatment. It will get better within weeks to months.
But if the symptom persists or intolerable then we
can add one of the following, Beta blockers,
Carbamazepine, Gabapentine or Baclofen.
Consent
Written informed consent was obtained from the
patient for publication of this case report and
accompanying images. A copy of the written consent
is available for review by the Editor-in-Chief of this
journal.
Competing Interest
The authors declare that they do not have any
competing interests.
References
1. Jorge C, Kattah MD. Superior oblique myokymia.
Curr Neurol Neurosci Rep 2003; 3: 395–400.
2. Duane A. Unilateral rotary nystagmus. Am Ophthal
Soc 1976; 11: 63–67.
3. Webster R. Recurrent superior oblique myokymia in
a patient with retinitis pigmentosa. Clin Exp Optom
2004; 87(2): 107–109.
4. Lee JP. Superior oblique myokymia. A possible
etiologic factor. Arch Ophthalmol 1984; 102: 1178–
79.
5. Hoyt WF, Keane JR. Superior oblique myokymia:
report and discussion on five case of benign
intermittent uniocular microtremor. Arch
Ophthalmol 1970; 84: 461–67.
6. Brazis PW. The natural history and results of
treatment of superior oblique myokymia. Arch
Ophthalmol 1994; 112: 1063–67.
7. Leigh JR, Tomsak RL, Seidman SH, Dell ‘Ossolf.
Superior oblique myokymia. Arch Ophthalmol 1991;
109: 1710–13.
48
BJM Vol. 21 No. 1 Calf Muscle Myokymia - A Brief Review

Introduction
Primary Hyperparathyroidism (PHPT) is an
unstimulated and inappropriately high secretion of
parathyroid hormone for the concentration of plasma
ionized calcium. Primary hyperparathyroidism is
estimated to be prevalent in approximately 1% of adult
population and the usual causes are parathyroid
adenoma, hyperplasia and, rarely, parathyroid
carcinoma. The diagnosis of PHPT is a rarity in
developing countries probably because of the difficulty
of making a diagnosis in an environment where there
are limited facilities for serum calcium estimation,
parathyroid hormone assay and parathyroid gland
imaging. The diagnosis can be very perplexing
especially because the expected hypercalcaemia
associated with PHPT may be masked by calcium,
protein or vitamin D deficiency. It is a case report of
PHPT presenting with severe respiratory distress, due
to chest wall deformity, fever, multiple fractures in
different long and short bones with pneumonia
secondary to parathyroid adenoma.
Case Report
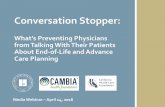
A 26-year-old male hailing from Patuakhali presented
to us with weakness, tingling and numbness of the
limbs for the last 6 years, gradually developing deformity
of chest wall with shortness of breath for 15 months,
decreasing in height for the same duration, unable to
walk for the last 2 months. This young man presented
with weakness of the limbs for the last 6 years. At first
there was proximal muscle weakness, later it became
CHEST WALL DEFORMITY WITH SEVERE
RESPIRATORY DISTRESS- A RARE PRESENTATION OF
PARATHYROID ADENOMA
A K M MOTIUR RAHMAN BHUIYAN1, MONZOOR QUADER2, NIZAM UDDIN AHMED2, MOHAMMAD ABUL
KALAM AZAD2, MD ZILAN MIAH SARKER3, MOHAMMAD MOBAROCK HOSSAIN4
Abstract
Primary hyperparathyroidism is a generalized disorder of calcium, phosphate, and bone metabolism
due to an increased secretion of PTH. The elevation of circulating hormone usually leads to
hypercalcemia and hypophosphatemia. There is great variation in the manifestations. Patients may
present with multiple signs and symptoms, including recurrent nephrolithiasis, peptic ulcers, mental
changes and extensive bone resorption. We present a 26 year old young man of Primary
Hyperthyroidism due to adenoma with severe respiratory distress due to chest wall deformity as a
result of multiple vertebrae and rib fracture. His diagnosis was confirmed by Imaging and FNAC. He
was referred to surgery department but due to poor respiratory and cardiac reserve and also fragile
mandible he was repeatedly refused in preanesthetic check up.
1. Assistant Professor, Department of Medicine, BSMMU.
2. Medical Officer, Department of Medicine, BSMMU.
3. Professor, Department of Medicine, BSMMU.
4. Resident, Department of Cardiology, BSMMU
Fig 1: Severe chest deformity
Bangladesh J Medicine 2010; 21 : 49-52

Investigation shows, Hb: 10.8gm/dl, ESR: 100 mm in
1st hour. Total count 8000/cmm.Thyroid Function test,
TSH 1.92mIU/L, FT4:8.94pmol/L, FT3:2.28pmol/L, S
Creatinine: 0.9mg/dl, S Alkaline Phosphatase: 1703
U/L, Serum corrected Calcium: 15.7mg/dl, S Inorganic
Phosphate: 3.5 mg/dl, S PTH: more than 2500pg/ml,
S Electrolytes and S urea in normal.
X-Ray Skull, hands, pelvis, both knees: Diffuse
Osteopenia with absorption of distal phalanx in both
hands. Bones of the pelvic cavity with thoracic cavity
are deformed. Kyphoscoliosis with reduction of body
height of dorsal vertebrae at different level is seen.
All skeletal survey is competitive with
Hyperparathyroidism.
SG of thyroid: A mixed echogenic area having
internal calcification is noted within the both
parathyroid gland, right one is measuring about 15x13
mm and left one is measuring about 38x22 mm. Both
are suggestive of parathyroid mass. FNAC of
parathyroid mass: Smear show mostly chief cells
and cell with abundant eosinophilic cytoplasm
arranged in clusters and small round nuclei
suggestive of parathyroid adenoma. Spirometry:
Severe restrictive airway disease. Echocardiography:
within normal limit. Parathyroid Scintigraphy:
Suggests suspected case of intrathyroidal parathyroid
adenoma.
Table-I
Laboratory data of patient with their related normal
range
Laboratory variables Patient’s Normal
value Value
S Calcium mg/dl 15.7 8.6-10.8
S Phosphate mg/dl 03.5 2.5-5.0
S Alkaline Phosphatase U/L 1703 100-290
S PTH pg/ml >2500 10-60
Fig.-2: Generalized wasting
generalized. Now he is unable to walk and cannot do
his daily activities. He had multiple low trauma fractures
which healed spontaneously. Now for the last 15
months his height is decreased which is due to multiple
vertebral fracture. He also developed severe shortness
of breath due to chest wall deformity. He had
kyphoscoliosis with fracture of multiple ribs and clavicle.
Other systemic examination including cardiovascular,
respiratory and abdomen revealed no abnormality.
Fig.-3: CXR: Suggestive of old healed pulmonary
inflammatory lesion, old healed fracture of multiple ribs
with chest deformity
Fig.-4: X-ray right knee and elbow joint: severe bone
resorption with fracture
50
Chest Wall Deformity with Severe Respiratory Distress BJM Vol. 21 No. 1

After the investigations we have diagnosed him as a
case of primary hyperparathyroidism. We have treated
him with optimum medical management by
consultation with endocrinologist and latter referred
him to endocrine surgery wing of surgery department
of BSMMU. Who agreed for the surgical removal of
the adenoma. But due to poor respiratory and cardiac
reserve and also fragile mandible and chest he was
repeatedly refused in the preanaesthetic checkup.
So he was discharged with adequate medical
management and return after improvement of general
condition for anaesthesia fitness and adenoma
removal.
Discussion
Primary hyperparathyroidism (PHPT) is a disease
commonly due to solitary parathyroid adenoma. It
was considered rare in developing countries but
recent experience has shown that its apparent rarity
may be due to paucity of reports from these countries
and also to limited diagnostic facilities. Our case
has shown that with adequate facilities, more reports
of the disease may soon be emanating from
developing countries. Primary hyperparathyroidism
(PHPT) has protean manifestations. The advent of
automated serum biochemical analysis has highly
augmented its diagnosis. The incidence of metabolic
bone disease in patients with PHPT in developing
countries is very high. The reasons for this are the
high prevalence of protein, vitamin D and dietary
calcium deficiencies and the high dietary phytate
and phosphates in some cultures. It is therefore
pertinent for clinicians practicing in the developing
countries to note that nutritional deficiencies can
be seen in their patients, unlike those from the
developed nations, making hypercalcaemia irrelevant
in the diagnosis of PHPT.
Severe respiratory distress with chest wall deformity
although uncommon, they suggest a late presentation
of the disease and the severity of the disease.
Parathyroidectomy is the treatment of choice in
PHPT. Success of the surgery is determined largely
by early diagnosis and localization of the adenoma
before surgery.
Parathyroidectomy is indicated in patients who meet
some of the following criteria:1. Age <50 years; 2.
Serum Calcium concentrations>1mg/dl above the
upper limit of normal;3. 24 hr urinary calcium
>400mg;4. Creatinine clearance reduced by 30%; 5.
Reduced bone mineral density(BMD; T score<-2.5) at
any site. Open parathyroidectomy is the treatment
of choice in PHPT.
References
1. Fauci A S, Braunwald E L, Kasper D, and Hauser S.
Harrsion’s Principles of Internal Medicine, vol.
2,McGraw-Hill, New York, NY, USA, 2008.
2. Goldman L and Ausiello D A, Cecil medicine,
Sunders- Elsevier, 23rd edition, 2007.
3. Burney E R, R. Jones K, Peterson K et al., “Surgical
correction of primary hyperparathyroidism improves
quality of life,” Surgery, vol. 124, no. 6, pp. 987–
992, 1998.
4 Cummings W C, Otolaryngology, Head and Neck
Surgery, vol. 3, Mosby, St. Louis, Miss, USA, 2005.
5. Morgan GM, Ganapathi SA, Grant AJ, “Pathological
fractures in primary hyperparathyroidism: a case
report highlighting diagnostic difficulties,” Injury
2002; 33 (3): 288–291.
6. Hamidi S, Hedayat SA, Kamalian N. “Primary
hyperparathyroidism: a review of 177 cases,” Medical
Science Monitor 2006; 12 (2): CR86–CR89.
7. Burney, Jones K R, Christy B, and N. W. Thompson
NW. “Health status improvement after surgical
correction of primary hyperparathyroidism in
patients with high and low preoperative calcium
levels”. Surger 1999; 125(6): 608– 614.
8. Jonard S, Gauthier-Morgenstern M, Douillard C et
al., “Vitamin D deficiency and severe
hyperparathyroidism,” Annales d’Endocrinologie
2002; 63( 61): 540–546.
9. Kumar A, Kumar S, Aggarwal S, Kumar R, Tandon
N, “Thoracoscopy: the preferred method for excision
of mediastinal parathyroids,” Surgical Laparoscopy,
Endoscopy and Percutaneous Techniques 2002; 12
(4): 295–300.
10. Pattou F, Huglo D, Proye C, “Radionuclide scanning
in parathyroid diseases,” British J Surgery 1998;. 85
(12): 1605–1616.
Fig.-5: Parathyroid scintigraphy showing Adenoma
51
BJM Vol. 21 No. 1 Chest Wall Deformity with Severe Respiratory Distress

11. Alvarado R, Meyer-Rochow G, Sywak M, Delbridge
L, Sidhu S, “Bilateral internal jugular venous
sampling for parathyroid hormone determination in
patients with nonlocalizing primary
hyperparathyroidism,” World J Surg 2010; 1 34: (6):
1299–1303.
12 Patel C N, Salahudeen H M, Lansdown M,
Scarsbrook A F, “Clinical utility of ultrasound and
Tc sestamibi 4 Case Reports in Medicine SPECT/
CT for preoperative localization of parathyroid
adenoma in patients with primary
hyperparathyroidism,” Clin Radiol 2010; 65 (4), 278–
287.
13. Su A W, Chen C F, Huang C K. Chen PCH, Chen
WM, Chen TH, “Primary hyperparathyroidism with
brown tumor mimicking metastatic bone
malignancy,” J Chinese Medical Association 2010;
73(3): 177–180.
14. Res´endiz-Colosia J A, Alvarado-Cabrero I, Flores-
D´ýaz R et al., “Multiple maxillofacial brown tumors
as primary hyperparathyroidism manifestation,”
Gaceta Medica de Mexico 2008; 144 (2) 155–160.
15. Lanitis S, Sivakumar S, Zaman N, Westerland O,
Al Mufti R, Hadjiminas D J, “Recurrent acute
pancreatitis as the first and sole presentation of
undiagnosed primary hyperparathyroidism,” Ann
Royal Coll Surg England 2010; 92 (2): W29–W31.
16. Siddiqui F, Weissman DE. “Hypercalcemia of
malignancy #151.” J Palliative Med 2010; 13 (1); 77–
78.
17. Berger AD, Wu WB, Eisner H, Cooperberg MR, Duh
QY, Stoller ML. “Patients With Primary
Hyperparathyroidism—why do some form stones?”
J Urology 2009; 181 (5): 2141–2145.
18 Suh JM, Cronan JJ, Monchik JM. “Primary
hyperparathyroidism: is there an increased
prevalence of renal stone disease?” Am J Roentgen
2008; 191 (3); 908–911.
19. Vander Walde LH, Liu ILA, Haigh PI. “Effect of bone
mineral density and parathyroidectomy on fracture
risk in primary hyperparathyroidism,” World J Surg
2009; 33 (3): 406–411.
20. VanderWalde LH, Liu IL, O’Connell TX, Haigh PI.
“The effect of parathyroidectomy on bone fracture
risk in patients with primary hyperparathyroidism,”
Archives of Surg 2006; 141(9): 885–89.
21. Wu B, Haigh PI, Hwang R et al. “Underutilization of
parathyroidectomy in elderly patients with
primaryhyperparathyroidism,” J Clin Endocrinol
Metabolism 2010; 95(9), 4324–30.
52
Chest Wall Deformity with Severe Respiratory Distress BJM Vol. 21 No. 1

Introduction
Seborrheic dermatitis, also known as seborrheic
eczema, is a chronic papulo-squamous dermatosis
that is associated with increased sebum production
(seborrhea) of the scalp and the sebaceous follicle -
rich areas of the face and trunk.1 Seborrheic dermatitis
is a common disease and occurring in 2% to 5% of the
population. Dandruff, the mildest form of seborrheic
dermatitis, is probably far more common and is present
in an estimated 15-20% of the population. Seborrheic
dermatitis is more common in patients with
Parkinson’s disease or mood disorders and those with
HIV/ AIDS than in the general population. The
prevalence of seborrheic dermatitis among HIV-positive
and AIDS patients between 34% and 83%. The disease
is characterized by scaling on an erythematous base.
Itching may be severe. In extreme cases a greasy, dirty
crust with an offensive odor covers the entire scalp.
The lesions may also become generalized and progress
to a generalized exfoliative erythroderma (erythroderma
desquamativum).2 The cause of seborrheic dermatitis
CLINICO-EPIDEMIOLOGICAL PROFILE OF
SEBORRHEIC DERMATITIS
LUBNA KHONDKER1, MD ABDUL WAHAB2, MD SHIRAJUL ISLAM KHAN3
Abstract
A cross sectional study was carried out with total one hundred thirty seven patients of seborrheic
dermatitis for a period of total two years from department of Dermatology and Venereology,
Bangabandhu Sheikh Mujib Medical University (BSMMU) Dhaka, Bangladesh to assess the clinico-
epidemiological profile of seborrheic dermatitis. The mean age of the patients was 36±6.6 years and
among the patients, highest percentage of patients, 88(64.2%) were in between the 31-40 years
old, 71(51.8%) had higher secondary level of education, 79(57.7%) had monthly family income
>10,000 taka, 124(90.5%) were married, 79(57.7%) were male and 58(42.30%) were involve in
business. It was observed that 88(64.2%) had complaints of itching, followed by 79(57.7%) had
complaints of greasy crust and 58(42.3%) had complaints of seborrhea. It was seen that maximum
48(35.0%) had been suffering for less than 1 year of duration and 88(64.2%) had involvement of
scalp, followed by eyebrow 37(27%) and other areas. It was observed that erythema was mild in
58(42.3%) cases; moderate in 31(22.6%) cases, severe in 27(19.7%) cases and 21(15.3%) had no
erythema. It was showed that 77(56.2) % had mild type papular eruption, 16(11.7) had moderate
and 7(5.1) had severe papular eruption and 37(27.0) had no papular eruption and it was observed
that squamation was mild in 74(54.0) cases, moderate in 43(31.4) cases, and severe in 20(14.0)
cases. It was showed that 58(42.3%) had no associated disease but 37(27.0) had pityriasis versicolor,
20(14.0) had acne vulgaris, 16(11.7%) had neurological disorder and some other disease associated
with seborrheic dermatitis.
Key words: Seborrheic dermatitis, clinical profile, epidemiological profile.
1. Specialist in Dermatology and Venereology, Bangabandhu Sheikh Mujib Medical University (BSMMU),
Shahbag, Dhaka, Bangladesh.
2. Associate Professor, Department of Dermatology and Venereology, BSMMU
3. Specialist in Dermatology and Venereology, Combined Military hospital (CMH), Dhaka cantonment, Dhaka,
Bangladesh.
is unknown; Immunological, nutritional,
environmental and lifestyle factors that might increase
the predisposition to seborrheic dermatitis. There may
also be a hormonal influence, not only those the
disease begin to develop at puberty, but seborrheic
dermatitis is more common in men than in women,
suggesting an influence of androgens on the
pilosebaceous unit. Seborrheic dermatitis is also
associated with chronic alcoholic pancreatitis,
hepatitis C virus and various cancers.3. Arsenic, gold,
methyldopa, cimetidine, and narcoleptics drugs; post
encephalitic parkinsonism, epilepsy, poliomyelitis,
syringomyelia, biotin deficiency and abnormal
metabolism of essential fatty acids have been proposed
as possible mechanisms. 1 Seborrheic dermatitis may
be coincident with other dermatological disorders, e.g.
rosacea, ocular irritation or blepharitis. Diseases
associated with Malassezia spp. are also commonly
found in patients with seborrheic dermatitis, these
include pityriasis versicolor and pityrosporum
folliculitis. Seborrheic dermatitis in HIV-positive and
Bangladesh J Medicine 2010; 21 : 25-28

