Acute leukaemias Myelodyplasia - Semmelweis Egyetem€¦ · idarubicin 12 mg/m2 iv. on day 2, 4, 6,...
101
Acute leukaemias Myelodyplasia Dr. Varga Gergely Dr. Varga Gergely Semmelweis Egyetem III. Sz. Belgyógyászati Klinika
Transcript of Acute leukaemias Myelodyplasia - Semmelweis Egyetem€¦ · idarubicin 12 mg/m2 iv. on day 2, 4, 6,...
-
Acute leukaemiasMyelodyplasia
Dr. Varga GergelyDr. Varga GergelySemmelweis Egyetem
III. Sz. Belgyógyászati Klinika
-
Acute leukaemia
-
1st case: 84 y.o. maleHx: myocardial infarct, hypertension.C/o fatigue, weakness and leg oedema, looks pale.Painful ulcers in the mouth for one week.O/E Hepatosplenomegaly, no lymphadenomegaly.Lab.: WBC: 136.000, Hb 85 g/l, PLT: 18.000, LDH: 3288
U/lU/lBloodfilm:
Diagnosis: acute leukaemia
-
AML: typical signsAnaemia:
Palor, weakness, palpitationThrombocytopenia:
GI & nasal bleeding, petechias
Neutropenia:Infections: Infections: Mouth: neutropenic ulcerPneumonia (fungal!)
Hyperviscosity: confusion
Bony pain
Hyperthermia/fever (due to the proliferation)
-
1st case: 84 y.o. maleTreatable / curable?
Myeloid or lymphoid in origin?Morphology, immunohystochemistryFlow cytometryFlow cytometry
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?
-
1st case: 84 y.o. maleTreatable / curable?
Myeloid or lymphoid in origin?Morphology, immunohystochemistryFlow cytometryFlow cytometry
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?
-
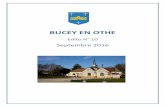
The demography of the AML
100
Incidency/ 100.000
50
Sibling Allogeneic Transplant
MUD transplant
High dose chemo
0
20 40 60 800 Age
De novo, young, no comorbidity:Good prognosis
Elderly, post-MDS, post chemo,several comorbidity: poor prognosis
?Low dose chemotherapy
Only supportion (BSC)
-
1st case: 84 y.o. maleTreatable / curable? No curative treatment in this age
group, BSC, cytoreduction if necessary
Myeloid or lymphoid in origin?Morphology, immunohystochemistryFlow cytometry
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?
-
1st case: 84 y.o. maleTreatable / curable? Kuratív kezelés reménytelen.
Cytoreductio, supportio indokolt.
Myeloid or lymphoid in origin?Morphology, immunohystochemistryFlow cytometry
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?
-
Morphology: AML M0
-
Morphology: AML M2
-
Morphology: AML M3
Auer rods
Hypogranular APL
-
Morphology: AML M4 (myelomonocytic)
-
Morphology: AML M6 (erythroid)
-
Morphology: AML M7 (megakaryocytic)
-
Morphology: ALL
-
Morphology: ALL (Burkitt)
-
Immunohistochemistry
-
Gyűjtő
Flow cytometry
anti
antiCD7
antiCD33
antiCD13
CD34 CD33
CD13
-
Flow cytometry
-
10 1 10 2 10 3 10 4
CD13- FITC -->
10
110
210
310
4
CD
34 P
E -
->CD
34
Flow cytometry in AML
10 20 30 40 50 60
FSC-Height -->
10
20
30
40
50
60
SS
C-H
eigh
t -->
SSC
10 20 30 40 50 60
FSC-Height -->
10
20
30
40
50
60
SS
C-H
eigh
t -->
10 1 10 2 10 3 10 4
CD45 PerCP -->
10
20
30
40
50
60
SS
C-H
eigh
t -->
SSC
CD45
10 1 10 2 10 3 10 4
CD7 FITC -->
10
110
210
310
4
CD
33 P
E -
->CD
33
CD7
CD13- FITC -->
CD13FSC-Height -->
10 1 10 2 10 3 10 4
CD45 PerCP -->
10
20
30
40
50
60
SS
C-H
eigh
t -->
FSC
CD45
FSC-Height -->
FSC
-
WHO classification of AL
-
1st case: 84 y.o. maleTreatable / curable? Kuratív kezelés reménytelen.
