Official Journal of Association of Physicians of India ...
42
Transcript of Official Journal of Association of Physicians of India ...


1ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Editor in Chief
Prof. Sanjeeb Kakati
Assistant Editors
Dr. P. Borthakur, Dr. S. M. Baruah, Dr. D. Das, Dr. A. Dutta
Editorial Board :Prof. S. Baruah, Prof. A. K. Das, Prof. A. K. Sen, Prof. R. P. Medhi, Prof. B. Doley, Prof. G. N. Gogoi,
Prof. B. P. Chakrabarty, Prof. A. K. Adhikari, Prof. R. K. Kotokey, Prof. D. J. Borah, Prof. G. Kar,Prof. R. N Mishra, Prof. K Chakrabarty, Prof. T. K. Saikia, Prof. P. Kar, Prof. B . Das, Prof. A. K. Barman,
Dr. A. C. Saikia, Dr. B. N. Mahanta, Prof. M. K. Roy, Dr. A. Ahad, Dr. P. K. Baruah,Dr. D. Mili, Dr. M. Mishra, Dr. S. Buragohain.
Copyright and Photocopying :No part of this publication may be reproduced, or transmittedin any form or by any means, electronic or mechanical, includingphotocopy without written permission from the Hon. Editor.Business Correspondence :Enquiries concerning subscription, advertisement, etc. shouldbe addressed to Prof. Sanjeeb Kakati, Hon. Editor, AssamJournal of Internal Medicine, Department of Medicine, AssamMedical College, Dibrugarh, Assam, India. PIN-786002 Mobile: 9435030173, E-mail : [email protected],[email protected] : www.apiassam.com
Edited, printed and published by :Prof. Sanjeeb Kakati, for the Association of Physicians of India,Assam Chapter.The Editor disclaims any responsibility or liability forstatements made and opinion expressed by authors or claimsmade by advertisers.Advertorial Enquiry :Prof. Sanjeeb Kakati, Hon. Editor, Assam Journal of InternalMedicine, Department of Medicine, Assam Medical College,Dibrugarh, Assam, India. PIN-786002 Mobile : 9435030173E-mail : [email protected], [email protected] at : P. C. Printsoft, Dibrugarh, Assam.
A PEER REVIEWED JOURNAL
BIANNUAL PUBLICATION – July 2017 (Next issue- January, 2018)
Official Journal of Association of Physicians of India, Assam Chapter
2ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Immediate Past President : Dr. Swaroop BaruahPresident : Dr. Atul Ch. SaikiaVice- Chairperson : Dr. R. BorpuzariHon. General Secretary : Dr. B. N. MahantaHon. Joint Secretary : Dr. A. Kalwar
Dr. Amol Deb GoswamiHon. Secretary (Headquarter) : Dr. S. M. BaruahHon. Treasurer : Dr. Nitya GogoiExecutive Body Members : Dr. N. G. Singh
Dr. Rini DowerahDr. D. BorthakurDr. B. BhuyanDr. Pritam BorthakurDr. Madhab MishraDr. D. D. MilliDr. G. C. KhandelwalDr. Krishna Bora
Editor of the Assam Journal ofInternal Medicine : Dr. Sanjeeb KakatiCo-opted Members : General Secretaries of all the District Branches
OFFICE BEARERS OF THE ASSOCIATION OF PHYSICIANSOF INDIA, ASSAM CHAPTER
With best complement from

3ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
C O N T E N T S
Official Journal of Association of Physicians of India, Assam Chapter
Editor in Chief : PROF. SANJEEB KAKATI
ASSAM JOURNAL OF INTERNAL MEDICINE
E D I T O R I A LEchocardiography in ESRD patients on CAPD 5Mriganka Shekhar Chaliha
O R I G I N A L A R T I C L EEchocardiographic Changes in Patients with ESRD on CAPD with special reference 8to iPTH and Vit-D level - A Single Centre StudyS Singh, P K Doley, V P Singh, P Pant, D P Kar, V Ganige, N Singh
Depression in Type 2 Diabetes Mellitus : Prevalence and Association with Clinical 14and Sociodemographic ParametersK Saikia, B Choudhury, A Choudhury, S K Agarwal, A K Bhuyan
Assessment of volume of bleed in Intra-cerebral Hemorrhage as a reliable and easy to use 18yardstick in prediction of 7 day mortalityD Das, K Bhattachrjee, S K Ghintala
Clinical Profile of Cryptococcal Meningitis : Hospital Based Study 22S Bawri, M Das , A Kayal, M Goswami, L J Basumatary, P Borah
Complications Profile of Diabetes Mellitus in a Tertiary care Hospital 26in Upper AssamP Dihingia, S M Baruah, T K Das, C Dutta, T Karthikeyan
R E V I E W A R T I C L EPhysical Factors of Carcinogenesis 29P S Roy, A Inamdar, T Nyodu, M Hazarika
C A S E R E P O R T
Kartagener’s Syndrome : Case Presentation 33B Hazarika, R Korwa

4ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
C O N T E N T S
C A S E R E P O R TSheehan’s Syndrome Presenting as Cardiac Tamponade 36R Choudhury, J. Idiculla, R Pradeep
Cryptogenic Burkholderia cepacia Sepsis in A Haemoglobin E Disease Patient with 38Splenic and Hepatic AbscessesS Baruah, B Thakuria, T Das, S Kalunkhe
5ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Cardiovascular mortality is significantly increased inpatients with Chronic Kidney Disease(CKD) leading toearlier atherosclerosis, valvular and pericardial disease ,arrhythmias and heart failure. Use of echocardiographyplays a crucial role in the evaluation of these patients .Over time, a combination of CKD and other medicalconditions such as hypertension and diabetes leads tomyocardial fibrosis and development of LVH. The termknown as ‘cardiorenal syndrome’ (CRS) includes a broadspectrum of diseases in which both heart and kidney areinvolved. A consensus conference of the Acute DialysisQuality Initiative Group1 has proposed the term‘cardiorenal syndrome’ to define a clinical overlap betweenkidney and heart dysfunction. Left ventricular hypertrophy(LVH) represents the key feature in uremic cardiopathyand it is related to CRS type 4 (chronic renocardiac/cardiorenal syndrome).
Essentially three pathophysiological factors have beenidentified in relation to LVH of CKD and ESRD patients: (1) related to afterload, (2) related to preload, and(3) not related to afterload or preload2, 3, 4. The factors inthe first category are represented by an increase in systemicarterial resistance, elevated arterial blood pressure, andreduced large-vessel compliance2-5. All these three factorsresult in myocardial cell thickening and concentric LVremodeling often together with activation of the intracardiacrenin-angiotensin system4,6. Oxidative stress and xanthineoxidase activation as well as the phosphodiesterase-5pathway may also be involved in the development of LVH7.
E d i t o r i a l
* Associate Professor of Cardiology, Correspondence Address : Dr.Mriganka Shekhar Chaliha, Associate Professor of Cardiology, AssamMedical College and Hospital, Dirbugarh. Email :[email protected]
Mriganka Shekhar Chaliha*
©
Echocardiography in ESRD patients on CAPD
Among the preload-related factors, the role of intravascularvolume expansion (salt and fluid loading) has to beunderlined, as well as secondary anemia8-10, resulting inmyocardial cell lengthening and eccentric or asymmetricLV remodeling. Both afterload- and preload-relatedfactors operate with additive and synergistic effects. As aresult, myocardial hypertrophy induces the activation ofcellular apoptotic signals and activates metabolic pathwaysto increase extracellular matrix production up to fibrosis.11,
12 Fibrosis leads to progressive impairment in contractilitywith stiffening of the myocardial wall, systolic and diastolicdysfunction, dilated cardiomyopathy and congestive heartfailure13. Renin-angiotensin-aldosterone system activationinduces hyperaldosteronemia promoting cardiac fibrosisthrough the generation of signals leading to profibrotictransforming growth factor production6. LVH can also bepromoted by iron and/or erythropoietin14 or vitamin Ddeficiency15. Recent studies have pointed out novelbiomarkers involved in the pathogenesis of LVH.
One of these is represented by FGF23, a memberof the fibroblast growth factor family primarily involved inCKD-mineral and bone disorder (MBD) and secondarilyto hyperparathyroidism.The pathogenesis of CKD-MBDhas always been ascribed to a decline in 1,25-dihydroxyvitaminD [1,25(OH)2 D3] levels leading toincreases in serum parathyroid hormone(PTH) andsubsequent alterations in calcium and phosphorusmetabolism16,17. Vitamin D deficiency, together withsecondary hyperparathyroidism and hyperphosphatemia,was reported as a main factor contributing to highcardiovascular risks in CKD patients18 .
In the present study, published in this issue, LVH

6ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
was found in 60 % of cases ( at the beginning) and 43.3%of cases ( 1 year after CAPD). It is seen that iPTH level >300pg/ml was significantly associated with LVH comparedto iPTH level < 300pg/ml ( P< 0.048 and 0.019). Vit –Dlevel of <30 ng/ml was associated with LVH(P<0.02).Earlier experimental studies showed associationbetween vitamin D deficiency and impairment of cardiaccontractile function, increased myocardial collagen content,and increased cardiac mass19-21. In the present study,published here, there was appreciable reduction in LVHcases after 1 year of CAPD .The reduction in the degreeof LVH can be achieved by fluid balance and bloodpressure control together with anemia control22. Foley etal.23 found that improvements in LVmass and systolicfunction 1 year after the initiation of dialysis. Covic et al.24
reported a regression of LV mass in hemodialysis patientsassociated with improvements in anemia, serum phosphatelevel, and calcium-phosphate product.
In the present study (published in this issue) diastolicdysfunction ( 66% at baseline and 60 % at 1 year ofCAPD) and systolic dysfunction (33% at base line and30 % at 1 year of CAPD ) have been noted as commonabnormalities in CKD patients. Cardiac alteration inpatients with CKD leads to dysfunction in both diastolicand systolic properties. Echocardiographic abnormalities(impairment of EF and increased end-systolic and end-diastolic LV volumes) are frequently reported from theearly stages of CKD to ESRD. Diastolic function wasdetermined in the present study by measuring E/A ratioby special doppler inflow velocity (E is peak early diastolevelocity and A is peak atrial filling velocity of left ventricleacross mitral valve). E/A ratio less than 0.75 and morethan 1.8 was considered as diastolic dysfunction.However,the accurate assessment of diastolic function inthese patients is challenging as the wide variations involume status makes mitral inflow velocity measurementsdifficult25. Therefore the ratio of early mitral flow velocityto early mitral annulus velocity (E/E /) has been found tobe a reliable measure of LV filling in ESRD patients26.InCKD patients, Tissue Doppler Imaging ( TDI) is moresensitive to detect diastolic dysfunction than conventionalechocardiography27-30.
One question that comes here under the context is –Is it relevant to measure systolic and diastolic function ofLV in uraemic population ? In a previous study by Hsiao
et al. LV dysfunction, LVH and LV diastolic dysfunctionwere found to influence prognosis31. In the same way , ina study by Kim et al. diastolic dysfunction was a significantmarker of rapid decline in residual renal function and theoccurrence of cardiovascular events in patients placed inCAPD32 . Diastolic dysfunction has been observed inpatients receiving renal replacement therapy for ESRD inmany studies33,34. In a study by Duran et al., diastolicfunction of LV was not significantly altered aftermaintenance of haemodialysis treatment. Theydemonstrated that in the long run, the acute changes ofvolume, electrolytes and autonomic regulation due tohaemodialysis session does not affect left diastolicfunction35. For Lee et al., the prevalence and severity ofdiastolic LV dysfunction is higher in PD patients36.Someauthors suggest that Left ventricular mass and diastolicfunction are closely related to each other in all dialysispatients37. Similarly, fractional shortening, a measurementof global LV systolic function, could over estimatecontractility in patients with concentric hypertrophy. Indialysis patients, tissue velocity and strain imaging can detectchanges in LV function better and are less affected by thevolume status of the patients38.The present study in referencedid not find any improvement in cardiac function withtreatment of 1 year. Perhaps a longer duration of study anduse of TDI could have shown such an improvement.
REFERENCES :1. Ronco C: The cardiorenal syndrome: basis and common ground
for a multidisciplinary patient-oriented therapy. CardiorenalMed. 2011; (1): 3–4.
2. Ritz E, Wanner C: The challenge of sudden death in dialysispatients. Clin J Am SocNephrol. 2008; (3): 920–29.
3. Gross ML, Ritz E: Hypertrophy and fibrosis in thecardiomyopathy of uremia – beyond coronary heart disease.Semin Dial. 2008; (21): 308–18.
4. Ritz E: Left ventricular hypertrophy in renal disease: beyondpreload and afterload. Kidney Int. 2009; (75): 771–73.
5. Mominadam S, Ozkahya M, Kayikcioglu M, Toz H, Asci G,Duman S, Ergin P, Kirbiyik S, Ok E, Basci A: Interdialytic bloodpressure obtained by ambulatory blood pressure measurementand left ventricular structure in hypertensive hemodialysispatients. Hemodial Int. 2008, 12 (3): 322-27.
6. Steigerwalt S, Zafar A, Mesiha N, Gardin J, Provenzano R: Roleof aldosterone in left ventricular hypertrophy among African-American patients with end-stage renal disease on hemodialysis.Am J Nephrol.2007;( 27): 159–63.
7. Xu X, Hu X, Zhang P, Zhao L, Wessale JL, Bache RJ, Chen Y:Xantine oxidase inhibition with febuxostat attenuates systolicoverload-induced left ventricular hypertrophy and dysfunctionin mice. J Card Fail. 2008; (14): 746–53.
8. Di Lullo L, Floccari F, Polito P: Right ventricular diastolic functionin dialysis patients could be affected by vascular access. NephronClinPract. 2011; (118): 258–262.
7ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
9. Martin LC, Franco RJ, Gavras I, Matsubara BB, Garcia S,Caramori JT, Barretti BB, Balbi AR, Barsanti R, Padovani C,Gavras H: Association between hypervolemia and ventricularhypertrophy in hemodialysis patients. Am J Hypertens. 2004;(17): 1163–69.
10. McRae JM, Levin A, Belenkie I: The cardiovascular effects ofarteriovenous fistulas in chronic kidney disease. A cause forconcern?Semin Dial. 2006;( 19): 349–52.
11. Nishida K, Kyoi S, Yamaguchi O, Sadoshima J, Otsu K: The roleof autophagy in the heart. Cell Death Differ 2009; 16: 31–38.
12. Dorm GW 2nd: Apoptotic and non-apoptotic programmedcardiomyocyte death in ventricular remodeling. Cardiovasc Res.2009; (81): 465–73.
13. Zoccali C, Benedetto FA, Tripepi G, Mallamaci F: Cardiacconsequences of hypertension in hemodialysis patients. SeminDial. 2004; (17): 299–303.
14. Sakurabayashi T, Miyazaki S, Yuasa Y, Sakai S, Suzuki M,Takahashi S, Hirasawa Y: L -Carnitine supplementation decreasesthe left ventricular mass in patients undergoing hemodialysis.Circ J. 2008; (72): 926–31.
15. Strozecki P, et al: Parathormon, calcium, phosphorus and leftventricular structure and function in normotensive hemodialysispatients. Ren Fail. 2001; (23): 115–26.
16. Moe S, Drueke T, Cunningham J: Definition, evaluation andclassification of renal osteodistrophy: a position statement fromKidney Disease Improving Global Outcome (KDIGO). KidneyInt. 2006; (69): 1945–53.
17. Moe S, Drueke TB, Block A, et al: KDIGO clinical practiceguideline for the diagnosis, evaluation, prevention and treatmentof chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney Int. 2009; (113):S1– S130.
18. Burhiya R, Li S, Chen S, Mc Cullough PA, Bakris GL: Plasmaparathyroid hormone level and prevalent cardiovascular diseasein CKD stages 3 and 4: an analysis from the Kidney EarlyEvaluation Program (KEEP). Am J Kidney Dis. 2009;( 53):S3–S10.
19. Weishaar RE, Simpson RU: Involvement of vitamin D3 withcardiovascular function. II. Direct and indirect effects. Am JPhysiol. 1987;( 253): E675– E683.
20. Weishaar RE, Simpson RU: Vitamin D3 and cardiovascularfunction in rats. J ClinInvest.1989;( 79): 1706–12.
21. Weishaar RE, Simpson RU: The involvement of the endocrinesystem in regulating cardiovascular function: Emphasis on vitaminD3. Endocr Rev. 1989; (10): 351–65.
22. Culleton BF, Walsh M, Klarenbach SW, Mortis G, Scott-DouglasN, Quinn RR, Tonelli M, Donnelly S, Friedrich MG, Kumar A,Mahallati H, Hemmelgarn BR, Manns BJ: Effect of frequentnocturnal hemodialysis vs conventional hemodialysis on leftventricular mass and quality of life: a randomized controlledtrial. JAMA. 2007; (298): 1291–99.
23. Foley RN, Parfrey PS, Kent GM, Harnett JD, Murray DC,Barre PE: Serial change in echocardiographic parameters andcardiac failure in end-stage renal disease. J Am SocNephrol. 2000;(11): 912–16.
24. Covic A, Mardare NG, Ardeleanu S, Prisada O, Gusbeth-TatomirP, Goldsmith DJ: Serial echocardiographic changes in patientson hemodialysis: an evaluation of guideline implementation. JNephrol. 2006; (19): 783–93.
25. Raggi P, Boulay A, Chasan-Taber S, Amin N, Dillon M, BurkeSK, ChertowGM.Cardiac calcification in adult hemodialysis
patients. A link between end-stage renal disease and cardiovasculardisease. J Am CollCardiol. 2002 ;39(4):695-701
26. Sharma R, Pellerin D, Gaze DC, Mehta RL, Gregson H, StreatherCP, Collinson PO, Brecker SJ. Mitral peak Doppler E-wave topeak mitral annulus velocity ratio is an accurate estimate of leftventricular filling pressure and predicts mortality in end-stagerenal disease. J Am SocEchocardiogr. 2006;19(3):266-73.
27. Hayashi SY, Brodin LA, Alvestrand A, Lind B, Stenvinkel P,Mazza do Nascimento M, Qureshi AR, Saha S, Lindholm B,Seeberger A. Improvement of cardiac function after haemodialysis.Quantitative evaluation by colour tissue velocityimaging.Nephrol Dial Transplant. 2004 Jun;19(6):1497-506.
28. Garcia MJ, Thomas JD, Klein AL. New Dopplerechocardiographic applications for the study of diastolic function.J Am CollCardiol 1998; 32(4): 865-75.
29. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, QuiñonesMA. Doppler tissue imaging: a noninvasive technique forevaluation of left ventricular relaxation and estimation of fillingpressures. J Am CollCardiol 1997; 30(6): 1527-33.
30. Hayashi SY, Rohani M, Lindholm B, Brodin LA, Lind B, BaranyP, Alvestrand A, Seeberger A. Left ventricular function in patientswith chronic kidney disease evaluated by colour tissue Dopplervelocity imaging. Nephrol Dial Transplant 2006; 21(1): 125-32.
31. Hsiao SH, Lin SK, Huang WC, Chiu-Yen Lee CY,YangSH,ChiouKR, Liu CP. Para-meters derived from myocardial tissue dop-pler imaging associated with major events in patients with uremia.ActaCardiol Sin.2007; 23: 254-62.
32. Kim JK, Kim SG, Kim MG, Kim SE, Kim SJ, Kim HJ, Song YR.Left ventricular diastolic dysfunction as a predictor of rapiddecline of residual renal function in patients with peritonealdialysis. J Am SocEchocardiogr. 2012;25(4):411-20.
33. Kimura H, Takeda K, Tsuruya K, Mukai H, Muto Y, Okuda H,Furusho M, Ueno T, Nakashita S, Miura S, Maeda A, Kondo H.Left ventricular mass index is an independent determinant ofdiastolic dysfunction in patients on chronic hemodialysis: a tissueDoppler imaging study. Nephron Clin Pract.2011;117(1):c67-73.
34. RaizadaV , Skipper B , Taylor RA , Luo W , Harford AA , ZagerPG , Rohrscheib M , Spalding CT. Left ventricular diastolicfunction in patients on hemodialysis. J Investig Med. 2010;58(6): 791-5.
35. Duran M, Unal A, Inanc MT, Esin F, Yilmaz Y, Ornek E. Effectof maintenance hemodialysis on diastolic left ventricular functionin endstage renal disease. Clinics (Sao Paulo). 2010; 65(10): 979-84.
36. Lee J-K, Lin HH, Tsai CT, Chen JJ , Kuo CC , Lien YC , Lin JW, Huang JW , Hwang SW , Hwang JJ , Tseng CD , Chiang FT ,Chen JJ , Wu CK .Differential association of proinflammatorycytokines with left ventricular diastolic dysfunction in subjectswith and without continuous ambulatory peritonealdialysis.NutrMetabCardiovasc Dis. 2012; 22(11): 974-80.
37. Weiss G, Lhotta K, Reibnegger G, König P, Knapp E. Divergenteffects of hemodialysis and continuous ambulatory peritonealdialysis on cardiac diastolic function. Perit Dial Int 1997; 17(4):353-9.
38. Skulsted H, Urheim S, Edvardsen T, et al. Grading of myocardialdysfunction by tissue Doppler echocardiography for riskstratification and prognosis of patients with left ventricularhypertrophy: a comparison between velocity, displacement, andstrain imaging in acute ischemia. J Am CollCardiol. 2006:47(8):1672-82
8ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Echocardiographic Changes in Patients withESRD on CAPD with special reference to iPTH
and Vit-D level - A Single Centre Study
S Singh*, P K Doley** , V P Singh** , P Pant** , D P Kar** , V Ganiger** , N Singh***
O r i g i n a l A r t i c l e
AbstractBackground: Cardiac function abnormalities are common in CKD patients. We conducted this study : 1. to assess the
cardiac function in ESRD patients on CAPD. 2. impact of CAPD on iPTH and Vit-D level and their association with changesin the echo-cardiographic parameters. 3. influence of CAPD on anemia and hypertension in patients with ESRD.Material and Methods: We included 30 (thirty) ESRD patients on CAPD who were on 4 exchange per day irrespective ofunderlying etiology in our study, which was conducted in a tertiary centre in eastern UP, India. All patients were clinicallyevaluated thoroughly and subjected for complete blood count, renal function test, serum calcium, phosphate, albumin, iPTH,Vitamin D and 2-D echocardiography at the time of initiation of CAPD and at 12 months. Results and observations: Out ofthirty patient male to female ratio was 1.7:1 (63.33 vs 33.66). Mean age of presentation was 45.66±24.34. Mean iPTH levelat the beginning and at the end of study were 223.12 ± 140.21 pg/ml and 214 ± 111.68 pg/ml respectively. Vit-D level were26.71 ± 11.11 ng/ml and 31.85 ± 14.60ng/ml respectively at 0 and 12 months. LVH, systolic and diastolic dysfunctions werepresent in 60% (n=18), 33% (n=10), 66% (n=20) at the beginning and 43.33% (n=13), 30% (n=9) and 60% (n=18) at the endof the study respectively. iPTH level > 300pg/ml was significantly associated with LVH and diastolic dysfunction ascompared to iPTH level < 300pg/ml ( p=0.048 and 0.019). Vit –D level of <30 ng/ml was associated significantly with LVH(p=0.02) and diastolic dysfunction (p=0.04). Significant association of LVH (p= 0.04) and systolic dysfunction (p=0.02)was seen with hemoglobin level of < 10gm/dl. Mean BP changes were significant upon completion of the study. Conclusion:Diastolic dysfunction is the commonest echocardiographic abnormality in ESRD patients on CAPD followed by LVH andsystolic dysfunction. Significant BP control was seen at the end of study, though it was short term study. High iPTH level> 300pg/ml were significantly associated with LVH and diastolic dysfunction. Vit-D level < 30 ng/ml were correlated wellwith the LVH and diastolic dysfunction.
*HOD and Associate Professor of Nephrology ** Senior Resident.*** Medical officer, Centre for Clinical Investigation. Deptt. ofNephrology. IMS, BHU, Vanaras, UP, India. Correspondence Address: Dr. Prodip Kr. Doley, Deptt. Of Nephrology. GMCH, Guwahati -32.Assam. Email: [email protected].
Key Words: ESRD, LVH, systolic dysfunction, diastolicdysfunction, iPTH, Vit-D.
INTRODUCTION :Advances in the renal replacement therapy had
changed the outlook of ESRD patients in a significant way.Continuous ambulatory peritoneal dialysis is increasinglyaccepted treatment modality for RRT amongst ESRDpatients worldwide. It has been suggested that patients onCAPD are fairly better in terms of fluid and hypertensioncontrol but are at the greater risk for developingatherosclerosis due to more production of atherogeniclipids, which in turn had adverse impact on cardiovascularmorbidity and mortality1. Cardiac alterations develop earlyin the course of CKD, which tend to progress with time in
majority of patients with ESRD and these alterations canbe efficiently demonstrated by echocardiography. Thepresence of LVH (48-75 %) in ESRD patients increasesthe risk for cardiac ischemia, congestive heart failure andarrhythmias and a strong predictor of cardiovascularmortality2. These alterations in LVH and LV dilatation isprincipally mediated by hemodynamic factor like chronicpressure, volume overload or both and anemia, thoughother factors like metabolic and neurohormonal mechanismare also seen to contribute3,4. CAPD exerts beneficialeffects on cardiovascular system in ESRD patients bypreventing the volume overload, lack of intra and inter-dialytic volume changes, better control of BP, constantelectrolyte and acid base balance. The prevalence of CVrisk factors has been found to change with time duringfollow up. Significant decreases in hypertension and leftventricular hypertrophy have been observed in the firstyear of therapy; but after 5 years, the risk factors arefound in same proportions noted at the start of the

9ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
treatment5. We designed a prospective study to analyzevarious echocardiographic alterations of cardiac functionin ESRD patients on CAPD.
MATERIAL AND METHODS :We included 30 (thirty) ESRD patients on CAPD
who were on 4 exchange per day irrespective of underlyingetiology in our study, which was conducted in a tertiarycentre in eastern UP, India. A person was labeled as ESRDif his or her GFR was less than 15mL/min/1.73 m2 as perModified Diet in Renal Disease (MDRD) formula. Nopatients in our study group used icodextrin base exchange.Patient with obvious clinical evidence of coronary arterydisease, valvular heart disease and rheumatic heart disease,congenital heart disease and primary cardiomyopathieswere excluded from the study. All patients were clinicallyevaluated thoroughly and subjected for complete bloodcount, renal function test, serum calcium, phosphate,albumin, iPTH, Vitamin D and 2-D echocardiography atthe time of initiation of CAPD and at 12 months. BMIand efficacy of CAPD was not correlated with this studythough we performed KT/V in each and every patient asper protocol. 2D-Echocardiography machine GE LOGIQ400 PRO was used with 3.5 MHz transducer probe. TheM-mode recording perpendicular to the long axis throughthe centre of the left ventricle at the papillary muscle levelwas taken as standard measurements of the systolic anddiastolic wall thickness and chamber dimensions. The leftventricular ejection fraction (LVEF) was taken as measureof left ventricular systolic dysfunction and ejection fraction<55% was considered as systolic dysfunction. Diastolicfunction was determined by measuring E/A ratio by specialdoppler inflow velocity (E is peak early diastole velocityand A is peak atrial filling velocity of left ventricle acrossmitral valve). E/A ratio less than 0.75 and more than 1.8was considered as diastolic dysfunction. LVH wasdiagnosed when interventricular septum thickness or leftventricular posterior wall thickness was > 12 mm.Hypertension was defined as BP > 140/90 mmHg in rightarm supine position and anemia was diagnosed withhemoglobin <13.5 gm/dl in male and 12.5 gm/dl in female.Vit –D insufficiency and deficiency were defined as Vit-Dlevel < 15-30ng/ml and < 15ng/ml respectively. iPTHvalue of 150-300 pg/ml was the target range as per NKF/KDIGO guideline. Statistical analysis was done by SPSS
software version 15 by using Fisher’s exact test. A ‘p’valueof < 0.05 were considered significant.
We conducted this study to evaluate the cardiacfunction anomalies in ESRD patients on CAPD, influenceof CAPD on iPTH and Vit-D level and their associationwith changes in the echo-cardiographic parameters. Effectsof CAPD on anemia and hypertension were alsoevaluated.
RESULTS AND OBSERVATIONS :We studied 30 (Thirty) ESRD patients on CAPD
irrespective of underlying etiology, who were on 4exchanges per day and patients were followed up for 12months. During this follow up periods we performed allnecessary investigations in each and every patient. Resultswere analyzed by using SPSS-15 software version. Weevaluated all the parameters in two separate occasions,one at beginning of the study and another at the end of 12months.
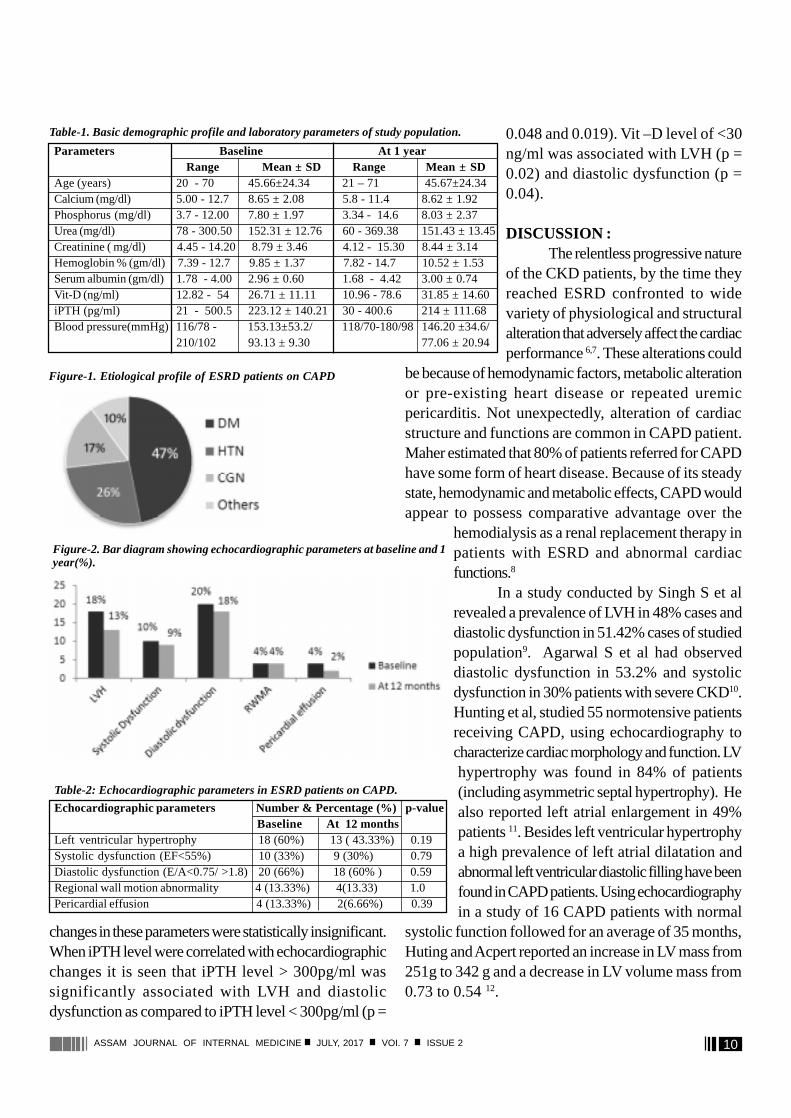
Out of thirty patient male to female ratio was 1.7:1(63.33 Vs 33.66). Mean age of presentation was45.66±24.34. Diabetes account for 46.66% patients andwas the most common cause of ESRD followed byhypertension in 26.66% and chronic glomerulonephritisin 16.66% . Basic demographic and laboratory parameterswere presented in Table-1 and etiological profile in Figure-1.Mean iPTH level at the beginning of the study and at theend of 12 months were 223.12 ± 140.2 pg/ml and 214 ±111.68 pg/ml respectively. Likewise Vit-D level were26.71 ± 11.11 ng/ml and 31.85 ± 14.60 ng/ml respectively.No significant difference of iPTH and Vit-D level werenoticed amongst the diabetic and non-diabetic ESRDpopulation. Anemia was seen in each and every patient.A marked change in the serum albumin level was not seenat the end of the study. The mean systolic and diastolicblood pressure were 153.13 ± 53.2/ 93.13 ± 9.30 mmHgand 146.20 ± 34.6/77.06 ± 20.94 mmHg at start of thestudy and at the end of the study respectively and changeswere statistically significant.
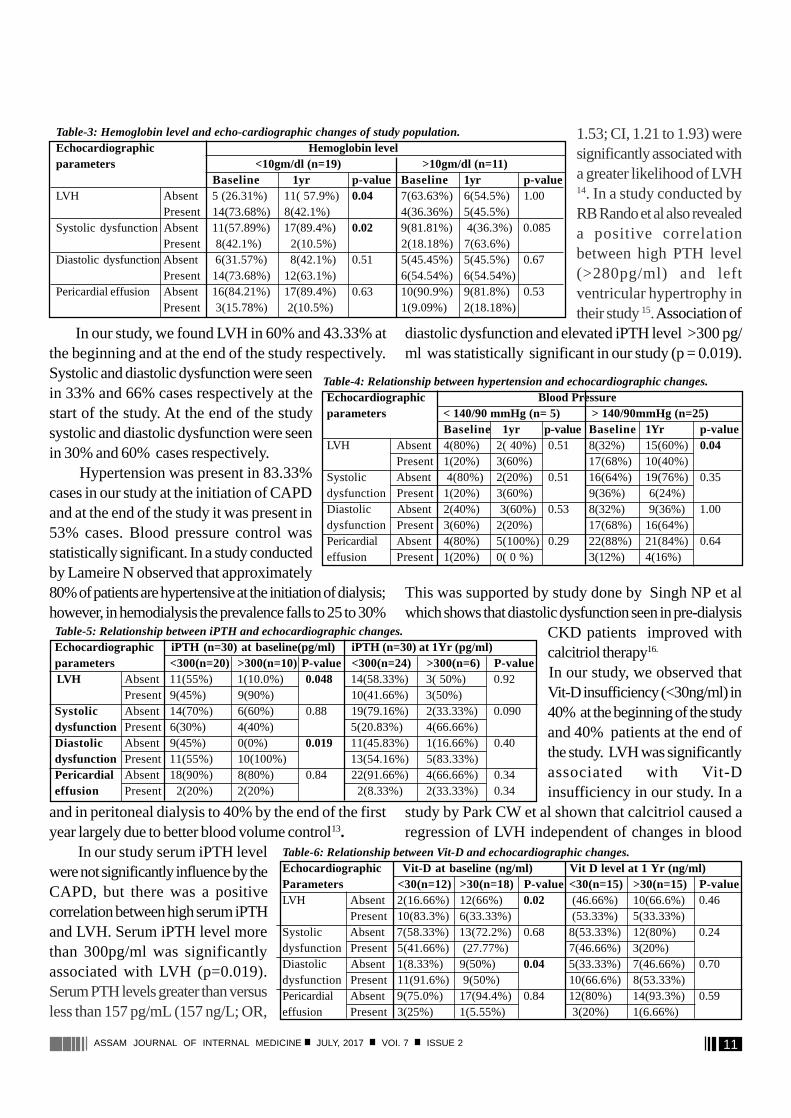
On analyzing the echocardiographic changes, LVHwas present in 60% cases at the beginning and 43.33% atthe end of the study. Systolic and diastolic dysfunctionwere seen in 33% and 66% cases at the start of the study.At the end of the study systolic and diastolic dysfunctionwere seen in 30% and 60% cases respectively. The
10ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
changes in these parameters were statistically insignificant.When iPTH level were correlated with echocardiographicchanges it is seen that iPTH level > 300pg/ml wassignificantly associated with LVH and diastolicdysfunction as compared to iPTH level < 300pg/ml (p =
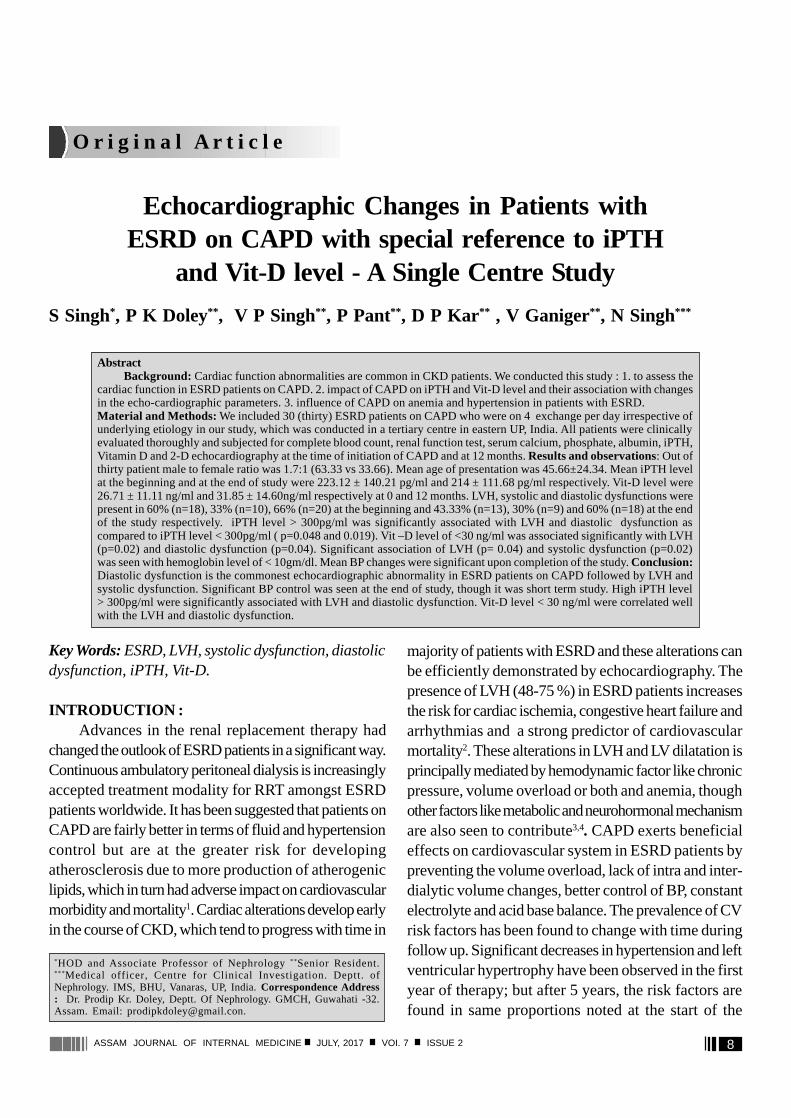
Parameters Baseline At 1 year Range Mean ± SD Range Mean ± SD
Age (years) 20 - 70 45.66±24.34 21 – 71 45.67±24.34Calcium (mg/dl) 5.00 - 12.7 8.65 ± 2.08 5.8 - 11.4 8.62 ± 1.92Phosphorus (mg/dl) 3.7 - 12.00 7.80 ± 1.97 3.34 - 14.6 8.03 ± 2.37Urea (mg/dl) 78 - 300.50 152.31 ± 12.76 60 - 369.38 151.43 ± 13.45Creatinine ( mg/dl) 4.45 - 14.20 8.79 ± 3.46 4.12 - 15.30 8.44 ± 3.14Hemoglobin % (gm/dl) 7.39 - 12.7 9.85 ± 1.37 7.82 - 14.7 10.52 ± 1.53Serum albumin (gm/dl) 1.78 - 4.00 2.96 ± 0.60 1.68 - 4.42 3.00 ± 0.74Vit-D (ng/ml) 12.82 - 54 26.71 ± 11.11 10.96 - 78.6 31.85 ± 14.60iPTH (pg/ml) 21 - 500.5 223.12 ± 140.21 30 - 400.6 214 ± 111.68Blood pressure(mmHg) 116/78 - 153.13±53.2/ 118/70-180/98 146.20 ±34.6/
210/102 93.13 ± 9.30 77.06 ± 20.94
Table-1. Basic demographic profile and laboratory parameters of study population. 0.048 and 0.019). Vit –D level of <30ng/ml was associated with LVH (p =0.02) and diastolic dysfunction (p =0.04).
DISCUSSION :The relentless progressive nature
of the CKD patients, by the time theyreached ESRD confronted to widevariety of physiological and structuralalteration that adversely affect the cardiacperformance 6,7. These alterations could
be because of hemodynamic factors, metabolic alterationor pre-existing heart disease or repeated uremicpericarditis. Not unexpectedly, alteration of cardiacstructure and functions are common in CAPD patient.Maher estimated that 80% of patients referred for CAPDhave some form of heart disease. Because of its steadystate, hemodynamic and metabolic effects, CAPD wouldappear to possess comparative advantage over the
hemodialysis as a renal replacement therapy inpatients with ESRD and abnormal cardiacfunctions.8
In a study conducted by Singh S et alrevealed a prevalence of LVH in 48% cases anddiastolic dysfunction in 51.42% cases of studiedpopulation9. Agarwal S et al had observeddiastolic dysfunction in 53.2% and systolicdysfunction in 30% patients with severe CKD10.Hunting et al, studied 55 normotensive patientsreceiving CAPD, using echocardiography tocharacterize cardiac morphology and function. LVhypertrophy was found in 84% of patients(including asymmetric septal hypertrophy). Healso reported left atrial enlargement in 49%patients 11. Besides left ventricular hypertrophya high prevalence of left atrial dilatation andabnormal left ventricular diastolic filling have beenfound in CAPD patients. Using echocardiographyin a study of 16 CAPD patients with normal
systolic function followed for an average of 35 months,Huting and Acpert reported an increase in LV mass from251g to 342 g and a decrease in LV volume mass from0.73 to 0.54 12.
Table-2: Echocardiographic parameters in ESRD patients on CAPD.
Echocardiographic parameters Number & Percentage (%) p-value Baseline At 12 months
Left ventricular hypertrophy 18 (60%) 13 ( 43.33%) 0.19Systolic dysfunction (EF<55%) 10 (33%) 9 (30%) 0.79Diastolic dysfunction (E/A<0.75/ >1.8) 20 (66%) 18 (60% ) 0.59Regional wall motion abnormality 4 (13.33%) 4(13.33) 1.0Pericardial effusion 4 (13.33%) 2(6.66%) 0.39
Figure-1. Etiological profile of ESRD patients on CAPD
Figure-2. Bar diagram showing echocardiographic parameters at baseline and 1year(%).
11ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
In our study, we found LVH in 60% and 43.33% atthe beginning and at the end of the study respectively.Systolic and diastolic dysfunction were seenin 33% and 66% cases respectively at thestart of the study. At the end of the studysystolic and diastolic dysfunction were seenin 30% and 60% cases respectively.
Hypertension was present in 83.33%cases in our study at the initiation of CAPDand at the end of the study it was present in53% cases. Blood pressure control wasstatistically significant. In a study conductedby Lameire N observed that approximately80% of patients are hypertensive at the initiation of dialysis;however, in hemodialysis the prevalence falls to 25 to 30%
and in peritoneal dialysis to 40% by the end of the firstyear largely due to better blood volume control13. In our study serum iPTH levelwere not significantly influence by theCAPD, but there was a positivecorrelation between high serum iPTHand LVH. Serum iPTH level morethan 300pg/ml was significantlyassociated with LVH (p=0.019).Serum PTH levels greater than versusless than 157 pg/mL (157 ng/L; OR,
1.53; CI, 1.21 to 1.93) weresignificantly associated witha greater likelihood of LVH14. In a study conducted byRB Rando et al also revealeda positive correlationbetween high PTH level(>280pg/ml) and leftventricular hypertrophy intheir study 15. Association of
diastolic dysfunction and elevated iPTH level >300 pg/ml was statistically significant in our study (p = 0.019).
This was supported by study done by Singh NP et alwhich shows that diastolic dysfunction seen in pre-dialysis
CKD patients improved withcalcitriol therapy16.
In our study, we observed thatVit-D insufficiency (<30ng/ml) in40% at the beginning of the studyand 40% patients at the end ofthe study. LVH was significantlyassociated with Vit-Dinsufficiency in our study. In a
study by Park CW et al shown that calcitriol caused aregression of LVH independent of changes in blood
Table-4: Relationship between hypertension and echocardiographic changes.Echocardiographic Blood Pressureparameters < 140/90 mmHg (n= 5) > 140/90mmHg (n=25)
Baseline 1yr p-value Baseline 1Yr p-valueLVH Absent 4(80%) 2( 40%) 0.51 8(32%) 15(60%) 0.04
Present 1(20%) 3(60%) 17(68%) 10(40%)Systolic Absent 4(80%) 2(20%) 0.51 16(64%) 19(76%) 0.35dysfunction Present1(20%) 3(60%) 9(36%) 6(24%)Diastolic Absent 2(40%) 3(60%) 0.53 8(32%) 9(36%) 1.00dysfunction Present3(60%) 2(20%) 17(68%) 16(64%)Pericardial Absent 4(80%) 5(100%) 0.29 22(88%) 21(84%) 0.64effusion Present 1(20%) 0( 0 %) 3(12%) 4(16%)
Table-5: Relationship between iPTH and echocardiographic changes.Echocardiographic iPTH (n=30) at baseline(pg/ml) iPTH (n=30) at 1Yr (pg/ml)parameters <300(n=20) >300(n=10) P-value <300(n=24) >300(n=6)P-value LVH Absent 11(55%) 1(10.0%) 0.048 14(58.33%) 3( 50%) 0.92
Present 9(45%) 9(90%) 10(41.66%) 3(50%)Systolic Absent 14(70%) 6(60%) 0.88 19(79.16%) 2(33.33%) 0.090dysfunction Present 6(30%) 4(40%) 5(20.83%) 4(66.66%)Diastolic Absent 9(45%) 0(0%) 0.019 11(45.83%) 1(16.66%) 0.40dysfunction Present 11(55%) 10(100%) 13(54.16%) 5(83.33%)Pericardial Absent 18(90%) 8(80%) 0.84 22(91.66%) 4(66.66%) 0.34effusion Present 2(20%) 2(20%) 2(8.33%) 2(33.33%) 0.34
Table-6: Relationship between Vit-D and echocardiographic changes.Echocardiographic Vit-D at baseline (ng/ml) Vit D level at 1 Yr (ng/ml)Parameters <30(n=12) >30(n=18) P-value <30(n=15) >30(n=15) P-valueLVH Absent 2(16.66%) 12(66%) 0.02 (46.66%) 10(66.6%) 0.46
Present 10(83.3%) 6(33.33%) (53.33%) 5(33.33%)Systolic Absent 7(58.33%) 13(72.2%)0.68 8(53.33%) 12(80%) 0.24dysfunction Present5(41.66%) (27.77%) 7(46.66%)3(20%)Diastolic Absent 1(8.33%) 9(50%) 0.04 5(33.33%) 7(46.66%) 0.70dysfunction Present11(91.6%) 9(50%) 10(66.6%) 8(53.33%)Pericardial Absent 9(75.0%) 17(94.4%)0.84 12(80%) 14(93.3%) 0.59effusion Present 3(25%) 1(5.55%) 3(20%) 1(6.66%)
Table-3: Hemoglobin level and echo-cardiographic changes of study population.Echocardiographic Hemoglobin levelparameters <10gm/dl (n=19) >10gm/dl (n=11)
Baseline 1yr p-value Baseline 1yr p-valueLVH Absent 5 (26.31%) 11( 57.9%)0.04 7(63.63%) 6(54.5%) 1.00
Present 14(73.68%) 8(42.1%) 4(36.36%) 5(45.5%)Systolic dysfunction Absent 11(57.89%) 17(89.4%)0.02 9(81.81%) 4(36.3%) 0.085
Present 8(42.1%) 2(10.5%) 2(18.18%) 7(63.6%)Diastolic dysfunctionAbsent 6(31.57%) 8(42.1%) 0.51 5(45.45%) 5(45.5%) 0.67
Present 14(73.68%) 12(63.1%) 6(54.54%) 6(54.54%)Pericardial effusion Absent 16(84.21%) 17(89.4%) 0.63 10(90.9%) 9(81.8%) 0.53
Present 3(15.78%) 2(10.5%) 1(9.09%) 2(18.18%)

12ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
pressure, suggesting a direct effect on attenuation ofventricular hypertrophy17. Preclinical studies also supporta role for vitamin D deficiency in the development of LVHin age related decline in kidney function and chronic kidneydisease patients18. Left ventricular diastolic dysfunction wassignificantly associated with Vit-D level of less than 30 ng/ml which contradicts to the study conducted by Hoorn etal and Anil Pandit et al. Whether this association was perse due to Vit-D insufficiency or diabetes mellitus andhypertension, it is difficult to ascertain because majorityof our study population had both the disease, which inturn can influence the diastolic function. Despite growingmedical literature suggesting Vit D deficiency is associatedwith cardiovascular disease, in a study conducted by AnilPandit et al, involving a large number of unselectedpatients, Vit D deficiency is not associated with LVdiastolic dysfunction and an abnormal LAV index19. Inhis study lack of association may be due to exclusion ofpatients with serum creatinine of more than 2mg/dl andadoption of different echocardiographic parameter fordiastolic dysfunction (LAVI). Recently, the Hoornstudy showed in a prospective manner that Vit D levelsat baseline were not associated with LAVI over asubsequent 8 years of follow-up20.
CONCLUSION :Some amount of cardiac function abnormality is
common in CKD patient due to various factors. Diastolicdysfunction is the commonest echocardiographicabnormality in ESRD patients on CAPD followed by LVHand systolic dysfunction. Significant BP control was seenat the end of study, though it was a short term study.Anemia is well known association of various forms ofcardiac function abnormalities. High iPTH level > 300pg/ml were significantly associated with LVH and diastolicdysfunction. Vit-D level of < 30 ng/ml was correlatedwell with presence of LVH and diastolic dysfunction. Toestablish the effects of iPH and Vit –D on heart in ESRDpatients on CAPD needs further well designed randomizedcontrol studies with large number of patients.Drawback:
Our study was a short term study with small numberof patients. Echocardiographic findings were not evaluatedin relation to the basic diseases. Adequacy of CAPD wasnot taken into account.
REFERENCE :1. Maiorca R et al. Morbidity and mortality of CAPD and
hemodialysis. Kidney Int 1993; (Suppl 40) : S4-152. Parfrey PS et al. Outcome and risk factors for left
ventricular disorders in chronic uremia.Nephol DialTransplant1996;11: 1277-1285.
3. London GM,Fabiani F et al. Uremic cardiomyopathy: Aninadequate lef ventricular hypertrophy.Kidney Int 31:973-980,1987.
4. Levin , Thompson CR, Either J,Carlisle EJF,TobeS,Mendelssohn D, Burgess E, Jindal K,Barrett B,SngerJ,Djurdjev O:Left ventricular mass index increases earlyin renal disease; Impact of decline in hemoglobinAm JKidney Dis 34:125-134,1999.
5. Lameire N,Bernaert P, Lambert MC,vijt D. Cardiovascularrisk factors and their management in patients oncontinuous ambulatory peritoneal dialysis. Kidney Int1994;46 (suppl 48) ) S31-38.
6. Del Greco, F.; Simon, NM.; Roguska, J.; Walker, C :Hemodynamic studies in chronic uremia. Circulation 40:87-95 (1969).
7. Ikram H, Lynn K.L; Bacley R.R, Little P.J: Cardiovascularchanges in chronic hemodialysis patients. Kidney into24: 371-376 (1983).
8. Friedman, H.S.; Shah, B.N.; Kim, H.G.;Bove, L.A.; DelMonte, M.M.; Smith, A.J.: Clinical study of the cardiacfindings in patients on chronic maintenancehemodialysis: the relationship to coronary risk factors.Clin. Nephrol. 16: 75-85 (1981).
9. Shivendra S, Doley PK, Pragya P, Shiv Sankar M, SinghVP, Singh Neelam et al: Echocardiographic changes inpatients with ESRD on maintenance hemodialysis- Asingle centre study:J Cardiovasc Dis and Diagn 2014, Vol-2,Issue 4.
10. S Agarwal, P Dangri, OP Karla, S Rajpal (2003) :Echocardiographic assessment of cardiac dysfunction inpatients of chronic renal failure.JIACM 4: 296-303).
11. Hunting J, Kramer W, Reitinger J, Kuhn K, Wizemann V,Schutterle G. Cardiac structure and function in continuousambulatory peritoneal dialysis: Influence of bloodpurification and hypercirculation. Am Heart J 1990: 119:344-52.
12. Huting J, Alpert MA. Progression of left ventricularhypertrophy in end-stage renal disease treated bycontinuous ambulatory peritoneal dialysis depends onhypertension and hypercirculation. Clin Cardiol 1992;15:190-196.
13. Lameire N: Cardiovascular risk factors and bloodpressure control in continuous ambulatory peritonealdialysis. Perit Dial Int 1993;13(Suppl 2):S394-S395.
14. Austin G. Stack Rajiv Saran: Clinical correlates andmortality impact of left ventricular hypertrophy amongnew ESRD patients in the United States. American journalof kidney disease: Volume-40,Issue-6,December 2002,Pages 1202-1210.)
15. RB Rando, LE Rohde, L Camerlato, JP Ribeiro and RCManfro: The role of secondary hyperparathyroidism inleft ventricular hypertrophy of patients under chronichemodialysis. Braz J Med Biol Res, September 2005,Volume 38(9) 1409-1416.
13ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
16. Singh NP,Sahni V Garg D and Nair M: Effect ofpharmacological suppression of secondaryhyperparathyroidism on cardiovascular hemodynamicsin predialysis CKD patients: A preliminary observation.Hemodial Int. 2007 Oct;11(4): 417-423.
17. Park CW, Oh YS, Shin YS, Kim CM, Kim YS, Kim SY, ChoiEJ, Chang YS, Bang BK. Intravenous calcitriol regressesmyocardial hypertrophy in hemodialysis patients withsecondary hyperparathyroidism.Am J KidneyDis. 1999;33:73–81.
CONSENT FORM FOR CASE REPORTS
For a patient’s consent to publication of information about them in a journal or thesis
Name of person described in article or shown in photograph :_________________________________
Subject matter of photograph or article : ________________________________________________
Title of article : __________________________________________________________________
Medical practitioner or corresponding author : ____________________________________________
I_________________________________ [insert full name] give my consent for this information about
MYSELF OR MY CHILD OR WARD/MY RELATIVE [insert full name]:__________________________,
relating to the subject matter above (“the Information”) to appear in a journal article, or to be used for thepurpose of a thesis or presentation.
I understand the following :1. The Information will be published without my name/child’s name/relatives name attached and every attempt will be made
to ensure anonymity. I understand, however, that complete anonymity cannot be guaranteed. It is possible that somebodysomewhere - perhaps, for example, somebody who looked after me/my child/relative, if I was in hospital, or a relative - mayidentify me.
2. The Information may be published in a journal which is read worldwide or an online journal. Journals are aimed mainly athealth care professionals but may be seen by many non-doctors, including journalists.
3. The Information may be placed on a website.4. I can withdraw my consent at any time before publication, but once the Information has been committed to publication it
will not be possible to withdraw the consent.
Signed:__________________________________ Date: ______________________
Signature of requesting medical practitioner/health care worker:
__________________Date:______________
18. Rahman A, Hershey S, Ahmed S, Nibbelink K, SimpsonRU. Heart extracellular matrix gene expression profile inthe vitamin D receptor knockout mice. J Steroid BiochemMol Biol. 2007;103:416–419.
19. Anil Pandit, Farouk Mookadam, Sailaja Boddu, Aryal Pandit,Alwar Tandar, Hari Chaliki,Stephen Cha and Howard R Lee:Vitamin D levels and left ventricular diastolic function OpenHeart 2014;1: doi:10.1136/openhrt-2013-000011.
20. Hoorn T, Zoccali C,Packham D et al:. Vitamin D reduces leftatrial volume in patients with left ventricular hypertrophy andchronic kidney disease. Am Heart J 2012;164:902–9.

14ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Depression in Type 2 Diabetes Mellitus : Prevalence andAssociation with Clinical and Sociodemographic Parameters
K Saikia*, B Choudhury** , A Choudhury*** , S K Agarwal*** , A K Bhuyan****
O r i g i n a l A r t i c l e
AbstractAims and Objective: To study the prevalence of depression in patients of type 2 Diabetes Mellitus as well as to
determine the association with different clinical and sociodemographic parameters. Material and Methods: Total 220subjects with type 2 Diabetes Mellitus were enrolled into the study between August 2014 to October 2014 in GauhatiMedical College which is a tertiary care centre in North-East India. Detailed history was taken and clinical examinations withrelevant investigations were done in all the subjects. Assessment of depression was done by the Assamese version of PHQ-9 questionnaire in each of the subjects. Binary logistic regression analysis was carried out to determine the association ofdifferent factors with depression. Results and Observation: The prevalence of depression was found to be 38.17% in ourstudy. Out of this the prevalence of severe depression was 18.18%, moderately severe 8.18%, moderate 4.54% and milddepression 7.27%. The following factors were found to be associated significantly with depression – longer duration of thedisease, higher HbA1c, being on insulin, presence of hypertension, presence of complications, unemployment, lower incomeand higher cost of medications. Factors that were not related to depression were – age, sex, BMI and use of OHA. Conclusion:A high prevalence of depression was found in patients with type 2 diabetes mellitus in North-East India. Several clinical andsociodemographic factors were identified which had a significant association with depression in these subjects.
*Assistant Professor of Endocrinology, Assam Medical College,Dibrugarh, ** Associate Professor, *** Senior Resident, **** Registrar,Department of Endocrinology, Gauhati Medical College, Guwahati.Correspondence Address : Dr. Bipul Choudhury, Associate Professor,Department of Endocrinology, Gauhati Medical College, Guwahati,Assam, India- 781032. E-mail : [email protected]
Key Words : Depression, Questionnaire
INTRODUCTION:The co-existence of diabetes and depression has been
highlighted by several studies. The chronic nature ofdiabetes is associated with significant morbidity andmortality, as well as substantial financial burdens on thepart of the patient. A more than co-incidental effect of thedisease is observed in the mental dimension also, in factthe relation between depression and diabetes has beenfound to be bidirectional. People with diabetes have beenfound to have 1.4-3 times higher prevalence of depressionas compared to healthy normal population1. Differentfactors like age, duration of diabetes, glycaemic control,presence of complications, employment, use of insulin etc.are implicated to have associations with depression inpeople with diabetes. Although studies from different partsof the world have addressed this, issue reports from Indiaare limited in number. The present study was therefore
undertaken with the objective to study the prevalence ofdepression in type 2 diabetes mellitus and to find theassociation of clinical and sociodemographic parametersof diabetic patients with depression.
MATERIAL AND METHODS :The present study was done between August 2014
to October 2014 in Gauhati Medical College & Hospital,which is a tertiary care hospital in Assam, India. Total220 patients of type 2 diabetes mellitus, of all age groupsand either sex, were enrolled into the study. A detailedhistory of the subjects including demographic profile,socioeconomic status and monthly cost of therapy wasrecorded. Thorough physical examination was done inall subjects. The Assamese version of PHQ-9questionnaire was used to assess the presence as well asdegree of depression. Scores of 5, 10, 15 & 20 weretaken as cut off points for mild, moderate, moderatelysevere and severe depression respectively, as per PHQ-9 instruction manual. Patients having the inability tocomprehend the written questionnaire were excludedfrom the study. BMI was determined in the subjects byusing the formula weight (kg) /height (m2 ). Blood pressure
15ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
was measured by applying the cuff in right arm of the patientin supine position while measuring twice at 15 minuteintervals and the average of the two values were taken.Retinopathy was diagnosed based on fundus examination.Spot urinary albumin to creatinine ratio (UACR) e” 30mg/gm or serum creatinine level more than 1.5 mg/dl inmales and 1.4 mg/dl in females indicated presence ofnephropathy. Neuropathy was diagnosed clinically by thepresence of impaired vibration sense on testing by 128Hz tuning fork, impaired response to testing with 10 gmmonofilament, impaired response to pin prick and loss ofankle jerk. Whenever the results of nerve conductionresults were available from the patient’s records they wereused as additional data for the presence of neuropathy.ECG was done in all cases with echocardiography inselected patients. History of coronary artery disease, ifany, was recorded. History of CVA was recorded whenpresent, and previous records were reviewed. Peripheralvascular disease was assessed clinically by ankle brachialindex along with Doppler study in selected patients. Theestimation of HbA1c was done by HPLC method.
Statistical analysis was done by SAS 9.3. Data wereexpressed as mean, standard deviation and proportions.Binomial regression analysis was carried out to determinethe association of independent factors with depression.
RESULTS & OBSERVATION :A total of 220 cases were evaluated. The clinical and
demographic characteristics of the study subjects arestated in table 1.
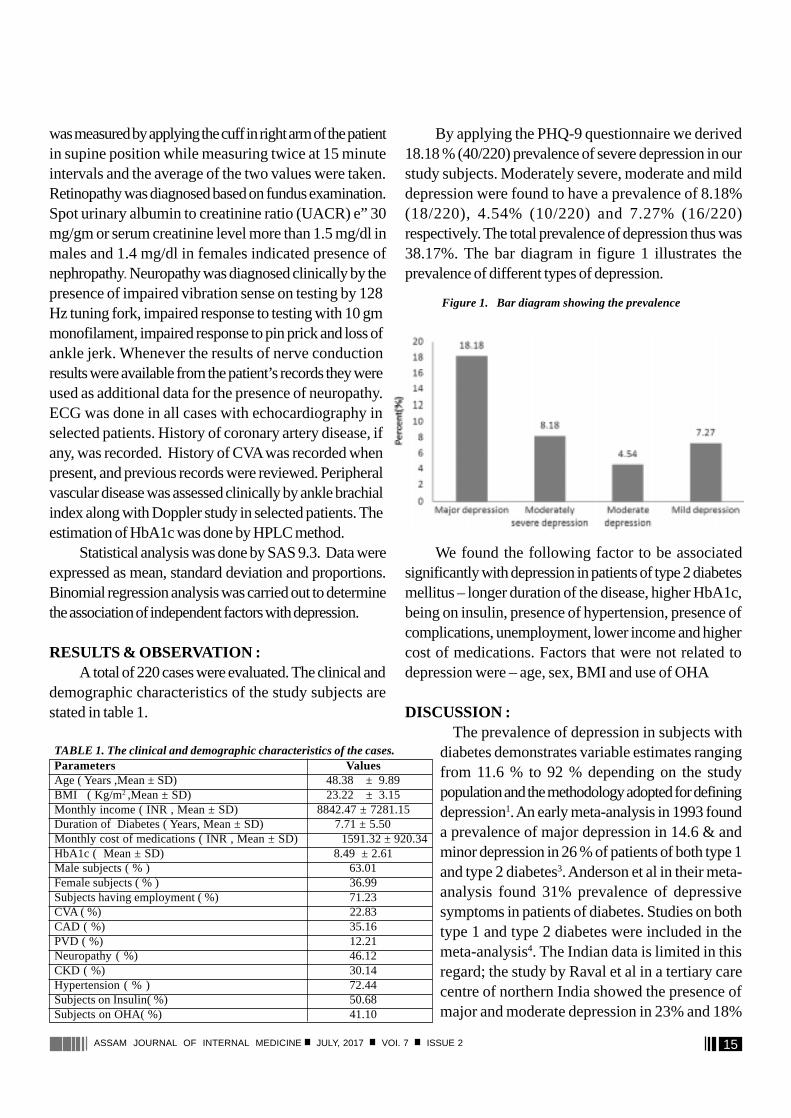
By applying the PHQ-9 questionnaire we derived18.18 % (40/220) prevalence of severe depression in ourstudy subjects. Moderately severe, moderate and milddepression were found to have a prevalence of 8.18%(18/220), 4.54% (10/220) and 7.27% (16/220)respectively. The total prevalence of depression thus was38.17%. The bar diagram in figure 1 illustrates theprevalence of different types of depression.
We found the following factor to be associatedsignificantly with depression in patients of type 2 diabetesmellitus – longer duration of the disease, higher HbA1c,being on insulin, presence of hypertension, presence ofcomplications, unemployment, lower income and highercost of medications. Factors that were not related todepression were – age, sex, BMI and use of OHA
DISCUSSION :The prevalence of depression in subjects with
diabetes demonstrates variable estimates rangingfrom 11.6 % to 92 % depending on the studypopulation and the methodology adopted for definingdepression1. An early meta-analysis in 1993 founda prevalence of major depression in 14.6 & andminor depression in 26 % of patients of both type 1and type 2 diabetes3. Anderson et al in their meta-analysis found 31% prevalence of depressivesymptoms in patients of diabetes. Studies on bothtype 1 and type 2 diabetes were included in themeta-analysis4. The Indian data is limited in thisregard; the study by Raval et al in a tertiary carecentre of northern India showed the presence ofmajor and moderate depression in 23% and 18%
TABLE 1. The clinical and demographic characteristics of the cases.Parameters ValuesAge ( Years ,Mean ± SD) 48.38 ± 9.89BMI ( Kg/m2 ,Mean ± SD) 23.22 ± 3.15Monthly income ( INR , Mean ± SD) 8842.47 ± 7281.15Duration of Diabetes ( Years, Mean ± SD) 7.71 ± 5.50Monthly cost of medications ( INR , Mean ± SD) 1591.32 ± 920.34HbA1c ( Mean ± SD) 8.49 ± 2.61Male subjects ( % ) 63.01Female subjects ( % ) 36.99Subjects having employment ( %) 71.23CVA ( %) 22.83CAD ( %) 35.16PVD ( %) 12.21Neuropathy ( %) 46.12CKD ( %) 30.14Hypertension ( % ) 72.44Subjects on Insulin( %) 50.68Subjects on OHA( %) 41.10
Figure 1. Bar diagram showing the prevalence

16ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
of patients of type 2 diabetes respectively5. Ourobservations are reflective of the pattern in a tertiary carecentre of the north-eastern India – a prevalence of 38.17%with 18.18% severe, 8.18% moderately severe, 4.54%moderate and 7.27% mild depression.
We found that the presence of micro andmacrovascular complications of diabetes have a significantassociation with depression. Several studies report similarfindings. Roy et al found depression to be a risk factor forretinopathy in subjects of type 1 diabetes6. Lin et al in aprospective cohort study of 4623 subjects of type 2diabetes found major depression to be associated withadverse microvascular and macrovascular outcomes7. Inanother longitudinal study by Clouse et al in women withdiabetes a significantly increased risk of having clinicallyevident coronary heart disease was found in subjects withmajor depression8.
Poor glycaemic control, as reflected by a higherHbA1c, had a significant association with depression inour study subjects. Glycaemic control as a risk factor fordepression is a conflicting issue, with non-uniform resultsof the studies seeking the relationship between the two. Ameta-analysis by Lustman et al in 2000 found depressionto be significantly associated with hyperglycaemia9. Thestudy of Papelbaum et al demonstrated higher levels ofglycated haemoglobin in patients of type 2 diabetes withdepression10. Similarly Wagner et al showed theassociation of higher depressive symptoms symptoms withhigher HbA1c11. Other studies have however found nosignificant association between glycaemic control anddepressive symptoms12-16. This difference might beattributed to the variation of study methodologies.
The duration of diabetes has been found to beassociated with depression17. We observed a longerduration of the disease to be associated significantly withdepression. We also found that the form of therapy alsoaffected psychological health. The prevalence ofdepression was more among insulin users, whereassubjects who were on oral hypoglycaemic agents (OHA)did not show this association. The study of Peyrot et aldemonstrates findings similar to this observation18. Several demographic and psychosocial factors areimplicated to have association with depression in subjectswith diabetes - age, female sex, lower education andsocioeconomic status, unemployment, lack of social
support, presence of other medical diseases, smokingetc19-24. We found the significant association of the followingfactors with depression - unemployment, lower incomeand higher cost of medications. Age, sex & BMI – thesefactors were not related to depression in our study. There are certain limitations to our study. As the studywas cross-sectional no prospective data could be obtainedto observe the effect of different factors in the developmentof depression. The study sample was also small and hencethe data may not be extrapolated to a larger sample size.
CONCLUSION :The present study underscores the high prevalence
of depression among patients of type 2 diabetes mellitusin north-east India and identifies the independent factorsthat are associated with it. The significant association ofdiabetes with depression stresses the need for carefulconsideration in the management of patients with diabetesmellitus.
REFERENCES :1. Andreoulakis E, Hyphantis T, Kandylis D ,Iacovides A :
Depression in diabetes mellitus: a comprehensive review ;HIPPOKRATIA 2012; 16(3): 205-214.
2. Spitzer RL, Kroenke K, Williams JB. Validation and utility of aself-report version of PRIME-MD: the PHQ primary care study.Primary Care Evaluation of Mental Disorders. Patient HealthQuestionnaire. JAMA 1999; 282: 1737-44.
3. Gavard JA, Lustman PJ, Clouse RE : Prevalence of depressionin adults with diabetes. An epidemiological evaluation; DiabetesCare 1993; 16: 1167-1178.
4. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ : Theprevalence of comorbid depression in adults with diabetes. Ameta-analysis. Diabetes Care 2001; 24: 1069-1078.
5. Raval A, Dhanaraj E, Bhansali A, Grover S, Tiwari P: Prevalence& determinants of depression in type 2 diabetes patients in atertiary care centre. Indian J Med Res. 2010 Aug: 132;195-200.
6. Roy MS, Roy A, Affouf M : Depression is a risk factor for poorglycemic control and retinopathy in African-Americans with type1 diabetes. Psychosom Med. 2007; 69: 537-542.
7. Lin EH, Rutter CM, Katon W, Heckbert SR, Ciechanowski P,Oliver MM, et al : Depression and advanced complications ofdiabetes: a prospective cohort study. Diabetes Care. 2010; 33:264-269.56.
8. Clouse RE, Lustman PJ, Freedland KE, Griffith LS, McGill JB,Carney RM : Depression and coronary heart disease in womenwith diabetes. Psychosom Med. 2003; 65: 376-383.
9. Lustman PJ, Anderson RJ, Freedland KE, De Groot M, CarneyRM, Clouse RE : Depression and poor glycemic control. A meta-analytic review of the literature. Diabetes Care. 2000; 23: 934-942.
10. Papelbaum M, Moreira RO, Countinho W, Kupfer R, Zagury L,Freitas S, et al : Depression, glycemic control and type 2 diabetes.Diabetol Metab Syndr. 2011; 3: 26-29.
11. Wagner JA, Abbott GL, Heapy A, Yong L : Depressive symptomsand diabetes control in African Americans. J Immigr Minor Health.2009; 11: 66-70.
17ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
1. Letter of submission.2. Copyright statement signed by all the authors.3. Three copies of manuscript with copies of illustrations attached to each.4. Title page
Title of manuscriptFull name(s) and affiliations of author (s); institution(s) and city(ies) from which work originated.Name, Address, Telephone, Fax numbers and e-mail address of corresponding author.Number of pages, number of figures and number of tables.
5. Structured abstract (objectives, methods, results, conclusion) alongwith title, and key words6. Article proper (double spaced on A/4 size paper).7. Acknowledgements (separate sheet).8. References (double spaced, separate sheet, Vancouver style).9. Maximum number of references for Original articles - 20, Short articles - 10, Case reports - 6, Documentation - 3,
Correspondence - 3.10. Each table on separate sheet.11. Figures/diagrams on separate sheet.12. Photographs in envelope appropriately marked.13. Covering letter signed by all authors confirming that they have read and approved the contents and also confirming that
the manuscript is not submitted or published elsewhere.14. Statement regarding Ethics Committee Approval and informed consent from subjects.15. CD's / DVD's are essential.16. Online submission : [email protected]. Mailing Address : Prof. Sanjeeb Kakati, Editor, Assam Journal of Internal Medicine, Department of Medicine, Assam
Medical College, Dibrugarh, Assam, India. PIN-786002.
Manuscript Submission : Check list for Contributors
A r t i c l e S u b m i s s i o nASSAM JOURNAL OF INTERNAL MEDICINE
12. Grey M, Whittemore R, Tamborlane W. Depression in Type 1diabetes in children. Natural history and correlates. J PsychosomRes. 2002; 53: 907– 911.
13. Ciechanowski PS, Katon WJ, Russo JE, Hirsch IB : Therelationship of depressive symptoms to symptom reporting,self-care and glucose control in diabetes. Gen Hosp Psychiatry.2003; 25: 246-252.
14. Surwit RS, van Tilburg MAL, Parekh PI, Lane JD, Feinglos MN: Treatment regimen determines the relationship betweendepression and glycemic control. Diabetes Res Clin Pract. 2005;69: 78-80.
15. Paschalides C, Wearden AJ, Dunkerley R, Bundy C, Davies R,Dickens CM : The associations of anxiety, depression andpersonal illness representations with glycaemic control and healthrelated quality of life in patients with type 2 diabetes mellitus. JPsychosom Res. 2004; 57: 557-564.
16. Egede LE, Ellis C, Grubaugh AL. The effect of depression onself-care behaviors and quality of care in a national sample ofadults with diabetes. Gen Hosp Psychiatry. 2009; 31: 422-427.
17. Talbot F, Nouwen A, Gingras J, Belanger A, Audet J: Relationsof diabetes intrusiveness and personal control to symptoms of
depression among adults with diabetes.Health Psychol 1999;18:537–542.
18. Peyrot M, Rubin RR: Levels and risks of depression and anxietysymptomatology among diabetic adults. Diabetes Care 1997;20: 585–590.
19. Egede LE, Zheng D : Independent factors associated with majordepressive disorder in a national sample of individuals withdiabetes. Diabetes Care. 2003; 26:104 –111.
20. Egede LE, Zheng D, Simpson K: Comorbid depression isassociated with increased health care use and expenditures inindividuals with diabetes.Diabetes Care 2002; 25:464–470.
21. Friis R, Nanjundappa G: Diabetes, depression and employmentstatus. Soc Sci Med 1986 ; 23:471–475,
22. Hanninen JA, Takala JK, Keinanen-Kiukaanniemi SM:Depression in subjects with type 2 diabetes: predictive factorsand relation to quality of life. Diabetes Care. 1999; 22:997–998.
23. Haire-Joshu D, Heady S, Thomas L, Schechtman K, Fisher EBJr: Depressive symptomatology and smoking among personswith diabetes.Res Nurs Health 1994 ;17: 273–282.
24. Roy A, Roy M: Depressive symptoms in African-American
type 1 diabetics. Depress Anxiety. 2001 ;13:28–31. 1986.
18ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Assessment of volume of bleed in Intra-cerebralHemorrhage as a reliable and easy to use yardstick
in prediction of 7 day mortalityD Das*, K Bhattachrjee** , S K Ghintala***
O r i g i n a l A r t i c l e
AbstractBackground : Intra-cerebral hemorrhage is extravasation of blood into the brain parenchyma and its mortality rates
change depending on the volume, severity and site of bleed inside the brain parenchyma. The present study was undertaken tomeasure the volume of intra-cerebral bleed and correlate the same with mortality within 7 days of presentation to hospital.Aims and objectives: To determine 7 days mortality according to volume of intra-cerebral bleed and to predict the prognosisusing Glasgow Coma Scale. Material and methods: The study was conducted in the Medicine department of a tertiary careteaching hospital of north eastern India.The admitted patients diagnosed as cerebrovascular accidents on the basis of CT brain ashaving intra-cerebral hemorrhage were included in the study. Study design: Hospital based single centered observational study.Results and observations: In this study out of total 100 patients of intra-cerebral bleed, 60 were finally selected on the basisof inclusion and exclusion criteria,which constituted the study group and were analyzed. Of the 60 cases 78.3% were males and21.7% were females. Maximum numbers of cases were between 65-75 years of age constituting 50% of cases. Hypertension, whichis the major risk factor for intra-cerebral hemorrhage was identified in 75% cases of which males and females constituted 77.8%and 22.2% respectively. Bleeding volume more than 50 ml, 30-50 ml and less than 30ml were found in 23.3%, 33.3% and 43.4%cases respectively.Upon observing the mortality pattern, patients who suffered bleed volume of >50ml had 85.7% mortality with100% hypertension. Hypertension can be considered as one of the risk factors because patients with a ICH volume >50ml withhypertension showed higher mortality rate. Glasgow Coma Scale is also a good predictor of mortality though not statisticallysignificant. Conclusion: Hematoma volume is a significant yardstick which plays a role in influencing the functional outcome,prognosis and mortality. It may be worth mentioning that the ICH volume of 50 ml or more is probably as significant as a volumeof 60 ml or more determining the clinical severity, final outcome including mortality in patients with ICH.
* Associate Professor, ** Associate Professor, *** Post Graduate trainee,Department of Medicine, Silchar Medical College, Silchar.Correspondence Address : Dr Dwijen Das, Associate Professor,Department of Medicine, Silchar Medical College & Hospital, PO-Ghungoor, City: Silchar, Dist.. Cachar, State- Assam.
Keywords: Brain, Cerebral hemorrhage, Hematoma,Hypertension, Risk factor.
INTRODUCTION :Intra-cerebral hemorrhage (ICH) is the extravasation
of blood into the brain parenchyma and is most commonin elderly and its incidence is more in those receivinganticoagulant therapy1. The mortality rates changedepending on the volume of bleed, severity and site ofbleed inside the brain parenchyma2. Hypertension andamyloid angiopathy are the primary causes whilecoagulopathy, trauma, intracranial neoplasm, drugs are thesecondary causes for intracranial hemorrhage3. The volumeof bleeding depicted in CT scan brain has the potentialprognostic capability to find the mortality rate in intracerebral hemorrhage cases4. The CT scan imaging of thebrain is the standard investigation to detect the presence
or absence of intra-cerebral hemorrhage and it is moresensitive than MRI brain for the detection of acutebleed5.The population studies reported 30 days mortalityof 44% -51% in ComputedTomographic era6. Themortality of patients depend more on the volume ofhemorrhage, lesser extent on the level of impairment ofconsciousness and other factors7. If the volume of intra-cerebral hemorrhage increases in size after hospitaladmission, it may worsen the outcome. Studies have beencorrelating the volume of bleed and mortality 8. The presentstudy was undertaken to measure the volume of intra-cerebral bleed and correlate the same with mortality within7 days of presentation to hospital.
AIMS AND OBJECTIVES :1.To determine 7 days mortality according to volume ofICH.2. To determine the prognosis of patient using GlasgowComa scale (GCS) for first 7 days.MATERIAL AND METHODS :STUDY SETTING-
19ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
The present study was conducted in the department ofMedicine in a tertiary care teaching hospital in NorthEastern India for a period of one year.
STUDY DESIGN :The present study was a hospital based single
centered observational study.The patients who were admitted in the department
of Medicine, Silchar Medical College with cerebrovascularaccidents and diagnosed on the basis of CT brain as havingintra-cerebral hemorrhage were included in the study. Eachpatient was followed up for a period of one week duringwhich they were treated with anti-hypertensives, anti-cerebral edema measures as well as interventions to preventaspiration pneumonia, bedsores and sepsis and otherassociated complications.
Inclusion criteria :One hundred cases of new onset cerebrovascular
accidents (onset within 2 days) diagnosed clinically andCT brain correlation as intra-cerebral hemorrhage,admitted in the Medicine department were included in thestudy.
Exclusion criteria-Presence of factors which could alter the outcome
like patients with intra-ventricular extension of the bleed,ischemic stroke, intra-cerebral tumors, presence ofaspiration pneumonia or sepsis at the time of presentationor during the course of stay in the hospital, presence ofconcurrent subdural, extradural and subarachnoidhemorrhage, use of antiplatelet medication (Aspirin),anticoagulant medication (Warfarin),Diabetes Mellitus(DM), previous history of ischemic or hemorrhagic stroke,past or present evidence of coronary artery disease,acuteor chronic kidney diseases, chronic liver disease,decompensated chronic pulmonary diseases andcoagulopathies and malignancies anywhere in the bodywere excluded from the study.
Thorough clinical history and physical examinationswere done in each case. Necessary investigations includingcomplete blood count, fasting blood glucose, blood urea,serum(s.) creatinine, s. sodium, s. potassium, fasting lipidprofile, liver function test, X-ray chest, ultrasound abdomenand fundoscopy based on indications were undertaken.
Hematoma size was calculated by using formula ABC/2, where A is the greatest hemorrhage diameter by CT, Bis the diameter 90° to A, and C is the thickness ofhemorrhage, the total volume of hemorrhage is estimated.According to Luby et al. (2012), the ABC/2 method isthe most sensitive, reliable and accurate of all.
Glasgow Coma Scale (GCS) was used to measurethe neurological status. The patients’ GCS at day 1 andday 7 were recorded.
Statistical analysis was done and p value < 0.05 wastaken as statistical significant.
RESULTS AND OBSERVATION :In this study out of total 100 patients of intra-cerebral
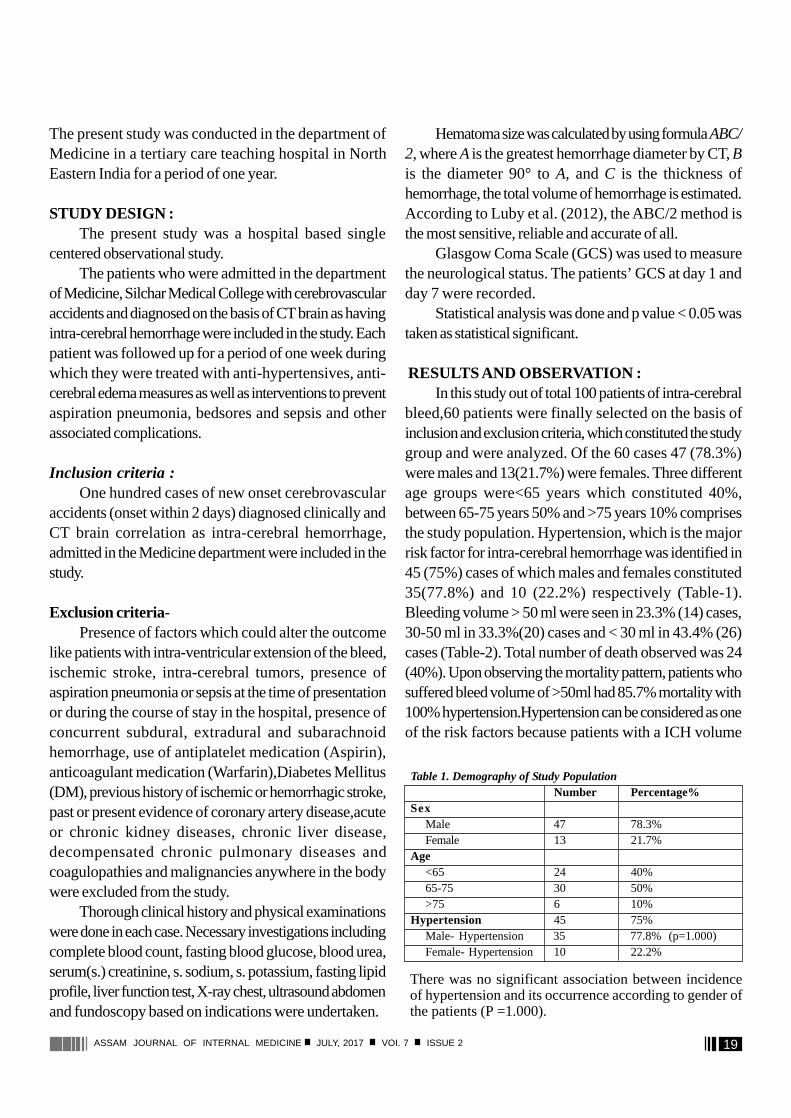
bleed,60 patients were finally selected on the basis ofinclusion and exclusion criteria, which constituted the studygroup and were analyzed. Of the 60 cases 47 (78.3%)were males and 13(21.7%) were females. Three differentage groups were<65 years which constituted 40%,between 65-75 years 50% and >75 years 10% comprisesthe study population. Hypertension, which is the majorrisk factor for intra-cerebral hemorrhage was identified in45 (75%) cases of which males and females constituted35(77.8%) and 10 (22.2%) respectively (Table-1).Bleeding volume > 50 ml were seen in 23.3% (14) cases,30-50 ml in 33.3%(20) cases and < 30 ml in 43.4% (26)cases (Table-2). Total number of death observed was 24(40%). Upon observing the mortality pattern, patients whosuffered bleed volume of >50ml had 85.7% mortality with100% hypertension.Hypertension can be considered as oneof the risk factors because patients with a ICH volume
Table 1. Demography of Study PopulationNumber Percentage%
SexMale 47 78.3%Female 13 21.7%
Age<65 24 40%65-75 30 50%>75 6 10%
Hypertension 45 75%Male- Hypertension 35 77.8% (p=1.000)Female- Hypertension 10 22.2%
There was no significant association between incidenceof hypertension and its occurrence according to gender ofthe patients (P =1.000).
20ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
>50ml with hypertension showed an increased mortalityrate.
DISCUSSION :Cerebrovascular diseases have recently emerged as
a major health problem affecting the population includingdeveloping countries like India. Its incidence has increasedmany folds lately with the emergence of several riskfactorslike coronary artery diseases, diabetes mellitus,hypertension, dyslipidemia and significant contribution fromincreased life expectancy9,10,11. Other factors influencingthe incidences are smoking, stress and sedentary lifestyleand probably dietary habits. Intra-cerebral hemorrhagecan be caused by a variety of etiological factors like headtrauma, transformation of prior ischemic lesion, metastaticbrain tumors, drugs like cocaine, amphetamine, arterio-venous malformations, amyloid angiopathy and capillarytelangiectasias12,13. A 60ml of blood volume is almost fatal
to the patient and mortality rate in this group of patients aremuch higher than comparison with those with smaller volumeof ICH. A blood volume of 3cm in diameter carries a poorprognosis, 3cm-1cm in diameter carries a moderate and<1cm in diameter carriers a favorable outcome14. Thusvolume of blood is one of the factors that can influence theoutcome.
In the present series 78.3% cases were males and21.7% were females, whereas Junshan Zhouet al.24
reported 64.2% males and 35.8% females in their seriesof 615 ICH patients.
In the present series 50% patients were in the agegroup of 65-75 years, which is almost in agreement withthe series reported by Togha M and Bakhtavar K21 whofound 69% of subjects between 60 to 80 years of age. Inthe present series mortality was observed in 40% cases,which is in agreement with the study by Joseph P.Broderick15 who reported 44% mortality in theirseries.Flaherty ML et al.23 in their study reported 31%mortality in 7 days.
In the present study patients with a ICH volume >50 ml, 30-50ml and <30 ml showed mortality in85.7%,40% and 15.4% cases respectively. Joseph P.Broderick15 in their series reported 30 day mortality in93%, 64% and 23% in patients with ICH volume >60 ml,30-60 ml and <30 ml in their series.Similarly SalihovicDet al. reported mortality rate of 85%, 62.5% and 36%in ICH volume >60ml, 30-60ml and <30 ml respectivelyintheir series.20On literature search no data was found tocompare the mortality according the ICH volume >50 ml,30-50 ml and <30 ml.
According to Molshatzkiet al. the mean hematomavolume for a severe stroke was 50.2 ml16. The FUNCscore by Rost et al said that the hemorrhage size is usedfrequently in clinical decisions in patients with ICH, andscores predicting mortality and good functional outcomehave been developed using ICH volumes categorized as<30 cm3, 30 to 60 cm3, and >60 cm3.17
Although a number of studies have been undertakenconsidering 60 ml volume of bleed as a severe mode ofstroke presentation, the present series observes that avolume of bleed equivalent to 50 ml or more worsens theprognosis towards a disastrous outcome and as such itwas felt that for better awareness on the part of the clinician,a volume of bleed of 50 ml or more should be considered to
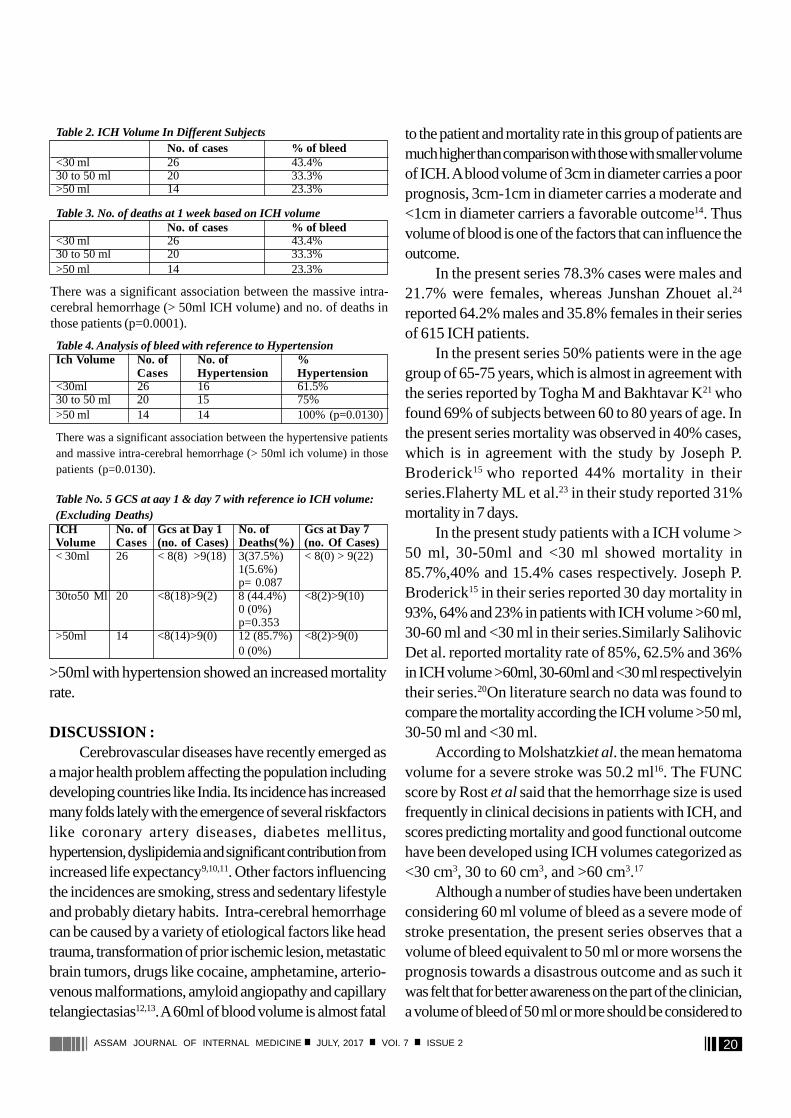
Table 4. Analysis of bleed with reference to HypertensionIch Volume No. of No. of %
Cases Hypertension Hypertension<30ml 26 16 61.5%30 to 50 ml 20 15 75%>50 ml 14 14 100% (p=0.0130)
There was a significant association between the hypertensive patientsand massive intra-cerebral hemorrhage (> 50ml ich volume) in thosepatients (p=0.0130).
Table No. 5 GCS at aay 1 & day 7 with reference io ICH volume:(Excluding Deaths)ICH No. of Gcs at Day 1 No. of Gcs at Day 7Volume Cases (no. of Cases) Deaths(%) (no. Of Cases)< 30ml 26 < 8(8) >9(18) 3(37.5%) < 8(0) > 9(22)
1(5.6%)p= 0.087
30to50 Ml 20 <8(18)>9(2) 8 (44.4%) <8(2)>9(10)0 (0%)p=0.353
>50ml 14 <8(14)>9(0) 12 (85.7%) <8(2)>9(0)0 (0%)
Table 2. ICH Volume In Different SubjectsNo. of cases % of bleed
<30 ml 26 43.4%30 to 50 ml 20 33.3%>50 ml 14 23.3%
Table 3. No. of deaths at 1 week based on ICH volumeNo. of cases % of bleed
<30 ml 26 43.4%30 to 50 ml 20 33.3%>50 ml 14 23.3%
There was a significant association between the massive intra-cerebral hemorrhage (> 50ml ICH volume) and no. of deaths inthose patients (p=0.0001).

21ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
bear a fatal outcome especially in the developing countries.All these values are quite different from our
observation. Our study suggests that 60 cm3 hematomavolume is too high to call it a severe stroke, if the hematomais as large as 50 cm3, it can be stamped as severe stroke.This also supports the view of Hemphill et al. in “TheICH score” published in Stroke 2001 where they havementioned that hematoma volume >30 cm3 is anindependent poor prognostic factor for 30-day mortalityand morbidity18. This proposition is in alignment with theviews of Hemphill et al.18,19 where hematoma volumeexceeding 30cm3 was considered an independent poorprognostic factor not only in terms of 30-day mortalityand morbidity but also in the longer duration of 1 yearfunctional outcome. However, the present series studiedthe outcome for shorter period.
In the present series hypertension was significantlyassociated with the cases having fatal outcome and wasdetected in all cases with ICH volume >50 ml andhypertension was present in 75% of the total casesirrespective of volume of bleed, whereas A H G Rasooletal.25 reported hypertension in 90% of patients with acuteICH and reported it as one of the important contributor ofmortality in ICH which is similar with the findings of thepresent study. However the contributing role of hypertensionin influencing the presentation, prognosis and outcome inICH needs to be evaluated in a series comprising of largenumber of cases vis-a-vis control over an extended duration.
CONCLUSION :ICH is an extremely critical and life threatening
condition which may alter the fate of the sufferer in secondsrather than minutes. It is prudent for the clinicians to developstrategies to cope with this menace. Hematoma volume isa significant yard-stick which play a role in developingtreatment strategy and influence the functional outcome,prognosis and mortality. It may be worth mentioning thatthe ICH volume of 50 ml or more is probably as significantas a volume of 60 ml or more determining the clinicalseverity and mortality in patients with ICH.
REFERENCES :1. Gebel JM, Broderick JP. Intracerebral hemorrhage. NeurolClin
2000; 18: 419-38.2. Flaherty ML, Woo D, Haverbush M, Sekar P, Khoury J,
Sauerbeck L. et.al.Racial variations in location and risk ofintercerebral hemorrhage. Stroke 2005; 4: 662-72.
3. Qureshi AI, Tuhrim S, Broderick JP, Batjier HH, Hondo H, HanleyDF. Spontaneous intracerebral hemorrhage. N Engl J Med 2001;344: 1450-60.
4. Narayan RK, Maas AL, Servadei F, Skolnick BE, Tillinger MN,Marshall LF. Progression of traumatic intracerebral hemorrhage: aProspective observational study. J Neurotrauma 2008; 25(6): 629-39.
5. Chelsea S, Julio A, Sidney S, Michael et.al. Comparison of MRI andCT fordetection of Acute Interacerebral Hemorrhage. JAMA 2004;292(15): 1823- 1830.
6. Tuhrim S, Dambrosia J, Price T, Mohr J, Wolf P, Hier D, Kase C.Intracerebralhemorrhage: external validation and extension of a modelfor prediction of30-day survival. Ann neurol 1991; 29:658-663.
7. Portenoy R, Lipton R, Berger A, Lesser M, Lantos G.Intracerebralhaemorrhage: a model for the prediction of outcome.J NeurolNeurosurg Psychiatry 1981; 50: 976-979.
8. Yanaka K, Kamezaki T, Yamada T, Takano S, Meguro K, Nose T. Acutesubdural hematoma prediction of outcome with a linear discriminantfunction. Neurol Med Chir(Tokyo)1993; 33(4): 552-8.
9. Guohong C, Yanfen Z, Weijun T. Risk factors for intracerebralhemorrhage andcoronary heart diseases over a 3-year period inpatients admitted to some hospital of Tongliao city of NeiMonggolAutonomous Region: Retrospective analysis on case data. NeuralRegeneration Research 2007; 2(9): 569-573.
10. Adrin A, Juan M, Luis G E, Montserrat O, Cecilia T. Diabetes is anindependentrisk factor for in-hospital mortality from acutespontaneous intracerebralhemorrhage. Diabetes Care 2000; (23):1527-1532.
11. Roman H, Ivanka V, Jan M, Bohdan K,Martin G, Helena V, Stanislavl.Occurrence of dyslipidemia in spontaneous intracerebralhemorrhage. European Journal of Lipid Science andTechnology2006; 108(5): 383-388.
12. Jose LRS, Carlos C, Fernando B. Intracerebral hemorrhage in youngpeople analysis of risk factors, location, causes, and prognosis.Stroke 1991; 30: 537-541.
13. Marianna S, Daniel GK, Michael A, Alan M, Joyce, L, Rudy J.Cocaineinduced intracerebral hemorrhage in a patient with cerebralAmyloid Angiopathy. Journal of ForensicSciences 2010; 55(5):1389-1392.
14. Stephan AM, Fred R. Treatment of intracerebralhaemorrhage.Lancet Neurol 2005; 4: 662-672.
15. Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G. Volumeofintracerebral hemorrhage: a powerful and easy-to-use predictorof 30-daysmortality. Strok 1993;24(7):987-993.
16. Molshatzki N, Orion D, Tsabari R, Schwammenthal Y, MerzeliakO, Toashi M, et al. Chronic kidney disease in patients with acuteintracerebral hemorrhage: Association with large hematoma volumeand poor outcome. CerebrovascDis 2011;31:271 7
17. Rost NS, Smith EE, Chang Y, Snider RW, Chanderraj R, Schwab K, et al.Prediction of functional outcome in patients with primary intracerebralhemorrhage: The FUNC score. Stroke 2008;39:2304 9.
18. Hemphill JC 3rd, Bonovich DC, Besmertis L, Manley GT, JohnstonSC. The ICH score: A simple, reliable grading scale for intracerebralhemorrhage. Stroke 2001;32:891 7.
19. Hemphill JC 3rd, Farrant M, Neill TA Jr. Prospective validation ofICH score for 12 month functional outcome. Neurology2009;73:1088 94.
20. Salihovic D, Smajlovic D and Ibrahimagic OC. Does the volume andlocalization of intracecerebral hematoma affect short-term prognosisof ptaients with intracerebral hemorrhage? ISRN Neuroscience 2013May 8; 2013: 327968. Doi 10.1155/2013/327968.
21. Togha M, Bakhtavar K. Factors associated with in-hospital mortalityfollowing intracerebral hemorrhage: a three –year study in Tehran,Iran. BMC Neurology 2004;4:9. Doi: 10.1186/1471-2377-4-9.
22. Tuhrim S, Horowitz DR, Sacher M: Validation and comparison ofmodels predicting survival following intracerebral hemorrhage. CritCare Med. 1995; 23: 950-954. Doi: 10.1097/00003246-199505000-00026.
23. Flaherty ML, Haverbusch M, Sekar P, et al. Long-term mortalityafter intracerebral hemorrhage. Neurology. 2006; 66:1182–86.
22ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Clinical Profile of Cryptococcal Meningitis :Hospital Based Study
S Bawri*, M Das** , A Kayal*** , M Goswami*** , L J Basumatary**** , P Borah****
O r i g i n a l A r t i c l e
AbstractBackground : Cryptococcosis is a fungal infection caused by encapsulated yeast of the genus Cryptococcus and most cases
are caused by Cryptococcus neoformans. Material and Method: The aim of the study is to study the clinical profile ofcryptococcal meningitis. This is a prospective observational study conducted from September 2014 –September 2016 at GauhatiMedical College. Detailed neurological evaluation along with investigation was done in all the patients. Results and Observations: A total of 16 patients were included among which 10 patients were immunocompromised (7 were HIV positive, 3 onimmunosuppressant drug) and 6 were immunocompetant. 13 were male and 3 were female. Mean age was 35 ± 4 years andduration of symptom was 2 weeks ± 4 days/3 weeks ± 5 days for immunocompromised / immunocompetant patients. Mostcommon features were headache(81%), vomiting(75%),altered sensorium(62%),fever(56%),seizure(43%),neck rigidity(93%),Papilloedema(93%).Baseline investigations were normal and Cerebrospinal Fluid(CSF) analysis revealed with low to normalsugar and normal protein with normal Adenosine Deaminase and Cryptococcal Antigen was positive in all patients.CD4 countswas d”100 in all HIV patients. Computerized Tomography (CT) Scan revealed normal in 6, hydrocephalus in 6 & cerebral oedemain 4 patients. Magnetic Resonance Imaging (MRI) showed leptomeningeal enhancement in 4 & enlarged Virchow Robin spaces in6 patients. Out of 16 patients, 6 patients succumbed. Conclusion: In the present study, patients presented with headache,vomiting, altered sensorium with positive meningeal signs .On evaluation cryptococcal antigen was positive and Patients weretreated with antifungal. All cases of meningitis should be screened for cryptococcal antigen.
*DM Resident, ** Associate Professor, *** Professor, **** Assistant Professor,Department of Neurology, Gauhati Medical College, GuwahatiCorrespondence Address : Dr Ashok Kumar Kayal, Professor,Department of Neurology, Gauhati Medical College, Guwahati, Assam-781032, Email:[email protected]
Key Words: Cryptococcal Meningitis,Immunocompromised / Immunocompetant patients.
INTRODUCTION :Cryptococcosis is a fungal infection caused by
encapsulated yeast of the genus Cryptococcus.Cryptococcus has a worldwide distribution. Most casesare caused by Cryptococcus neoformans1. Theincubation period is unknown and transmission is believedto result from inhalation of aerosolized organisms. Themanagement of cryptococcal meningoencephalitis isdiscussed in 3 risk groups: (1) Human ImmunodeficiencyVirus (HIV)–infected individuals, (2) organ transplantrecipients, and (3) non–HIV infected and non transplanthosts2.
AIM OF THE STUDY :The aim was to study the clinical profile of
cryptococcal meningitis.
MATERIAL AND METHOD :� Inclusion cliteriaAll patients irrespective of age and sex presenting withfeatures suggestive of meningitis with laboratory evidenceof Cryptococcus antigen� Exclusion cliteriaPatients with tumors, Trauma, previously diagnosedcryptococcal meningitis, bacterial meningitis and viralmeningitis.� It is prospective observational study at GauhatiMedical College, Guwahati, a tertiary care hospital in thenorth east region� It is conducted from September 2014 –September2016� Detailed neurological evaluation along with routineblood, liver function test, renal function test, electrolytes,VDRL, HIV and chest x-ray done in every patient.� CSF study including total count includingdifferentiating count, sugar, protein, stains for acid fastbacilli, gram’s stain, fungal stain, Adenosine Deaminase,cryptococcal antigen done in every patients.� Neuro-imaging was performed in every patient
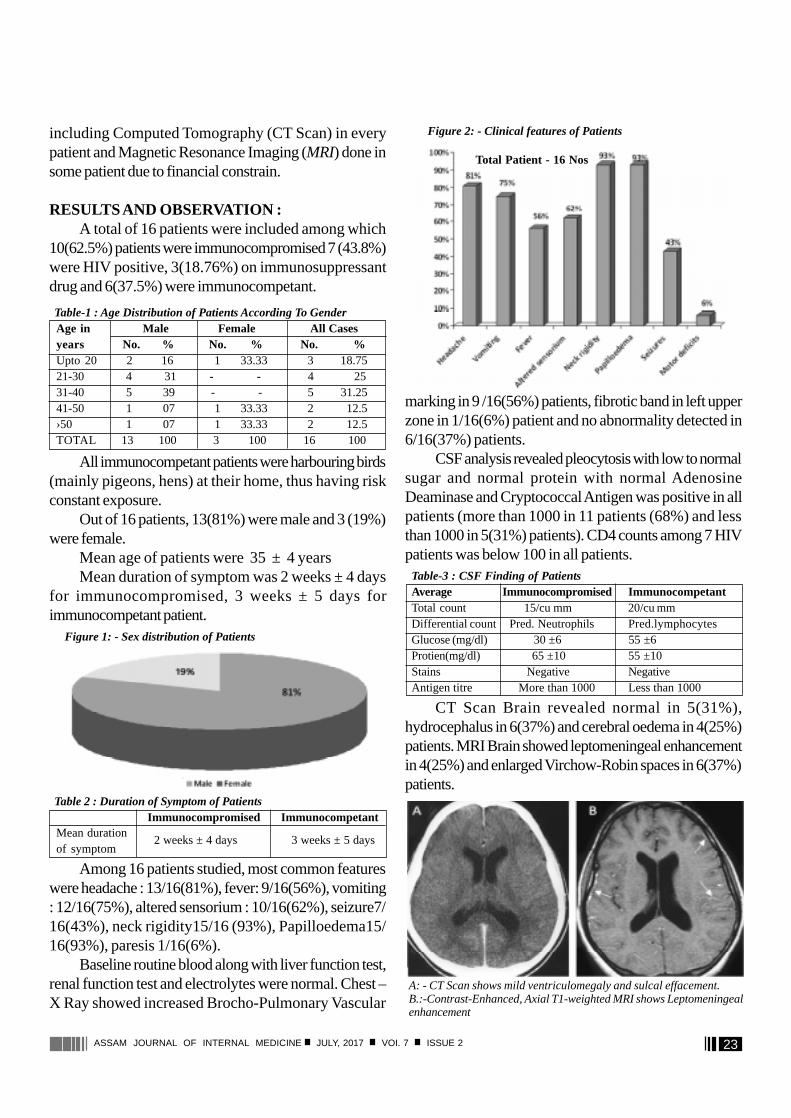
23ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
including Computed Tomography (CT Scan) in everypatient and Magnetic Resonance Imaging (MRI) done insome patient due to financial constrain.
RESULTS AND OBSERVATION :� A total of 16 patients were included among which10(62.5%) patients were immunocompromised 7 (43.8%)were HIV positive, 3(18.76%) on immunosuppressantdrug and 6(37.5%) were immunocompetant.
� All immunocompetant patients were harbouring birds(mainly pigeons, hens) at their home, thus having riskconstant exposure.� Out of 16 patients, 13(81%) were male and 3 (19%)were female.� Mean age of patients were 35 ± 4 years� Mean duration of symptom was 2 weeks ± 4 daysfor immunocompromised, 3 weeks ± 5 days forimmunocompetant patient.
� Among 16 patients studied, most common featureswere headache : 13/16(81%), fever: 9/16(56%), vomiting: 12/16(75%), altered sensorium : 10/16(62%), seizure7/16(43%), neck rigidity15/16 (93%), Papilloedema15/16(93%), paresis 1/16(6%).� Baseline routine blood along with liver function test,renal function test and electrolytes were normal. Chest –X Ray showed increased Brocho-Pulmonary Vascular
marking in 9 /16(56%) patients, fibrotic band in left upperzone in 1/16(6%) patient and no abnormality detected in6/16(37%) patients.� CSF analysis revealed pleocytosis with low to normalsugar and normal protein with normal AdenosineDeaminase and Cryptococcal Antigen was positive in allpatients (more than 1000 in 11 patients (68%) and lessthan 1000 in 5(31%) patients). CD4 counts among 7 HIVpatients was below 100 in all patients.
� CT Scan Brain revealed normal in 5(31%),hydrocephalus in 6(37%) and cerebral oedema in 4(25%)patients. MRI Brain showed leptomeningeal enhancementin 4(25%) and enlarged Virchow-Robin spaces in 6(37%)patients.
Table-1 : Age Distribution of Patients According To GenderAge in Male Female All Casesyears No. % No. % No. %Upto 20 2 16 1 33.33 3 18.7521-30 4 31 - - 4 2531-40 5 39 - - 5 31.2541-50 1 07 1 33.33 2 12.5›50 1 07 1 33.33 2 12.5TOTAL 13 100 3 100 16 100
Figure 1: - Sex distribution of Patients
Table 2 : Duration of Symptom of Patients Immunocompromised Immunocompetant
2 weeks ± 4 days 3 weeks ± 5 daysMean durationof symptom
Figure 2: - Clinical features of Patients
Total Patient - 16 Nos
Table-3 : CSF Finding of PatientsAverage Immunocompromised ImmunocompetantTotal count 15/cu mm 20/cu mmDifferential count Pred. Neutrophils Pred.lymphocytesGlucose (mg/dl) 30 ±6 55 ±6Protien(mg/dl) 65 ±10 55 ±10Stains Negative NegativeAntigen titre More than 1000 Less than 1000
A: - CT Scan shows mild ventriculomegaly and sulcal effacement.B.:-Contrast-Enhanced, Axial T1-weighted MRI shows Leptomeningealenhancement
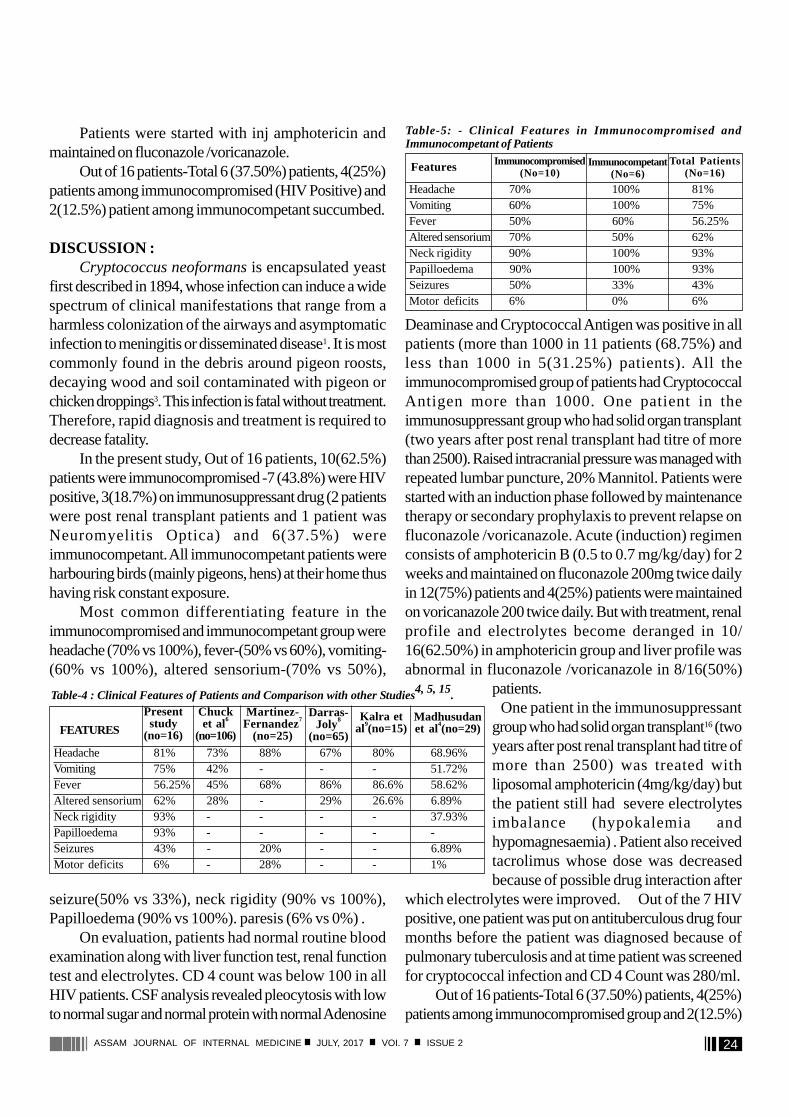
24ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
� Patients were started with inj amphotericin andmaintained on fluconazole /voricanazole.� Out of 16 patients-Total 6 (37.50%) patients, 4(25%)patients among immunocompromised (HIV Positive) and2(12.5%) patient among immunocompetant succumbed.
DISCUSSION :Cryptococcus neoformans is encapsulated yeast
first described in 1894, whose infection can induce a widespectrum of clinical manifestations that range from aharmless colonization of the airways and asymptomaticinfection to meningitis or disseminated disease1. It is mostcommonly found in the debris around pigeon roosts,decaying wood and soil contaminated with pigeon orchicken droppings3. This infection is fatal without treatment.Therefore, rapid diagnosis and treatment is required todecrease fatality.
In the present study, Out of 16 patients, 10(62.5%)patients were immunocompromised -7 (43.8%) were HIVpositive, 3(18.7%) on immunosuppressant drug (2 patientswere post renal transplant patients and 1 patient wasNeuromyelitis Optica) and 6(37.5%) wereimmunocompetant. All immunocompetant patients wereharbouring birds (mainly pigeons, hens) at their home thushaving risk constant exposure.
Most common differentiating feature in theimmunocompromised and immunocompetant group wereheadache (70% vs 100%), fever-(50% vs 60%), vomiting-(60% vs 100%), altered sensorium-(70% vs 50%),
seizure(50% vs 33%), neck rigidity (90% vs 100%),Papilloedema (90% vs 100%). paresis (6% vs 0%) .
On evaluation, patients had normal routine bloodexamination along with liver function test, renal functiontest and electrolytes. CD 4 count was below 100 in allHIV patients. CSF analysis revealed pleocytosis with lowto normal sugar and normal protein with normal Adenosine
Deaminase and Cryptococcal Antigen was positive in allpatients (more than 1000 in 11 patients (68.75%) andless than 1000 in 5(31.25%) patients). All theimmunocompromised group of patients had CryptococcalAntigen more than 1000. One patient in theimmunosuppressant group who had solid organ transplant(two years after post renal transplant had titre of morethan 2500). Raised intracranial pressure was managed withrepeated lumbar puncture, 20% Mannitol. Patients werestarted with an induction phase followed by maintenancetherapy or secondary prophylaxis to prevent relapse onfluconazole /voricanazole. Acute (induction) regimenconsists of amphotericin B (0.5 to 0.7 mg/kg/day) for 2weeks and maintained on fluconazole 200mg twice dailyin 12(75%) patients and 4(25%) patients were maintainedon voricanazole 200 twice daily. But with treatment, renalprofile and electrolytes become deranged in 10/16(62.50%) in amphotericin group and liver profile wasabnormal in fluconazole /voricanazole in 8/16(50%)
patients.One patient in the immunosuppressant
group who had solid organ transplant16 (twoyears after post renal transplant had titre ofmore than 2500) was treated withliposomal amphotericin (4mg/kg/day) butthe patient still had severe electrolytesimbalance (hypokalemia andhypomagnesaemia) . Patient also receivedtacrolimus whose dose was decreasedbecause of possible drug interaction after
which electrolytes were improved. Out of the 7 HIVpositive, one patient was put on antituberculous drug fourmonths before the patient was diagnosed because ofpulmonary tuberculosis and at time patient was screenedfor cryptococcal infection and CD 4 Count was 280/ml.
Out of 16 patients-Total 6 (37.50%) patients, 4(25%)patients among immunocompromised group and 2(12.5%)
Headache 81% 73% 88% 67% 80% 68.96%Vomiting 75% 42% - - - 51.72%Fever 56.25% 45% 68% 86% 86.6% 58.62%Altered sensorium 62% 28% - 29% 26.6% 6.89%Neck rigidity 93% - - - - 37.93%Papilloedema 93% - - - - -Seizures 43% - 20% - - 6.89%Motor deficits 6% - 28% - - 1%
Table-4 : Clinical Features of Patients and Comparison with other Studies4, 5, 15.
Madhusudanet al4(no=29)FEATURES
Presentstudy
(no=16)
Chucket al6
(no=106)
Martinez-Fernandez7
(no=25)
Darras-Joly8
(no=65)
Kalra etal9(no=15)
Table-5: - Clinical Features in Immunocompromised andImmunocompetant of Patients
Headache 70% 100% 81%Vomiting 60% 100% 75%Fever 50% 60% 56.25%Altered sensorium 70% 50% 62%Neck rigidity 90% 100% 93%Papilloedema 90% 100% 93%Seizures 50% 33% 43%Motor deficits 6% 0% 6%
Total Patients(No=16)Features Immunocompromised
(No=10)Immunocompetant
(No=6)

25ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
patient among immunocompetant succumbed. Cause ofDeath in 4 (25%) was aspiration pneumonia, sepsis (3 inimmunosuppressant and 1 in immunocompetant group),2/16(12.5%) had intractable seizure (1 each inimmunosuppressant and immunocompetant group).
In the study by Satishchandra et al10, 11, the incidenceof cryptococcal meningitis (31.9%) was at par withtuberculous meningitis (32.2%) in HIV patients. Mortalityfrom HIV associated cryptococcal meningitis remains highin many countries due to multiple factors. Some of theminclude the insufficiency of antifungal drugs, and thecomplications such as raised intracranial pressure. The poorprognostic factors are depressed level of consciousness,signs of raised intracranial pressure, depressed CSF cellcounts and glucose levels and CSF cryptococcal antigentitre > 1024.
In the present study, mortality was 37.5%. In thestudy done by Khanna et al12, mortality was 32.18%. Inthe present study, the poor prognostic factors13, 14 includedaltered sensorium, and CD4 count of less than 50/ml. Thisis in concordance with various other studies which haveshown that altered sensorium is associated with poorprognosis Response to therapy with amphotericin B andfluconazole was good and recovery was seen in 62.5%of the patients
REFERENCES :1. Cryptococcal Meningitis: Claudia Fabrizio, Sergio Carbonara and
Gioacchino Angarano Clinic of Infectious Diseases, UniversityOf Bari, Italy.
2. Clinical Practice Guidelines for the Management of CryptococcalDisease: 2010 Update by the Infectious Diseases Society of
America.3. Cryptococcosis: Louisiana Office of Public Health – Infectious
Disease Epidemiology Section; Revised 08/21/20044. Madhusudan NS “Demographic, Laboratory and Immunological
Profile of HIV Seropositive Cryptococcal Meningitis”. Journal ofEvolution of Medical and Dental Sciences 2014 March 17: 3(11):2720-2726
5. Aslam SMS et al: Study of Cryptococcal Meningitis in HIVSeropositive Patients in a Tertiary Care Centre; JIACM 2009;10(3): 110-5
6. Chuck SL, Sande MA. Infections with Cryptococcus neoformansin the acquired immunodeficiency syndrome. N Engl J Med 1989;321 (12): 794-9.
7. Martinez-Fernandez EM, Lopez-Cortes LF, Regordan C,Cordero-Matia E. Meningitis by Cryptococcus neoformans in patientswith HIV infection. Neurologia 1999; 14 (5): 218-23.
8. Darras-Joly C, Chevret S, Wolff M et al. Cryptococcus neoformansinfection in France: epidemiologic features of and early prognosticparameters for 76 patients who were infected with humanimmunodeficiency virus. Clin Infect Dis 1996; 23 (2): 369-76.
9. Kalra SP, Chadha DS, Singh AP et al. Cryptococcal meningitis inacquired immunodeficiency syndrome. J Assoc Physicians India1999; 47 (10): 958-61.
10. Satishchandra P et al.Seizures in HIV-seropositive individuals:NIMHANS experience and review. Epilepsia. 2008: 49(6):33–41.
11. Satishchandra P, et al .Neurological manifestations associated withHIV infection: Indian Perspective. Medicine Update 2010: 20.
12. Khanna N, Chandramukhi A, Desai A et al. Cryptococcosis in theimmunocompromised Host with special reference to AIDS. IndianJ Chest Dis Allied Sci 2000; 42 (4): 311-5.
13. Deepak Nayak M et al: Cryptococcal Meningitis: Looking beyondHIV; International Journal of Scientific and Research Publications:2013 March:3(3).
14. Kumar S et al: Cryptococcal meningitis in HIV infected: Experiencefrom a North Indian tertiary center; Neurology India: 2008October-December:56(4).
15. Imwidthaya P, Pougvarin N. Cryptococcosis in AIDS. PostgradMed J 2000; 76: 85-8.
16. Chang HH et al.Voriconazole inhibition of tacrolimus metabolismin a kidney transplant recipient with fluconazole-resistantcryptococcal meningitis. International Journal of InfectiousDiseases : 2010: 14: e348–e350.
26ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Complication Profile of Diabetes Mellitusin a Tertiary care Hospital in Upper Assam
P Dihingia*, S M Baruah** , T K Das** , C Dutta*** , T Karthikeyan ****
O r i g i n a l A r t i c l e
AbstractBackground : Chronic complications are the major outcome of type 2 diabetes mellitus, which reduce the quality of life
of patients, incur heavy burdens to the health care system, and increase diabetic mortality. The aims of this study were todescribe the prevalence of chronic complications among both urban and rural population admitted in the ASSAM MEDICALCOLLEGE, a tertiary care hospital in upper Assam. Material & Methods : This cross-sectional hospital-based study wascarried out in the patients admitted in a medical unit of a Tertiary care centre. The survey was conducted for a period of oneyear from March 2016 to Feb 2017 among the diabetes patients. The subjects were assessed clinically and informations wereobtained from the routine Diabetic profile. Results : In our study, among the complications of Diabetes Mellitus, the mostprevalent complication is Nephropathy (55.6%) followed by neuropathy (34.7%), retinopathy (19.1%), CerebrovascularAccident (7.1%), Hyperglycaemic Hyperosmolar State (5.98%), Coronary Artery Disease (5.3) and diabetic Ketoacidosic(3.5%). Compared to other Indian studies nephropathy was found to the most common complication in our study. Conclusions: Chronic complications are highly prevalent among type 2 diabetic patients; in our part of the country. Nephropathy isfound to be more prevalent. The glycaemic control of diabetic patients with chronic complications are poor, and future effortsshould be directed at intensive blood glucose control, strengthening early diagnosis and improving case management toprevent and minimize the occurrence of complications. The high prevalence of Nephropathy alike rest of the world should beconsidered as a curtain raiser for a larger study in this regard.
* Associate Professor, ** Assistant Professor, *** Register, **** SenoirResedent. Correspondence Address : Dr. Prasanta Dihingia, AssociateProfessor, Department of Medicine, Assam Medical College, Dibrugarh.PIN-786002. Email: [email protected]
Keywords: Glycemic Control, Neuropathy,Nephropathy, Retinopathy.
INTRODUCTION :Diabetes mellitus (DM) is a major public health
problem depicting a rising prevalence worldwide6.India isone of the epicentres of the global diabetes mellituspandemic. Rapid socioeconomic development anddemographic changes, along with increased susceptibilityfor Indian individuals, have led to the explosive increase inthe prevalence of diabetes mellitus in India over the pastfour decades.
DM is the leading cause of end-stage renal disease(ESRD), nontraumatic lower extremity amputations, andadult blindness. It also predisposes to cardiovasculardiseases. With an increasing incidence worldwide, DMwill be likely a leading cause of morbidity and mortality inthe future.1
In prediction, India along with China will account fornearly a third of the estimated 300 million adult diabeticsby the year 2025.5
AIMS AND OBJECTIVES :· To find the profile of complications of Diabetesmellitus· To correlate HbA1c with disease duration.
REVIEW OF LITERATURE :Diabetes-related complications affect many organ
systems and are responsible for the majority of morbidityand mortality associated with the disease. Diabetes-relatedcomplications can be divided into vascular and nonvascularcomplications and are similar for type 1 and type 2 DM.The complications, affecting the eyes, kidneys, andperipheral nervous system, were collectively calledmicrovascular complications, to distinguish them from theless diabetes-specific but highly prevalent macrovasculardisease complications. Microvascular disease andperipheral neuropathy resulted in blindness, kidney failure,and amputations.12
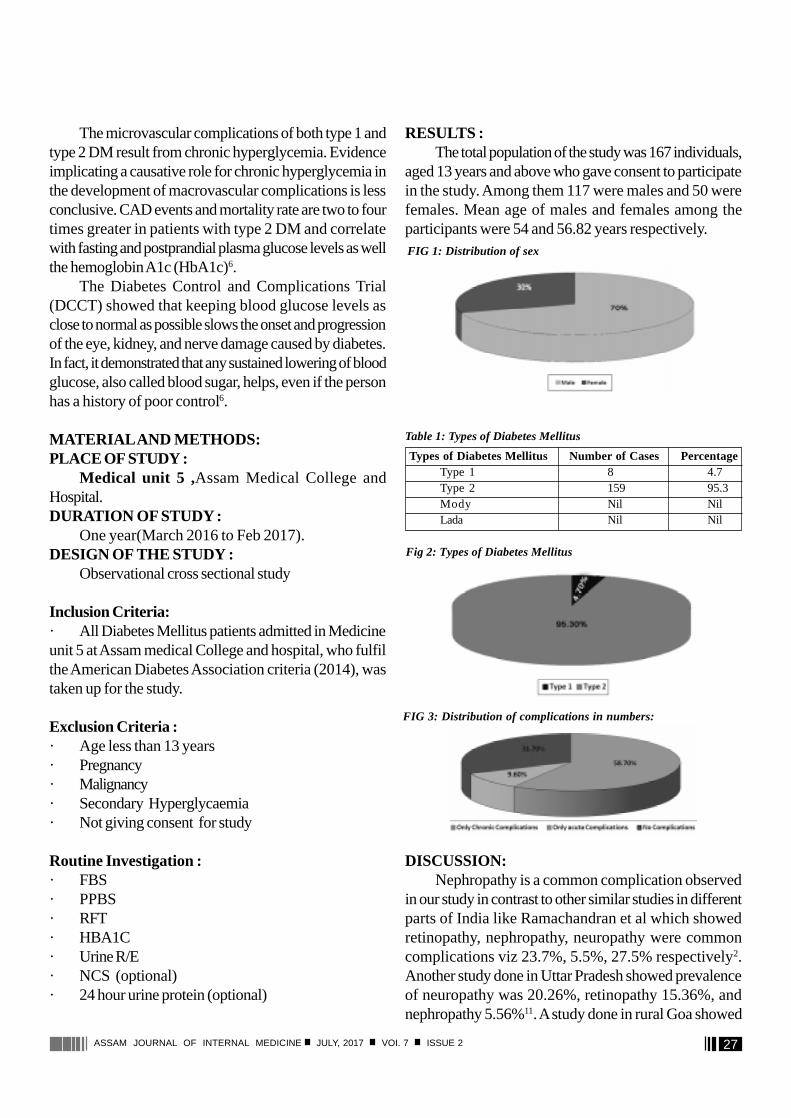
27ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
The microvascular complications of both type 1 andtype 2 DM result from chronic hyperglycemia. Evidenceimplicating a causative role for chronic hyperglycemia inthe development of macrovascular complications is lessconclusive. CAD events and mortality rate are two to fourtimes greater in patients with type 2 DM and correlatewith fasting and postprandial plasma glucose levels as wellthe hemoglobin A1c (HbA1c)6.
The Diabetes Control and Complications Trial(DCCT) showed that keeping blood glucose levels asclose to normal as possible slows the onset and progressionof the eye, kidney, and nerve damage caused by diabetes.In fact, it demonstrated that any sustained lowering of bloodglucose, also called blood sugar, helps, even if the personhas a history of poor control6.
MATERIAL AND METHODS:PLACE OF STUDY :
Medical unit 5 ,Assam Medical College andHospital.DURATION OF STUDY :
One year(March 2016 to Feb 2017).DESIGN OF THE STUDY :
Observational cross sectional study
Inclusion Criteria:· All Diabetes Mellitus patients admitted in Medicineunit 5 at Assam medical College and hospital, who fulfilthe American Diabetes Association criteria (2014), wastaken up for the study.
Exclusion Criteria :· Age less than 13 years· Pregnancy· Malignancy· Secondary Hyperglycaemia· Not giving consent for study
Routine Investigation :· FBS· PPBS· RFT· HBA1C· Urine R/E· NCS (optional)· 24 hour urine protein (optional)
RESULTS :The total population of the study was 167 individuals,
aged 13 years and above who gave consent to participatein the study. Among them 117 were males and 50 werefemales. Mean age of males and females among theparticipants were 54 and 56.82 years respectively.
DISCUSSION:Nephropathy is a common complication observed
in our study in contrast to other similar studies in differentparts of India like Ramachandran et al which showedretinopathy, nephropathy, neuropathy were commoncomplications viz 23.7%, 5.5%, 27.5% respectively2.Another study done in Uttar Pradesh showed prevalenceof neuropathy was 20.26%, retinopathy 15.36%, andnephropathy 5.56%11. A study done in rural Goa showed
FIG 1: Distribution of sex
Types of Diabetes Mellitus Number of Cases PercentageType 1 8 4.7Type 2 159 95.3Mody Nil NilLada Nil Nil
Table 1: Types of Diabetes Mellitus
Fig 2: Types of Diabetes Mellitus
FIG 3: Distribution of complications in numbers:
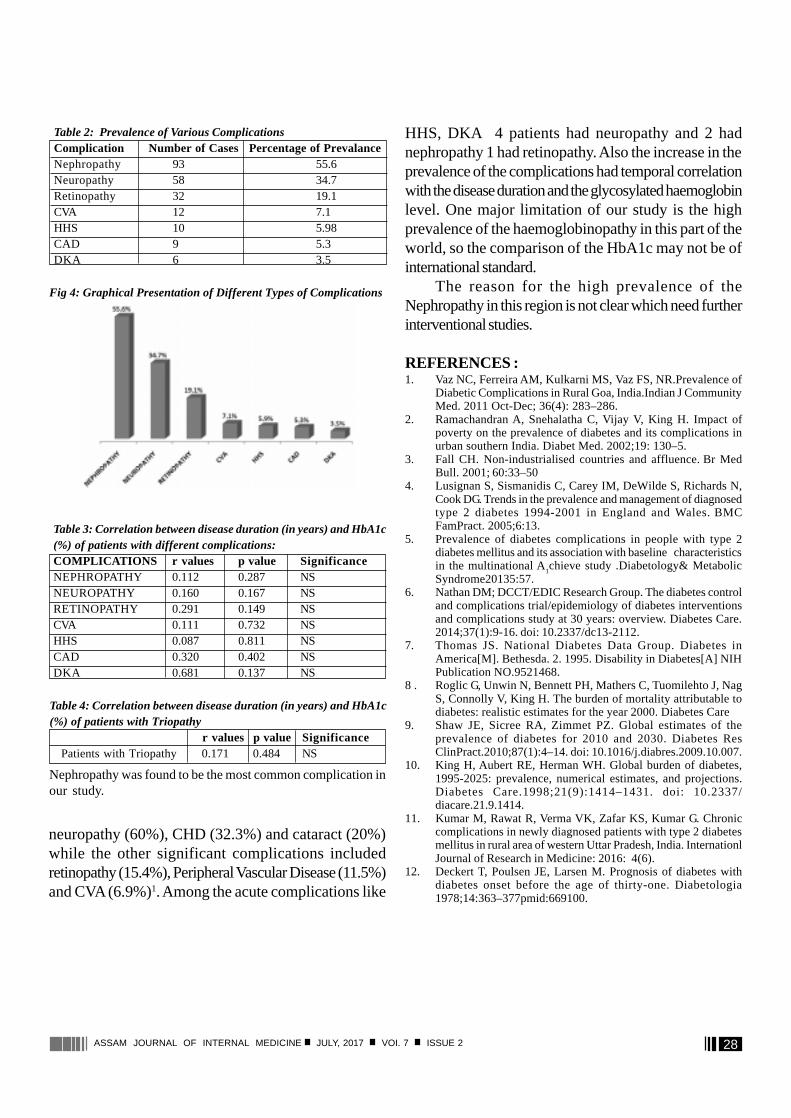
28ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
HHS, DKA 4 patients had neuropathy and 2 hadnephropathy 1 had retinopathy. Also the increase in theprevalence of the complications had temporal correlationwith the disease duration and the glycosylated haemoglobinlevel. One major limitation of our study is the highprevalence of the haemoglobinopathy in this part of theworld, so the comparison of the HbA1c may not be ofinternational standard.
The reason for the high prevalence of theNephropathy in this region is not clear which need furtherinterventional studies.
REFERENCES :1. Vaz NC, Ferreira AM, Kulkarni MS, Vaz FS, NR.Prevalence of
Diabetic Complications in Rural Goa, India.Indian J CommunityMed. 2011 Oct-Dec; 36(4): 283–286.
2. Ramachandran A, Snehalatha C, Vijay V, King H. Impact ofpoverty on the prevalence of diabetes and its complications inurban southern India. Diabet Med. 2002;19: 130–5.
3. Fall CH. Non-industrialised countries and affluence. Br MedBull. 2001; 60:33–50
4. Lusignan S, Sismanidis C, Carey IM, DeWilde S, Richards N,Cook DG. Trends in the prevalence and management of diagnosedtype 2 diabetes 1994-2001 in England and Wales. BMCFamPract. 2005;6:13.
5. Prevalence of diabetes complications in people with type 2diabetes mellitus and its association with baseline characteristicsin the multinational A
1chieve study .Diabetology& Metabolic
Syndrome20135:57.6. Nathan DM; DCCT/EDIC Research Group. The diabetes control
and complications trial/epidemiology of diabetes interventionsand complications study at 30 years: overview. Diabetes Care.2014;37(1):9-16. doi: 10.2337/dc13-2112.
7. Thomas JS. National Diabetes Data Group. Diabetes inAmerica[M]. Bethesda. 2. 1995. Disability in Diabetes[A] NIHPublication NO.9521468.
8 . Roglic G, Unwin N, Bennett PH, Mathers C, Tuomilehto J, NagS, Connolly V, King H. The burden of mortality attributable todiabetes: realistic estimates for the year 2000. Diabetes Care
9. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of theprevalence of diabetes for 2010 and 2030. Diabetes ResClinPract.2010;87(1):4–14. doi: 10.1016/j.diabres.2009.10.007.
10. King H, Aubert RE, Herman WH. Global burden of diabetes,1995-2025: prevalence, numerical estimates, and projections.Diabetes Care.1998;21(9):1414–1431. doi: 10.2337/diacare.21.9.1414.
11. Kumar M, Rawat R, Verma VK, Zafar KS, Kumar G. Chroniccomplications in newly diagnosed patients with type 2 diabetesmellitus in rural area of western Uttar Pradesh, India. InternationlJournal of Research in Medicine: 2016: 4(6).
12. Deckert T, Poulsen JE, Larsen M. Prognosis of diabetes withdiabetes onset before the age of thirty-one. Diabetologia1978;14:363–377pmid:669100.
Table 2: Prevalence of Various ComplicationsComplication Number of Cases Percentage of PrevalanceNephropathy 93 55.6Neuropathy 58 34.7Retinopathy 32 19.1CVA 12 7.1HHS 10 5.98CAD 9 5.3DKA 6 3.5
Fig 4: Graphical Presentation of Different Types of Complications
Table 3: Correlation between disease duration (in years) and HbA1c(%) of patients with different complications:COMPLICATIONS r values p value SignificanceNEPHROPATHY 0.112 0.287 NSNEUROPATHY 0.160 0.167 NSRETINOPATHY 0.291 0.149 NSCVA 0.111 0.732 NSHHS 0.087 0.811 NSCAD 0.320 0.402 NSDKA 0.681 0.137 NS
Table 4: Correlation between disease duration (in years) and HbA1c(%) of patients with Triopathy
r values p value Significance Patients with Triopathy 0.171 0.484 NS
Nephropathy was found to be the most common complication inour study.
neuropathy (60%), CHD (32.3%) and cataract (20%)while the other significant complications includedretinopathy (15.4%), Peripheral Vascular Disease (11.5%)and CVA (6.9%)1. Among the acute complications like
29ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Physical Factors of Carcinogenesis
P S Roy*, A Inamdar** , T Nyodu*** , M Hazarika****
R e v i e w A r t i c l e
*Assistant Professor, ** DCH Fellow, *** Senior Resident, **** AssistantProfessor, Dept of Medical Oncology, Dr B Borooah Cancer Institute,Guwahati. Correspondence Address : Dr Partha S Roy, Dept of MedicalOncology, Dr B Borooah Cancer Institute, Gopinath Nagar, A. K. AzadRoad, Guwahati, Assam, PIN-781016. [email protected]
Key words: Environmental factors, physical factors,carcinogenesis.
INTRODUCTION :The first observation in the natural history of
carcinogenesis concerning the intervention of a substancein the appearance of a tumor belongs to Sir Percival Pott,from 1775, who understands that there is a relationbetween soot and the appearance of scrotal cancer inchimney-sweeps. In 1977, four researchers, Muir,Higginso, Doll and Peto explained the evidences fromepidemiological studies that 80% of all cancers werecaused by environmental factors.
Current understanding of biological mechanisms ofcarcinogenesis suggests that all cancers are originatedfrom both environment and genetics, implying that thereare multiple external factors combined with internalgenetic changes are responsible for cancer. Preventionof the disruption of cellular signalling and protectivepathways can be accomplished by preventingcarcinogenic exposures from outside the body from anysource. Prevention of carcinogenic exposures is still amajor priority. Also, individuals with particular geneticpredispositions may be more susceptible to the effectsof environmental exposures than others.
Among the key environmental factors are chemicalcarcinogens, physical carcinogens, infectious agents and life-style. Physical carcinogens are highly variable in theirchemical structure, and many of them are poorly understood.Some physical carcinogens are naturally occurring, whileothers are synthetic. Physical carcinogens include fibers,particulate matter, hard and soft synthetic materials and gels.
No specific pathway has been isolated that correctlyidentifies the way physical agents cause cancer. Most likely,cancer can be caused by a variety of different pathways.Primary targets for physical factors include cellularregulatory proteins which are essential for control of cellgrowth, DNA repair and programmed cell death. Amongmolecular targets on carcinogenesis are somatic mutation(genetic changes) and aberrant DNA methylation(epigenetic changes) at the genomic level and the post-translational modifications at protein level. To complicatematters, some physical carcinogens act in concert withgenetic factors and other environmental agents to producecancer. For instance, asbestos can cause cancer on itsown; however, it has much stronger carcinogenic potentialwhen combined with exposure to cigarette smoke.
Following are considered as physical factors ofcarcinogenesis: Ionizing radiation, Non-ionizing radiations(e.g., Ultraviolet light, Radiofrequency and microwaveradiation, Electromagnetic fields), Asbestos andNanoparticles.
Ionizing Radiation (IR):Ionizing Radiation is defined as radiation that has
sufficient energy to ionize molecules by displacing electronsfrom atoms. IR can be electromagnetic, such as X-raysand gamma rays, or can consist of particles, such aselectrons, protons, neutrons, alpha particles, or carbonions. Natural sources of IR make up about 80% of humanexposure and medical sources make up about 20%. Ofthe natural sources, exposure to radon is the mostsignificant exposure risk to humans. It is clear from epidemiologic studies of radiationworkers, survivors of atomic bomb and Chernobyl victimsthat IR can induce cancer6. The incidences of solidtumours, such as breast, ovary, bladder, lung, and coloncancers, were estimated to have increased by a factor of

30ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
2 in the exposed group during this time period. Theepidemiology studies following the nuclear power plantdisaster in Chernobyl showed a clear increase in thyroidcancer as early as 4 years after the accident. Young childrenwere most vulnerable to radiation exposure. The largestsource of radiation exposure to the population is radon,which is a natural radioactive gas. Another important sourceof human exposure to IR is medical X-ray devices, andthere is a growing concern about the dramatically increaseduse of whole body CT scans for diagnostic purposes. Fora typical CT scan, a patient will receive about 100-foldmore radiation than from a typical mammogram7. Cancerpatients who receive radiation therapy are at risk ofdeveloping secondary tumours induced by the radiationtherapy treatment. The most sensitive tissues for thedevelopment of secondary cancer have been found to bebone marrow (leukaemia), the thyroid, breast, and lung.
Electromagnetic radiation, such as X-rays or gammarays, are sparsely ionizing and therefore classified as lowlinear energy transfer (LET) radiation, whereas particulateradiation, such as neutrons, protons, and alpha particles,are examples of high LET radiation1. The biologic effectsof IR are due to the local deposition of energy in radiationtracks. The distance between the depositions of energy isbiologically very relevant and unique to the energy andthe type of radiation.
The direct and indirect effects of radiation induce moreor less identical types of lesions in DNA. Radiation-induced lesions consist of more than 100 chemically distinctbase lesions, such as the mutagenic lesions thymine glycoland 8-hydroxyguanine2,3,4. Furthermore, damage to thesugar moiety in the backbone of DNA and some types ofbase damage can result in single-strand breaks (SSB) ordouble-strand break (DSB). It has been estimated that1Gy of ionizing radiation gives rise to about 40 DSBs,1,000 SSBs, 1,000 base lesions, and 150 DNA-proteincross-links per cell2. DSBs are the critical lesions that leadto cell lethality following exposure to ionizing radiation.
Terminally differentiated and stationary cells, such askidney, lung, brain, muscle, and liver cells, are generallymore resistant to radiation- induced killing than are cellswith a high turnover rate, such as different epithelial cells,spermatogonia, and hair follicles. IR can induce cell deathin tissues by many different mechanisms. Cell death inducedby IR may in some cases be associated with autophagy,
also called autophagocytosis, in which cells degrade cellularcomponents via the lysosomal machinery. Finally, tissuecan undergo necrotic cell death following exposure to IR.
Medical exposure to ionizing radiation :The medical applications of ionizing radiation have
greatly expanded worldwide due to an increasing use ofX-rays in diagnostic imaging and interventional radiology,the development of new technologies usingradiopharmaceuticals for diagnosis and treatment in nuclearmedicine, and the multiple applications of X-rays, gamma-rays and charged particles in radiotherapy. Radiationinduced cancer risk increases with doses, with higher riskfor children and young people, as they are significantlymore sensitive to radiation exposure than adults.Epidemiological studies in humans demonstrate that ionizingradiation can give rise to cancer in multiple anatomicalsites: leukaemia (short latency) and tumours in solid organs(long latency: bone, lung, liver, thyroid, breast, etc).
Ultraviolet light :Depending on the wavelength, UV light is categorized
into UVA (320 to 400 nm), UVB (290 to 320 nm), andUVC (240 to 290 nm) radiation. Most of the UVC lightemitted from the sun is absorbed by the ozone layer in theatmosphere, and, thus, living organisms are mostly exposedto UVA and UVB irradiation.
UVC light is more damaging to DNA than UVA andUVB because the absorption maximum of DNA is around260 nm. The formation of these lesions results in thebending of the DNA helix, resulting in the interference withboth DNA and RNA synthesis which in turn can formSSBs and base lesions in DNA of exposed cells.
The incidence of skin cancer, especially melanoma, ison the increase due to higher rates of sun exposure in thegeneral population. Risk of contracting melanoma appearsto be linked to high sunlight exposure during childhood. UVlight can initiate carcinogenesis by inducing DNA lesions aswell as suppressing the immune system, resulting in a greaterprobability that initiated cells survivability and growth intotumours8,9. Basal cell carcinoma (BCC) and squamous cellcarcinoma (SCC) are the two most common skin cancertypes. BCC and SCC occur predominantly in sun-exposedareas of the skin. The tumour suppressor genes p53 andp16 are frequently inactivated in BCC and SCC.

31ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Radiofrequency and Micro wave radiation :Radiofrequency radiation (RFR) is electromagnetic
radiation in the frequency range between 3 kHz to 300MHz; whereas microwave radiation (MR) is in thefrequency range between 300 MHz to 300 GHz. RFRand MR do not have sufficient energies to cause ionizationsin target tissues. Rather, the radiation energy is convertedinto heat as the radiation energy is absorbed. Sources ofradiofrequency and microwave radiation include mobilephones, radio transmitters of wireless communication,radars, medical devices, and kitchen appliances.
Because human exposure to RFR has increaseddramatically in recent years, it is important to knowwhether this type of radiation gives rise to genotoxicdamage. One confounding factor when assessing thegenotoxic effect of RFR, and MR, is the heating effectthat affects the tissue when the radiation energy isabsorbed. A recent study controlling for the potentialheating effect of exposure found that RFR induces DNAdamage in human spermatozoa in-vitro, which is analarming finding. It has been suggested that MR may affectthe folding of proteins in cells that promote new proteinsynthesis.
A number of studies have focused on the potentialcancer risks from mobile phone usage, and some of thesestudies indicate that long-term mobile phone usage maybe associated with increased risks of developing braintumours. Some studies have shown a connection betweenproximity to mobile phone base stations and increasedcancer incidence, whereas another study found noassociation between exposure to RFR from mobile phonebase stations and early childhood cancers.
Electromagnetic fields:An electromagnetic field (EMF) is a physical field
produced by electrically charged objects that can affectother charged objects in the field. Typical sources of EMFsare electric power lines, electrical devices, and magneticresonance imaging (MRI) machines.
A low frequency EMF does not transmit energy highenough to break chemical bonds therefore; it is not thoughtto directly damage DNA or proteins in cells. EMFs havebeen shown to induce nongenotoxic effects in cells, suchas interference with cellular signalling pathways whichcould contribute to neurodegeneration10.
There is no strong link between EMF exposure andincreased risks of contracting adult leukaemia, braintumours, or breast cancer. Furthermore, a studyinvestigating whether EMF exposure was associated withheritable effects found no correlation between parentalexposure and childhood cancer.
Asbestos :Asbestos is the generic name for a group of naturally
occurring inorganic fibrous silicates that have been widelyused in building materials for its heat, sound, and electricalinsulating qualities. Asbestos becomes a serious healthhazard if the fibres are inhaled over a long period of time,and these health effects are increased dramatically if theexposed individual is a smoker. It was first reported in1935 that asbestos might be an occupational health hazardthat could induce cancer. The use of asbestos productspeaked in the 1970s, yet remains a major health hazard inmany places around the world today. Asbestos exposureaccount for the largest proportion of occupational cancers.
Asbestos fibres can enter cells and induce reactiveoxygen species (ROS). ROS have been implicated tooriginate from affected mitochondria leading to inductionof SSBs and base damage. If not successfully repaired,asbestos-induced DNA damage has been shown to resultin chromosome aberrations, micronuclei formation, andincreased rates of sister chromatid exchanges.Lung Cancer:
Epidemiologic studies have found a strong linkbetween asbestos exposure and lung cancer. It has beenestimated that about 5% to 7% of all lung cancers areattributable to asbestos exposure; and asbestos andtobacco smoking act in synergy to induce lung cancer.Mesothelioma:
After being taken up by lung tissues, asbestos fibrescan translocate into the pleura which are covered with aprotective lining, the mesothelium, which consists ofsquamous-like epithelial cells. Mesothelial cells caninternalize asbestos fibres, resulting in the induction of ROSand inflammatory responses, subsequently leading to theinitiation and progression of malignant mesothelioma.Nanoparticles :
Nanoparticles are defined as ultrafine particles of thesize range 1 to 100 nm in diameter. The production ofnanoparticles has increased dramatically in recent years,

32ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
and they are found in many industrial and consumerproducts such as paint, cosmetics, and sunscreens. Theyalso have many potential medical applications, such asdelivery vehicles for specific drugs to specific target tissuesor tumours.
Many of the cellular effects of nanoparticles are similarto the effects exerted by asbestos, such as the generationof ROS and inflammation. Nanoparticles have been shownto induce oxidative DNA damage, such as DNA strandbreaks and 8-hydroxyguanine lesions both in cell culture15
and in vivo. Nanoparticles have also been found to affectthe immune system and can induce the release of the pro-inflammatory cytokine TNF-á from cells. Somenanoparticles, such as titanium dioxide, which is used aspigments in paint, have been classified by the InternationalAgency for Research on Cancer (IARC) as a group 2Bcarcinogen (possible carcinogenic to humans). However,rigorous epidemiologic data is lacking to fully evaluate thecancer-inducing potential of nanoparticles16.
CONCLUSION :Evidence from various studies either confirms or
implicates role of environmental factors in the developmentof a wide range of malignancies by stimulating intracellularsignaling pathways. Although, no specific pathway has beenisolated that correctly identifies the way physical agentscause cancer, intracellular DNA is the target of most ofthe physical agents. Some physical carcinogens act inconcert with genetic and other environmental factors toproduce cancer. Prevention of the disruption of cellular
signaling can be accomplished by preventing carcinogenicexposures. However, prevention of carcinogenicexposures is still a major priority and is considered as amajor public health concern.
Acknowledgments : The authors declare that there isno conflict of interests.
REFERENCES :1. Hall E, Giaccia A. Radiobiology for the Radiologist. Philadelphia:
Lippincott Williams & Wilkins; 2012.2. Ward JF. DNA damage produced by ionizing radiation in
mammalian cells: identities, mechanisms of formation, andrepairability. Prog Nucleic Acid Res Mol Biol 1988;35:95–125.
3. Hutchinson F. Chemical changes induced in DNA by ionizingradiation. Prog Nucleic Acid Res Mol Biol 1985;32:115–154.
4. Friedberg E, Walker G, Siede W, et al. DNA Repair and Mutagenesis.2nd ed. Washington, D.C.: ASM Press; 2006.
5. Gudkov AV, Komarova EA. The role of p53 in determiningsensitivity to radiotherapy. Nat Rev Cancer 2003;3:117–129.
6. Thompson DE, Mabuchi K, Ron E, et al. Cancer incidence inatomic bombsurvivors. Part II: Solid tumors, 1958–1987. RadiatRes 1994;137:S17–67.
7. National Research Council. Health Risks from Exposure to LowLevels of Ionizing Radiation: BEIR VII Phase 2. Washington,D.C.: National Academy Press; 2006.
8. Murphy GM. Ultraviolet radiation and immunosuppression. BrJ Dermatol 2009;161(Suppl 3):90–95.
9. Fisher MS, Kripke ML. Systemic alteration induced in mice byultraviolet light irradiation and its relationship to ultravioletcarcinogenesis. Proc Natl Acad Sci U S A 1977;74:1688–1692.
10. Consales C, Merla C, Marino C, et al. Electromagnetic fields,oxidative stress, and neurodegeneration. Int J Cell Biol2012;2012:683897.
11. Shukla RK, Kumar A, Gurbani D, et al. TiO(2) nanoparticlesinduce oxidative DNA damage and apoptosis in human liver cells.Nanotoxicology 2013;7:48–60.
12. Shi H, Magaye R, Castranova V, et al. Titanium dioxidenanoparticles: a review of current toxicological data. Part FibreToxicol 2013;10:15.
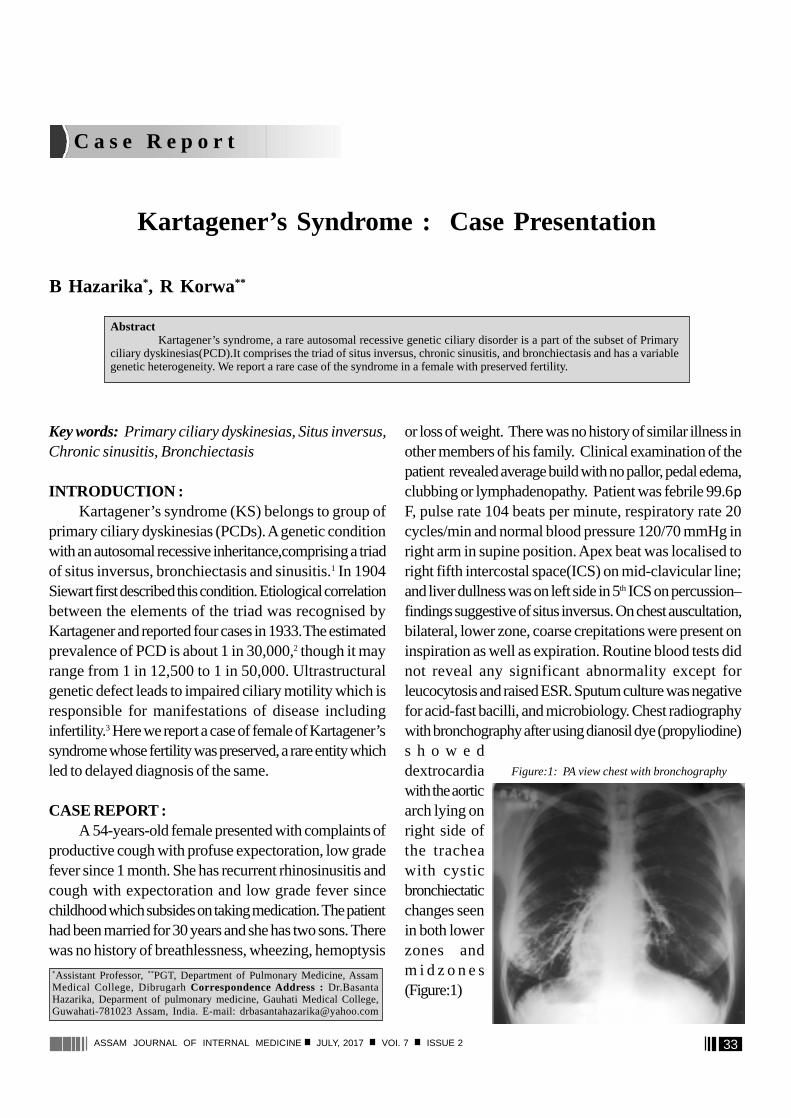
33ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
C a s e R e p o r t
Kartagener’s Syndrome : Case Presentation
B Hazarika*, R Korwa**
AbstractKartagener’s syndrome, a rare autosomal recessive genetic ciliary disorder is a part of the subset of Primary
ciliary dyskinesias(PCD).It comprises the triad of situs inversus, chronic sinusitis, and bronchiectasis and has a variablegenetic heterogeneity. We report a rare case of the syndrome in a female with preserved fertility.
Key words: Primary ciliary dyskinesias, Situs inversus,Chronic sinusitis, Bronchiectasis
INTRODUCTION :Kartagener’s syndrome (KS) belongs to group of
primary ciliary dyskinesias (PCDs). A genetic conditionwith an autosomal recessive inheritance,comprising a triadof situs inversus, bronchiectasis and sinusitis.1 In 1904Siewart first described this condition. Etiological correlationbetween the elements of the triad was recognised byKartagener and reported four cases in 1933. The estimatedprevalence of PCD is about 1 in 30,000,2 though it mayrange from 1 in 12,500 to 1 in 50,000. Ultrastructuralgenetic defect leads to impaired ciliary motility which isresponsible for manifestations of disease includinginfertility.3 Here we report a case of female of Kartagener’ssyndrome whose fertility was preserved, a rare entity whichled to delayed diagnosis of the same.
CASE REPORT :A 54-years-old female presented with complaints of
productive cough with profuse expectoration, low gradefever since 1 month. She has recurrent rhinosinusitis andcough with expectoration and low grade fever sincechildhood which subsides on taking medication. The patienthad been married for 30 years and she has two sons. Therewas no history of breathlessness, wheezing, hemoptysis
*Assistant Professor, ** PGT, Department of Pulmonary Medicine, AssamMedical College, Dibrugarh Correspondence Address : Dr.BasantaHazarika, Deparment of pulmonary medicine, Gauhati Medical College,Guwahati-781023 Assam, India. E-mail: [email protected]
or loss of weight. There was no history of similar illness inother members of his family. Clinical examination of thepatient revealed average build with no pallor, pedal edema,clubbing or lymphadenopathy. Patient was febrile 99.6pF, pulse rate 104 beats per minute, respiratory rate 20cycles/min and normal blood pressure 120/70 mmHg inright arm in supine position. Apex beat was localised toright fifth intercostal space(ICS) on mid-clavicular line;and liver dullness was on left side in 5th ICS on percussion–findings suggestive of situs inversus. On chest auscultation,bilateral, lower zone, coarse crepitations were present oninspiration as well as expiration. Routine blood tests didnot reveal any significant abnormality except forleucocytosis and raised ESR. Sputum culture was negativefor acid-fast bacilli, and microbiology. Chest radiographywith bronchography after using dianosil dye (propyliodine)s h o w e ddextrocardiawith the aorticarch lying onright side ofthe tracheawith cysticbronchiectaticchanges seenin both lowerzones andm i d z o n e s(Figure:1)
Figure:1: PA view chest with bronchography
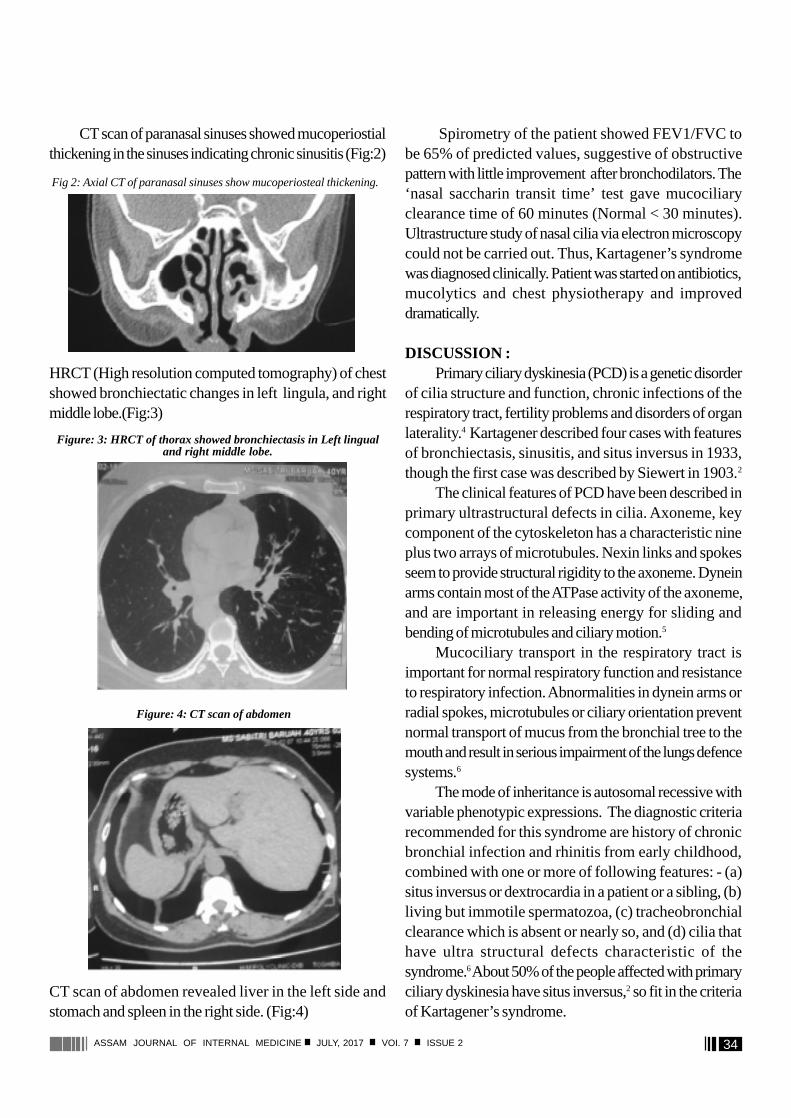
34ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
CT scan of paranasal sinuses showed mucoperiostialthickening in the sinuses indicating chronic sinusitis (Fig:2)
HRCT (High resolution computed tomography) of chestshowed bronchiectatic changes in left lingula, and rightmiddle lobe.(Fig:3)
CT scan of abdomen revealed liver in the left side andstomach and spleen in the right side. (Fig:4)
Spirometry of the patient showed FEV1/FVC tobe 65% of predicted values, suggestive of obstructivepattern with little improvement after bronchodilators. The‘nasal saccharin transit time’ test gave mucociliaryclearance time of 60 minutes (Normal < 30 minutes).Ultrastructure study of nasal cilia via electron microscopycould not be carried out. Thus, Kartagener’s syndromewas diagnosed clinically. Patient was started on antibiotics,mucolytics and chest physiotherapy and improveddramatically.
DISCUSSION :Primary ciliary dyskinesia (PCD) is a genetic disorder
of cilia structure and function, chronic infections of therespiratory tract, fertility problems and disorders of organlaterality.4 Kartagener described four cases with featuresof bronchiectasis, sinusitis, and situs inversus in 1933,though the first case was described by Siewert in 1903.2
The clinical features of PCD have been described inprimary ultrastructural defects in cilia. Axoneme, keycomponent of the cytoskeleton has a characteristic nineplus two arrays of microtubules. Nexin links and spokesseem to provide structural rigidity to the axoneme. Dyneinarms contain most of the ATPase activity of the axoneme,and are important in releasing energy for sliding andbending of microtubules and ciliary motion.5
Mucociliary transport in the respiratory tract isimportant for normal respiratory function and resistanceto respiratory infection. Abnormalities in dynein arms orradial spokes, microtubules or ciliary orientation preventnormal transport of mucus from the bronchial tree to themouth and result in serious impairment of the lungs defencesystems.6
The mode of inheritance is autosomal recessive withvariable phenotypic expressions. The diagnostic criteriarecommended for this syndrome are history of chronicbronchial infection and rhinitis from early childhood,combined with one or more of following features: - (a)situs inversus or dextrocardia in a patient or a sibling, (b)living but immotile spermatozoa, (c) tracheobronchialclearance which is absent or nearly so, and (d) cilia thathave ultra structural defects characteristic of thesyndrome.6 About 50% of the people affected with primaryciliary dyskinesia have situs inversus,2 so fit in the criteriaof Kartagener’s syndrome.
Fig 2: Axial CT of paranasal sinuses show mucoperiosteal thickening.
Figure: 3: HRCT of thorax showed bronchiectasis in Left lingualand right middle lobe.
Figure: 4: CT scan of abdomen

35ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
Screening tests like Exhaled nasal nitricoxide(ENNO) measurement (usually low in PCD) andSaccharin test to assess mucociliary function of nasalepithelium(which is delayed in Kartageners) can be done.Diagnostic tests like electron microscopic confirmation ofthe ultrastructural ciliary defect and video recording forciliary beat pattern and frequency analysis are done. Adultfemales reported a range of fecundity, some achievingpregnancy with no difûculty, others reporting consistentinfertility despite unprotected intercourse.7,8
Female patient in our case did not have fertility issuesand had diagnosis of the syndrome considerably laterepresenting the fact that kartagener’s syndrome has avariable phenotypic presentation. Due to lack of facilitiesfor ENNO and electron microscopic study, in our casediagnosis was made clinico-radiologically.
CONCLUSION : Kartagener’s syndrome (KS) is a rare diseasebelongs to group of primary ciliary dyskinesias(PCDs).This disease comprising a triad of situs inversus,bronchiectasis and sinusitis. Treatment with antibiotics,
physiotherapy and appropriate surgical intervention hasimproved the prognosis in these patients and, in manycases, lifespan may be normal. Early diagnosis is important.Once bronchiectasis is established, prognosis worsenssignificantly.
REFERENCES:1. Barthwal MS. Kartagener’s syndrome in a fertile male - An
uncommon variant. Lung India. 2006;23:123–125.2. Seaton D. Bronchiectasis. In: Seaton A, Seaton D, Leitch AG,
editors. Crofton and Douglas’s respiratory diseases. 5th ed.Oxford: Blackwell Science; 2004. pp. 794–828.
3. Palange AA, Shahid M, Sisode MS, Vaishnav B. Kartagener’ssyndrome: Case Report. International J. of Healthcare &Biomedical Research, October 2013: 2(1): 67-69.
4. Lobo LJ, Zariwala MA, Noone PG. Ciliary dyskinesias: primaryciliary dyskinesia in adults Eur Respir Mon 2011: 52, 130–149.
5. King SM. The dynein microtubule motor. Biochim Biophys Acta.2000; 1496: 60-75
6. Fraser, Muller NL, Colman N et al. Bronchiectasis and otherBronchial Abnormalities.In: Fraser and Pare’s, editors. Diagnosisof diseases of the Chest. 4th ed. Philadelphia. W.B.SaundersCompany; 1999: 2281 – 2283.
7. American Journal of Respiratory and Critical Care Medicine. 2004:169
8. Bush A, Cole P, Hariri M, Mackay I, Phillips G, O’Callaghan C,Wilson R, Warner JO. Primary ciliary dyskinesia: diagnosis andstandards of care. Eur Respir J 1998; 12:982–988.
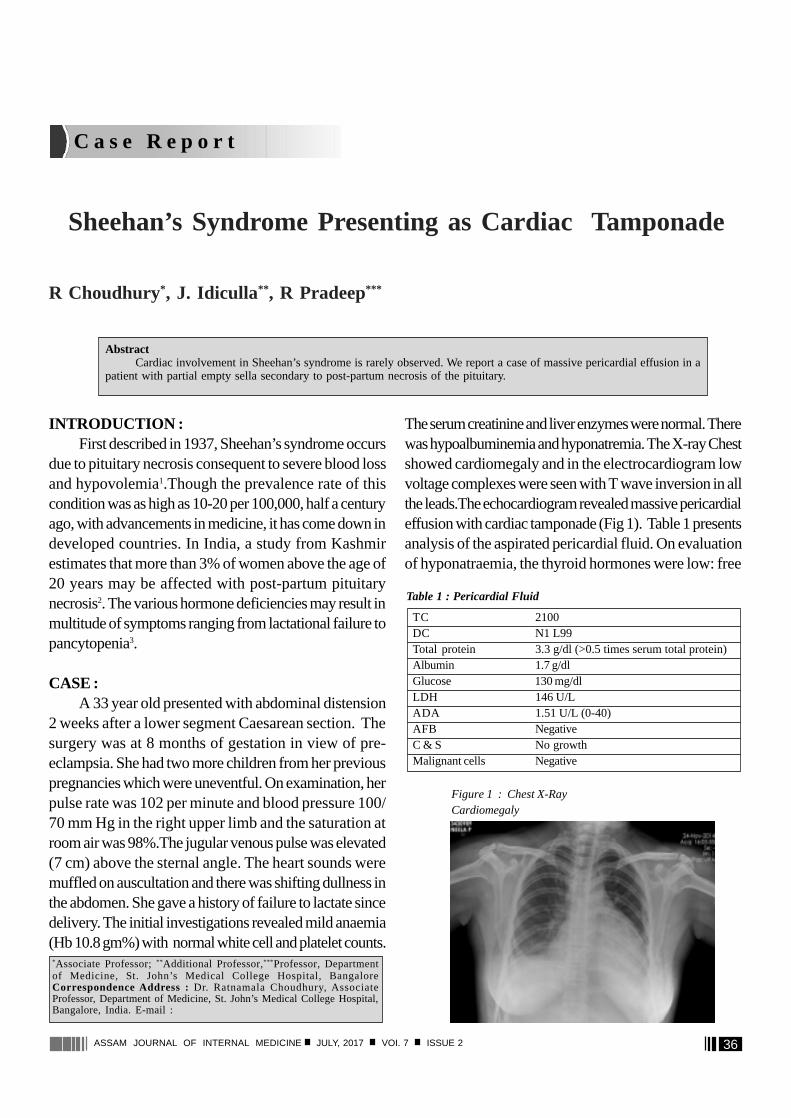
36ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
C a s e R e p o r t
Sheehan’s Syndrome Presenting as Cardiac Tamponade
R Choudhury*, J. Idiculla** , R Pradeep***
*Associate Professor; ** Additional Professor,*** Professor, Departmentof Medicine, St. John’s Medical College Hospital, BangaloreCorrespondence Address : Dr. Ratnamala Choudhury, AssociateProfessor, Department of Medicine, St. John’s Medical College Hospital,Bangalore, India. E-mail :
AbstractCardiac involvement in Sheehan’s syndrome is rarely observed. We report a case of massive pericardial effusion in a
patient with partial empty sella secondary to post-partum necrosis of the pituitary.
INTRODUCTION :First described in 1937, Sheehan’s syndrome occurs
due to pituitary necrosis consequent to severe blood lossand hypovolemia1.Though the prevalence rate of thiscondition was as high as 10-20 per 100,000, half a centuryago, with advancements in medicine, it has come down indeveloped countries. In India, a study from Kashmirestimates that more than 3% of women above the age of20 years may be affected with post-partum pituitarynecrosis2. The various hormone deficiencies may result inmultitude of symptoms ranging from lactational failure topancytopenia3.
CASE :A 33 year old presented with abdominal distension
2 weeks after a lower segment Caesarean section. Thesurgery was at 8 months of gestation in view of pre-eclampsia. She had two more children from her previouspregnancies which were uneventful. On examination, herpulse rate was 102 per minute and blood pressure 100/70 mm Hg in the right upper limb and the saturation atroom air was 98%.The jugular venous pulse was elevated(7 cm) above the sternal angle. The heart sounds weremuffled on auscultation and there was shifting dullness inthe abdomen. She gave a history of failure to lactate sincedelivery. The initial investigations revealed mild anaemia(Hb 10.8 gm%) with normal white cell and platelet counts.
The serum creatinine and liver enzymes were normal. Therewas hypoalbuminemia and hyponatremia. The X-ray Chestshowed cardiomegaly and in the electrocardiogram lowvoltage complexes were seen with T wave inversion in allthe leads.The echocardiogram revealed massive pericardialeffusion with cardiac tamponade (Fig 1). Table 1 presentsanalysis of the aspirated pericardial fluid. On evaluationof hyponatraemia, the thyroid hormones were low: free
TC 2100DC N1 L99Total protein 3.3 g/dl (>0.5 times serum total protein)Albumin 1.7 g/dlGlucose 130 mg/dlLDH 146 U/LADA 1.51 U/L (0-40)AFB NegativeC & S No growthMalignant cells Negative
Table 1 : Pericardial Fluid
Figure 1 : Chest X-RayCardiomegaly
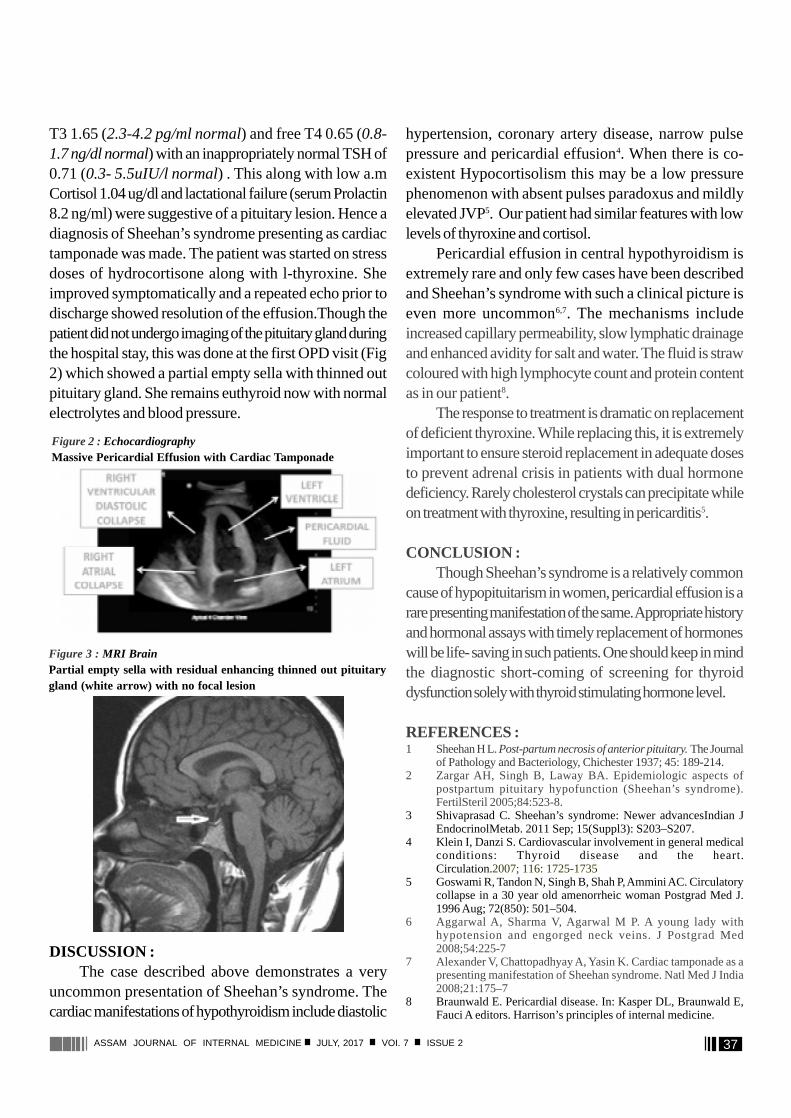
37ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
T3 1.65 (2.3-4.2 pg/ml normal) and free T4 0.65 (0.8-1.7 ng/dl normal) with an inappropriately normal TSH of0.71 (0.3- 5.5uIU/l normal) . This along with low a.mCortisol 1.04 ug/dl and lactational failure (serum Prolactin8.2 ng/ml) were suggestive of a pituitary lesion. Hence adiagnosis of Sheehan’s syndrome presenting as cardiactamponade was made. The patient was started on stressdoses of hydrocortisone along with l-thyroxine. Sheimproved symptomatically and a repeated echo prior todischarge showed resolution of the effusion.Though thepatient did not undergo imaging of the pituitary gland duringthe hospital stay, this was done at the first OPD visit (Fig2) which showed a partial empty sella with thinned outpituitary gland. She remains euthyroid now with normalelectrolytes and blood pressure.
DISCUSSION :The case described above demonstrates a very
uncommon presentation of Sheehan’s syndrome. Thecardiac manifestations of hypothyroidism include diastolic
Figure 2 : EchocardiographyMassive Pericardial Effusion with Cardiac Tamponade
Figure 3 : MRI BrainPartial empty sella with residual enhancing thinned out pituitarygland (white arrow) with no focal lesion
hypertension, coronary artery disease, narrow pulsepressure and pericardial effusion4. When there is co-existent Hypocortisolism this may be a low pressurephenomenon with absent pulses paradoxus and mildlyelevated JVP5. Our patient had similar features with lowlevels of thyroxine and cortisol.
Pericardial effusion in central hypothyroidism isextremely rare and only few cases have been describedand Sheehan’s syndrome with such a clinical picture iseven more uncommon6,7. The mechanisms includeincreased capillary permeability, slow lymphatic drainageand enhanced avidity for salt and water. The fluid is strawcoloured with high lymphocyte count and protein contentas in our patient8.
The response to treatment is dramatic on replacementof deficient thyroxine. While replacing this, it is extremelyimportant to ensure steroid replacement in adequate dosesto prevent adrenal crisis in patients with dual hormonedeficiency. Rarely cholesterol crystals can precipitate whileon treatment with thyroxine, resulting in pericarditis5.
CONCLUSION :Though Sheehan’s syndrome is a relatively common
cause of hypopituitarism in women, pericardial effusion is arare presenting manifestation of the same. Appropriate historyand hormonal assays with timely replacement of hormoneswill be life- saving in such patients. One should keep in mindthe diagnostic short-coming of screening for thyroiddysfunction solely with thyroid stimulating hormone level.
REFERENCES :1 Sheehan H L. Post-partum necrosis of anterior pituitary. The Journal
of Pathology and Bacteriology, Chichester 1937; 45: 189-214.2 Zargar AH, Singh B, Laway BA. Epidemiologic aspects of
postpartum pituitary hypofunction (Sheehan’s syndrome).FertilSteril 2005;84:523-8.
3 Shivaprasad C. Sheehan’s syndrome: Newer advancesIndian JEndocrinolMetab. 2011 Sep; 15(Suppl3): S203–S207.
4 Klein I, Danzi S. Cardiovascular involvement in general medicalconditions: Thyroid disease and the heart.Circulation.2007; 116: 1725-1735
5 Goswami R, Tandon N, Singh B, Shah P, Ammini AC. Circulatorycollapse in a 30 year old amenorrheic woman Postgrad Med J.1996 Aug; 72(850): 501–504.
6 Aggarwal A, Sharma V, Agarwal M P. A young lady withhypotension and engorged neck veins. J Postgrad Med2008;54:225-7
7 Alexander V, Chattopadhyay A, Yasin K. Cardiac tamponade as apresenting manifestation of Sheehan syndrome. Natl Med J India2008;21:175–7
8 Braunwald E. Pericardial disease. In: Kasper DL, Braunwald E,Fauci A editors. Harrison’s principles of internal medicine.
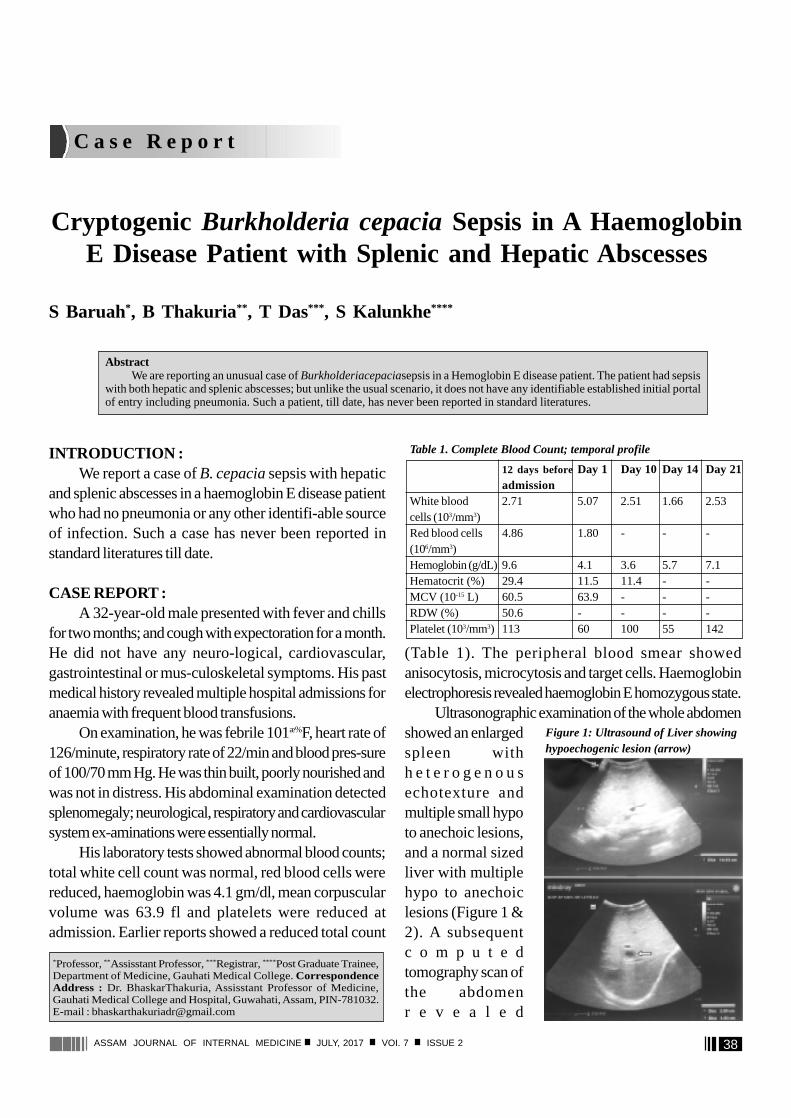
38ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
C a s e R e p o r t
Cryptogenic Burkholderia cepacia Sepsis in A HaemoglobinE Disease Patient with Splenic and Hepatic Abscesses
S Baruah*, B Thakuria** , T Das*** , S Kalunkhe****
INTRODUCTION :We report a case of B. cepacia sepsis with hepatic
and splenic abscesses in a haemoglobin E disease patientwho had no pneumonia or any other identifi-able sourceof infection. Such a case has never been reported instandard literatures till date.
CASE REPORT :A 32-year-old male presented with fever and chills
for two months; and cough with expectoration for a month.He did not have any neuro-logical, cardiovascular,gastrointestinal or mus-culoskeletal symptoms. His pastmedical history revealed multiple hospital admissions foranaemia with frequent blood transfusions.
On examination, he was febrile 101æ%F, heart rate of126/minute, respiratory rate of 22/min and blood pres-sureof 100/70 mm Hg. He was thin built, poorly nourished andwas not in distress. His abdominal examination detectedsplenomegaly; neurological, respiratory and cardiovascularsystem ex-aminations were essentially normal.
His laboratory tests showed abnormal blood counts;total white cell count was normal, red blood cells werereduced, haemoglobin was 4.1 gm/dl, mean corpuscularvolume was 63.9 fl and platelets were reduced atadmission. Earlier reports showed a reduced total count
AbstractWe are reporting an unusual case of Burkholderiacepaciasepsis in a Hemoglobin E disease patient. The patient had sepsis
with both hepatic and splenic abscesses; but unlike the usual scenario, it does not have any identifiable established initial portalof entry including pneumonia. Such a patient, till date, has never been reported in standard literatures.
*Professor, ** Assisstant Professor, *** Registrar, **** Post Graduate Trainee,Department of Medicine, Gauhati Medical College. CorrespondenceAddress : Dr. BhaskarThakuria, Assisstant Professor of Medicine,Gauhati Medical College and Hospital, Guwahati, Assam, PIN-781032.E-mail : [email protected]
(Table 1). The peripheral blood smear showedanisocytosis, microcytosis and target cells. Haemoglobinelectrophoresis revealed haemoglobin E homozygous state.
Ultrasonographic examination of the whole abdomenshowed an enlargedspleen withh e t e r o g e n o u sechotexture andmultiple small hypoto anechoic lesions,and a normal sizedliver with multiplehypo to anechoiclesions (Figure 1 &2). A subsequentc o m p u t e dtomography scan ofthe abdomenr e v e a l e d
Table 1. Complete Blood Count; temporal profile
12 days beforeDay 1 Day 10 Day 14 Day 21admission
White blood 2.71 5.07 2.51 1.66 2.53cells (103/mm3)Red blood cells 4.86 1.80 - - -(106/mm3)Hemoglobin (g/dL) 9.6 4.1 3.6 5.7 7.1Hematocrit (%) 29.4 11.5 11.4 - -MCV (10-15 L) 60.5 63.9 - - -RDW (%) 50.6 - - - -Platelet (103/mm3) 113 60 100 55 142
Figure 1: Ultrasound of Liver showinghypoechogenic lesion (arrow)
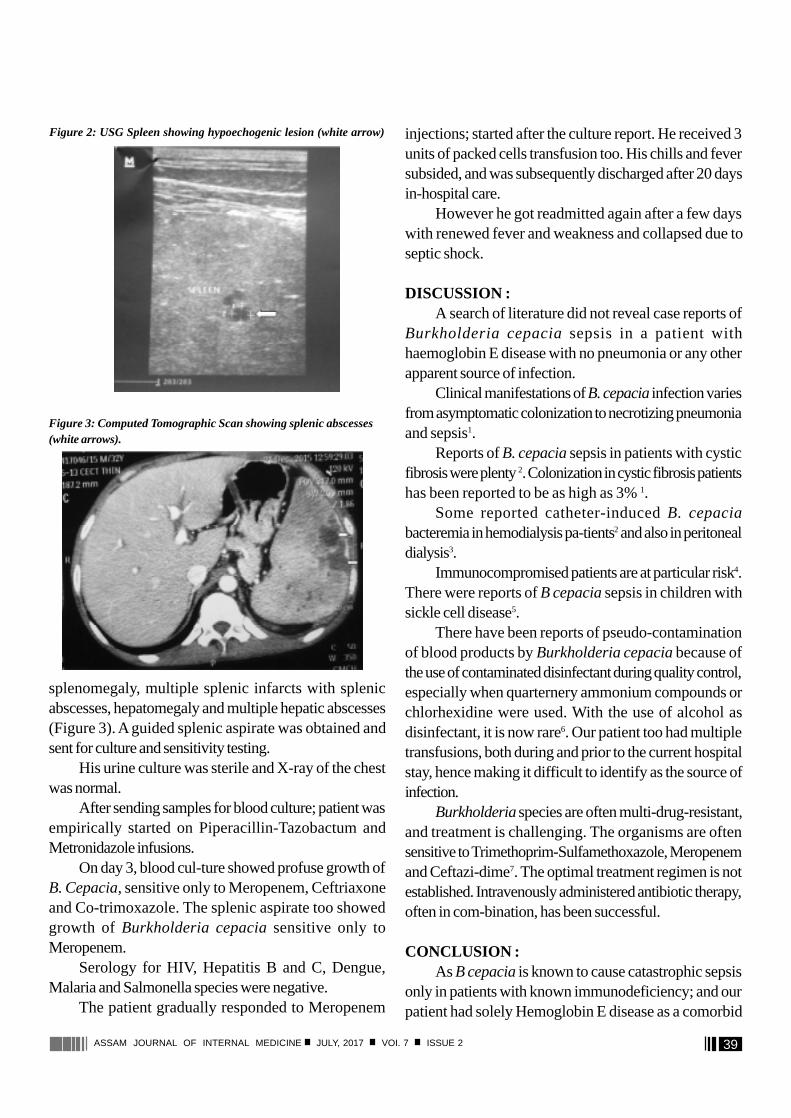
39ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
splenomegaly, multiple splenic infarcts with splenicabscesses, hepatomegaly and multiple hepatic abscesses(Figure 3). A guided splenic aspirate was obtained andsent for culture and sensitivity testing.
His urine culture was sterile and X-ray of the chestwas normal.
After sending samples for blood culture; patient wasempirically started on Piperacillin-Tazobactum andMetronidazole infusions.
On day 3, blood cul-ture showed profuse growth ofB. Cepacia, sensitive only to Meropenem, Ceftriaxoneand Co-trimoxazole. The splenic aspirate too showedgrowth of Burkholderia cepacia sensitive only toMeropenem.
Serology for HIV, Hepatitis B and C, Dengue,Malaria and Salmonella species were negative.
The patient gradually responded to Meropenem
injections; started after the culture report. He received 3units of packed cells transfusion too. His chills and feversubsided, and was subsequently discharged after 20 daysin-hospital care.
However he got readmitted again after a few dayswith renewed fever and weakness and collapsed due toseptic shock.
DISCUSSION :A search of literature did not reveal case reports of
Burkholderia cepacia sepsis in a patient withhaemoglobin E disease with no pneumonia or any otherapparent source of infection.
Clinical manifestations of B. cepacia infection variesfrom asymptomatic colonization to necrotizing pneumoniaand sepsis1.
Reports of B. cepacia sepsis in patients with cysticfibrosis were plenty 2. Colonization in cystic fibrosis patientshas been reported to be as high as 3% 1.
Some reported catheter-induced B. cepaciabacteremia in hemodialysis pa-tients2 and also in peritonealdialysis3.
Immunocompromised patients are at particular risk4.There were reports of B cepacia sepsis in children withsickle cell disease5.
There have been reports of pseudo-contaminationof blood products by Burkholderia cepacia because ofthe use of contaminated disinfectant during quality control,especially when quarternery ammonium compounds orchlorhexidine were used. With the use of alcohol asdisinfectant, it is now rare6. Our patient too had multipletransfusions, both during and prior to the current hospitalstay, hence making it difficult to identify as the source ofinfection.
Burkholderia species are often multi-drug-resistant,and treatment is challenging. The organisms are oftensensitive to Trimethoprim-Sulfamethoxazole, Meropenemand Ceftazi-dime7. The optimal treatment regimen is notestablished. Intravenously administered antibiotic therapy,often in com-bination, has been successful.
CONCLUSION :As B cepacia is known to cause catastrophic sepsis
only in patients with known immunodeficiency; and ourpatient had solely Hemoglobin E disease as a comorbid
Figure 2: USG Spleen showing hypoechogenic lesion (white arrow)
Figure 3: Computed Tomographic Scan showing splenic abscesses(white arrows).

40ASSAM JOURNAL OF INTERNAL MEDICINE JULY, 2017 VOI. 7 ISSUE 2
The Review Process for Articles inASSAM JOURNAL OF INTERNAL MEDICINE
1. Authors submitting a manuscript for publication in the journal agree to the review process.2. The submitted manuscripts are initially reviewed by editors. If it is found suitable for publication it is sent for
further.3. Review by two reviewers, experts in the field.4. The paper will not be accepted for publication if it obtains two negative recommendations.5. Papers are reviewed confidentially and anonymously with “double-blind review process”6. Reviewers must not use knowledge of the manuscript before it is published.7. The paper is assigned an editorial number in order to identify it at later stages of the publishing process.8. An author is informed of the result of the review. The author may appeal a decision to reject a manuscript by
making a request to the Editor.9. The final decision is made by the Editors.10. Upon receipt of the accepted manuscript, the authors will be informed by e-mail, usually within six weeks from
submission.
11. The first author receives a copy of the journal issue in which his/her article is printed.
condition; this case report might prove as a good stimulusto study the associated abnormalities in Hemoglobin Edisease patients to immunohematolgic cell lines other thanred blood cells.
REFERENCES :1. Zuckerman JB, Seder DB. Infection control practice in cys-tic
fibrosis centers. Clin Chest Med. 2007;28(2):381-404.2. Mandell, Douglas, and Bennett’s Principles and Practice of
Infectious Diseases, 7th ed. Churchill Livingstone, An Imprint ofElsevier. 2009.
3. Yap Dy, Chan Jf, Yip T, Mok Mm, Kwan L, Lo Wk, Chan Tm.Burkholderia Cepacia Exit-Site Infection In Peritoneal Dialysis
Patients-Clinical Characteristics And Treatment Outcomes. PeritDial Int. 2015 Oct 22. Pii: Pdi.2015.00122
4. Baylan O. An opportunistic pathogen frequently isolated fromimmunocompromised patients: Burkholderia cepacia complex.Mikrobiyol Bul. 2012 Apr;46(2):304-18.
5. Berry MD, Asmar BI. Pseudomonas cepacia bacteremia in childrenwith sickle cell hemoglobinopathies. Pediatr Infect Dis J. 1991Sep;10(9):696-9.
6. Ebner W, Meyer E, Schulz-Huotari C, Scholz R, Zilow G, DaschnerFD. Pseudocontamination of blood components withBurkholderia cepacia during quality controls. Transfus Med. 2005Jun;15(3):241-2.
7. Zhou J, Chen Y, Tabibi S, Alba L, Garber E, Saiman L. Antimicrobialsusceptibility and synergy studies of Burkholderia cepacia complexisolated from patients with cystic fibrosis. Antimicrob AgentsChemother. 2007;51(3):1085-1088.








![OFFICIAL GAZETTE OF THE HELLENIC REPUBLIC · ΕΠΙΣΗΜΗ ΜΕΤΑΦΡΑΣΗ traduction officielle official translation amtliche Übersetzung Φ09222/6416 [emblem] official gazette](https://static.fdocument.pub/doc/165x107/5fcc1c5ad22df16cce77e303/official-gazette-of-the-hellenic-republic-oe-oe-traduction.jpg)