AIDS patients is more severe than the usual immune
deficiencies.4 Patients with seborrhoeic dermatitis may
show up regulation of interferon (IFN)-g, expressed
interleukin (IL)-6, expressed-IL-1a, and IL-4.
Expressions of cytotoxicity activating ligands and
recruitment of natural killer (NK) cells have also been
noted.2 Unfortunately there is no data base study with
the profile of disease over Bangladeshi people. Limited
information is available regarding this. The present
study was designed to assess the profile of seborrheic
dermatitis.
Materials and Methods
This was a cross sectional study, carried out for a
period of total two years from January 2008 to December
2009. Total one hundred thirty seven patients of
seborrheic dermatitis were subjected purposively from
department of Dermatology and Venereology,
Bangabandhu Sheikh Mujib Medical University
(BSMMU), Dhaka, Bangladesh. Purposive type non-
probability sampling technique was followed in this
study. Questionnaire was developed for collection of
relevant information. By face to face interview and also
from clinical record data were collected from patient.
The patient of seborrheic dermatitis was identified first
and verbal and written consent was taken from
patients. Then clinical conditions of the patient were
recorded by us. After collection of data, all the data
were analyzed by software SPSS (Statistical Package
for Social Science) method.
Results
Total one hundred thirty seven patients were studied
for a period of total two years. The mean age of the
patients in table-I was 36±6.6 years and their highest
percentage of patients, 88(64.2%) were in between
the 31-40 years old, followed by 20(14%) were 21 to
30 years old, 16(11.7%) were 41-50 years old, 7(5.1%)
were 51-60 years old and 6(16.2%) were in between
the 11-20 years old. It was found that 15(10.9%) had
primary level of education, 27(19.7%) had secondary
level of education, 71(51.8%) had higher secondary
level of education, 21(15.3%) had graduation level of
education and 3(2.2%) were illiterate. Among the
patients, more than half the patients 79(57.7%) had
monthly family income >10,000 taka and 37(27%) had
monthly family income 6000 to10, 000 taka and
21(15.3%) had monthly family income 1000 to 5000
taka. The mean monthly family income was 10,432.43
taka with standard deviation of 4,186.88 taka and it
was observed that 124(90.5%) were married and only
13(9.5%) were unmarried. It was found from figure I
that majority of patients 79(57.7%) were male and
58(42.3%) were female. Figure II showed that majority
of the patients 58(42.30%) were involve in business
and 21(15.30%) were house wife, 27(19.70%) were
service holder, 20(14%) were student and 11(8%) were
engaged in other types of occupation. The table II
observed that 88(64.2%) had complaints of itching,
followed by 79(57.7%) had complaints of greasy crust
and 58(42.3%) had complaints of seborrhea. Among
the 137 patients, 48(35.0%) had been suffering for
less than 1 years of duration, 31(22.6%) had been
suffering for 1 to 5 years of duration, 37(27%) had
been suffering from 6 to 10 years and 21(15.3%)
patient had been sufferings for more than 10 years.
Regarding site of the lesion, maximum 88(64.2%) had
involvement of scalp, followed by face 37(27%), trunk
21(15.3%), creases (naso-labial, submammary, axilla,
groin and gluteal creases) 20(14%), ear 16(11.7%), and
involvement of other area were 15(10.9%). Table III
showed that erythema was mild in 58(42.3%) cases,
moderate in 31(22.6%) cases, severe in 27(19.7%)
cases and 21(15.3) had no erythema. It was observed
that 77(56.2%) had mild type papular eruption,
16(11.75) had moderate and 7(5.1%) had severe
papular eruption and 37(27.0%) had no papular
eruption. Regarding grading of squamation of the
patients, it was observed that squamation was mild
in 74(54.0%) cases, moderate in 43(31.4%) cases, and
severe in 20(14.0%) cases. Table IV showed the
distribution of patients by associated diseases and
it was observed that 58(42.3%) had no associated
disease but 37(27.0) had pityriasis versicolor, 20(14.0)
had acne vulgaris, 16(11.7%) had neurological disorder,
3(2.2%) had rosacea, 2(1.4%) had psychiatric disorder
and 1(0.7%) had HIV infection.
Table I
Distribution of the patient by epidemiological profile
(n=137)
Epidemiological profile Frequency
Age(in years)
11-20 6(4.4%)
21-30 20(14.0)
31-40 88(64.2)
41-50 16(11.7)
51-60 7(5.1)
Level of educational
Primary level 15(10.9)
Secondary level 27(19.7)
Higher Secondary level 71(51.8)
Graduate and above 21(15.3)
Illiterate 3(2.2)
Monthly income
1000-5000 21(15.3)
6000-10000 37(27.0)
>10000 79(57.7)
Marital status
Married 124(90.5%)
Unmarried 13(9.5%)
26
Clinico-Epidemiological Profile of Seborrheic Dermatitis BJM Vol. 21 No. 1

Table II
Distribution of the patient by complaints, duration of
lesions and site of lesions (n=137).
Parameters Frequency
Complaints
Itching 88(64.2%)
Greasy crust 79(57.7%)
Seborrhoea 58(42.3%)
Duration of lesion
Less than 1 year 48(35.0%)
1 to 5 years 31(22.6%)
6 to 10 years 37(27.0%)
More than 10 years 21(15.3%)
Site of lesion
Scalp 88(64.2%)
Face (eyebrow, eyelid etc) 37(27%)
Trunk 21(15.3%)
Creases area 20(14%)
Ear 16(11.7%)
Others 15(10.9%)
Table III
Distribution of patients by clinical findings (n=137).
Clinical findings Frequency
Erythema
Normal 21(15.3%)
Mild 58(42.3%)
Moderate 31(22.6%)
Severe 27(19.7%)
Papular eruption
Normal 37(27.0%)
Mild 77(56.2%)
Moderate 16(11.7%)
Severe 7(5.1%)
Squamation
Normal 0(00%)
Mild 74(54.0%)
Moderate 43(31.4%)
Severe 20(14.0%)
Table IV
Distribution of patients of seborrheic dermatitis by
associated diseases (n=137)
Associated diseases Frequency
No 58(42.3%)
Pityriasis versicolor 37(27.0)
Acne vulgaris 20(14.0)
Neurological disorder 16(11.7%)
Rosacea 3(2.2%)
Psychiatric disorder 2(1.4%)
HIV infection 1(0.7%)
Discussion
Total one hundred thirty seven patients were enrolled.
The mean age of the patients was 36±6.6 years and
their highest percentage of patients, 88(64.2%) were
in between the 31-40 years old, followed by 20(14%)
were 21 to 30 years old, 16(11.7%) were 41-50 years
old, 7(5.1%) were 51-60 years old and 6(16.2%) were
in between the 11-20 years old, similar to the study
finding of Baysal et al where thirty two adult patients
with seborrheic dermatitis were recruited for the study
with mean age 33.31±9.03 years and age ranged from
18-57 years.6 It was found that majority of patients
79(57.7%) were male and 58(42.3%) were female,
similar to the study finding of Baysal et al where
Fig.-I: Distribution of the patient by sex.
Fig.-2: Distribution of the patient by occupation.
27
BJM Vol. 21 No. 1 Clinico-Epidemiological Profile of Seborrheic Dermatitis

among thirty two adult patients 19(59.4%) were male
and 13(40.6%) were female and also similar to the
study finding of Koca et al where among eighty four
adult patients 52(61.9%) were male and 32(38.1%)
were female.6,7
It was observed that 88(64.2%) had complaints of
itching, followed by 79(57.7%) had complaints of greasy
crust and 58(42.3%) had complaints of seborrhea and
regarding site of the lesion, maximum 88(64.2%) had
involvement of scalp, followed by face 37(27%) and
trunk 21(15.3%), similar finding observed by Freedberg
and James.1,2 Table III showed that erythema was
mild in 58(42.3%) cases, moderate in 31(22.6%) cases,
severe in 27(19.7%) cases and 21(15.3) had no
erythema. It was observed that 77(56.2%) had mild
type papular eruption, 16(11.75) had moderate and
7(5.1%) had severe papular eruption and 37(27.0%)
had no papular eruption. Regarding grading of
squamation of the patients, it was observed that
squamation was mild in 74(54.0%) cases, moderate
in 43(31.4%) cases, and severe in 20(14.0%) cases,
similar finding observed by Freedberg.1 It was
observed that 58(42.3%) had no associated disease
but 37(27.0) had pityriasis versicolor, 20(14.0) had
acne vulgaris, 16(11.7%) had neurological disorder,
3(2.2%) had rosacea, 2(1.4%) had psychiatric disorder
and 1(0.7%) had HIV infection, similar finding observed
by Gupta et al, where seborrheic dermatitis were
associated with rosacea and acne vulgaris.8
Conclusion
The study revealed that majority of patients of
seborrheic dermatitis were within the thirty one to
forty years old, higher secondary level of education,
monthly family income more than ten thousand taka,
married, male and engaged in business mainly. Among
the patients, most patients had itching and greasy
crust than seborrhea, duration of lesion mainly less
than one year, involve mainly scalp and then face
and trunk. It was observed that majority of patients
had mild type erythema, papular eruption and
squamation and associated with pityriasis versicolor
and acne vulgaris mainly.
References:
1. Freedberg IM, Eisen AZ, Wolff K, Austen KF,
Goldsmith LA and Katz SI. Fitzpatrick’s Dermatology
in General Medicine. 6th edition. The McGraw- Hill
Companies; 2003:1198-1204.
2. James WD, Berger TG and Elston D. Andrews’
Diseases of the skin- Clinical Dermatology. 10th
edition. Saunders Elsevier; 2006:191-192.
3. Gupta AK, Bluhm R. Seborrheic dermatitis. J
European Academy Dermatol Venereol 2004; 18: 13-
26.
4. Dunic I, Vesic S, Jevtovic DJ. Oral candidiasis and
seborrheic dermatitis in HIV infected patients on
highly active antiretroviral therapy. HIV Med. 2004
Jan; 5(1): 50-54.
5. Kose O, Erbil H, Gur AR. Oral itraconazole for the
treatment of Seborrheic dermatitis: an open,
non-comparative trial. J Europ Academy Dermatol
Venereol (JEADV) 2008; 19(2): 172-175.
6. Baysal V, Yildirim M, Ozcanli C and Ceyhan M.
Itraconazole for the treatment of Seborrheic
dermatitis: a new treatment modality. Intern Society
Dermatol Int J Dermatol 2004; 43:63-66.
7. Koca R, Altinyazar HC, Esturk E. Is topical
metronidazole effective in seborrheic dermatitis?
Adouble blind study. Int J Dermatol. 2003 Aug; 42(8):
632-5
8. Gupta AK, Bluhm R, Cooper EA, Summerbell RC,
Batra R. Seborrheic dermatitis. Dermatol Clin. 2003
Jul; 21(3): 401-412.
9. Hay RJ, Graham-Brown RA.” Dandruff and
seborrhoeic dermatitis: causes and management “.
Clin Experiment Dermatol 1997 ; 22 (1): 3–6
10. Janniger CK, Schwartz RA. “Seborrheic dermatitis”.
Am Family Physician 1995; 52 (1): 149–55, 159–
60.
11. Nowicki R. “Modern management of dandruff “(in
Polish). Polski Merkuriusz Lekarski 2006 Jan; 20
(115): 121–4.
12. Parry ME, Sharpe GR. “Seborrhoeic dermatitis is
not caused by an altered immune response to
Malassezia yeast”. British J Dermatol 1998 Aug; 139
(2): 254–63.
13. Schwartz RA, Janusz CA, Janniger CK. “Seborrheic
dermatitis: an overview”. Am Family Physician
2006 July ; 74 (1): 125–30.
14. Schwartz JR, Rocchetta H, Asawanonda P, Luo F,
Thomas JH. Does tachyphylaxis occur in long-
term management of scalp seborrheic dermatitis with
pyrithione zinc-based treatments? Int J
Dermatol 2009; 48(1):79-85.
15. Wolverton SE. Comprehensive Dermatologic Drug
Therapy. W. B. Saunders Company; 2001: 62-66.
16. Johnson BA and Nunley JR. Treatment of Seborrheic
dermatitis. Am Academy Family Physicians 2000;
61:2703-10.
17. Elish D, Silverberg NB. Infantile seborrheic
dermatitis. Cutis 2006; 77(5):297- 300.
18. Bergbrant IM. Seborrhoeic dermatitis and
Pityrosporum ovale: cultural, immunologic and
clinical studies. Acta Derm Venereol 1991; Suppl.
167: 10-36.
28
Clinico-Epidemiological Profile of Seborrheic Dermatitis BJM Vol. 21 No. 1

Introduction
Functional gastrointestinal disorders and in
particular irritable bowel syndrome is a common
disorder and has a world wide distribution. The over
all prevalence rate is similar (approximately 10-20%)
in most industrialized countries1, 2, 3. A few studies
conducted in Bangladesh reported that IBS is a
common disorder in this population4, 5, 6. However
their sample sizes were small and included selected
groups of subjects. In the first community based
survey using Rome II criteria, authors reported a
prevalence of IBS of 24.4% in a rural population4.
It has been suggested that the variation in the
prevalence of IBS may be due to the application of
different diagnostic criteria. The prevalence estimates
for IBS from population survey among American,
European and Australian adults vary from 2.1-32%
due to the diversity of definitional criteria used7, 8, 9,
10, 11. The prevalence estimates varies even in the
COMPARATIVE PREVALENCE OF IRRITABLE BOWEL
SYNDROME (IBS) USING MULTIPLE DIAGNOSTIC
CRITERIA
IRIN PERVEEN1, MAHMUD HASAN2
Abstract
Object : The variation in the prevalence of IBS may be due to the application of different diagnostic
criteria. This study aimed to find out the comparative prevalence of IBS in an urban community
using different standard definitions (Rome and Manning criteria) and to determine the degree of
agreement between these definitions.
Methods: This population-based cross-sectional survey involved interview of 1503 persons (15 -
97years) in an urban community using a valid questionnaire based on internationally accepted
Manning and Rome criteria. The threshold for a positive diagnosis varied from two to three Manning
criteria, Rome I and Rome II criteria. Statistical analysis was performed with Statistical package for
social science (SPSS) programmers and the level of significance was set at P d” 0.05. A Kappa (K)
statistics were calculated to assess the agreement between the study definitions.
Results : A response rate of 97.2% yielded 1503 questionnaires for analysis. Prevalence estimates
of IBS according to Manning > 2, Manning > 3, Rome-I and Rome-II criteria were 7.3, 1.8%, 7.7% and
8.1% respectively. IBS was 1.3 to 1.7 times more prevalent in females than males irrespective of the
diagnostic criteria used. A ‘substantial’ to ‘near perfect’ agreement between all commonly used
definitions of IBS with highest level of agreement between Rome-I and Rome-II (k of 0.912) were
found in the present study.
Conclusion: The prevalence of IBS varies significantly depending of the diagnostic criteria employed.
It can be assumed that nearly all the standard definitions (Manning >2, Rome I and Rome II) are
almost equally sensitive in identifying IBS subjects in the community.
1. Consultant, Gastroenterology, BIHS Hospital, Darus Salam, Dhaka, Bangladesh.
2. Former Chairman and Professor, Department of Gastroenterology, BSMMU
same population when different diagnostic criteria
are used simultaneously9,12, 13, 14. In general, studies
requiring only two Manning criteria gave a higher
prevalence estimates than those requiring more
stringent criteria, such as 3 Manning or Rome criteria.
Although Masud et. al.4 used Rome II and Manning
criteria in the rural survey, no comparative study was
conducted in Bangladesh using multiple criteria in
the same population.
The aim of the present study was to find out the
overall prevalence of IBS in an urban community of
Bangladesh using different standard definitions
(Rome and Manning criteria). This study also aimed
to assess how the use of different diagnostic criteria
influences estimated IBS prevalence.
Materials and Methods
This observational study was conducted from the
months of November 2004 to March 2005. A valid
Bangladesh J Medicine 2010; 21 : 1-6
ORIGINAL ARTICLES

questionnaire was administered, using home-based
personal interviews, to 1503 subjects aged > 15 years
in a defined area of Dhaka city of Bangladesh.
Questionnaire: The questionnaire was based on
previously published study12 conducted abroad and
internationally accepted Manning and Rome criteria
for diagnosis. Bengali translation of the questionnaire
was validated by the method of forward and backward
translation. For quality assurance, and to evaluate
the comprehensibility and appropriateness of the
information, an initial survey with the questionnaire
was done on 30 selected samples. That initial survey
showed that the questions were easily
understandable by the study population.
Study definitions:
For the study, 4 main definitions of IBS were
considered: “Manning ³ 2”, “Manning ³ 3”, “Rome-1”,
and “Rome-II”. “Manning ³ 2” required the presence
of recurrent abdominal pain (more than six times in
the past one year) and two or more of the six
“Manning” criteria occurring at least 25% of time in
the past one year. “Manning 3” required recurrent
abdominal pain and three or more Manning criteria
(appendix-1).
“Rome –I” criteria required recurrent abdominal pain
(more than six times in the past one year) and at
least one of the three abdominal pain symptoms as
out lined in appendix-1 occurring more than a quarter
of the time in the past one year, plus two or more of
the five Rome defaecation symptoms occurring more
than 25% of the time in the preceding one year.
“Rome-II” criteria required abdominal pain and at
least two or more of the three abdominal pain
symptoms (appendix-1) occurring more than a quarter
of the time in the preceding one-year.
Appendix I
Diagnostic Criteria for Irritable Bowel Syndrome.
Manning Criteria Rome I Criteria Revised Rome Criteria
( Rome II)
Two or more of the following At least 3 months of continuous *At least 12 weeks, which need not be
symptoms: or recurrent symptoms of consecutive, in the preceding 12 months
of abdominal discomfort or pain that has
2of 3 features:
*Abdominal pain relieved by *Abdominal pain or discomfort –
defaecation. 1.Relieved with defaecation; and/or 1.Relieved with defaecation; and/or
*Looser stools with 2. Associated with a change in 2.Onset associated with a change in
onset of pain. frequency of stool; and/or frequency of stool; and/or
*More frequent stools with 3. Associated with a change in 3. Onset associated with a change in
the pain onset. consistency of stool: and/or form (appearance) of stool.
*Passage of mucous with *Two or more of the following, at least *Symptoms that cumulatively support
stools on one-fourth of occasions or days: the diagnosis of IBS:
*Abdominal distension 1. Altered stool frequency (for 1. Abnormal stool frequency
(visible). research purpose “altered” may be (for research purposes, “abnormal”
*Sensation of incomplete defined as >3 bowel movements each may be defined as greater than 3
rectal evacuation. day or <3 bowel movements each week); bowel movements per day and less
than 3 bowel movements per week);
2. Altered stool form (hard /lumpy 2. Abnormal stool form (lumpy /
or loose/watery ) ; hard or loose/watery stool);
3. Abnormal stool passage (straining, 3. Altered stool passage (straining,
urgency ,or feeling of incomplete urgency, feeling of incomplete
evacuation); evacuation);
4. Passage of mucous; andUsually 4. Passage of mucous;
with :
*Bloating or feeling of abdominal 5. Bloating or feeling of abdominal
distension. distension.
2
Comparative Prevalence of IBS Using Multiple Diagnostic Criteria BJM Vol. 21 No. 1

No laboratory tests or endoscopic examinations were
done in the study due to lack of feasibility.
Statistical analysis: The statistical analysis was
performed with computer-based Statistical package
for social science (SPSS) programmers. Age and sex
specific prevalence of IBS was found out by each of
the three criteria. Six comparisons were made between
the criteria i.e. each of the two Rome definitions were
compared separately to the Manning definitions and
comparisons were also made between Manning
definitions and Rome definitions. Kappa (k) values,
along with 95% confidence interval, were calculated
for each comparison. Significance value during
comparisons were assessed using Chi-squared test
with Yates’ correction, whenever necessary, and the
level of significance was set at P d” 0.05 .
Results
The area included in this study had 1547 persons
aged 15 years and above. Of them, 744 were male and
793 were female, out of which 726 males (97.58%)
and 777 females (97.98%) were interviewed and
included in this study. The mean age of the study
population was 32.18 ±12.98 years with an age range
of 15 to 97 years.
Prevalence of IBS
The sociodemographic characters and the crude, age
and gender specific, prevalence estimates of IBS
subjects are described in table-I. The overall,
unadjusted estimates ranged from 1.8 (Manning >3)
to 7.3 (Manning >2) cases per 100 using Manning
definitions, and from 7.7 to 8.8 cases per 100 using
the Rome study definitions. When more liberal
Table-I
Sociodemographic characteristics, prevalence, and individual symptom of IBS segregated by different study definitions
Variable Manning > 2 Rome-I Rome- II
Mean age ,years 33.65 + 13.24 33.87 + 13.24 33.59 + 13.6
Gender; n (prevalence) Male 41(6.5%) {P< .016} 53 (7.3%) {P< 0.05} 49 (6.7%) (P–ns }
Female 69(8.9%) 79(10.2%) 67 (8.6%)
Total 110(7.3%) 132(8.8%) 116(7.7%)
Age; prevalence (n)
15-24 years 6.31(43) 7.46(39) 6.9(36)
25-34 years 7.14(26) 9.07(33) 8.0(29)
35-44 years 8.9(27) {P-ns} 9.51(29 {P-ns} 8.2(25) {P-ns}
45-54 years 7.17(16) 9.41(21) 7.2(16)
55-64 years 7.7(5) 10.8(7) 10.8(7)
> 65 13.04(3) 13.04(3) 13.04(3)
Pain with more bowel movement, n,(%) 110 (100%) 132 (100%) 116(100%)
Pain with less bowel movement, n, (%) 7(6.36%) 11(.3%) 11(9.5%)
Pain associated with loose stools, n, (%) 78 (70.9%) 86(65.2%) 86(74.1%)
Pain associated with hard stools, n, (%) 20 (18.2%) 29(22.0%) 30(26.1%)
>3 bowel motions per day , n, (%) 26 (23.6%) 34(25.8%) 29(25%)
< 3 bowel motions/ week, n, (%) 4 (3.6%) 6(4.5%) 6(5.2%)
Loose stools, n, (%) 56 (50.9%) 70(53.0%) 67(57.8%)
Hard stools, n, (%) 19 (17.2%) 28(21.2%) 23(19.8%)
Straining, n, (%) 10(9.1%) 15(11.4%) 14(12.06%)
Urgency, n, (%) 4 (3.6%) 7(5.3%) 6(5.2%)
Incomplete Evacuation, n, (%) 25(22.7%) 29(22.1%) 25(21.5%)
Pain decreasing with bowel movements, n, (%) 32(29%) 51(38.6%) 43(37%)
Mucous, n, (%) 9(8.2%) 16(12.2%) 15(13%)
Bloating/ distension, n, (%) 59(53.6%) 65(49.2%) 54(46.5%)
ns- Not significant
3
BJM Vol. 21 No. 1 Comparative Prevalence of IBS Using Multiple Diagnostic Criteria