Cytoreductio, supportio indokolt.
Myeloid or lymphoid in origin?Morphology, immunohystochemistryFlow cytometry: AML, M1
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?
-
1st case: 84 y.o. maleTreatable / curable? Kuratív kezelés reménytelen.
Cytoreductio, supportio indokolt.
Myeloid or lymphoid in origin?Morphology, immunohystochemistryFlow cytometry: AML, M1
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?
-
1st case: 84 y.o. maleTreatable / curable? Kuratív kezelés reménytelen.
Cytoreductio, supportio indokolt.
Myeloid or lymphoid in origin?Morphology, immunohystochemistryFlow cytometry: AML, M1
Prognosis: poorCytogenetics (cytogenetics, FISH, PCR)Not done
Is stem cell transplant an option?No
-
1st case: 84 y.o. maleHistory of treatment:Transfusion, antibiotics, mouth care continously.1. Low dose azacitidin trial: short lived response, then
progression.2. Hidroxyurea (oral) for cytoreduction: no response.3. Etoposid (oral): tolerated well with a relatively good 3. Etoposid (oral): tolerated well with a relatively good
response for 4 months.Then he developed a pneumonia showed no response
to antibiotics.PM: fungal chest infection with brain involvement.
-
2nd case: 23 y.o. womanNothing remarkable in her medical historyAdmitted to ICU with quickly developed neurological
problems leading to seizures. CT showed subdural haemorrhageWBC: 3.600, hgb: 66 g/l, PLT: 15.000, LDH: 1200, INR:
4,5, APTT: 100, D-dimer: 10,2, fibrinogen 0.14,5, APTT: 100, D-dimer: 10,2, fibrinogen 0.1Bloodfilm:
Diagnosis:
-
2nd case: 23 y.o. womanNothing remarkable in her medical historyAdmitted to ICU with quickly developed neurological
problems leading to seizures. CT showed subdural haemorrhageWBC: 3.600, hgb: 66 g/l, PLT: 15.000, LDH: 1200, INR:
4,5, APTT: 100, D-dimer: 10,2, fibrinogen 0.14,5, APTT: 100, D-dimer: 10,2, fibrinogen 0.1Bloodfilm:
Diagnosis: probable acute promyelocytic leukaemia complicated with DIC
-
Acute promyelocytic leukaemia (APL, FAB M3)
Young adultsWBC is usually normalHypergranular promyelocytes
(hypo-, microgranular in 20%)
Diffuse intravascularcoagulation (DIC)coagulation (DIC)
Flow cytometry: CD13+, CD33+, CD34-, HLA DR-Cytogenetics: t(15;17)PCR: PML-RARαBefore the ‘90s 50% periinduction mortality due to DICNow: complett response (CR): 80-90%
-
Cytogenetics
-
WHO classification of AL
-
PML-RARα: block of differerentation
N-CoR: nuclear coreceptors, HDAC: histone deacetylase
-
PML-RARα: genes involvedClass of genes Examples
Regulators of the cell cycle Cyclins, cyclin-dependent kinases and CDK inhibitors
Cell surface adhesion molecules
CD11b, CD18
Intrinsic host defense systems and extrinsic cytokines
Monocyte chemo-attractant factor, interleukins
Neutrophil granule proteins Defensin, secondary granule proteins, leukocyte alkaline phosphatase, lactoferrinalkaline phosphatase, lactoferrin
Colony-stimulating factors IL-1, IL-8, G-CSF
Colony-stimulating factor receptors
M-CSFR, G-CSFR
Regulators of apoptosis and terminal cell division
Transglutaminase II, bcl2
Structural proteins, enzymes, chromatin components
Clotting factors Thrombomodulin, tissue factor, urokinase, tissue plasminogen activator and its inhibitors
Transcription factors RARs, STATs, Hox genes
-
Mechanism of DIC in APL
Lab. signs: PLT↓, INR↑, APTT↑, Fibrinogen ↓, D-dimer↑
Mediators secreted by the abnormal granulocytes activate the coagulation cascade and the fibrinolysis
Treatment:Supportion: FFP, PLT transfusionall trans retionic acid (ATRA) + chemotherapy alternatively arsenic trioxide
-
ATRA syndrome (Capillary leak syndrome)Signs:• Fever• High WBC: ATRA facilitates the maturation of neutrophils. This
often results in increasing WBC. These cells infilrates the lung, the liver etc leading to organ failure.