criteria were used, such as Manning >2 without pain,
prevalence estimate rose to 27.9% and when more
strict criteria were used, such as pain with Manning
>3, prevalence estimate dropped to 1.8%. The gender-
specific prevalence ranged from 2.6 (Manning >3) to
10.2 cases per 100 in women (Rome-I), and from 1
(Manning >3) to 7.3(Rome-I) cases per 100 in men.
IBS was 1.3-1.7 times more prevalent in females than
in males irrespective of the diagnostic criteria used
(P-0.016 in Manning >2, 0.019 in Rome-I). No other
sociodemographic variable (occupation, financial
status) was found to affect IBS prevalence estimates
irrespective of the diagnostic criteria used.
Overlap of IBS Diagnostic Categories:
There was considerable overlap applying the different
diagnostic definitions. For example, 132 subjects met
criteria for Rome I and, of them, 114 also met the
Rome II criteria (k-0.91). On the other hand, 12(10.9%)
of the subjects who met the Manning criteria did not
meet Rome-II criteria. Table- 2 shows the
concordance / agreement between the different
diagnostic criteria. Highest level of agreement was
found between Rome-I and Rome-II comparison by
k-value of 0.912(95% confidence interval: 0.875-0.949).
Lowest agreement was seen in the Manning >3 versus
Manning >2 comparisons by k value of 0.301(95% CI:
0.201-0.401) in this study.
Table- II
Degree of agreement between the Manning and Rome
criteria
a) Manning > 2 vs. Rome-I
Rome-I
IBS No IBS Total
Manning >2
IBS 109 1 110
No IBS 23 1370 1393
Total 132 1371 1503
Kappa (95% CI) = 0.89( 0.85-0.93}; P< .022
b) Manning > 2 vs. Rome-II
Rome-II
IBS No IBS Total
Manning>2 2
IBS 98 12 110
No IBS 18 1375 1393
Total 116 1387 1503
Kappa(95% CI) = 0.856(0.805-0.907); P< 0.000
c) Rome-I vs. Rome-II
Rome-II
IBS No IBS Total
Rome-I
IBS 114 18 132
No IBS 2 1369 1371
Total 116 1387 1503
Kappa (95%CI) = 0.912(0.875-0.949); P<0.
d) Manning > 2 vs. Manning > 3
Manning > 3
IBS No IBS Total
Manning > 2
IBS 22 88 110
No IBS 5 1388 1393
Total 27 1476 1503
Kappa (95%CI) = 0.301(0.201-0.401); P<0.0
e) Rome-I vs. Manning > 3
Manning > 3
IBS No IBS Total
Rome-I
IBS 27 105 132
No IBS 0 1371 1371
Total 116 1476 1503
Kappa (95%CI) = 0.319(0.227-0.411); P<0.000.
f) Manning > vs. Rome II
Rome-II
IBS No IBS Total
Manning >3
IBS 27 0 27
No IBS 89 1387 1476
Total 116 387 1503
Kappa (95%CI) = 0.59(0.259-0.459); P<0.000.
Discussion
This is the first study to obtain comparative
prevalence on IBS using multiple diagnostic criteria
in an urban population of Bangladesh. In the present
study an IBS prevalence of 1.8%, 7.3%, 8.8% and 7.7%
were found using Manning > 3, Manning > 2, Rome I
4
Comparative Prevalence of IBS Using Multiple Diagnostic Criteria BJM Vol. 21 No. 1

and Rome II criteria respectively. The prevalence of
IBS varied from 16.5-24.4% in three surveys conducted
in Bangladesh4, 5, 6. The studies by Rahman et al6
and Raihan et al5 were not population based. Although
the authors reported a prevalence of 30.5% and 24.4%
using Manning criteria and Rome II criteria
respectively in the only rural community-based
survey4; Manning criteria did not required the
persistence of symptoms (> 25% of the time) in their
study. The prevalence was 8.5% when strict Rome II
criteria were used. This is similar to Rome II study
definition of the present survey. Studies from other
developing countries reported IBS prevalence of 4.4-
30.2% using Manning criteria7, 15, 16, 17. But none of
these were population-based and only a few were in
the urban area involving selected subjects. When more
stringent criteria were used in this study, such as
Rome-I or Rome-II, prevalence estimates were 7.7-
8.8 %, which is comparable to other studies3, 12, 18,
19 conducted in western urban areas. A lower
prevalence of IBS (7.3%) was found in the present
study in comparison to that of other urban studies
conducted in western countries (13.6-22%)8, 12, 20
using two or more Manning criteria. But Boice et.
al.12 did not used the pain criteria where as others
did not required the persistence of symptoms (i.e.
>25% of times)8, 20. In this survey data were collected
by personal interview with a high response rate and
accuracy rate. Besides all the persons in the locality
were included in the survey, so the data of present
study likely to reflect the true prevalence of IBS.
A greater preponderance of IBS symptoms in women
compared to men in the present study (1.3 to 1.7times)
supports the previous findings of female
preponderance of IBS in Bangladesh4, 5, 6 and also in
western countries9, 20, 21. Like in other studies4, 6, 14
a downward trend of IBS prevalence with increasing
age was also noted in the present data.
Due to lack of feasibility, no investigation was done
on the IBS subjects. Studies showed that in the
absence of alarm symptoms diagnostic criteria have
a positive predictive value of approximately 98% and
that additional diagnostic tests have a yield of 2% or
less22.
Overlapping of IBS study definitions
The diagnostic thresholds of IBS vary on two
dimensions: duration and severity. Although the
original publication by Manning did not require the
duration criteria, in the present study Manning
definitions required symptoms to be chronic or
recurrent for at least 12 weeks which may or may not
be consecutive in the past one year. The present study
demonstrated good agreement between all commonly
used definitions of IBS according to Kappa values
(table-2). Highest level of agreement was found
between Rome-I and Rome-II: for which a k of
0.912(95% confidence interval: 0.875-0.949) was
calculated. This finding is consistent with that of
Thompson et al. in Canadian population23. Lowest
agreement was seen in the Manning >3 versus
Manning >2 comparisons by k value of 0.301(95% CI:
0.201-0.401) in this study. Saito13 and Kay24
calculated k values of 0.72 and 0.76 respectively,
when comparing two or more Manning symptoms (no
pain required in the study of Kay et al.) with the
original Rome criteria (Rome-I). The results were
similar to the k value of present study (k-0.89). But
they found lower k-values of 0.2524 and 0.4313
compared to our k of 0.85 when comparing two or
more Manning with the revised Rome criteria (Rome-
II). From the data of present study it can be assumed
that nearly all the standard definitions (Manning >2,
Rome I and Rome II) are almost equally sensitive in
identifying IBS subjects in the urban community of
Bangladesh.
Conclusion
This study demonstrated that prevalence of IBS in
urban population of Bangladesh is similar to most
other recent population-based studies. Prevalence
estimates varied widely depending on the diagnostic
criteria used and we support the previous finding that
the prevalence of IBS is greatly influenced by how
the requirement for abdominal pain is defined. Rome-
I proved more sensitive than the Rome-II in the
community-based survey for diagnosing IBS.
Substantial to near perfect agreement was found
between different study definitions. There seems to
be little advantage in applying the new criteria in
clinical practice but more restrictive Rome-II criteria
are the most relevant to use in research. More
research is required and preferably with some
appropriate investigations to find out the exact
prevalence of IBS in urban population.
Acknowledgement
We would like to thank to Dr. Saidur Rahman
Mashreky, BMRC, Dhaka, Bangladesh for Statistical
analysis, Dr. Md. Nowfel Islam, Dr Shabnam Akhter
, Md. Shahidul Islam, Md. Shafiqul Islam and the
Habitants of ward-41, Dhaka City Corporation for kind
co-operation.
References
1. Thompson WG, Heaton KW. Functional bowel
disorder in apparently healthy people.
Gastroenterology 1980; 79: 283-288.
5
BJM Vol. 21 No. 1 Comparative Prevalence of IBS Using Multiple Diagnostic Criteria

2. Stewart WF, Liherman JM, et al. Epidemilogy of
constipation (EPOC) study in the United States:
relation of clinical subtypes to socio-demographic
features. AM J Gastroenterol 1999; 94: 3530-3540.
3. Maxwel PR, Mandel MA, Kumar D. Irritable bowel
syndrome. Lancet 1997; 350: 191-195.
4. Masud MA, Hasan M, Khan AKA. Irritable bowel
syndrome in a rural community in Bangladesh:
prevalence, symptom pattern, and health care
seeking behaviour. Am J Gastroenterology 2001; 96:
1547-1552.
5. Raihan ASMA, Roy PK, Khanam M, Rahman MT,
Hasan M. Manning criteria in the diagnosis irritable
bowel syndrome in Bangladesh. Bangladesh J Med
1995; 6: 59-61.
6. Rahman M, Hasan M. Functional bowel disorders
in apparently healthy people. Bangladesh J Med
2001; 12: 105-112.
7. Jain AP, Gupta OP, Jajoo UN, Sidhwa HK. Clinical
profile of irritable bowel syndrome at a rural based
teaching hospital in Central India. J Assoc Phy India
1999; 39: 385-386.
8. Jones R, Lydeard S. Irritable bowel syndrome in
the general population. Bri Med J1991; 304: 87-
90.
9. Kay L, Jorgensen T, Jensen KH. The epidemiology
of irritable bowel syndrome in a random population:
prevalence, incidence, natural history and risk
factors. J Int Med 1994; 236: 23-30.
10. Talley NJ, Zinsmeister AR, Van Dyke C, Melton
LJ. Epidemiology of colonic symptoms and the
irritable bowel syndrome. Gastroenterology 1991;
101: 927-934.
11. Talley NJ, Phillips SF, Melton L J, Mulvihill C,
Wiltgen C, Zinsmeister AR. Diagnostic value of
Manning Criteria in irritable bowel syndrome.
Gut1990; 31: 77-81.
12. Boyce PM, Natasha A, Koloski BA, Talley NJ.
Irritable bowel syndrome according to varying
diagnostic criteria: are the new Rome II criteria
unnecessary restrictive for research and practice.
Am J Gastroenterol 2000; 95: 3176-3182.
13. Saito YA, Locke GR,III, Talley NJ, Zinsmeister AR,
Fett SL, Melton LJ, III. A comparison of the Rome
and Manning criteria for case identification in
epidemiological investigation of irritable bowel
syndrome. Am J Gastroenterol 2000; 95: 2816-2824.
14. Drossman DA, Li Z, Andruzzi E, Temple R, Talley
NJ, Thompson WG, et al. US householder survey of
functional gastrointestinal disorders: Prevalence,
socio-demography and health impact. Dig Dis Sci
1993; 38: 1559-1580.
15. Danivat D, Tankeyoon M, Srirataneban A.
Prevalence of irritable bowel syndrome in non-
western population. Br Med J 1988; 296: 1710.
16. Kapoor KK, Nigam P, Rastogi CK, Kumar A, Gupta
AK. Clinical profile of irritable bowel syndrome.
Indian J Gastroenterol 1985; 4: 15-16.
17. Olubuyide IO, Olawuyi F, Fasanmade AA. A study
of irritable bowel syndrome diagnosed by Manning
criteria in an African population. Dig Dis Sci 1995;
40: 983-985.
18. Talley NJ, Boyce P, Jones M. Identification of
distinct upper and lower gastrointestinal symptoms
groupings in an urban population. Gut1998; 42:
690-695.
19. Talley NJ, Zinsmeister AR, Melton LJ. Irritable
bowel syndrome in a community: symptom
subgroups, risk factors and health care utilization.
Am J Epidemiol 1995; 142: 76-83.
20. Heaton KW, O’ Donnel LJD, Braddon FEM, Mountford
RA, Huges AO, Cripps PJ. Symptoms of irritable
bowel syndrome in a British urban community:
consulters and non- consulters. Gastroenterology
1992; 102: 1962-67.
21. Drossman DA, Mc kee DC, Sandler RS, Mitchell
CM, Crammer EM, Lowman BC, Burger AL
Psychosocial factors in the irritable bowel syndrome:
a multivariate study of patients and non- patients
with irritable bowel syndrome. Gastroenterology
1998; 95: 701-708.
22. Hamm LR, Sorrells SC, Harding JP, Northcutt AR,
Heath AT, Kapke GF, et al. Additional investigations
fail to alter diagnosis of irritable bowel syndrome in
subjects fulfilling Rome criteria. Am J Gastroenterol
1999;94: 1279-82.
23. Thompson WG, Irvine EJ, Pare P, Ferrazzi S, Rance
L. Functional gastrointestinal disorders in Canada.
First population-based survey using Rome II criteria
with suggestions for improving the questionnaire.
Dis Dig Sci 2002: 47: 225-235.
24. Kay L, Jorgensen T, Lanng C. Irritable bowel
syndrome: which definitions are consistent? J Int
Med 1998; 244: 489-494.
6
Comparative Prevalence of IBS Using Multiple Diagnostic Criteria BJM Vol. 21 No. 1

Introduction:
Osteoarthritis (OA) is a leading cause of disability in
the elderly1. It is more common in women than in
men2. People with OA use health-care services at a
higher rate than a representative group of all
adults3,4,5. The number of people with OA disability
is expected to be doubled by the year 20206.
The goals of management of patients with
osteoarthritis are to control pain and swelling,
minimize disability, improve the quality of life, and
educate the patient about his or her role in the
management team. Management should be
individualized to the patient’s expectations, level of
function and activity, to the joints involved and the
severity of the patient’s disease, to occupational and
vocational needs, and to the nature of any coexisting
medical problems7.
EVIDENCE BASED NON PHARMACOLOGIC
MANAGEMENT OF OSTEOARTHRITIS: A REVIEW
ROWSAN ARA1, MD ZAHID ALAM2, MOHAMMAD FERDOUS UR RAHAMAN3, MONZOOR QUADER3,
JANNATARA SHEFA4
Abstract:
Osteoarthritis (OA) is a leading cause of disability in the elderly. The management of OA can be
divided into non pharmacologic interventions, pharmacologic interventions, and surgical options.
There are, at present, no specific pharmacologic therapies that can prevent the progression of joint
damage due to OA. Non pharmacologic therapies remain the main stay of management of OA patients.
There are varieties of conventional and non conventional non pharmacological options are available.
Among them, there is reasonably strong evidence of efficacy for exercise programs, weight loss,
patient education, and wedged shoe insoles is available.
Key words: Osteoarthritis, non pharmacologic therapy, management.
1. MD (Rheumatology) final part student, Bangabandhu Sheikh Mujib Medical University, Dhaka.
2. Junior consultant, Cardiology, BIRDEM, Dhaka
3. Medical Officer, Dept of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka.
4. Lecturer, Department of Community Medicine, Enam Medical College, Dhaka.
The management of OA can be divided into non-
pharmacologic interventions, pharmacologic
interventions, and surgical options. There are, at
present, no specific pharmacologic therapies that
can prevent the progression of joint damage due to
OA.
This review will discuss available evidences for non
pharmacologic management of osteoarthritis.
Non pharmacologic therapy:
There are varieties of conventional and non
conventional non pharmacological options are
available (Table 1)8. Among them, there is reasonably
strong evidence of efficacy for exercise programs,
weight loss, patient education, and wedged shoe
insoles is available for knee OA 9.
Table-I
Non pharmacolgic Management of Osteorarthritis
Conventional Options Unconventional Options
Patient education Transcutaneous electrical nerve stimulation
Arthritis self-help courses Pulsed electromagnetic fields
Weight loss Static magnets
Temperature modalities Acupuncture
Exercise Spa therapy
Orthotics Yoga
Modified activities of daily living
Bangladesh J Medicine 2010; 21 : 41-45
REVIEW ARTICLES

Patient Education and Psychosocial Support:
Patient education is an important first step in OA
therapy. The patient should be an integral part of the
decision-making team. To do this effectively, the
patient should understand the nature of OA, including
its natural history and treatment options. Some
patients may develop significant emotional
disturbances related to the pain and changes in
normal daily activities. These may include mood
disorders, such as depression, or sleep disorders8.
The patient evaluation should include an assessment
of current coping mechanisms such as activity
avoidance and denial. Some authors have suggested
that the impact of psychosocial support may be as
substantial as that of medical therapy. As an
example, regular reinforcement of management issues
with patients by telephone has been associated with
decreased joint pain and increased functional
status10,11,12. A meta-analysis of self-management
for OA of the knee in 2006 concluded that such
interventions produced significantly better psychologic
outcomes than those achieved by control subjects13.
However, pain and function may not be substantially
improved by instruction in self-management14.
Weight loss:
Obesity is an important risk factor in the development
of OA of the knee15,16. One study noted an increased
risk of developing OA of the knee in patients with
high body mass indices (1.5 and 2.1 for men and
women, respectively) 17. In a follow-up study using
the same population, the risk of developing OA was
reduced following weight loss; a ten-pound weight
loss over 10 years decreased the odds for developing
knee OA by 50 percent18.
Regimens of weight loss and exercise have been
associated with improvement in pain and disability
in OA of the knee19. In addition to reducing the risk
of progression of OA, weight loss of even modest
degree, may produce improvement in joint pain and
function. In a prospective study 316 overweight people
with symptomatic and radiographic OA of the knees
were randomly assigned to one of four groups: diet
alone, exercise alone, diet and exercise, or education
in healthy living. The combination of diet and exercise
was the most effective and was associated with
decreased knee pain and improved self-reported and
measured function20. Another study suggested that
a reduction in the percentage body fat, rather than
weight, may be significant in reducing pain from OA
of the knee21. The symptom-relieving effects of weight
loss have been shown to last as long as 1 year22.
Temperature modalities:
Heat and cold modalities have been used for many
years in the treatment of OA despite the paucity of
adequate controlled, randomized clinical studies.
Moist superficial heat can raise the threshold for
pain23, produce analgesia by acting on free nerve
endings24, and decrease muscle spasm25.
Warm applications can be in the form of warm soaks
or heating pads. Individual sessions should not
exceed a temperature of 45°C or last more than
approximately 30 minutes26.
Exercise
An appropriate exercise program is an integral part
of the optimal, multidisciplinary management of OA.
The relationship between exercise and arthritis has
been the subject of considerable controversy. This
issue has been well addressed in two large,
randomized trials of the impact of exercise on the
disability associated with OA. In one study, 102
patients with documented OA of one or both knees
were randomized to receive either a combined program
of supervised fitness walking and education or routine
medical care and telephone contact showed that a
program of supervised fitness walking and patient
education can improve functional status without
worsening pain or exacerbating arthritis-related
symptoms in patients with osteoarthritis of the
knee27. “The Fitness Arthritis and Seniors Trial
(FAST)” compared the impact of 18 months of aerobic
exercise, resistance exercise, or a health education
program on several measures of disability, physical
performance, and pain in elderly subjects with OA of
the knee concluded that older disabled persons with
osteoarthritis of the knee had modest improvements
in measures of disability, physical performance, and
pain from participating in either an aerobic or a
resistance exercise program and exercise should be
prescribed as part of the treatment for knee
osteoarthritis28.
A systematic review of randomized clinical trials,
which investigated the effectiveness of exercise
therapy for OA of the hip or knee, concluded that,
there is evidence of modest benefits from exercises29.
Meta-analyses of randomized trials focused on OA of
the knee, appeared in 2006 and 200913, 30. The authors
of the meta-analyses concluded that exercise
regimens for patients with OA of the knee led to
improved physical health and an at least short term
beneficial effect on OA. Home-based exercise
interventions also significantly improve symptoms in
those with knee OA 31.
42
Evidence Based Non Pharmacologic Management of Osteoarthritis: A Review BJM Vol. 21 No. 1