• Oedema: Mediators secreted by the neutrophils increase the membrane permeability leading to capillary leakage, which membrane permeability leading to capillary leakage, which results in extravasal fluid retention.
More frequent if initial WBC>10.000Typically in first week25% in ATRA monotherapy;
-
2nd case: 23 y.o. womanTreatable / curable?
Yes: young with no major comorbidity
Diagnosis megerősítéseImmunohistochemistryFlow cytometryFlow cytometryCytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?Siblings?MUD search?
-
2nd case: 23 y.o. womanTreatable / curable?
Yes: young with no major comorbidity
Diagnosis: APLImmunohistochemistryFlow cytometry: CD13+, CD33+, CD34-, HLA DR-Flow cytometry: CD13+, CD33+, CD34-, HLA DR-Cytogenetics (cytogenetics, FISH, PCR):
46XY, t(15;17), PML-RARA confirmed with PCR
Is stem cell transplant an option?Siblings?MUD search?
-
2nd case: 23 y.o. womanTreatable / curable?
Yes: young with no major comorbidity
Diagnosis: APLImmunohistochemistryFlow cytometry: CD13+, CD33+, CD34-, HLA DR-Flow cytometry: CD13+, CD33+, CD34-, HLA DR-Cytogenetics (cytogenetics, FISH, PCR):
46XY, t(15;17), PML-RARA confirmed with PCR
Is stem cell transplant an option?Siblings: noMUD search? no (curable with conventional chemo)
-
Treatment aproach generally in AMLAML
Good: M2 t(8;21),M4 inv(16):
Intermediate: normal, del 7q, +8, t(9,11), -y
Poor: -7, -5, complexcytogenetical abnorm (>2), inv(3), t(6,9), flt3 ITD?
treatable patient
Supportion only
APL M3 t(15;17):different treatment
Chemotherapy
If no remission orrelapse
In case of HLA identicalsibling donor transplant in 1st remission
Transplant in case ofeither HLA identical sibor MUD donor
In case of relapse
Chemotherapy
Chemotherapy
-
The treatment of APL
ATRA 45 mg/m2 orallyidarubicin 12 mg/m2 iv. on day 2, 4, 6, 8
APL M3 t(15;17):different treatment from the othe types of AML
Anthracyclin based postremission treatment
Treatment of relapse:Treatment of relapse:As2O3 (arsenic trioxide)Autologues transplant Mylotarg (anti CD 33 antibody)Combination chemoAllogeneic transplant
Anthracyclin based postremission treatment
Maintenance treatment for 2 years:6 MP/100 mg/m2/dayMTX 10 mg/m2/weekATRA for 2 weeks in every 3 months
-
2nd case: 23 y.o. woman
Developed ATRA syndrome and DIC
� stop ATRA, add
ATRA 45 mg/m2 orallyidarubicin 12 mg/m2 iv. on day 2, 4, 6, 8
APL M3 t(15;17):different treatment from the othe types of AML
Anthracyclin based postremission treatment � stop ATRA, add dexamethason
Died in fungal sepsis
Anthracyclin based postremission treatment
Maintenance treatment for 2 years:6 MP/100 mg/m2/dayMTX 10 mg/m2/weekATRA for 2 weeks in every 3 months
-
3rd case: 54 y.o. maleNothing remarkable in his medical history.
C/o fatigue, weakness for1 month.
Admitted to general ward with perianal infection.with perianal infection.
WBC: 9.600,hgb: 76 g/l, PLT: 35.000, flagged by the lab with immatured cells in the differential
Sent for outpatient haematologist review
-
3rd case: 54 y.o. maleO/E:
no hepatosplenomegaly,
no lymphadenomegaly,
gingival hyperplasia
Diagnosis:
possible acute leukaemia
monocytic?
Admitted to haematology
ward
-
3rd case: 54 y.o. male
Marrow:
Diagnosis: acute leukaemia
-
3rd case: 54 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?ImmunohistochemistryFlow cytometryFlow cytometry
Prognosis?Cytogenetics (cytogenetics, FISH, PCR).
Is stem cell transplant an option?Siblings?MUD search?
-
3rd case: 54 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?ImmunohistochemistryFlow cytometry: AML-M4Flow cytometry: AML-M4
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?Siblings?MUD search?
-
3rd case: 54 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?ImmunohistochemistryFlow cytometry: AML-M4Flow cytometry: AML-M4
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?Siblings?MUD search?
-
AML 5 survival (AML11 trial)Good: M3 t(15;17), M2 t(8;21), M4 inv(16):
curable in 70-75%Intermediate: normal, del 7q, +8, t(9,11), -y
normal & flt3 ITD -ve: curable in aprx 55%normal & flt3 ITD +ve: curable in
-
Cytogenetics
-
WHO classification of AL
-
3rd case: 54 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.Myeloid or lymphoid in origin?
ImmunohistochemistryFlow cytometry: AML-M4
Prognosis?Cytogenetics (cytogenetics, FISH, PCR).46XY, flt3 ITD +ve: poor prognosis
Is stem cell transplant an option?Siblings?MUD search?
-
3rd case: 54 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.Myeloid or lymphoid in origin?
ImmunohistochemistryFlow cytometry: AML-M4
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)46XY, flt3 ITD +ve: poor prognosis
Is stem cell transplant an option?Siblings?MUD search?
-
3rd case: 54 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.Myeloid or lymphoid in origin?
Immunohistochemistry.Flow cytometry: AML-M4.
Prognosis?Cytogenetics (cytogenetics, FISH, PCR).46XY, flt3 ITD +ve: poor prognosis
Is stem cell transplant an option? YesSiblings: one HLA identical sib 48 y.o. healthy maleMUD search? no
-
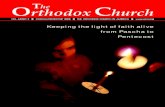
OS DFS
Role of transplant in the treatment of AML
Only chemo n=1314Age: 66 years (44-91)CR in 60%5 OS only in 13%
Transpalnt (RIC) n=253Age: 55 years (18-72)2 DFS: 41%
-
AML
Good: M2 t(8;21),M4 inv(16):
Intermediate: normal, del 7q, +8, t(9,11), -y
Poor: -7, -5, complexcytogenetical abnorm (>2), inv(3), t(6,9), flt3 ITD?
treatable patient
Supportion only
APL M3 t(15;17):different treatment
Role of transplant in the treatment of AML
Chemotherapy
If no remission orrelapse
In case of HLA identicalsibling donor transplant in 1st remission
Transplant in case ofeither HLA identical sibor MUD donor
In case of relapse
Chemotherapy
Chemotherapy
-
3rd case: tratmentAML
1. 7+3 (DA) induction:BM showed 8% residual blasts
2. FlagIDA reinduction: CRHLA identical sib identified
3. 2x HD-AC consolidation
treatable patient
Poor: -7, -5, complexcytogenetical abnorm (>2), inv(3), t(6,9), flt3 ITD?