Patients with moderate to severe OA may not have
as much symptomatic benefit from exercise as those
with mild disease. This was illustrated in a study
that randomly assigned middle aged adults with
symptomatic and radiographically apparent (grade III
of IV) OA of the knee to aerobic exercise or to no
intervention. After six weeks there were no significant
differences between groups in knee pain or function.
Self-reported quality of life was significantly better
in those who exercised and this difference persisted
for up to six months, at which time observations were
ended32.
Orthotics and Bracing
Orthotics ranging from insoles to braces can be
effective in providing symptomatic relief and are
probably underused by most physicians. Studies have
demonstrated that lateral wedged insoles provide
substantial relief to those with medial compartment
knee OA, particularly those with varus deformity33.
In some studies, those with milder symptoms
obtained greater benefit34. Knee braces have been
evaluated as well. Valgus bracing of patients with
medial compartment OA can reduce pain and increase
levels of activity35. In one study, medial taping of the
patella reduced the pain of those with patellofemoral
compartment OA by 25%36.
Heel lifts have been tried in those with hip OA. In
one uncontrolled study, most patients reported
diminished symptoms. Time to improvement
lengthened with the radiographic stage of OA37. Those
with carpometacarpal joint arthritis should initially
be offered conservative management, including the
use of splints. In one trial, 70% of patients treated
with a 7-month intervention that included the use of
splints were able to improve their symptoms
considerably and avoid surgical intervention38.
The appropriate use of a cane can be an important
adjunct, particularly in OA of the hip. It has been
estimated that a cane can provide up to a 40%
reduction in hip contact forces during ambulation39.
The cane should be used in the hand contralateral to
the affected hip or knee40 and should be advanced
with the affected limb while walking. The appropriate
cane size is that which results in about a 20-degree
flexion of the elbow during use41.
Modification in Activities of Daily Living
Physician advice and occupational therapy can provide
useful insights into modifications of daily activities
to reduce OA symptoms. These interventions can
range from using an elevated toilet seat or shower
bench in someone with lower extremity OA to using
appliances designed to open jars in patients with
hand OA. Assistance from occupational therapists
can be valuable8.
Transcutaneous electrical nerve stimulation (TENS)
A double-blind, randomized, controlled study of 78
patients with knee OA found that daily TENS for four
weeks resulted in significant short-term improvement
in knee pain, flexion, and duration of morning
stiffness42. A double-blind, cross-over trial of 36
patients with knee OA was unable to confirm a positive
response to TENS 43. TENS use for 3 weeks was
compared with 3 weekly hyaluronic acid injections in
60 patients with OA of the knee. Pain relief was
observed in both groups through the 6 months of
follow-up44.
Pulsed electromagnetic fields:
Pulsed electromagnetic fields have been tested in
double-blind, placebo-controlled trials. In one study,
a primary end point of pain reduction was not
achieved45. Another study did not meet its primary
end point but reported an improvement in knee
stiffness in subjects younger than 65 years, without
an accompanying reduction in pain46.
Static magnets:
In one double-blind, randomized, placebo-controlled
trial of 43 patients, the WOMAC pain and physical
function subscales, along with a 50-foot walk,
demonstrated a statistically significant benefit of
static magnets at 2 weeks47. Another 29-patient
double-blind, placebo-controlled trial in knee OA
reported a benefit over placebo after 4 hours of use,
but there were no significant differences between
groups at 6 weeks of continued treatment48.
Acupuncture:
Early clinical trials49, 50 and one literature review51
concluded that acupuncture shows promise in the
treatment of knee pain from OA.
Spa therapy:
Spa therapy also has advocates. It has been touted
for low back pain and for lower extremity OA52.
However, randomized, controlled studies are
lacking53.
Yoga:
Yoga has also shown some symptomatic benefit in
OA of the hands, based on limited testing54.
Conclusion:
The treatment of OA includes a variety of possible
non-pharmacologic and pharmacologic interventions.
This review discusses only evidences of non
pharmacologic aspect of management. Treatment
43
BJM Vol. 21 No. 1 Evidence Based Non Pharmacologic Management of Osteoarthritis: A Review

should be tailored to the individual and consists of a
combination of modalities. These provide symptom
relief but have no proven effect on the progression of
disease. Structure and disease modification has yet
to be achieved in OA. Trials that are under way could
determine whether this is a realistic goal.
References:
1. Guccione AA, Felson DT, Anderson JJ. The effects
of specific medical conditions on the functional
limitations of elders in the Framingham Study. Am
J Public Health 1994;84:351-8.
2. Felson DT. Epidemiology of osteoarthritis. In: Brandt
KD, Doherty M, Lohmander LS, editors.
Osteoarthritis. Oxford, England: Oxford University
Press 2003. P.9-16.
3. Bridges-Webb C, Britt H, Miles DA, Neary S, Charles
J, Traynor V. Morbidity and treatment in general
practice in Australia. Aust Fam Physician
1993;22:336–46.
4. Felts W, Yelin E. The economic impact of rheumatic
diseases in the United States. J Rheumatol
1989;16:867–84.
5. Gabriel SE, Crowson CS, Campion ME, O’Fallon WM.
Direct medical costs unique to people with arthritis.
J Rheumatol 1997;24:719–25.
6. Badley EM. Population projections and the effect
on rheumatology. Ann Rheum Dis 1991; 50:3–6.
7. Available from http://www.uptodate.com/contents/
nonpharmacologic-therapy-of-osteoarthritis
8. Lozada CJ. Management of Osteoarthritis. In:
Firestein GS, Budd RC, Harris ED Jr, McInnes IB,
Ruddy S, Sergent JS, editors. Kelly’s Textbook of
Rheumatology. 8th ed. Philadelphia: Saunders
Elsevier; 2009. p.1563-73
9. Jordan KM, Arden NK, Doherty M, Bannwarth B,
Bijlsma JW, Dieppe P, et al. EULAR
Recommendations 2003; an evidence based approach
to the management of knee osteoarthritis: Report of
a task force of the standing committee for
international clinical studies including therapeutic
trials (ESCISIT). Ann Rheum Dis 2003; 62:1145.
10. Rene J, Weinberger M, Mazzuca SA. Reduction of
joint pain in patients with knee osteoarthritis who
have received monthly telephone calls from lay
personnel and whose medical treatment regimens
have remained stable. Arthritis Rheum 1992;
35:511.
11. Weinberger M, Hiner SL, Teirney WM. Improving
functional status in arthritis: the effect of social
support. Soc Sci Med 1986; 23:899.
12. Weinberger M, Teirney WM, Booher P, Katz BP. Can
the provision of information to patients with
osteoarthritis improve functional status? Arthritis
Rheum 1989; 32:1577.
13. Devos-Comby L, Cronan T, Roesch SC. Do exercise
and self-management interventions benefit patients
with osteoarthritis of the knee? A Meta analytic
review. J Rheumatol 2006; 33:744.
14. Buszewicz M, Rait G, Griffin M, Nazareth I, Patel A,
Atkinson A, et al. Self management of arthritis in
primary care: randomised controlled trial. BMJ
2006; 333:879.
15. Coggon D, Reading I, Croft P, McLaren M, Barrett
D, Cooper C. Knee osteoarthritis and obesity. Int J
Obes Relat Metab Disord 2001; 25:622-7.
16. Sturmer T, Gunther KP, Brenner H. Obesity,
overweight and patterns of osteoarthritis: The Ulm
Osteoarthritis Study. J Clin Epidemiol 2000; 53:
307-13.
17. Felson DT, Anderson JJ, Naimark A, Walker AM,
Meenan RF. Obesity and knee osteoarthritis: the
Framingham study. Ann Intern Med 1988; 109:18.
18. Felson, DT. Weight loss reduces the risk for
symptomatic knee osteoarthritis in women. Ann
Intern Med 1992; 116:535.
19. Messier SP, Loeser RF, Mitchell MN, Valle G,
Morgan TP, Rejeski WJ, et al: Exercise and weight
loss in obese older adults with knee osteoarthritis:
A preliminary study. J Am Geriatr Soc 2000;
48:1062-72.
20. Messier SP, Loeser RF, Miller GD, Morgan TM,
Rejeski WJ, Sevick MA, et al. Exercise and dietary
weight loss in overweight and obese older adults
with knee osteoarthritis: the Arthritis, Diet, and
Activity Promotion Trial. Arthritis Rheum 2004;
50:1501.
21. Toda Y, Toda T, Takemura S, Wada T, Morimoto T,
Ogawa R., et al: Change in body fat, but not body
weight or metabolic correlates of obesity, is related
to symptomatic relief of obese patients with knee
osteoarthritis after a weight control program. J
Rheumatol 1998; 25:2181-6.
22. Christensen R, Astrup A, Bliddal H. Sustained
weight loss as a treatment of osteoarthritis in obese
patients: Long-term results from a randomized trial.
Ann Rheum Dis 2005; 64(III):66.
23. Hollander JL, Horvath SM. The influence of physical
therapy procedures on the intra-articular
temperature of normal and arthritis subjects. Am J
Med Sci 1949; 218:543?
24. Fischer E, Solomon S. Physiological responses to
heat and cold. In: Licht S, editor. Therapeutic Heat
and Cold . New Haven: CT; 1965. p.126.
25. Hicks JE, Gerber LH. Rehabilitation in the
management of patients with osteoarthritis. In:
Moskowitz RW, Howell DS, Goldberg VM, Mankin
HJ, editors. Osteoarthritis: Diagnosis and Medical/
Surgical Management. WB Saunders: Philadelphia;
1992. p.433.
44
Evidence Based Non Pharmacologic Management of Osteoarthritis: A Review BJM Vol. 21 No. 1

26. Lehman JF, DeLateur BJ. Diathermy and superficial
heat, laser, and cold therapy. In: Kottke FJ, Lehman
JF, editors. Krusen’s Handbook of Physical Medicine
and Rehabilitation. 4th ed. Philadelphia: WB
Saunders; 1990:283-367.
27. Kovar PA, Allegrante JP, MacKenzie CR, Peterson
MG, Gutin B, Charlson ME. Supervised walking in
patients with osteoarthritis of the knee. Ann Intern
Med 1992; 116:529.
28. Ettinger WH Jr, Burns R, Messier SP, Applegate W,
Rejeski WJ, Morgan T, et al. A randomized trial
comparing aerobic exercise and resistance exercise
with a health education program in older adults
with knee osteoarthritis: The Fitness Arthritis
Seniors Trial (FAST). JAMA 1997;277:25.
29. van Baar ME, Assendelft WJ, Dekker J, Oostendorp
RA, Bijlsma JW. Effectiveness of exercise therapy
in patients with osteoarthritis of the hip or knee.
Arthritis Rheum 1999; 42:1361.
30. Fransen M, McConnell S. Land-based Exercise for
Osteoarthritis of the Knee: A Meta analysis of
Randomized Controlled Trials. J Rheumatol 2009;
36:1109.
31. Thomas KS, Muir KR, Doherty M, Jones AC, O’Reilly
SC, Bassey EJ. Home based exercise programme for
knee pain and knee osteoarthritis: Randomised
controlled trial. BMJ 2002; 325:752.
32. Thorstensson CA, Roos EM, Petersson IF, Ekdahl
C. Six-week high-intensity exercise program for
middle-aged patients with knee osteoarthritis: a
randomized controlled trial. BMC Musculoskelet
Disord 2005; 6:27.
33. Kerrigan DC, Lelas JL, Goggins J, Merriman GJ,
Kaplan RJ, Felson DT. Effectiveness of a lateral-
wedge insole on knee varus torque in patients with
knee osteoarthritis. Arch Phys Med
Rehabil 2002;83:889-93.
34. Keating EM, Faris PM, Ritter MA, Kane J. Use of
lateral heel and sole wedges in the treatment of
medial osteoarthritis of the knee. Orthop
Rev 1993; 22:921-4.
35. Pollo FE, Otis JC, Backus SI, Warren RF, Wickiewicz
TL. Reduction of medial compartment loads with
valgus bracing of the osteoarthritic knee. Am J
Sports Med 2002; 30:414-21.
36. Cushnaghan J, McCarthy C, Dieppe P. Taping the
patella medially: A new treatment for osteoarthritis
of the knee joint? BMJ 1994; 308:753-5.
37. Ohsawa S, Ueno R. Heel lifting as a conservative
therapy for osteoarthritis of the hip: Based on the
rationale of Pauwels’ intertrochanteric osteotomy.
Prosthet Orthot Int 1997;21:153-8.
38. Berggren M, Joost-Davidsson A, Lindstrand J,
Nylander G, Povlsen B. Reduction in the need for
operation after conservative treatment of
osteoarthritis of the first carpometacarpal joint: A
seven year prospective study. Scand J Plast
Reconstr Surg Hand Surg 2001;35:415-7.
39. Brand RA, Crowninshield RD. The effect of cane
use on hip contact force. Clin Orthop 1980;147:
181-4.
40. Chan GN, Smith AW, Kirtley C, Tsang
WW. Changes in knee moments with contrateral
versus ipsilateral cane usage in females with knee
osteoarthritis. Clin Biomech 2005; 20:396-404.
41. Blount WP. Don’t throw away the cane. J Bone
Joint Surg Am 1956; 38:695-708.
42. Zizic TM, Hoffman KC, Holt PA, Hungerford DS,
O’Dell JR, Jacobs MA, et al. The treatment of
osteoarthritis of the knee with transcutaneous
electrical nerve stimulation. J Rheumatol 1995;
22:1757.
43. Lewis B, Lewis D, Cumming G. The comparative
analgesic efficacy of transcutaneous electrical nerve
stimulation and a non-steroidal anti inflammatory
drug for painful osteoarthritis. Br J Rheumatol
1994;33:455.
44. Paker N, Tekdos D, Kesiktas N, Soy D. Comparison
of the therapeutic efficacy of TENS versus intra-
articular hyaluronic acid injection in patients with
knee osteoarthritis: A prospective, randomized
study. Adv Ther 2006;23:342-53.
45. Pipitone N, Scott DL. Magnetic pulse treatment for
knee osteoarthritis: A randomised, double-blind,
placebo-controlled study. Curr Med Res Opin 2001;
17:190-6.
46. Thamsborg G, Florescu A, Oturai P, Fallentin E,
Tritsaris K, Dissing S. Treatment of knee
osteoarthritis with pulsed electromagnetic fields: A
randomized, double-blind, placebo-controlled study.
Osteoarthritis Cartilage 2005;13:575-81.
47. Hinman MR, Ford J, Heyl H. Effects of static
magnets on chronic knee pain and physical
function: A double-blind study. Altern Ther Health
Med 2002; 8:50-5.
48. Wolsko PM, Eisenberg DM, Simon LS, Davis RB,
Walleczek J, Mayo-Smith M, et al: Double-blind,
placebo-controlled trial of static magnets for the
treatment of osteoarthritis of the knee: Results of a
pilot study. Altern Ther Health Med 2004; 10:36-
43.
49. Tillu A, Tillu S, Vowler S. Effect of acupuncture on
knee function in advanced osteoarthritis of the knee:
A prospective, non-randomised controlled study.
Acupunct Med 2002; 20:19-21.
50. Berman BM, Singh BB, Lao L, Langenberg P, Li H,
Hadhazy V, et al: A randomized trial of acupuncture
as an adjunctive therapy in osteoarthritis of the
knee. Rheumatology (Oxford) 1999; 38:346-54.
51. Ezzo J, Hadhazy V, Birch S, Lao L, Kaplan G,
Hochberg M, et al: Acupuncture for osteoarthritis of
the knee: A systematic review. Arthritis
Rheum 2001; 44:819-25.
52. Guillemin F, Virion JM, Escudier P, De Talancé N,
Weryha G. Effect on osteoarthritis of spa therapy at
Bourbonne-les-Bains. Joint Bone Spine 2001;
68:499-503.
53. Ernst E, Pittler MH. How effective is spa treatment?
A systematic review of randomized studies. Dtsch
Med Wochenschr 1998; 123:273-7.
54. Garfinkel M, Schumacher Jr. HR. Yoga. Rheum Dis
Clin North Am 2000; 26:125-32
45
BJM Vol. 21 No. 1 Evidence Based Non Pharmacologic Management of Osteoarthritis: A Review

FEEDING PRACTICE AMONG ANEMIC AND NON-
ANEMIC INFANTS AND YOUNG CHILDREN IN A
SELECTED RURAL AREA
MITHUN ALAMGIR1, JANNATARA SHEFA2, KHAN SHAKIL AHMED3, SHAFINAZ GAZI4, MOHAMMAD
FERDOUS UR RAHAMAN5, MD. ABUL KALAM AZAD6
Abstract:
Background: Iron deficiency is a major public health problem worldwide especially in developing
countries. It is now a major public health problem in Bangladesh & leading cause of morbidity and
mortality of in young children (6-23months). Recent surveys in Bangladesh show very high prevalence
figures of anemia ranging from 70%-90% among young children.1 Objective: To find out the feeding
practice among the anemic & non anemic infants (6-11months) & young children (12-23months) in
rural Bangladesh. Methods: This cross sectional comparative study was conducted on purposively
selected anemic and non-anemic 150 infants and young children residing in a rural area (Village:
Shadapur, Thana: Nowabgonj) of Bangladesh to determine the association between feeding practice
and anemia status. Infants ranging from 6-11 months & children ranging from 12-23 months were
the enrollment criteria for the study. Pre tested structured questionnaire was used to collect the
data from parents & anemia status was determined by the field level Spectrophotometer. The test
statistics used to analyze the data were descriptive statistics and Chi-square (χ2) test.
Result: Of the 150 children in the study, 77(51.3%) were infants and the rest 73(48.7%) were
young children. Among the breast fed (67%) babies nearly 74% was fed on demand, the rest 26%
was given scheduled feeding. 60% of the respondents started complimentary feeding from 6
months, 26.7% before 6 months and 13.3% after 6 months. 53.3% of the respondents followed
standard guideline (WHO/UNICEF guidelines) in feeding their babies. The prevalence of anemia
was 55.3% in 6 – 23 months children. The prevalence of anemia was a bit higher in the infants then
young children. Breast-fed on demand was found to be significantly higher in non-anemic infants.
About 85% non-anemic infants & 90% children were given WHO/UNICEF guidelines in giving
complementary food. Conclusions: the best solution as it is evident from the present study that
anemia was significantly less prevalent among children whose mothers followed the guideline than
those children whose mothers did not follow it.
1. Assistant Professor, Department of Community Medicine, Enam Medical College, Dhaka.
2. Lecturer, Department of Community Medicine, Enam Medical College, Dhaka.
3. Assistant Professor, Department of Forensic Medicine, Enam Medical College, Dhaka.
4. MS student, Department of Anatomy, Bangabandhu Sheikh Mujib Medical University, Dhaka.
5. Medical officers, Department of Medicine, BSMMU, Bangabandhu Sheikh Mujib Medical University, Dhaka.
6. Associate professor, Department of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka.
Introduction:
Iron deficiency is a major public health problem
worldwide especially in developing countries. There
are about 2 million individual are affected by various
types of anemia, most of them are in IDA (Iron
deficiency anemia) in developing countries. It is now
a leading cause of morbidity and mortality of in young
children. Anemia is a major public health problem in
Bangladesh; under 6-23 months aged children are the
most vulnerable group. Recent surveys in Bangladesh
show very high prevalence figures of anemia ranging
from 70%-90% among young children.1 The last
anemia survey in Bangladesh describes in 6-11
months children 76% are anemic. In 12-23 months
the prevalence is 58%.2 In rural area, 61% children
are anemic as compared to 73% in urban area, in age
group 6-23 months.
In country like India, Nepal and Sri Lanka the
prevalence of IDA also high in this group (India 77%,
Nepal 88%, Srilanka 55%).3
Improper feeding, early weaning, insufficient breast
feeding, low birth weight etc are the main cause of
IDA in children 6-23 months of age. In these age
group children cannot depend on breast milk alone
to meet their iron requirements.
Bangladesh J Medicine 2010; 21 : 19-24

Generally IDA is due to two of bioavailability of dietary
iron and large loss of iron from the body. Food
containing ascorbic acid (Vitamin C) and heam iron
increase absorption of iron from whole meal. Ascorbic
acid is very important for absorption of non-heam
iron. National nutrition survey in Bangladesh showed
dietary iron is quite high in poor but 86% was
anemic.4
For infant and young children, IDA has potentially
irreversible effect on cognitive motor and language
development, future learning capacity, school
performance and immunity.
Proper feeding and caring practice has a role on IDA
of children. WHO suggested that after exclusive
breast feeding up to 4-6 months of life the evolving
nutritional requirements of infants should be met by
nutritionally adequate and safe complementary feed
while breast feeding continues for up to 2 years of
age as beyond. However in developing countries giving
a hygienic food to a baby is sometimes difficult in
poor society can increase their risk of infection. In
these cases WHO recommend exclusive breast feed
up to 6 months of age and after that proper caring
practice is needed to caring a child.
The cause of high prevalence of IDA in 6-23 months
of age is defective feeding practice. 6-23 months
children cannot depend only on breast milk alone. To
meet their iron requirements WHO and UNICEF have
suggested that 6 months old infant should give in
addition of breast milk, frequent small complementary
meal that rich in energy, protein and micronutrients.
However, survey show that while breast-feeding is
generally continued well into the second year of life,
infants are given food that rarely contains item supply
adequate nutrients.5 In addition complementary food
is heavily shaded with cereal that contains high
amount of phytates, which is a potent iron absorption
–inhibitor. This makes infants highly susceptible to
IDA. In developing countries 39% children were given
complementary feeding from 4 months age, that is
early weaning, which is also a risk factor of IDA. 41%
of infants aged over 6 months are fed virtually nothing
else but breast milk until the age of 2 years, which is
late weaning and another risk factor of IDA. Apart
from these feeding problems the young children are
affected by worm infestation of poor hygiene one of
the important factors of caring practice. Helminthes
infection is also a major cause of IDA in young
children. Globally food fortification as iron
supplementation has proven to be a useful strategy
to address the IDA. WHO has recommended blanket
supplementation, without screening in all children
6-24 months of age.5 Education and treatment of
infection are given more importance in developing
countries.
It is evident in several studies that an Iron
intervention has rarely been effective due to a number
of reasons, mainly low compliance. It can result in
gastric irritation and abdominal discomforts.
Methods and Materials:
Study design
Cross Sectional Comparative study.
Study place
Village: Shadapur, Thana: Nowabgonj, District: Dhaka.
Study population
Infants and young children of selected rural area of
Bangladesh.
Study period
March – June’2007
Sample size
Purposively 150 samples have been taken from study
area.
Sampling Technique
Purposive sampling technique (Non Probable)
Ethical implication
As the study was conducted in a rural area, first of
all a written permission was taken from the local
authority. Then both verbal and written consent was
taken from the respondent parents.
Data Collection instrument
A questionnaire was prepared as a research
instruments in such a way that the interview could
flow as naturally as possible. They were designed
according to objectives of the study and were made
simple and easily understandable manner. The
questionnaire was pre-tested on a small number of
respondents at Keranigonj, Dhaka similar to the
study population to identify and difficulty for
understanding by the respondents. Then modified and
finalized the questionnaire for data collection.
Data collection technique
The purpose of the study was explained to the local
authority and to the respondents. Data was collected
from respondent through face to face interview by
using the Bangla pre-tested structured questionnaire.
To determine the anemia status blood was collected
from the baby by field level spectrophotometer.
Data processing and analysis
After completion of data collection data were
processed and edited manually to reduce error. Both
descriptive and analytical statistics were done by
SPSS (11.5 version)
20
Feeding Practice among Anemic and Non-Anemic Infants and Young Children BJM Vol. 21 No. 1

Selection criteria
For anemic inclusion:
1. Study population was within 6 – 23 months of
age
2. Hemoglobin level bellow 11 gm/dl
3. Free from any acute or chronic illness
4. Parents willing to participate
For non-anemic inclusion:
1. Study population was within 6 – 23 months of
age
2. Hemoglobin level equal or more than 11 gm/dl
3. Free from any acute or chronic illness
4. Parents willing to participate
Results:
The findings of the study intended to investigate the
association between anemia and feeding practice of
infants and young children are documented below.
Of the 150 children participated in the study,
77(51.3%) were infants ranging from
6 – 11 months and the rest 73(48.7%) were young
children ranging from 12 – 23 months. Fig. 1 shows
the distribution of the children by sex. Males and
females were almost equally distributed giving a male
to female ratio of roughly 1:1.
Table II shows the educational status of parents’ of
participating children. About 23% of the fathers were
illiterate, 13% primary level educated, 13.7%
secondary level educated, 35.1% SSC to HSC level
educated and 15.3% graduate and higher level
educated. In terms of mothers’ education, 35.3% were
illiterate, 18% primary, 14.7% secondary, 24.7% SSC
to HSC and only 7.3% graduate and postgraduate level
educated.
Table III shows the distribution of the respondents
by feeding practice of their babies. Two-third (66.7%)
the babies were breast fed. Of the breast fed babies
nearly three-quarter (74%) was fed on demand, while
the rest (26%) was given the same 2 times daily. Sixty
percent of the respondents informed that they started
complimentary feeding from 6 months, 26.7% before
6 months and 13.3% after 6 months. Over half (53.3%)
of the respondents followed standard guideline
(WHO/UNICEF guidelines) in feeding their babies.
About 75% of the mothers of breast-fed infants and
59.5% of mothers without breast-fed infants gave e”
3 and e” 5 complimentary feeds (CF) respectively in
24 hours, while 70.3% of the mothers of young
children gave 5 or more CFs in 24 hours.
Fig. 2 demonstrates age-wise distribution of anemia
among children ranging from 6 – 23 months. The
prevalence of anemia was 55.3%in 6 – 23 months
children. The prevalence of anemia was a bit higher
in the infants (6 – 11 months) compared to the young
children (12 – 23 months).
Table IV shows the association between breast feeding
status and anemia in infants. Anemia was not found
to be associated with whether the baby was breast-
fed or not (p = 0.918). Table V shows the association
between frequency of breast feeding and anemia in
infants. Breast-fed on demand was found to be
significantly higher in non-anemic infants (90.5%)
than that in anemic infants (66.7%) (p = 0.046).
Table VI shows the association between
complimentary feeding related variables and
development of anemia in young infants. More than
80% of the non-anemic infants were given
complimentary feeding from 6 months compared to
37.8% of the anemic infants (p = 0.001). About 85%
of the mothers of non-anemic infants followed
standard guidelines (WHO/UNICEF guidelines) in
giving complimentary feeding to their babies as
opposed to 26.7% of the mothers of anemic infants
(p < 0.001).
Table I
Distribution of the study children by age (n = 150)
Age (months) Frequency Percentage
Infant (6 – 11 months) 77 51.3
Young children
(12 – 23 months) 73 48.7
Fig.-1: Distribution of the children by sex (n = 150)
21
BJM Vol. 21 No. 1 Feeding Practice among Anemic and Non-Anemic Infants and Young Children

Table II
Distribution of children by parents’ educational status
Parents educational status Frequency Percentage
Fathers’ education
Illiterate 30 22.9
Primary 17 13.0
Secondary 18 13.7
S.S.C & H.S.C 46 35.1
Graduate & above 20 15.3
Mothers’ education
Illiterate 53 35.3
Primary 27 18.0
Secondary 22 14.7
S.S.C & H.S.C 37 24.7
Graduate & above 11 7.3
Table III
Distribution of the respondents by baby feeding
practice
Feeding practice Frequency Percentage
Baby breast fed (n = 150)
Yes 100 66.7
No 50 33.3
Frequency of breast feeding (n = 100)
Feeding on demand 74 74.0
Scheduled feeding 26 26.0
Complimentary feeding started (months)
< 6 40 26.7
From 6 90 60.0
> 6 20 13.3
WHO/Unicef guidelines followed
Yes 80 53.3
No 70 46.7
Frequency of CF* in infants with BF**
< 3 14 25.6
³ 3 40 74.1
Frequency of CF in infants without BF
< 5 15 40.5
³ 5 22 59.5
Frequency of CF in young children
< 5 22 29.7
³ 5 52 70.3
* CF = Complimentary feeding;
**BF = Breast feeding
Table-IV
Association between breast feeding status and anemia
in infants
Breast feeding Status of anemia p-
status# Anemic Non-anemic value
(n = 45) (n = 30)
Breast-fed 32(71.1) 21(70.0) 0.918
Not Breast-fed 13(28.9) 9(30.0)
# Data were analyzed using Chi-square (χ2) Test.
Figure in the parentheses denoted corresponding percentage.
Table-V
Association between frequency of breast feeding and
anemia in infants
Frequency of breast Status of anemia p-
feeding# Anemic Non-anemic value
(n = 33) (n = 21)
Feeding on demand 22(66.7) 19(90.5) 0.046
Scheduled feeding 11(33.3) 2(9.5)
# Data were analyzed using Chi-square (χ2) Test.
Figure in the parentheses denoted corresponding percentage.
Table VI
Association between complimentary feeding and anemia
in infants
Complimentary Status of anemia p-
Feeding Anemic Non-anemic value#
(n = 45) (n = 32)
Complimentary feeding started#
Below 6 months 19(42.2) 5(15.6)
From 6 months 17(37.8) 9(20.0) 26(81.3) 0.001
After 6 month 1(3.1)
Standard guide-line followed Yes
No 12(26.7) 27(84.4)
33(73.3) 5(15.6) < 0.001
# Data were analyzed using Chi-square (χ2) Test.
Figure in the parentheses denoted corresponding percentage
Fig. 2: Distribution of respondents by anemia (n = 150)
22
Feeding Practice among Anemic and Non-Anemic Infants and Young Children BJM Vol. 21 No. 1

Discussion:
The present study showed that 55.3% of 6 – 23 months
children were anemic. The prevalence of anemia was
a bit higher in 6 – 11 months infants (58.4%)
compared to
12 – 23 months children (52.1%). Recent survey in
Bangladesh shows very high prevalence of anemia
ranging from 70% - 90% among young children.1 The
last anemia survey in Bangladesh described 76% of 6
– 11 months children and 58% of 12 – 23 months
children as anaemic.2 In rural area 61% of children
are anemic in the age group of 6 – 23 months. In
country like India, Nepal and Srilanka the prevalence
of IDA are also high in these age group (India-77%,
Nepal-88%, Srilanka-55%).3 As of feeding practice,
two-third (66.7%) the babies were breast-fed. 60% of
the mothers started complementary feeding from 6
months, 26.7% before 6 months and 13.3% after 6
months. About 75% of the breast-fed infants and 60%
of non breast-fed infants were given e” 3 and e” 5
complementary feeds (CFs) respectively in 24 hours,
while 70.3% of the mothers of young children gave 5
or more CFs in 24 hours. Over half (53.3%) of the
mothers followed standard guideline (WHO/ UNICEF
guidelines). A nationwide community based cross
sectional study was conducted in Bangladesh on a
representative sample of 3049 children of 0-2 years
and on their mothers showed that half of the mothers
initiated breast feeding more than 1 hour after birth.
Prevalence of exclusive breast feeding among 6 months
and or below was 61%. More than half (50.8%) of the
children were given complementary feeding before 4
months and about 40% at 4 – 5 months of age. Among
1463 infants of 6-11 months, 51.4% were given 3 feeds
a day. Among 506 children 12 – 24 months over 56%
were given 3 feeds a day. It was reported that about
95% of the children of one year of age and 82.7% of
two years of age were breast fed throughout. About
2.8% of the children were suffering from severe
nutritional deficiency disorder and 14.1%-18% were
suffering from moderate nutritional deficiency disorder
respectively.6 The findings are consistent with the
findings of the present study. Contrary to these
findings that majority (97.8%) of children was
breastfed but only 10.4% of them were exclusively
breastfed up to 6 months. Weaning was started at
the age of 6 months in about 20% cases. 50%
continued breast feeding for a period 1-2 years.7
A hospital based analytic study was conducted in
Brisbane Australia in the year 2001; Data were
obtained from records held at Maternal and Infant
Health Clinics in the cities of Brisbane (population
100000). 80-90% of mothers brought their infants to
the clinics after 6 months of delivery. On the first
visit to the clinic social, family, feeding practice
history were recorded. At each subsequent visit, the
data, presents weight and feeding of the infant and
young children, status of health (especially anemia)
was assessed. Percentage of breast feeding at first
visit and subsequent 2 visits after 6 months was 67%,
68% and 69% which is fairly comparable to the
findings of the present study. Prevalence of anemia
after 6 months was 30%, almost that found in our
study (58.5%). Those who practices breast feeding as
well as proper complementary feeding (according to
hospital guideline), rate of anemia was only 10% which
is also much less compared to our sampled
population with similar characteristics. Rest of 20%
was among those who did not practice breast feeding,
complementary feeding regularly. The data of infants
and young children, who attended the Maternal and
Infant Health Clinics for 2 years, were used to test
the relationships of infant breast feeding with secular
trend and social class at 6-11 months and 12-23
months. At each of these age group, there was a highly
significant (p < 0.001) increase in the level of breast
feeding from 1982 to 1993. In the 1982 data, there
was a trend for more primiparous and upper class
mothers to breast feed during the first three months
than multiparous and lower class mothers but this
trend did not show the statistical significance. In
1993, the general prevalence of breast feeding had
increased and same trends were present. This study
showed that there has been a marked increase in
the prevalence of breast feeding amongst mothers so
that rate of nutritional anemia has been decreased a
lot.8
The prevalence of anemia among the infants who were
breast fed on demand was significantly less compared
to the scheduled breast feeding. The infants who were
given complementary feeding according WHO
guidelines were also less anemic compared to those
who did not follow the guideline meaning that it is a
standard one to prevent the infants being anemic.
The same was found true for young children too. The
findings of the study also revealed that time of starting
complementary feeding is also no less important,
because prevalence of anemia was significantly less
among the children who were given complementary
feeding from 6 months as opposed to those who were
given earlier or later than 6 months. However, feeding
the babies according to WHO/ UNICEF guidelines
was much lower which might be one of the reasons
of more than half of the infants and young children
(53.3%) being anemic. The guideline that WHO and
UNICEF recently endorsed as Global Strategy for
infant and young child feeding is to fulfill all the
23
BJM Vol. 21 No. 1 Feeding Practice among Anemic and Non-Anemic Infants and Young Children

nutrients needed by the growing children and also to
protect them from vicious cycle of malnutrition and
infection. Once some of the determinants of good
nutrition are not fulfilled, children start to suffer from
malnutrition and nutritional deficiency anemia. When
foods other than milk are introduced into the infant
diet, the situation is more complex because these
foods vary considerably in protein content and protein
quality within same country and among different
countries. Furthermore amount of weaning food
consumed and amount of milk consumed varies
among individuals. Most of the international
recommendation use protein: energy ratio (P: E) when
assessing the protein quality of weaning food. There
is assumption also in these calculations because both
the safe level of protein intake and the mean
requirement of energy at each age are included. As it
is mentioned that different country has different
feeding practice so worldwide WHO guideline is
acceptable. WHO shows the requirement of accurate
protein, energy and calorie requirement for specific
age group9.
Conclusion & Rcommendations
It has already been reflected in the discussion that
the children from 6 months onward become more
vulnerable to develop anemia because of increased
physiological demand for iron to form hemoglobin.
The mothers should therefore give their babies ideal
combination of complementary feeds along with breast
feeding. After the first year, though the daily need of
iron slightly decreased, 0.5 mg of iron still needed
each day until the end of two years. So the children
at this age too are at greater risk of developing anemia
fortifying further the need of complementary feeding
and continuation of breast feeding. At these two age
groups (6-11months and 12-23months) as iron demand
to be fulfilled from the exogenous source
complementary feeding to be given to the children
must be scientifically sound both in terms of
frequency and content. As long term iron therapy and
the intake of iron fortified food have got the deleterious
effect on the health, it is better avoiding them unless
otherwise indicated. Since feeding practice varies from
culture to culture, following WHO/UNICEF guideline
could be the best solution as it is already evident
from the present study that anemia was significantly
less prevalent among children whose mothers
followed the WHO/UNICEF guideline than those
children whose mothers did not follow it.
In the light of findings of the present study and
discussion thereof, the following recommendations
are put forward
1. Mothers should breastfed their babies on demand
and should be exclusive for the first 6 months.
2. Complementary feeding should be started at
completion of month 6 along with breast feeding.
3. Mothers must prepare the complementary feeds
in accordance with WHO/Unicef guidelines.
4. The diet should be rich in energy dense bioavailability
iron to prevent child from being anemic.
5. Mothers should be discouraged to give iron in
the form medication or food fortified with iron as
it carries the risk iron poisoning.
References
1. Andre B, Nicole D, Elaine F. Nutritional Survey
Report of HKI/IPHN .1999; 3-4.
2. Juergen M, Erhardt N. Nutritional Survey Report of
HKI/IPHN.2001; 120-122.
3. Allen P, Ana NS, Walsh KH Reports of PHNI/MEDS/
USAID. 2003; 34-38.
4. Hasan MN, Shakur D. Survey Report of BBS. 2004;
89-92.
5. Akre J, Black KH, Cohen RJ. WHO Nutritional
Survey Report. 2001; 24-36.
6. Hannan A. Rahman F. Surveillance on breastfeeding
and weaning situation & Child and maternal health
in Bangladesh. Report of 12th round survey. 2007;
94-95.
7. Azeem M, Rahman H. Breast feeding practice among
mothers working in a selected garment factory in
Tongi. Journal of Achieving Millennium
Development Goals 4 and 5. 2007; 203-204.
8. Eaton-Evans j, Townsend B, Dugdle A. The milk
feeding of infants in south-east Queensland.
Journal of Food and Nutrition.1985; 137 – 141.
9. Raiha, Axelsson. Journal of Follow-on Formula.
2000; 26-30.
10. Roeser HP. Iron. Journal of Food and Nutrition
.1986; 82 – 91.
11. Polhamus B, Dalenius k, Thompson D. Paediatric
Nutrition Surveillance. Nutrition in Clinical
Care.2003; 6: 132 – 134.
12. Thomas c. The Amaemia of Inflammation. Padiatric
Haematology.1996;43: 40-44.
13. Thomas A. A common cause of childhood Anaemia.
Paediatric Haematology.1994; 42: 20-23.
14. Sean R, Roy D. Deliberations and Evaluation of the
Approaches, Endpoints and Paradigms for Iron
Dietary Recommendation. American Institute of
Nutrition 1996; 2404 – 2409.
15. Roy SK, Chakrabarty B. Complimentary Feeding.
Report of 1st National conference on achieving MDG
.2007; 34-35.
16. Islam T, Roy S, Afsa N. Identification of inappropriate
feeding practice of children among selected slam
dwellers of Dhaka city. Report on 1st National
conference on achieving MDG.2007; 111-112.
17. Nazrul I. Report of National Nutritional Survey in
Bangladesh. 1993; 65-70.
24
Feeding Practice among Anemic and Non-Anemic Infants and Young Children BJM Vol. 21 No. 1

Introduction
Periodontitis is an infection of the tissues that hold
the teeth in place. In periodontitis, plaque builds
and hardens under the gums. The gums pull away
from the teeth, forming “pockets” of infection. The
infection leads to loss of the bone that holds the
tooth in its socket and might lead to tooth loss. There
are often no warning signs of early periodontitis. Pain,
abscess, and loosening of the teeth do not occur until
the disease is advanced. Since periodontitis affects
more than just the gums, it cannot be controlled with
regular brushing and flossing. Periodontitis should
be treated by a periodontist (a gum disease specialist)
or by a general dentist who has special training in
treating gum diseases.
Diabetes mellitus is a systemic disease with
several major complications affecting both the
quality and length of l i fe. One of these
complications is periodontal disease (periodontitis).
Periodontitis is much more than a localized oral
infection. Recent data indicate that periodontitis
may cause changes in systemic physiology. The
interrelationships between periodontitis and
diabetes provide an example of systemic disease
predisposing to oral infection, and once that
infection is established, the oral infection
exacerbates systemic disease.
Material and methods
This was a prospective cross-sectional study carried
out during the period of July’07 to June’08. Two
ORAL HYGIENE AMONG TYPE 2 DIABETES PATIENTS:
A STUDY OF 276 CASES
KULSUM UMME1, MAHMUD A2, AZAM MG3, AHMED JU4, NAZIMUDDIN K5
Summary
It is thought that poor oral health is associated with type 2 diabetes mellitus (DM). There has been
relatively little data to date concerning oral health and periodontal disease with glycaemic status
among DM patients in our country. The purpose of this cross-sectional study was to investigate the
oral hygiene and periodontal status among type 2 diabetes patients and found that dental caries
and periodontitis are strongly associated with poorly controlled of DM.
1. Asociate Professor, Dhaka Dental College, Dhaka
2. Medical officer GHPD BIRDEM, Dhaka
3. Senior research Officer, GHPD, BIRDEM, Dhaka
4. Register Medicine ll, BIRDEM, Dhaka
5. Professor of Medicine BIRDEM, Dhaka
hundred and seventy six patients with type 2 DM
were studied. Clinical data like periodontitis,
gingivitis, dental carries, oral ulcer, periodontal
abscess were examined and baseline
characteristics were recorded. Fasting plasma
glucose (FPG), 2-h post-prandial glucose (PPG),
glycated haemoglobin (HbA1c) were estimated. The
mean of glycosylated hemoglobin measurements
(HbAlc) was used to indicate the long-term control
of DM. The study participants were divided into
well- (HbAlc <7%) and poorly- (HbAlc >7%)
controlled diabetics.
Results
Fig.-1: Patients with Periodontitis (n=101) and their
glycemic status
Bangladesh J Medicine 2010; 21 : 34-36