Organising the transplant 4. Succesful transplant in the first
remission with no major problem5. Alive and well
Chemotherapy
Transplant in case ofeither HLA identical sibor MUD donor
-
4th case: 55 y.o. maleHx of diabetes for 10 years, on oral antidiabetics.C/o fatigue, weakness for 1 month.Admitted to the general ward
with fever and skin lumps.WBC: 100.000, HGB 98 g/l,
PLT 80.000.For haematologist review
due too these.
-
4th case: 55 y.o. maleO/E marked hepatosplenomegaly.Bloodfim:
Diagnosis: acute leukaemia (myelomonocytás?)
-
4th case: 55 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?Flow cytometry
Prognosis?Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?Siblings?MUD search?
-
4th case: 55 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?Flow cytometry: AML M4
Prognosis?Prognosis?Cytogenetics (cytogenetics, FISH, PCR).
Is stem cell transplant an option?Siblings?MUD search?
-
4th case: 55 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?Flow cytometry: AML M4
Prognosis: Prognosis: Good (46XY, inv 16)
Is stem cell transplant an option?Siblings?MUD search?
-
4th case: 55 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?Flow cytometry: AML M4
Prognosis: Prognosis: Good (46XY, inv 16)
Is stem cell transplant an option?Siblings? No.MUD search? No. (only in relapse)
-
4th case: 55 y.o. maleTreatable / curable?
Yes: young with no comorbidity, consented for chemo.
Myeloid or lymphoid in origin?Flow cytometry: AML M4
Prognosis: Prognosis: Good (46XY, inv 16)
Is stem cell transplant an option?Siblings? No.MUD search? No. (only in relapse)
Plan: Chemotherapy, monitoring of gene mutation
-
Terápiás válasz, minimális reziduális betegségIndukction Consolidation chemotherapies
1012
109
N of BlastsMorphology
Flow cytometry (abnormal coexpression of CD markers)
Cytogenetics?
No remission: poor prognosis� more aggressive treatment & transpalnt
„7+3” „7+3” „HD-AC” „HD-AC”„HD-AC”
10
106
103
Cytogenetics
Molecular genetics (bcr-abl in ALL)
?
?
FISH (inv 16)
Diagnosis Controll marrow tests
-
The fluorescens in situ hibridisation (FISH) test
Hybridisation
-
5q- 7q- +8
Options for FISH
-
AML
Good: M2 t(8;21),M4 inv(16):
Intermediate: normal, del 7q, +8, t(9,11), -y
Poor: -7, -5, complexcytogenetical abnorm (>2), inv(3), t(6,9), flt3 ITD?
treatable patient
Supportion only
APL M3 t(15;17):different treatment
Treatment plan at presentation
Chemotherapy
If no remission orrelapse
In case of HLA identicalsibling donor transplant in 1st remission
Transplant in case ofeither HLA identical sibor MUD donor
In case of relapse
Chemotherapy
Chemotherapy
-
AML
Good: M2 t(8;21),M4 inv(16):
Intermediate: normal, del 7q, +8, t(9,11), -y
Poor: -7, -5, complexcytogenetical abnorm (>2), inv(3), t(6,9), flt3 ITD?
treatable patient
Supportion only
APL M3 t(15;17):different treatment
The signification of the BM test on day 28
1st cycle chemo
Transplant in case ofeither HLA identical sibor MUD donor
1st cycle chemo
Chemotherapy
CR after induction chemo?
Salvage treatment (Flag-IDA)
No
Carry on according to the original plan
Yes
-
5th case: 60 y.o. male60 y.o. male.Hx: Diabetes, hypertension.Long standing anaemia, GP prescribed iron. Now developed pancytopenia, sent for haematologsist
outpatient review.WBC: 2.600, (ne: 23%), hgb: 81, MCV: 102, PLT: WBC: 2.600, (ne: 23%), hgb: 81, MCV: 102, PLT:
65.000, LDH: 300Bloodfim:Pseudo-Pelger anomaly, hypogranulatedgranulocytes, abnormal RBC morphology
Diagnosis: myelodysplasia→ Needs Transfusion→ Needs BM for staging
-
5th case: 60 y.o. male: bone marrow
Dysplasiás granulocyták
MicromegakaryocytákMicromegakaryocyták
-
MyelodysplasiaClonal disease, praeleukaemiaAbnormalities in 1/2/3 cell line. Hyperrcellular marrow, with dysplastic maturation → cytopenia
Rarely hypocellular marrow (differential: aplastic anaemia)
Patomechanism: deletion of genes rosponsible for maturation, apoptosis.
Patomechanism: deletion of genes rosponsible for maturation, apoptosis.
Growth advantege of the clone which suppresses the normal marrow.
Progression toward acute leukaemia.
-
MyelodysplasiaMainly in elderly pts (avearage 70 yo.) Primery or secoundery: post chemo- or radiotherapy
Currently no available treatment, except trials.
-
MDS blast
Myelodysplasia
Dysplastic cells, intramedullary apoptosis
-
Myelodysplasia: WHO classification
-
Myelodysplasia: IPSS
-
Myelodysplasia: kezelés• Szupporton
– transfusion + iron depletion!
• Intermediate:– biological modificators:
– EPO, GCSF– Immunsuppression– Thalidomid, lenalidomid
IPSSLow, Intermed-1
– Thalidomid, lenalidomid
– low dose chemo– Ara-C– 5-azacytidin
• Intensive chemo– AML type induction
• SC transplant– RISCT
IPSSIntermed-2, High
-
5th case: 60 y.o. maleTreatable / curable?
Maybe
Myeloid vagy lymphoid:Flow cytometry
Prognosis?Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?Siblings?MUD search?
-
5th case: 60 y.o. maleTreatable / curable?
Maybe
Myeloid vagy lymphoid: egyértelmű. Dg: RCMD.Flow cytometry: number of blasts: 5-10%
Prognosis?Prognosis?Cytogenetics (cytogenetics, FISH, PCR).
Is stem cell transplant an option?Siblings?MUD search?
-
5th case: 60 y.o. maleTreatable / curable?
Maybe.
Myeloid vagy lymphoid: egyértelmű. Dg: RCMD.Flow cytometry: number of blasts: 5-10%
Prognosis: IPSS: High/IntermedPrognosis: IPSS: High/IntermedCytogenetics : 45XY, -7: poor prognosis
Is stem cell transplant an option?Siblings?MUD search?
-
5th case: 60 y.o. maleTreatable / curable?
Maybe.
Myeloid vagy lymphoid: egyértelmű. Dg: RCMD.Flow cytometry: megerősítés, blast arány: 5-10%
Prognosis: IPSS: High/IntermedPrognosis: IPSS: High/IntermedCytogenetics : 45XY, -7: poor prognosis
Is stem cell transplant an option? YesSiblings? NoMUD search? ASAP
-
6th. case: 23 y.o. maleNothing ramarkable in medical history.Unwell for 2 weeks, fever and boney pain since
yesterday.WBC: 26.000, ne: 13%, hgb: 103, PLT: 35e, LDH: 3500Boodfim:Immatured blastsprobable lymphoid origin
Diagnosis: ALL?→ Needs BM for flow cytometry (diagnosis)cytogenetic (prognosis)
-
6th. case: 23 y.o. male
-
6th. case: ALL prognosis
-
ALL in generalMore common in children
-
ALL in general
-
Treatable / curable? Yes
Myeloid vagy lymphoid:Flow cytometry:
Prognosis?