Of the 276 patients 141(51.0%) were male, age was
53.6 ± 10.9 years. Duration of DM was 9.6 7.1
years. The percentage of periodontitis, dental
carries, gingivitis, periodontal abscess, oral
candidiasis, glossitis, oral ulcer and leukoplakia
were 37.0%, 32.2%, 5.1%, 1.4%, 1.4%, 1.1%, 1.1%
and 0.7% respectively. A significantly increased
frequency of dental caries with poorer control of
diabetes was observed (p<0.001). The extent of
periodontitis also increased with poorer control
(p<0.001).
Discussion
In chronic periodontitis, the tooth supporting
structures (alveolar bone and the periodontal
ligament) are destroyed. The disease has a
multifactorial origin. Complexes of commensal oral
anaerobic bacteria and perhaps viruses are thought
to interact with risk factors, such as smoking,
diabetes and depression, to create the conditions
which make a person susceptible to periodontitis.
The patient’s immuno-inflammatory response to the
bacteria causes the tissue destruction which occurs
in chronic periodontitis.
It is useful to distinguish chronic gingivitis from
periodontitis. Chronic gingivitis is the very common
inflammatory reaction occurring in the gingival
tissues in response to the accumulation of dental
plaque. It usually precedes the development of
periodontitis, but chronic gingivitis does not
inevitably progress to periodontitis.
The relationship between diabetes, gingivitis and
periodontitis
Although periodontitis is a recognised complication
of diabetes, people with well-controlled diabetes who
have good oral hygiene are not at increased risk of
periodontitis. However, their susceptibility to
periodontitis is significantly increased when their
diabetes is poorly controlled, particularly if they also
smoke. Recent epidemiologic evidence shows that
the prevalence of diabetes in patients with
periodontitis is significantly greater (by two times)
than in people without periodontitis. The gingival
and periodontal signs which may alert the clinician
that the patient has previously undiagnosed diabetes
or that the patient’s diabetes is poorly controlled,
include:
• persistence of gingival inflammation after standard
periodontal treatment (thorough supra-and
subgingival scaling and cleaning, oral hygiene
instruction)
• severe gingival inflammatory response to plaque
and proliferation of gingival tissues at the gingival
margin
• continuing alveolar bone loss despite periodontal
treatment (fig. 3)
• simultaneous formation of multiple periodontal
abscesses fig. 4)
Fig.-2: Disease frequency of patients (Periodontitis -
37.0%)
Fig.-1: Patient with poorly controlled diabetes shows
extensive alveolar bone loss involving most teeth. The
destruction of bone has been rapid even though the patient
has been undergoing periodontal therapy.
35
BJM Vol. 21 No. 1 Oral Hygiene Among Type 2 Diabetes Patients: A Study of 276 Cases

Diabetes increases susceptibility to periodontitis
• Advanced glycation end products deposited in the
tissues as a result of hyperglycaemia can alter
the phenotype of macrophages and other cells via
a specific cell-surface receptor. Macrophages are
key cells in the pathogenesis of periodontitis
through their ability to produce a large array of
cytokines. They also influence the inflammatory
response, the metabolism of fibroblasts and
lymphocytes and stimulate bone resorption via
prostaglandin E2. It is thought that the advanced
glycation end products transform the macrophages
into cells with a destructive phenotype, producing
pro-inflammatory cytokines in an uncontrolled
fashion.
• Neutrophils are the primary defence cells of the
periodontium. The reduced neutrophil function
observed in patients with diabetes is therefore
another mechanism increasing the susceptibility
to periodontitis.
Relationship between periodontitis and the ability
to control diabetes?
While periodontitis is a recognised complication of
poorly controlled diabetes, it has been proposed that
severe periodontitis may make the metabolic control
of diabetes more difficult. The process may be
mediated through the systemic release of
inflammatory cytokines (e.g. TNF-á) from periodontitis
lesions, and chronic low-level systemic exposure to
Gram negative organisms. periodontitis may
contribute to elevated proinflammatory cytokines/
serum lipids and potentially to systemic disease
arising from chronic hyperlipidemia and/or increased
inflammatory mediators. These cytokines can produce
an insulin resistance syndrome similar to that
observed in diabetes and initiate destruction of
pancreatic beta cells leading to development of
diabetes. Thus, there is potential for periodontitis to
exacerbate diabetes-induced hyperlipidemia, immune
cell alterations and diminished tissue repair capacity.
What can the patient do?
• People with diabetes need to practise high
standards of daily oral hygiene, including
brushing and flossing.
• Adjunctive use of a chlorhexidine mouthwash
(0.12%) or chlorhexidine gel (0.2%) twice daily
(used independently of toothpaste so that the
chlorhexidine is not inactivated) may be useful
in controlling the more severe disease.
• Medical practitioners who suspect a patient has
diabetes-related gingivitis or periodontitis should
ensure that an early referral is made to a dentist.
Dentists in turn need to refer advanced or suspect
cases to a periodontist.
Therefore, Medical and dental practitioners need to
be aware of the interrelationship between poorly
controlled or undiagnosed diabetes mellitus and
chronic gingivitis and periodontitis. This is
particularly important because of the rising
prevalence of diabetes in the community.
References
1. Soskolne WA, Klinger A. The relationship between
periodontal diseases and diabetes: an overview. Ann
Periodontol 2001; 6: 91-8.
2. Bjelland S, Bray P, Gupta N, Hirscht R. Dentists,
diabetes and periodontitis. Aust Dent J 2002; 47:
202-7.
3. Mealy B. Position paper. Diabetes and periodontal
diseases. J Periodontol 2000; 71: 664-78. http://
www.per io .o rg/resources -products/pd f/ l r -
diabetes.pdf [cited 2004 March]
4. Grossi SG, Genco RJ. Periodontal disease and
diabetes mellitus: a two-way relationship. Ann
Periodontol 1998; 3: 51-61.
5. Papapanou PN. Periodontal disease: epidemiology.
Ann Periodontol. 1996; 1: 1-36.
6. Hugoson A, Thorstensson H, Falk H, Kuylenstierna
J. Periodontal conditions in insulin-dependent
diabetics. J Clin Periodontol 1989; 16: 215-223.
7. Thorstensson H, Hugoson A. Periodontal disease
experience in adult long-duration insulin-dependent
diabetics. J Clin Periodontol 1993; 20: 352-358.
Fig.-2: The lower left lateral incisor (*) is very mobile
and has migrated from its usual location in the arch. The
tooth has lost more than two-thirds of its supporting bone
because of periodontitis and abscess formation.
36
Oral Hygiene Among Type 2 Diabetes Patients: A Study of 276 Cases BJM Vol. 21 No. 1

Introduction:
Women mental health is an important issue now
days. The World Health Organization (WHO)
observed women mental health as their theme of
World Mental Health Day in 1996. Mental health is
not a priority and women mental health is much
neglected in Bangladesh. Majority of the people of
Bangladesh are living in the rural areas where
psychiatric services are not available. In these areas
people are not aware of the scientific management
of psychiatric problem rather these patients are
thought to have possessed by spirit or deity. In a
study it was found that even people near Mitford
Hospital in old Dhaka city were not still aware of
the availability of psychiatric services in that hospital1. Lack of awareness about the illness and proper
training of the physicians, low education, poor socio-
economic status, prevailing superstitious and stigma
of mental illness may be the strong reasons of these
beliefs.
1. Associate Professor, Department of Psychiatry, Bangabandhu Sheikh Mujib Medical University (BSMMU),
Shahbagh, Dhaka, Bangladesh.
2. Assistant Professor, Department of Psychiatry, BSMMU, Shahbagh, Dhaka, Bangladesh.
3. Medical Officer, Department of Psychiatry, BSMMU, Shahbagh, Dhaka, Bangladesh.
4. Research Assistant, Department of Psychiatry, BSMMU, Shahbagh, Dhaka, Bangladesh.
PSYCHIATRIC MORBIDITY AMONG WOMEN WHOSE
HUSBANDS ARE LIVING ABROAD
M A SALAM1, MOHAMMAD S. AHSAN2, NAFIA F. CHOWDHURY3. SYED F. SHAMS3, NAHID M. MORSHED1,
MOHSIN ALI SHAH1, MONIRUL ISLAM4
Abstract:
Introduction: A large number of people working aboard leave their wives home in rural areas of
Bangladesh. Husbands living abroad apart from their wives, play a significant role on the mental
health status of these married women. This study was carried out to see the Psychiatric morbidity
among those women whose husbands were living in aboard. Methods: This is a cross-sectional
study. A total number of 960 female patients came for psychiatric consultation in the out-patient
department of a private hospital from January 2008 to December 2009. Among them, 150 patients
were included in this study whose husbands were living abroad. Diagnoses were made as per
criteria of Diagnosis and Statistical Manual for Mental and Behavioral Disorder (DSM-IV). Results:
Majority of the patients (76.52%) were in 15-30 years of age group and most of the female were
house wives. Regarding socio-economic status 61.73% were lower middle and 13.04% were low
socio economic condition respectively. It was found that 51.30% of the patients were major depressive
disorder, 27.83% were somatoform disorder (0f which 13.04% had conversion disorder and 12.17%
had psychogenic headache), 06.08% were schizophrenic, 06.95% had bipolar disorder and 04.35%
had anxiety disorders. Conclusion: This study reveals significant number of women suffering from
psychiatric illness in rural areas. More emphasis should be given in psychiatric health care services
in primary health care level in Bangladesh.
Key words: Women mental health, Primary health care.
Recently several studies have reported worldwide
higher prevalence of some mental illness among the
women population. In an epidemiological study on
mental illness in Bangladesh, the prevalence of
psychiatric illness was found to be 16.1% and
depression was found to be 6.40% 2. In last few
decades there is an uprising trend of migration of
workers from rural and urban areas from the different
regions of Bangladesh. Majority of the workers are
unskilled and migrate mostly to Middle-East
countries. Most of the migrants are from low and
lower-middle income groups. They leave behind their
wives at home in villages of Bangladesh as wages
are very low. They stay on average for a period of 3-
5 years in abroad, keeping their wives and other
family members in the villages. From a study it was
found that the lack of some one to confide in acts
as a vulnerable factor for development of depression
in women in rural areas3.
Bangladesh J Medicine 2010; 21 : 37-40

The wives of the persons who migrated abroad for
jobs are the population of the present study. This
group of people dwells in poverty has poor education,
early marriage, adjustment problem and has lack of
social support. So, psychiatric assessment of these
women was done to see the psychiatric illness. This
study was carried out at a district level private
hospital in Comilla district, which is situated in the
eastern part of Bangladesh, 100 kilometer away from
Capital city Dhaka. This town lies in the adjacent
areas of Dhaka-Chittagong Highway and Dhaka-
Chittagong inter-district train has a stopover in this
town. The trend among many physicians in
Bangladesh is as such that specialist doctors on
weekly holidays (Friday) visits to the different areas
of other districts from major city especially from Dhaka
to deliver service. The patients also come to the town
on weekly holiday to take the specialists’ service.
Good communication network drags people from the
adjacent areas to come to and take the opportunity
of seeking medical help from the town. So, a good
number of patients come to seek specialist service
at weekend.
Methods:
This is a cross-sectional study. A total number of
960 new female patients came for psychiatric
consultations for the the first time to the out-patient
department of a private hospital from January 2008
to December 2009. Data were collected from the
registrar book of the patient. Out of 960 female
patients, 115 female patients were included in this
study whose husbands went abroad for job. These
patients were interviewed by a qualified psychiatrist
and psychiatric diagnoses were made as per criteria
of Diagnosis and Statistical Manual for Mental and
Behavioral Disorder (DSM-IV). The collected data were
cleaned, sorted and analyzed and the results were
presented in tables and figures.
Results:
Table. I showed that the majority of the patients
(76.52%) were in 15-30 years of age group followed
by 31-40 year (18.26%) of age group. Regarding
occupation most of the female were house wives
(95.65%). About 90.43% of the female are living the
rural areas. In Table II it was found that 47.82%
have primary education and 22.60% are illiterate.
Regarding socio-economic status 61.73% are lower
middle and 13.04% are low socio economic condition
respectively.
Table- I
Age distribution of the subjects (n= 115)
Age in years Number &
Percentage (%)
15-30 88 (76.52%)
31-40 21(18.26%)
41-50 06(5.22%)
50+ 00 (0%)
Table- II
Other sample characteristics of the subjects (n=115)
Sample characteristics No (%)
Residence Urban 11 (9.57%)
Rural 104(90.43%)
Occupation Housewife 110(95.65%)
Service 05(4.35%)
Others 00(0%)
Education Illiterate 26(22.60%)
Primary 55(47.82%)
Secondary 33(28.70%)
Higher 01(0.87%)
In Table III, it was found that 51.30% of the patients
were Major Depressive Disorder and 27.83% were
Somatoform Disorder (of which 13.04% had
Conversion Disorder and 12.17% had Psychogenic
Headache), 06.08% were Schizophrenic, 06.95% had
Bipolar Mood Disorder and 04.35% had Anxiety
Disorders.
Fig-1: Distribution of socio economic status of the
subjects
38
Psychiatric Morbidity among Women Whose Husbands are Living Abroad BJM Vol. 21 No. 1

Discussion:
The aim of this study was to find out the psychiatric
morbidity among female patients whose husbands
are doing jobs in abroad. Service delivery model of
mental health care in the low income countries like
in Bangladesh is to provide most of the formal mental
health care in primary mental health care settings
as suggested by the World Health Organization
(WHO). Consultations for complex cases and
inpatients can be managed in primary care center 4.
In many settings informal care is provided by the
families, other community resources and care by
traditional healers may assure central importance 5.
In Bangladesh, the first mental hospital was
established in Pabna, north to the capital of
Bangladesh as Mental Hospital Pabna. Besides, most
of the government medical colleges in Bangladesh
are situated in urban cities and have their psychiatric
departments with either outpatient or both out and
inpatient facilities. Mental health care is not
incorporated in the primary care setting in
Bangladesh. So majority of Bangladeshi who are
residing in rural areas that need specialist mental
health services are inaccessible to the government
mental health facilities. With this existing reality in
this country, an alternate service model is growing
up. That is, the specialists residing in urban areas
come to the upazilla (previously known as thana) and
district town to deliver specialist mental health
service in weekly holidays (Friday).Thereby, providing
some form of mental health care in the primary care
level.
In present study, the highest numbers of psychiatric
patients were in age group 15-30 years (76.52%), which
was consistent with other studies like, in a study
done to see the diagnostic criteria group attending in
satellite consultation services in rural area and it
was seen that 30.57 % of the females were of 21-30
year age 6. Regarding psychiatric morbidity it was
observed that about 58.26% of the patients were
suffering from the Mood Disorder. Of them 51.30 %(
59) were suffering from Major Depressive Disorder.
Researchers have found in a study that depression
was twice as common as in men. The reasons for the
difference have been hypothesized to involve hormonal
differences, the effects of child birth, differing
psychosocial stressors for women 3. Another study
done in Bangladesh showed that 51.59 % were
suffering from Mood Disorder, 16.18 % were suffering
from Anxiety Disorder, 12.66 % Somatoform Disorder,
12.14 % were Schizophrenia which was very much
close to this study 7 .
The reason for the high percentage of depression
among women in Bangladesh can be explained in
many ways. Women in rural areas in Bangladesh have
to take a major role in household activities. In
addition they marry early, have to take of more than
Table- III
Distribution of psychiatric illness among the subjects (n=115)
Types Subtypes Frequency Percentage
Schizophrenia and other Schizophrenia 2 07 6.09%
psychotic disorders Delusional disorder 1
Brief psychotic disorder 4
Mood disorders Major depressive disorder 59(51.30%) 67 58.26%
Bipolar disorder 8(06.95 %)
Anxiety disorders Generalized anxiety disorder 1 05 4.35%
Panic disorder 1
Specific and Social phobia 1
Obsessive compulsive disorder 2
Somatoform disorders Conversion disorder 15(13.04%) 32 27.83%
Somatoform disorder NOS 3
Psychogenic headache 14(12.17 %)
Adjustment disorder 2 02 1.74%
Organic disorder Migraine
Seizure disorder 11 02 1.74%
39
BJM Vol. 21 No. 1 Psychiatric Morbidity among Women Whose Husbands are Living Abroad

2 to 3 children at home. They are the victim of many
maladjustment problems. High level of uneducated
women is also assumed to be associated with low
skill as well as poor coping mechanism. These factors
altogether perhaps play role in precipitating psychiatric
problems 3.
In Bangladeshi culture women are less rewarded for
their contribution in spite of their hard work and
contribution in the families. In this study the
husbands of the respondents were staying abroad
and used to come back home very seldom. Moreover,
having care of children 03 or more age below 14 is
vulnerable for depression. This could be a major factor
for the high rate of depression among the
respondents. Deprivation of mental support from the
spouse and deprivation of physical needs may play a
major role in causation of depression. It was also
observed that about 27.83% of the respondents were
suffering from Somatoform disorder. It included
conversion disorder 13.04% and psychogenic
headache 12.17%. Majority of the patients were of
age 15-30 years. This age group is very significant in
our cultural background. Early marriage, conflict in
social circumstances, social stigma all contribute to
produce physical symptoms of above diseases.
Schizophrenia and Bipolar Mood Disorder were
06.09%, and 06.96% respectively. Adjustment disorder
was 1.74% and Anxiety disorder 4.35%.
Conclusions:
This study showed that psychiatric morbidity among
the female patients is very considerable. It is a global
problem including Bangladesh. We know that
majority of the female psychiatric patients do not come
to the psychiatrists or hospital for treatment.
However this significant proportion of female
psychiatric patients indicates that there is an urgent
need to provide psychiatric services in all district level
hospital in Bangladesh.
References:
1. Rahim DA, Banu NM, Islam H. Female psychiatric
morbidity in out patient of Mitford Hospital.
Bangladesh J Psychiatry 1997; 11: 17-20.
2. Firoz AHM, Karim ME, Alam MF, Rahman AHMM,
Zaman MM. Prevalence, Medical Care, Awareness
and Attitude Towards Mental Illness in Bangladesh.
Bangadesh J Psychiatry 2006; 20(1): 9-36.
3. Ara N, Hossain GM, Islam MT. Women mental health
in rural part of Bangladesh. Bangladesh J Psychiatry
2001; 15: 5-10.
4. Mubbashar M. Mental health services in rural
Pakistan. In M. Tansellaand G. Thornicroft (eds).
Common Mental Disorders in Primary Care. London:
Routledge; 1999: 67-8.
5. Desjarlais R, Eisenberg L, Good B. World Mental
Health. Problems and priorities in law income
countries 1995; Oxford: Oxford University Press.
6. Alam F, Hamid A, Ahmad S, Ahsan MN, Diagnoses
of patients: An Observation in Psychiatric
Consultation services in rural Bangladesh,
Bangladesh Journal of Psychiatry 2000; 14:6-9.
7. Hamid A, Choudhury S, Nizamuddin M, Mohit MA,
Comparative study of patients in different outpatient
departments (OPDS) and pattern of Psychiatric
disorders in a district Hospital, Bangladesh Journal
of Psychiatry 2003;17:5-13.
40
Psychiatric Morbidity among Women Whose Husbands are Living Abroad BJM Vol. 21 No. 1

Introduction
Infectious complications after renal transplantation
(RT) may lead to prolonged hospitalization, sepsis,
and death 1,2. The majority of infections appear to be
due to gram-negative bacteria associated with urinary
tract infection or deep wound infection 3,4. Fungal
and other opportunistic infections may also occur 2,5,6.
Despite the propensity for infection in these patients,
reports of septic arthritis have been uncommon. We
report a case of septic arthritis in a renal transplant
recipient on immunosuppressive therapy who
responded well after prolong parenteral antibiotic
therapy.
Case Report
A 35-year-old man with a history of chronic
glomerulonephritis and resultant End-stage renal
disease had a renal transplant from a live related
donar in April, 2009. Prior to transplantation he was
on MHD for 5 months. He had an uncomplicated
postoperative course. Immunosuppressive treatment
included prednisolone, cyclosporine and
mycophenolate mofetil.
The patient did well until late September 2009, when
he began to experience. Continued fever along with
rigors, malaise, myalgia and night sweats that
responded little to antipyretics. A dry cough began 10
SEPTIC ARTHRITIS IN A RENAL TRANSPLANT
PATIENT
PRADIP KUMAR DUTTA1, SAYED MD JABED2, SAIBAL DAS3, MD NURUL HUDA3, MD MAMINUL ISLAM4 ,
DIPEN CHOWDHURY4,MD SHARIFUL ISLAM4, ABUL KASHEM1, DIPTI CHOWDHURY5
Abstract
Infectious complications in the renal transplant patient are common but the incidence of septic
arthritis in transplant patient is less documented. The knee was most commonly infected joint. We
report a case of monoarticular septic arthritis in a renal transplantation recipient. The ankle joint
was involved in our case. Septic arthritis may be missed as other rheumatological disorders may
mimic in transplant patient. If proper attention is not given to locomotor system it may not be
diagnosed early. Besides as pt is on immunosuppressive therapy prolonged antibiotic therapy is
warranted. Prompt and prolonged antibiotic therapy resulted in quick resolution of the joint infection
in our patient. Impaired host defenses, possible inadequate and delayed prior antibiotic therapy,
and intrinsic joint alterations are potential contributing factors to the development of septic arthritis
following renal transplantation. So in spite of the low frequency of occurrence of septic arthritis,
persistent attention to the locomotor system in the transplant patient is warranted.
1. Associate Professor of Nephrology, Chittagong Medical College
2. Honorary Medical Officer. Nephrology, Chittagong Medical College
3. Assistant Professor of Nephrology, Chittagong Medical College
4. MD (Nephrology) Thesis part student, Chittagong Medical College
5. Professor of Nephrology, Chittagong Medical College
days later which became productive with purulent
sputum with occasional haemoptysis within the next
week. The scenario was further complicated by
development of pain and swelling in the right ankle
joint without any history of trauma 10 days prior to
admission. Bowel and bladder habit was normal
throughout the course. He was non diabetic with no
previous history of tuberculosis, joint symptoms or
recent skin infection. Treatment with several oral
antibiotics failed to control symptoms. His
immunosuppressive therapy consisted of prednisone
15mg, cyclosporine 175 mg and mycophenolate mofetil
1 g daily. When the patient was admitted to our
institution for evaluation and treatment on 1st October
2009, he was found ill-looking and distressed with
frequent purulent cough. His pulse was 130/min, BP-
100/70mm (Hg), temp-1030F and Respiratory rate-25/
min, mildly anaemic with normal JVP. Chest
examination revealed creps on the left upper area.
Red, hot, swelled right ankle had Grade-III tenderness
with limited active and passive movements.
Otherwise, the results of his examination were
normal, and his transplanted kidney was not tender.
Initial investigation showed Hb-10.1g/dl with WBC-
25000/cm3, CXR showed left upper zone
consolidation.
Bangladesh J Medicine 2010; 21 : 53-54

In view of the above clinical and laboratory data, the
patient was diagnosed as a case of pneumonia and
septic arthritis and empirical parenteral antibiotic
treatment commenced with Inj.Meropenem,
inj.Flucloxacillin, inj.Metronidazole without stopping
immunosuppessive treatments. Cough disappeared
within 7 days with resolution of creps but intermittent
fever persisted along with joint symptoms till 20th
day of treatment and then gradually settled down.
Patient became symptom free from 25th day onwards.
Parenteral antibiotics were continued for 28 days.
Follow up investigations revealed resolution of
consolidation while CBC revealed WBC-12600/cm3
on 20th day of treatment. He was discharged on 3rd
December.
Discussion:
Bacterial, fungal, mycobacterium, and viral infections
have been well documented in RT patients 2,3,6,7,8.
Bacteria are the major cause of infections, which
usually occur in the urinary tract, although
septicemia, skin, and wound infections are common1,3,4 .Recent series from different institutions, 50
(29%) of 174 and 164 (32%) of 518 RT patients
developed infections 4,6.
In contrast, despite the high frequency of these other
infections, the incidence of septic arthritis appears
quite low. In one series, bomalaski et al reported only
6 of 800 transplanted patients developed septic
arthritis. and in 11 reported studies of RT patients
covering the period from 1964 through 1980, only 1
case of septic arthritis in 1,033 patients was reported4,5,7. E coli, Enterococcus, S marcescens, P
aeruginosa, M tuberculosis and atypical mycobacterial
organisms are common bacterial etiology7. Fungus
Cryptococcus and CMV were reported 2,8,9. In all
series, knee was the most common site of infection.
Synovial fluids commonly showed WBC within 40000-
70000/cm3 with PMN predominance and raised
peripheral WBC count 7,8,10,14. Most responded to
antimicrobials and aspirations, open drainage and
arthrotomy were required in some cases mainly in
mycobacterial etiology.7,11,12,13
Our patient had ankle arthritis which was not
commonly found in other studies 7,9,11,14 .But he
presented 6 month post transplant which was close
to the median time of presentation (5.5 months) and
also had immunosuppressive therapy and concomitant
chest infection as predisposing agents. High
peripheral WBC counts further supported the
diagnosis and respond to antibiotics suggested
bacterial infection though organisms could not be
identified. Joint and systemic symptoms
concomitantly disappeared along with normalization
of WBC count and relapses not occurred yet.
Conclusion:
Infections are common in RT patients; however,
infectious arthritis occurs infrequently. Reinfection
or relapsing infection may occur despite an apparently
adequate regimen of antibiotic therapy. If not treated
early, it may lead to open drainage, arthrotomy and
amputation. But early diagnosis and proper
antimicrobial therapy can alone effective as in our
patient. Immunosuppressives need not to withdraw
to clear the infection.
References:
1. Ramos E, Karmi S, Alonzi SV, Dagher FJ: Infectious
coinplications in renal transplant recipients. South
Med J 1980; 73:751-754.
2. Biaf ZF, Altmann G, Ostfield E: Fungal infections
after renal transplantation. Isr J Med Sci 1976;
12:674-677.
3. Eickhoff TC: Infectious complications in renal
transplant recipients. Transplant Proc 1973;
3:1233-1238.
4. Lobo PI, Rudolf LE, Krieger JN: Wound infections
in renal transplant recipients-a complication of
urinary tract infections during allograft malfunction.
Surgery 1982; 92:491-496.
5. Myerowitz RL, Medeiros AA, O’Brien TF: Bacterial
infection in renal homotransplant recipients: a study
of fifty-three bacteremic episodes. Am J Med 1972;
53:30.
6. Peterson PK, Ferguson R, Fryd DS, Balfour
HH,Rynasiewicz J, Simmons RL: Infectious diseases
in hospitalized renal transplant recipients: a
prospective study of a complex and evolving problem.
Medicine (Baltimore) 1982; 61:360-372.
7. Bomalasky JS, Williamson PK, Goldstein CS:
Infectious Arthritis in renal transplant
patient.Arthritis & Rheumatism 1986; 29:227–232.
8. Friedman HM, Pincus T, Gibilisco P, Baker D,
Glazer JP, Plotkin SA, Schumacher HR Jr: Acute
monoarticular arthritis caused by herpes simplex
virus and cytomegalovirus. Am J Med 1980; 69:241-
247.
9. Lefl RD, Smith EJ, Aldo-Benson MA, Aronoff
GR:Cryptococcal arthritis after renal
transplantation. South Med J 1981;74: 1290.
10. Irby R, Edwards WM, Gatter R: Articular
complications of homotransplantation and chronic
renal hemodialysis.J Rheumatol 1975;2: 91-99.
11. Ascher HL, Simmons RL, Marker S, Klugman
J,Najarion JS: Tuberculous joint disease in
transplant patients. Am J Surg 1978; 135:853-856
12. Bomalaski JS: Rheumatologic manifestations of
atypical mycobacteria (abstract). Arthritis Rheum
(suppl) 1983;26: S48.
13. Hall MC, Elmore SM, Bright RW, Pierce JC, Hume
DM: Skeletal complications in a series of human
renal allografts. JAMA 1969; 208: 1825-1829.
14. Vincenti F, Amend WJ, Feduska NJ, Salvatierra 0:
Septic arthritis following renal transplantation.
Nephron 1982; 30:253-256.
54
Septic Arthritis in a Renal Transplant Patient BJM Vol. 21 No. 1

Introduction
Vitiligo is an acquired pigmentary anomaly of the skin,
manifested by depigmented white patches surrounded
by a normal or a hyperpigmented border. Vitiligo
usually begins in childhood or young adulthood;
approximately one half of those with vitiligo acquire
the disease before the age of 20 years, and the
incidence decreases with increasing age. The
prevalence of the disease ranges from 0.5% to 1%.
All races and both sexes are equally affected 1.
Histologically melanocytes are completely absent in
the vitiliginous patches and usually there is no
inflammatory component1. Recently, research at the
molecular level has demonstrated deficiency of
antioxidant substances in vitiliginous skin. This leads
to cytotoxic action of reactive oxygen species such
as, super oxide anion and hydroxyl radical which are
generated by the ultraviolet damaged epidermis. The
free radicals are also cytotoxic to melanocytes and
inhibit tyrosinase 2.
SERUM ZINC LEVEL IN PATIENTS WITH VITILIGO IN
A TERTIARY HOSPITAL IN BANGLADESH
RUBAIYA ALI1, NARGIS AKHTAR 2, MOHAMMAD S. AHSAN3, AYESHA HASSAN4, MOHAMMAD ASIFUZZAMAN5
Abstract
Background: Vitiligo is a common and chronic skin disease in dermatological practice. It is found that
there is deficiency of anti-oxidant substances in vitiliginous skin. Zinc is considered as an anti
oxidant and also plays an important role in the process of melanogenesis. So far, studies have
shown a variation in zinc level in patients with vitiligo. Objective: The present study was done to
see the serum zinc level in patients with vitiligo. Methods: Total 30 patients with vitiligo were
purposively taken from the department of Dermatology and Venereology of Bangabandhu Sheikh
Mujib Medical University (BSMMU) and 30 healthy controls were taken and zinc level was estimated
in both groups. The duration of the study was six months from 1st September 2007 to 29th February
2008. Results: The study result showed that mean zinc level of vitiligo patients were 1.06 ± 0.08
and that of controls were 0.91± 0.33. Mean zinc level in both groups was found within normal
reference range. However, In vitiligo patients mean zinc level was observed higher than that of
controls. This difference was found statistically significant (p<0.05). Conclusion: In this study
serum zinc level in patients with vitiligo was found within normal range and higher than that of
control. However, further studies with larger sample size may give a more significant relation of
serum zinc and vitiligo.
Key words: Vitiligo, serum zinc.
1. Assistant Professor, Department of Dermatology and Venereology, Ad-Din Medical College and Hospital,
Dhaka.
2. Associate Professor, Department of Dermatology and Venereology, Bangabandhu Sheikh Mujib Medical
University (BSMMU), Dhaka.
3. Assistant Professor, Department of Psychiatry, BSMMU, Shahbagh, Dhaka..
4. Assistant Professor, Department of Dermatology and Venereology, Delta Medical College and Hospital,
Mirpur, Dhaka.
5. Assistant Professor, Department of Dermatology and Venereology, ZH Sikder Women’s Medical College
and Hospital.
Zinc is a trace element and its essentiality is related
mainly to its function as the metal moiety of the
important enzymes. Zinc is considered as an
antioxidant because the extracellular enzyme
superoxide dismutase is zinc dependent. Superoxide
dismutase is a group of metalloenzymes that protect
cells from the toxic effects of super oxide radicals3.Zinc also plays an important role in the process of
melanogenesis4. Thus zinc has a significant role in
the pathogenesis of vitiligo. In India Shameer et al5
found some interesting correlations between low zinc
levels and vitiligo. Similar finding was observed in
Germany 6. But Helmy et al7 found that serum Zinc
and copper levels were significantly higher in active
vitiligo patients than controls. So, there is variation
of serum zinc level among patients with vitiligo.
However, no such studies were carried out in
Bangladesh.
Bangladesh J Medicine 2010; 21 : 14-18

Methods
This was a case control study. Sampling technique
was purposive. Sample size (n) was 60 (30 case, 30
control). This study was conducted in the
Department of Dermatology and Venereology,
BSMMU, Shahbagh, Dhaka, Bangladesh. The study
period was of six months (1st September 2007 to
29th February 2008). Patients of vitiligo of any age
and both sexes were selected as cases. As controls,
age and sex matched healthy individual who were
not on any form of zinc medication were included.
However, patients having leukoderma secondary to
other causes, or history of suffering from other
obvious skin diseases, or undergoing treatment
with Zn or any history of zinc intake for 04 months
prior to this study, or suffering from any other
systemic diseases such as, cirrhosis of liver, viral
hepatitis, neoplastic condition, myocardial
infarction, steatorrhoea and renal failure were
excluded from the study. Patients who were
pregnant or consuming oral contraceptive pills were
also excluded.
Patients were diagnosed clinically and Wood’s lamp
examination was carried out to confirm it. Informed
written consent was taken from every one. A
questionnaire consisting of particulars of the
participants, socio-demographic data, clinical data
and laboratory findings was used. 5 ml of venous
blood was collected from both case and control
group in special sterile tubes and was centrifuged
for 15 minutes at 2000 rpm (Rotations per minute).
The supernatant serum was transferred to a
separate sterile tube (Appendorf tube) and kept at
-20 0 C in the deep freezer till the analysis. The
serum zinc level was measured by ‘Atomic
absorption spectrophotometry (AAS) [Flame
method] at Centre for Advanced Research in
Physical Chemical, Biological and Pharmaceuticals
Sciences, University of Dhaka.Data was checked
for inadequacy, irrelevancy, and inconsistency.
Irrelevant data were discarded. For the statistical
analysis, one Microsoft Windows- based software
package was used (SPSS 13 for Windows, SPPS
Incorporation, Chicago, IL, USA). Data process on
categorical scale was presented as frequency and
percentage and was analyzed by c2 tests. While
the data present on continuous scale was
presented as mean and SD and analyzed with the
help of Student ‘t’ test (Unpaired). Statistical
significance is set at 0.05 level and confidence
interval at 95% level.
Results
The mean age of the case group patients was 30.27
years with a standard deviation of ±11.09 and that in
controls 32.27 years with a standard deviation of
±11.08. As it was an age and sex matched study, so
distribution of respondents within different age
ranges were kept in equal number (Table-I).
Table-I
Distribution of the respondents by mean age and
standard deviation of both groups (n = 60)
Age (year) Group P value*
Case Control
11-20 18.00±1.73§ 19.40±.89 0.147
21-30 26.07±3.31 27.31±2.06 0.259
31-40 37.50±2.08 35.17±3.31 0.250
41-50 46.25±1.5 47.50±3.79 0.562
51-60 51.00±.0 57.50±3.54 0.122
Total 30.27±11.09 32.27±11.08 0.555
§ Mean ± Standard deviation
* Unpaired t test was used to measure the level of
significance. p value <.05 was considered as a level of
significance
Most of the participants were in the age group of 21-
30 (50%) (Table-II).
No significant difference was observed between groups
in term of frequency distribution of respondents in
different age groups (p>0.05) (Table-II).
Table II
Distribution of the respondents by frequency of age of
both groups (n = 60)
Age (year) Group p value*
Case Control
11-20 5 (16.7)# 5 (16.7)
21-30 15 (50.0) 15 (50.0)
31-40 4 (13.3) 4 (13.3) 0.969
41-50 4 (13.3) 4 (13.3)
51-60 2 (6.7) 2 (6.7)
Total 30 (100.0) 30 (100.0)
# Figure within parenthesis denoted corresponding
percentage.
* Chi square test was used to measure the level of
significance. p value <0.05 was considered as a level of
significance
15
BJM Vol. 21 No. 1 Serum Zinc level in patients with Vitiligo in a Tertiary Hospital in Bangladesh

Female respondents outnumbered their male
counterpart and male and female ratio is 1:1.7.
25 (83.3%) among the cases were nonsmoker, 04
(13.3%) smoker and 01 (3.3%) ex-smoker. However
among controls the numbers were 23 (76.7%), 5
(16.7%) and 2 (6.7%) respectively. No statistical
significance difference was found in term of smoking
habit of both groups (p>0.05).
Table III
Features of vitiligo patients (n=30)
Frequency Percent
Distribution
• Symmetrical 14 46.7
• Asymmetrical 16 53.3
Morphological pattern
• Localized or focal 18 60.0
• Acrofacial 5 16.7
• Generalized 7 23.3
Koebner sign 10 33.3
Itching over patches 7 23.3
Scaling 3 10.0
Table IV
Distribution of the respondents of both case and control
group by serum Zn level (n=60)
Zinc level Mean±SD (mg/L) p value*
Case 1.06±0.08 0.014
Control 0.91±0.33
* Unpaired‘t’ test was done to measure the level of
significance.
Only 04 (13.4%) patients had positive family history
of vitiligo (Fig-I).
Fifteen (50%) patients had 1-5 depigmented patches
and 08 (26.7%) patients had 6-10 patches, 04 (13.3%)
had 11-15 numbers of patches and 03 (10%) patients
had 16-20 no of patches. (Fig-III).
Fig.-I: Family history of Vitiligo among the case group (n=30)
Twenty one patients (70%) had been suffering for 1-
5 months; whereas, 07 (23.4%) patients for 6-10
months, patients (3.3%) for 11-15 months and one
patient (3.3%) had illness for 16-20 months of illness
(Fig-II).
Fig.-II : Duration of illness of the patients (n=30)
Fig.-III: Depigmented white patches of the patients
14(46.7%) patients had symmetrical distribution of
vitiligo patches and 53.3% had asymmetrical
distribution. Localized or focal pattern vitiligo was
observed more. Eighteen (60%) patients had localized
or focal pattern vitiligo followed by 7 (23.3%)
generalized pattern and 5 (16.7%) had acrofacial
pattern. Ten (33.3%) patients had koebner sign, 7
(23.3%) patients had itching over patches and 3
(10.0%) patients had scaling (Table-III).
Mean zinc levels of both case and control groups were
within normal reference level. In vitiligo patients mean
zinc level was observed higher than that of control
group. Mean serum zinc level in case group was
1.06±0.08 and in control group was 0.91±0.33. This
16
Serum Zinc level in patients with Vitiligo in a Tertiary Hospital in Bangladesh BJM Vol. 21 No. 1

difference was found statistically significant
(Table-IV).
Discussion
Zinc is categorized as a trace element as it
constitutes less than 0.005% of total body weight.
Normal serum zinc level ranges from 0.7-1.6 mg/L 8.
No statistically significant difference in mean values
of serum zinc levels was observed in relation to sex,
age, race, food habits and diurnal variation. Zinc is
an integral part of as many as 40 metalloenzymes. It
takes part in virtually all body functions from
spermatogenesis to growth to abstract thought
processes. Zinc deficiency characteristically causes
the cutaneous disorder of acrodermatitis
enteropathica manifestating as acral and periorificial
skin eruptions, alopecia, diarrhoea and growth
retardation. Some zinc investigators have also
reported low serum zinc levels in cutaneous leg ulcers
etc, while others have not found the same. Some
authors have found abnormalities of serum zinc level
in cutaneous disorders like psoriasis and lichen
planus9. In our study zinc level was found significantly
higher in vitiligo patients than controls. This finding
was not agreed with the finding of Shameer et al 5
(Zinc level was found reduced in 13of 60 patients -
26.6%).But Helmy et al7 aimed in his study to evaluate
whether the activity of the disease was associated
with a systemic oxidative stress manifested as
apoptosis of Peripheral Blood Mononuclear Cells
(PBMC) and also aimed to evaluate the role of Zinc
and copper in the pathogenesis of vitiligo. They found
that serum Zinc and copper levels were significantly
higher in active vitiligo patients than controls due to
higher percentage of apoptotic PBMCs in active vitiligo
with increased release of zinc and copper in serum.
Their results also confirmed that a systemic oxidative
stress had a role in active vitiligo leading to
melanocyte degeneration.
Serum zinc levels were studied in 75 patients of
different cutaneous disorders and 24 healthy controls
by Arora et al9. No significant correlation was found
in the cutaneous disorders studied i.e. vitiligo and
aphthous ulcers where serum zinc levels were found
to be 97.3 ±26.6 ì gm/100 ml and 105.2 ± 23.5 ìgm/
100 ml respectively.
In this study, mean age of the case group patients
was 30.27 years with a standard deviation of ±11.09
and in control group 32.27 years with a standard
deviation of ±11.08. As it was an age and sex matched
study, so distribution of respondents within different
age ranges were kept in equal number. Maximum
respondents of the case and control groups were
within 21-30 years age range (50.0 vs. 50.0) followed
by 11-20 years (16.7 vs. 16.7). This result was
comparable with Shameer et al 5. Mean age of their
respondents was 33.8 years. Male and female ratio
of their series was 4.5:1. But in our series it was
1:1.7.
Within case group only 04 (3.4%) patients had positive
family history of vitiligo. In Shameer et al 5series
33% of the patients had positive family history of
vitiligo.
Mean duration of suffering from vitiligo was 5.0
months with a standard deviation of ±3.79 months.
Maximum patients (70.0%) had been suffering from
vitiligo for 1 to 5 months.
Mean duration of suffering from vitiligo was 2 years
in Shameer et al series5.
Conclusion
In some earlier studies variable degree of correlation
between serum zinc
level and vitiligo were observed. In a recent study
conducted in India has shown low level of serum zinc
is a significant risk factor for vitiligo 4. But this study
on the contrary showed significant higher level of
serum zinc in vitiligo patients than that of controls.
Limitations of the study
• Sample number was small.
• Period of study was short.
• Confounders were not addressed.
• As purposive sampling was done, findings were
not free from biasness.
Recommendation
• Study with longer duration should be carried out
with larger sample size.
• Multicenter study should be carried out to reveal
accurate pattern of zinc status in vitiligo.
References:
1. Odom RB, James WD, Berger TG, (eds). Andrews’.
Diseases of the Skin. Clinical dermatology, 10th ed.
W.B. Saunders Company, Philadelphia. pp. 860-3.
2. Schallreuter KU, Wood JM, Berger J. Low catalase
levels in the epidermis of patients with vitiligo.
Invest Dermatol 1991; 97:1081-5.
17
BJM Vol. 21 No. 1 Serum Zinc level in patients with Vitiligo in a Tertiary Hospital in Bangladesh