6th. case: 23 y.o. male
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?Siblings?MUD search?
-
Treatable / curable? Yes
Myeloid vagy lymphoid:Flow cytometry: pre B-ALL
Prognosis?
6th. case: 23 y.o. male
Prognosis?Cytogenetics (cytogenetics, FISH, PCR)
Is stem cell transplant an option?Siblings?MUD search?
-
Treatable / curable? Yes
Myeloid vagy lymphoid:Flow cytometry: pre B-ALL
Prognosis?
6th. case: 23 y.o. male
Prognosis?Cytogenetics: no t(9;22), t(4;11) or hyperdiploid
Is stem cell transplant an option?Siblings?MUD search?
-
Treatable / curable? Yes
Myeloid vagy lymphoid:Flow cytometry: pre B-ALL
Prognosis?
6th. case: 23 y.o. male
Prognosis?Cytogenetics: no t(9;22), t(4;11) or hyperdiploid
Is stem cell transplant an option?Siblings? Needs HLA testingMUD search? If no remission or MRD positive
-
6th. case: 23 y.o. maleHappy end1st week periferal blood clear4th week BM morpologically normal8th week BM flow cytometry showed no abnormal
phenotype
in remission for 4 years.
-
Allogén őssejtátültetés
J Clin Invest. 1959; 38: 1709–1716.
Seattle csoport:
• Kutyakísérletek
• 1977, 100 végstádiumú AML
-
Súlyos morbiditás
Bortin, MM A compendium of reported human bone marrow transplants. Transplantation 1970
-
Acute GvHDInkompatibilitás•HLA antigének•Tumor antigének•Vírus antigének
Immunrendszer•Kondicionálás okozta
szövetkárosodásT-sejtek szövetkárosodás•IL-1, TNF, GM-CSF•T-sejt-aktiváció•Citokin vihar
Rizikó faktorok•Kondicionálás•Életkor•Nem•Fertőzések•SC forrás•T-sejt-tartalom
T-sejtek
-
Egyéb halálos
toxicitás
Chemotherapy dózisa és a gyógyulás esélye
Irreverzibilis csontvel ő-
károsítás
Esély a kurabilitásra
Autológ transzplantá-ció
-
Elég lenne az autológ „átültetés”?
• Nagydózisú kemoterápia adható
• Nincs donorkeresés• Alacsony mortalitás (5%)• Tárgyi feltételei egyszerűek
• Ritkán kuratív• Szennyezett graft• Hosszú távú toxicitás:
szekunder tumorok
-
Transzplantáció utáni halálozás1998-2002
Toxikus szerv-károsodás
Rokon donor Idegen donorGvHD
SUM05_20.ppt
Infekció
Egyéb
Ismeretlen
Center for International Blood and Marrow Transplant Research
Autológ
Relapsus (75%)
-
Syngenikus átültetés CML-ben
Ann Intern Med. 1994 120(8):646-52
-
Mi a különbség oka?
RECIPIENS DONOR
GvHD
GVL
-
Bizonyítékok a GVL hatásra:
1. Kevesebb relapsus allogénben, mint
autológban
2. Kevesebb relapsus GvHD kialakulása caseén, 2. Kevesebb relapsus GvHD kialakulása caseén,
mint ha nincs GvHD
3. Relapsus reagálhat az immunszuppresszió
leállítására
4. Relapsus reagálhat DLI-re
-
A GVL hatás mértéke:
Jelentős CMLLow grade NHL
Mérsékelt AMLMérsékelt AMLHodgkin-lymphomaMyeloma
Alig/nem ALLHigh grade NHL
-
Transzplantáció mérlegelése
Agresszív betegség Kemoterápiától gyógyulásAgresszív betegségRelapszusFiatal, kevés társbetegségMagas GVL hatás
Kemoterápiától gyógyulásvárhatóAlacsony GVL hatásNincs donor
Transzplantáció Kemoterápa