3. Yildirim M, Baysal V, Inaloz HS, Can MM. The role
of oxidants and antioxidants in generalized vitiligo
at tissue level. J Eur Academ Dermatol Venereol
2004; 18:683-6.
4. Prasad AS. Zinc: An overview. Nutrition 1995;
11:93-99.
5. Shameer P, Prasad PVS, Kaviarasan PK. Serum zinc
level in vitiligo case control study. Letter to Editor,
Ind J Dermatol Venerol Leprol 2005; 71(3):206-7.
6. Bruske K, Salfeld. Zinc and its status in some
dermatological diseases- a statistical assessment
(Article in German) Z Hautkrn 1987; 62 (S-1): 125-
31.
7. Helmy MI, Gayyar MAE, Hawas S, Eissa EA. Role
of oxidative stress in the pathogenesis of vitiligo. J
Pan-Arab League of Dermatologists 2004; 15(2):97-
105.
8. Scottish Trace Element and Micronutrient Reference
Laboratory.
9. Arora PN, Dhillon PS, Rajan SR, Sayal SK, Das AL.
Serum zinc levels in cutaneous disorders. Medical
J Armed Forces India. 2002; 58(4): 304-6.
18
Serum Zinc level in patients with Vitiligo in a Tertiary Hospital in Bangladesh BJM Vol. 21 No. 1

Introduction
Acute liver failure is defined as the presence of acute
liver disease associated with significant coagulopathy,
which has been arbitrarily defined by a prothrombin
time or factor V level of less than 50% of normal.
Fulminant hepatic failure is acute liver failure
associated with hepatic encephalopathy developing
within 8 weeks of illness.1 It is a multiorgan failure
syndrome with dramatic clinical features and often
fatal outcome. Acute viral hepatitis is the most
common cause.2 Others are drugs, chemical, poisons,
ischemia, hypoxia and metabolic abnormality.3
Histologically it is characterized by massive
parenchymal necrosis. Altered mental status
accompanied by jaundice is a hallmark of acute liver
failure. Most patients with fulminant hepatic failure
demonstrate features of multiorgan failure including
shock, renal failure, respiratory distress syndrome
and infection. Since there is no specific treatment
with proven efficacy, the principle of therepy in acute
STUDY ON AETIOLOGY AND OUTCOME OF
FULMINANT HEPATIC FAILURE IN BANGLADESHI
PATIENTS
SWADESH KUMAR CHAKROVORTTY 1, RAJIB BARUA 2, DEWAN SAIFUDDIN AHMED3, MOHAMMAD ABUL
KALAM AZAD4, ABU BAKAR SIDDIQUE5, MD. ABUL KALAM AZAD 6
Abstract
Fulminant hepatic failure is although uncommon but not rare in Bangladesh. It is the severe form of
acute hepatitis. This study was done to know the clinical presentation, aetiological background,
various complications and outcome of fulminant hepatic failure in Bangladesh. Total 28 patients
were included in the study, of them 71% were female and 29% were male. Half of the total patients
were in the age group of 16-25 years. Among the female patients 7 (35%) patients were pregnant.
The chief symptoms were jaundice, anorexia, nausea, vomiting and encephalopathy and 25%
developed bleeding manifestations. 19% patients developed renal failure, 40% had hyponatraemia
and 15.7% had hypoglycaemia. The known causes were hepatitis E virus (45.8%), hepatitis B virus
(25%), hepatitis A virus (4.1%) and antitubercular drugs (Isoniazide/Rifampicin) in 7.1% cases.
Pregnancy appears to be a risk factor for HEV induced fulminant hepatic failure. Prolonged
prothrombin time and raised serum bilirubin level were important prognostic factors but grade of
encephalopathy failed to be proved as a prognostic factor. Thereby improving sanitary facilities,
active immunization against HBV and HAV can prevent the incidence of fulminant hepatic failure
and close monitoring of renal function, serum electrolytes and blood glucose can reduce significant
mortality.
Key words: Fulminant hepatic failure, aetiology, outcome
1. Registrar, Cardiology Department, NICVD
2. Medical officer, Gastroenterology Department, BSMMU.
3. Associate Professor, Department of Gastroenterology, BSMMU.
4. Medical officer, Department of Medicine, BSMMU.
5. MD Gastroenerology( Thesis ),BSMMU.
6. Associte Professor, Department of Medicine, BSMMU.
liver failure includes intensive care for maintenance
of blood glucose, serum electrolytes and other
biochemical parameters and supportive therapy for
complications.4 Hepatic transplantation is considered
for patients reaching grade III or IV encephalopathy
due to FHF. The prognosis depends on aetiology, level
of consciousness at presentation and prothrombin
time. In FHF the hepatic pathology is potentially
reversible and survivors usually recover completely.1
The aims and objectives of the study were to evaluate
the clinical features, complications, prognostic
indices and outcome of fulminant hepatic failure in
Bangladeshi patients. Also to find out the aetiology
of the disease and to compare its features with that
of other studies at home and abroad.
Materials and methods
This study comprised of 28 patients with fulminant
hepatic failure of whom 20 were female and 8 were
male patients. The patients were collected from
different units of medicine wards (n=27) and pediatric
Bangladesh J Medicine 2010; 21 : 29-33

ward (n=1) of Dhaka Medical College Hospital from
January 2005 to January 2006. History taking and
physical examination of each patient were done
properly and was recorded in a printed data sheet.
During physical examination attention was given to
find out the stigmata of chronic liver disease to
exclude preexistent liver disease. Biochemical,
hematological investigations were done to establish
the diagnosis and for prediction of prognosis and
development of complications. Viral markers for
hepatitis A, B. C and E were done to find out the
aetiology. Patients were treated by supportive therapy
and followed up in the ward till they recovered or
expired. Improvements were assessed clinically
(reduction of jaundice, increase in liver span and
improvement of grade of encephalopathy) and
biochemically (by S. bilirubin, prothrombin time). The
mean duration of follow up was 3±1 week.
Data were entered systematically into computer with
Microsoft Excel and the test statistics used to analyze
the data were descriptive statistics.
The study was approved by the ethical review
committee of the institution.
Results and observations
Total 28 patients of fulminant hepatic failure were
selected for the study. 14 (50%) patients were in the
age group of 16-25 years and 7 (25%) patients were in
26-35 years. (Figure1). 20 (71%) patients were female
and the rest 8 (29%) patients were male. The male to
female ratio was 2:5 (Figure2). Among the female
patients 7 (35%) patients were pregnant.
Regarding the duration of illness from the onset of
jaundice to the time of presentation, 12 (42.8%)
patients presented within 7 days, 8 (28.5%) patients
from 8th to 14th day, 5 (17.8%) patients from 15th to
21st day and the rest 3 (10.7%) patients presented
from 22nd to 28th day.
All patients presented with jaundice with anorexia,
nausea, vomiting and encephalopathy. 7 (25%)
patients developed bleeding manifestations in the
form of haematemesis, melaena, haematuria or
pervaginal bleeding. 6 (21.4%) patients had
hepatomegaly and fever. 4 (14.2%) patients had
ascites. Table 1 showing the presenting features of
the patients
Table-I
Presenting features of the patients (n=8)
Features Number of patients Percentage
(n=28)
Jaundice 28 100
Encephalopathy 28 100
Anorexia/nausea/vomiting 28 100
Hepatomegaly 6 21.4
Ascites 4 14.2
Bleeding(Gastrointestinal
or genitourinary bleeding) 7 25
Fever 6 21.4
During presentation 1 (3.5%) in grade ², 6 (21.4%) in
grade ²², 7 (25%) in grade ²²² and the rest 14 (50%)
patients were in grade IV encephalopathy.
Serum bilirubin level of the study population showed
two third (74.9%) patients had between 5 and 20 mg/
dl, 4 (14.2%) had below 5 mg/dl and 3 (10.7%) had
above 20 mg/dl. Serum ALT level of 25 patients showed
12 (48%) patients had between 200 and 1000 U/L, 4
(16%) had less than 200 U/L and 3 (12%) patients
had above 2000 U/L. Prothrombin time was done in
24 cases showing two third patients had level below
50 sec and one third patients had above 50 sec. Serum
electrolytes were done in 20 (71.4%) patients. Out of
them 8 (40%) patients developed hyponatraemia and
3 (15%) patients developed hypokalaemia. Serum
creatinine was done in two third (75%) patients,
among them 4 (19%) patients had renal failure. Blood
sugar was estimated in 19 (67.8%) patients and 3
(15.7%) of them had hypoglycaemia.
Fig.-1: Age distribution of the patients
Fig.-2: Sex distribution of the patients
30
Study on Aetiology and Outcome of Fulminant Hepatic Failure in Bangladeshi Patients BJM Vol. 21 No. 1

Viral markers for hepatitis A, B, C and E were done in
24 (85.7%) cases. Among them 11 (45.8%) were
hepatitis E virus positive, 6 (25%) patients were
hepatitis B virus positive and 1 (4.1%) patient was
positive for hepatitis A virus. No patient was hepatitis
C virus positive. In 2 (7.1%) cases fulminant hepatic
failure was due to drug (antitubercular) toxicity. In 4
(16.6%) cases no cause could be identified.
Among 28 patients outcome of 4 patients could not
be known as they left the hospital by discharge on
risk bond. Of the remaining 24 patients, 14 (58.3%)
patients survived and 10 (41.6%) expired.
Of the 24 patients with known outcome, 7 patients
were in grade I or II encephalopathy and among them
4 (58%) recovered from the disease. 17 patients were
grade III or IV encephalopathy and 10 (59%) recovered
from the disease.
10 patients presented within 7 days of illness and 2
(20%) of them expired. 14 patients presented after 7
days and 8 (57%) of them expired (Figure3).
Prothrombin time was measured in 24 cases and
among them outcome of 21 patients could be known.
15 patients had prothrombin time <50 seconds and 3
(20%) of them died. 6 patients had prothrombin time
>50 seconds and 5 (83.3%) of them died (Figure4).
11 patients had serum bilirubin <10 mg/dl and 3
(27.2%) of them died. 13 patients had serum bilirubin
>10 mg/dl and 8 (61.5%) died (Figure5).
13 patients had serum ALT<1000 U/L and 7 (53.8%)
of them survived. 8 patients had serum ALT >1000
U/L and 7 (87.5%) of them survived.
Among the 6 patients with disease caused by hepatitis
B virus, 3 (50%) survived. Of the 11 patients with
disease caused by hepatitis E virus, 6 (54%) survived.
Only 1 patient in the study affected by hepatitis A
virus survived. Among the 2 patients due to anti
tubercular chemotherapy, 1 patient survived and the
other died. 4 patients were due to unknown cause
and 3 (75%) of them survived.
Among the female patients 7 were pregnant during
the attack, 5 (71.4%) patients of them were due to
hepatitis E virus and 3 (60%) of them expired.
Discussion
Acute liver failure is a dramatic, unpredictable and
often devastating clinical .condition. Acute viral
hepatitis is the most common cause. In the study
most of the patients (75%) were in the age group of
16-35 years. It is similar to the finding of Khan M et
al. 71% were female and 29% were male with M:F=
2:5. It is contrary to the finding of Khan M et al where
M:F was 3:1.3
Anorexia, nausea, vomiting, jaundice and altered
conscious level were the predominant features. These
features have also been recognized in studies by Lee
WM5 and Khan M et al.3 In the current study all the
patients presented within 4 weeks of the onset of
illness which is consistent the finding of Khan M et
al where all patients presented within 2 weeks of the
onset of illness.3 Bleeding from different sites is the
end result of the coagulopathy. Marison G et al.
reported bleeding from 50% cases but in our study
28.5% patients showed bleeding manifestation.6
Wilkinson SP et al. recorded 55% functional renal
failure in patients of fulminant hepatic failure.7 In
the present study 19% patients developed renal
failure which is much lower. We found hyponatraemia
in 40% patients but Khan et al3 reported 66% patients
with hyponatraemia which is much higher than our
observation. 15.7% of our patients developed
hypoglycaemia which is consistent with the result of
Khan M et al.3 They recorded hypoglycaemia in 8%
patients.
Fig.-3: Relationship between the duration of onset of
encephalopathy and death rate
Patients admitted after
7 days
Patient admitted within
7 days
Prothrombin time <50 sec Prothrombin time >50 sec
Fig.-4: Relationship between serum prothrombin time and
death rate
Serum bilirubin <10 mg/dl Serum bilirubin >10 mg/dl
Fig.-5: Relationship between serum bilirubin level and
death rate
31
BJM Vol. 21 No. 1 Study on Aetiology and Outcome of Fulminant Hepatic Failure in Bangladeshi Patients

In this study hepatitis E virus was the causative agent
in 45.8% cases and hepatitis B virus in 25% cases.
Fulminant hepatic failure due to hepatitis E virus is
rare in Western countries, reports from developing
countries showed that HEV is the common cause of
FHF.8 Sallic R et al reported only 16.6% of patients
with FHF in UK due to HEV infection9 but no cases of
FHF due to HEV from France, Germany and USA.10
Acharya SK et al showed 62% cases of HEV was the
causative agent of FHF.8 Mathiesen LR et al showed
hepatitis B virus as a causative agent of FHF in 30-
40% cases in western population.11 Khan et al.
recorded 38.7% of FHF was due to HBV in
Bangladesh.3
Among the 7 pregnant patients 71.4% were due to
HEV infection and 60% of them died. This is clearly
related to the observation of Acharya SK et al. who
showed that HEV induced FHF is more common in
pregnancy and carries a high mortality rate.12
Hepatic encephalopathy of varying grades is the
hallmark of FHF. In this study there was no significant
difference in survival among the patients of different
grades of encephalopathy. Survival rate of patients
having encephalopathy grade 1 and 2 was 58% and
grade 3 and 4 was 59%. Khan et al showed none of
grade 4 encephalopathy survived and Trey et al showed
only 17.6% of their patients from Grade 4
encephalopathy. These results are in contrary to our
findings.3,13
83.3% of the patients having prothrombin time >50
sec died and 20% of the patients having prothrombin
time <50 sec expired. So prolonged prothrombin time
appears to be a bad prognostic factor which is
consistent with the finding of O’Grady JG et al. They
found 98% of patients with prothrombin time >50 sec
were expired.14
27.2% of the patients with S. bilirubin <10 mg/dl
expired and 61.5% of the patients with S. bilirubin
>10 mg/dl expired. So high S. bilirubin is found to be
a bad prognostic factor which is in contrary to the
finding of Khan M et al as they showed no prognostic
role of S. bilirubin level.3
Patients who presented within 7 days of onset of
illness, 20% of them expired and 57% of the patients
who presented after 7 days of illness expired. This is
also similar to other study. Khan M et al showed
death rates of these groups are 46.7% and 85.1%
respectively.3
Acharya SK et al12 reported Isoniazide/ Rifampicin
is the major cause of drug induced acute hepatic
failure in India which is also consistent with our
observation as 8.3% of the FHF were due to
antitubercular drug (Isoniazide/ Rifampicin) and 50%
of them died.
Conclusion
Fulminant hepatic failure is a serious complication
of acute viral hepatitis in Bangladesh. In the present
study HEV was the leading cause of FHF followed by
HBV. It reflects the observation that HEV is the main
cause of acute viral hepatitis in Bangladesh. Poor
sanitation and ignorance regarding food hygiene may
be precipitating factors. Pregnancy appears to be a
risk factor for HEV induced fulminant hepatic failure.
Blood glucose level should be regularly monitored and
appropriate measures should be taken promptly as
hypoglycaemia is common in FHF which may
complicate the disease outcome. Maintenance of
input, output chart, monitoring of renal function and
serum electrolytes are also important as alteration
of renal function as well as S. electrolytes are common
complication in FHF. Prolonged prothrombin time is
an important prognostic factor but grade of
encephalopathy failed to be proved as a prognostic
factor. This may reflect the frequent alteration of the
grade of encephalopathy which needs more close
monitoring.
As there is no specific therapy and significant
mortality rate we should try to prevent acute viral
hepatitis by creating awareness oh people, improving
sanitary facilities and by active immunization against
HBV and HAV. Thus we can reduce morbidity and
mortality related to it. Also we should actively think
of establishment of specialized liver unit by which
we can provide proper care to fulminant hepatic failure
patients as well as facility for liver transplantation
for the selected group of patients who have least
chance of survival with conservative therapy.
References
1. Keeffe EB. Acute liver failure. In: Friedman SL,
McQuaid KR, Grendell JH. Current diagnosis &
treatment in gastroenterology. 2nd edition. Mc Graw
Hill 2003; 536-545.
2. Lucke B. The fulminant form of epidemic hepatitis.
Am J Pathol 1946; 4: 399.
3. Khan M, Dhar SC, Rahmatullah M, Jahir M.
Fulminant hepatic failure aetiology, clinical
presentation, prognostic indices and treatment
option. J Inst Postgrad Med Res 1993, 8: 7.
4. Lee WM. Acute liver failure. Am J Med 1994; 96:
53.
5. Lee WM. Medical progress: Acute liver failure. N
Engl J Med 1993; 329: 1862.
6. Marinos G, Riley J, Painter DM, Mclaughan GW.
Sulfasalazine induced fulminant hepatic failure. J
Clin gastroenterol 1992; 14:132.
32
Study on Aetiology and Outcome of Fulminant Hepatic Failure in Bangladeshi Patients BJM Vol. 21 No. 1

7. Wilkinson SP, Blendis LM, Williams R. Frequency
of renal failure and electrolyte disorder in fulminant
hepatic failure. Br Med T. 1974; 1: 186.
8. Acharya SK, Dasaralhys Kumar TL. Fulminant
hepatitis in a tropical population- clinical course,
cause and early predictor of outcome. Hepatology
1996; 23: 1448-55.
9. Sallic R, Tibbs C, Silva AE, Sheron N, Eddelslon A,
Williams R et al. Detection of hepatitis E but not C
in sera of patients with fulminant NANB hepatitis.
Hepatology 1999; 14: 68.
10. Ostapowicz G, Lee MW. Acute hepatic failure: A
western perspective. J of Gastroenterology and
Hepatology 2000; 15: 480-8.
11. Mathiesen LR, Skinoj P, Nielson J. Hepatitis B virus
and non A non B in fulminant hepatic failure. Gut
1980;21: 72.
12. Acharya SK, Panda SK, Saxena A, Gupta SD. Acute
hepatic failure in India: A perspective from the east.
J of Gastroenterology 2000; 15, 473-479.
13. Trey C, Lipwroth C, Davidson CS. Parameters
influencing survival in the first 318 patients
reported to fulminant hepatic failure surveillance
study. Gastroenterology 1967; 54: 291-300.
14. O’Grady, Schalm S, William R. Acute liver failure:
redefining the syndrome. Lancet 1993; 342: 273-
75.
33
BJM Vol. 21 No. 1 Study on Aetiology and Outcome of Fulminant Hepatic Failure in Bangladeshi Patients